")
Back to Journals » Patient Preference and Adherence » Volume 18
Spanish Translation and Cultural Adaptations of Physical Therapy Parent Educational Materials for Use in Neonatal Intensive Care
Authors McCarty DB, Sierra-Arevalo L, Caldwell Ashur AC, White JT , Villa Torres L
Received 13 September 2023
Accepted for publication 23 December 2023
Published 12 January 2024 Volume 2024:18 Pages 93—100
DOI https://doi.org/10.2147/PPA.S432635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Dana B McCarty,1 Leslie Sierra-Arevalo,2 Ana-Clara Caldwell Ashur,1 J Tommy White,3 Laura Villa Torres4
1Department of Health Sciences, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, USA; 2Physical and Occupational Therapy, Duke University Health System, Durham, NC, USA; 3North Carolina Clinical and Translational Sciences Institute, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 4Public Health Leadership Program, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Correspondence: Dana B McCarty, Department of Health Sciences, University of North Carolina at Chapel Hill School of Medicine, 3024 Bondurant Hall, CB#7135, Chapel Hill, NC, 27599-7135, USA, Tel +1 919 843 8792, Fax +1 919 966 3678, Email [email protected]
Background: A paucity of Spanish language, culturally relevant parent education materials in the healthcare setting results in suboptimal care for Latinx families and further perpetuates health disparities. The purpose of this article is to describe the process for Spanish translation and cultural adaptations to parent education materials of a parent-centered physical therapy program designed to support maternal mental health and infant development during Neonatal Intensive Care (NICU).
Methods: Two bilingual physical therapy (PT) students translated educational materials from English to Spanish and were proofread by a professional translator. Next, we conducted a materials review with 5 members of the Latine Community Review Board (CRB), a “standing” advisory group of natively Spanish-speaking, Latine North Carolinians who contract with research teams under the coordination of the Inclusive Science Program (ISP) of the North Carolina Translational and Clinical Sciences Institute (NC TraCS). Review session recruitment, facilitation, and data analysis were conducted by bilingual NC TraCS project managers and the primary investigator for the main feasibility study. Readability analyses were performed at the final stage of translation and adaptation.
Results: Themes from CRB review sessions for improvement included to 1) use parent-friendly language, 2) use the plural masculine form of gendered language for caregivers to include all gender identities in this neonatal context, 3) address challenges with direct translation, and 4) use written education materials to supplement in-person, hands-on training with parents and their infants. All translated materials received a grade level of 5 on the Crawford grade-level index.
Conclusion: Based on CRB feedback and readability analysis, the translation and cultural-adaptation process resulted in comprehensible written parent education materials for Spanish-speaking families. Review meetings with the CRB reinforced the need for Spanish materials in the healthcare setting. Further assessment of these materials with Spanish-speaking families in the NICU setting is needed.
Keywords: patient education, Spanish, translation, cultural adaptation, neonatal intensive care, parents
Introduction
Parents of extremely preterm infants experience high rates of postnatal anxiety, depression, and stress that negatively impact parent-infant bonding, mental health, and infant developmental outcomes.1,2 Both parent’s presence and engagement during the neonatal intensive care unit (NICU) stay is important for the current and future health of the parent and infant.3,4 Developmental outcomes for infants born preterm rely heavily on the development of the parent–infant relationship,5,6 but unfortunately, there are many barriers to facilitating positive parent–infant interactions in the NICU. Many parents perceive the NICU as an intimidating environment.7 Higher levels of parenting self-efficacy are associated with better coping responses and parental adjustment;8 therefore, providing family support materials and resources may reinforce newly-gained knowledge and bolster parenting confidence,9 which ultimately leads to positive psychological outcomes for parents and developmental outcomes of infants.
Patients who do not speak English or have limited English proficiency are at high risk of experiencing health disparities and barriers to accessing appropriate resources and support within the American healthcare system.10 Specifically, the lack of translated and culturally adapted patient education materials in hospital and healthcare settings presents a significant barrier to Latinx/ Hispanic patients receiving the standard of care.10,11 However, despite the well-documented need for translated and culturally adapted patient education materials and programs to support positive outcomes and experiences in Spanish-speaking patients,12 healthcare systems face multiple barriers to implementation,13 and there is limited consensus around best practices for how to translate medical education materials.14 In the NICU, Spanish-speaking families face numerous challenges to engaging in regular communication and receiving updates from their infant’s providers, navigating the physical hospital environment, and understanding their infant’s medical condition, which can exacerbate previously discussed mental health concerns.15
The Therapist Education and Massage for Parent-Infant Outcomes (TEMPO) program is a therapist-led and parent-centered program designed by the primary investigator (PI) (DM) to support parent mental health by training them to deliver massage and other therapeutic interventions throughout infant hospitalization while simultaneously supporting preterm infant development. TEMPO standardizes the nature and frequency of parent education through weekly therapy education sessions with a primary therapist. The components of TEMPO program are evidence-based and include infant massage,16 parent-delivered motor interventions focused on promoting midline orientation and opportunity for spontaneous active movement,17,18 principles of family-integrated care,19 and multiple modes of educational delivery20 to enhance parent retention and confidence in continuing activities post-discharge.
The Latinx/ Hispanic population is the fastest growing racial/ethnic group in the United States and has grown by more than 50% in the last decade, reaching more than 62.1 million in 2020;21 yet, evidence suggests that disparities in health access and outcomes are perpetuated in Spanish-speaking families.22 The purpose of this study was to translate and culturally adapt parent education materials into Spanish for a parent-centered physical therapy program,23,24 which was designed to support parent mental health and infant development during Neonatal Intensive Care.
Methods
Setting
The Newborn Critical Care Center (NCCC) of UNC Children’s Hospital, where the primary study was conducted, is a regional Level IV, 58-bed facility averaging 800 admissions annually. UNC Children’s serves children from all 100 counties in the state of North Carolina, which has more than 1 million Latinx/Hispanic residents according to 2020 census data. The primary feasibility study of the therapist-led and parent-centered educational program, TEMPO, as well as the study activities for translation of education materials, were approved by the Institutional Review Board of the University of North Carolina at Chapel Hill. The study was pre-registered at ClinicalTrials.gov under the identifier: NCT04121897 in October 2019.
Therapist Education and Massage for Parent-Infant Outcomes (TEMPO) Program
Two main education sessions in the TEMPO program were supplemented by written education materials: 1) the Early Parent Education pamphlet provided at the first educational session and 2) the Discharge Parent Education pamphlet provided at the final educational session immediately prior to discharge. A Template for Intervention Description and Replication (TIDieR) for TEMPO25 has been included in the supplementary section of this article (Appendix A).
Development of Materials, Initial Translation and Certified Translation
The Early Parent Education pamphlet and Discharge Parent Education pamphlets were originally developed by the PI (DM), a board certified pediatric clinical specialist in pediatrics, based on evidence-based approaches to preterm infant development.18–21 Both written educational pamphlets were initially translated by two bilingual physical therapy (PT) students (LSA, ACA) as part of their capstone project requirement for the Doctor of Physical Therapy degree. The translation was then proofread and edited for clarity by a local minority-owned, American Translators Association certified, professional translation service (Figure 1).
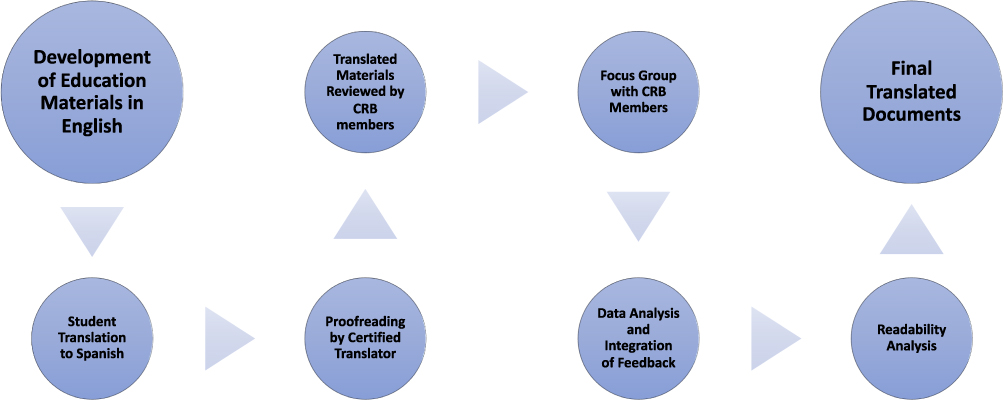 |
Figure 1 Outline of the translation and cultural adaptation process. Abbreviation: CRB, Community Review Board. |
Latine Advisory Board Reviews
This Latine Community Review Board (CRB) is a “standing” advisory group of natively Spanish-speaking, Latine North Carolinians who contract with research teams under the coordination of the Inclusive Science Program (ISP) of the North Carolina Translational and Clinical Sciences Institute (NC TraCS), to review Latine community-facing study materials and provide recommendations for improving or validating materials’ linguistic accuracy and cultural relevance. At the time that this study was conducted, NC TraCS had recruited a pool of 5 Latine CRB members with the intention of establishing an advisory group that reflects the diversity of local Latine communities with respect to countries of origin, educational attainment, and professional backgrounds. Per ISP procedures, bilingual ISP staff facilitated CRB members’ independent reviews of both the English and Spanish language document versions, and then utilized focus group methods to facilitate Spanish language group review sessions, solicit group feedback, and report key findings and suggested revisions. The study PI (DM) was present during review sessions so that when necessary, the bilingual facilitators (JTM, LVT) were able to ask the PI clarifying questions, such as related to study protocol or the intended meaning of English language materials, on behalf of the CRB members. All CRB members provided informed consent in accordance with the Declaration of Helsinki.
CRB member recruitment, review session facilitation, and data analysis were conducted by bilingual staff members (LVT, TW) of ISP. At the time of these reviews, the CRB was comprised of a total of 5 Spanish-speaking CRB members with experience reviewing health education materials. These members lived in North Carolina; collectively, they were born in Mexico, Venezuela, and Honduras; all were women and reflected diversity in age, parenting status, level of education, and English proficiency. Two of the review session participants were familiar with the NICU setting – one as a volunteer infant cuddler in a local NICU and the other as a hospital housekeeper in NICU. In total, CRB members reviewed 8 pages of translated, Spanish language TEMPO materials (the Early Parent Education pamphlet and the Discharge Parent Education pamphlet) as well as all correlating English language versions. All CRB members were compensated for their independent review time as well as the group review sessions.
A review meeting discussion guide has been attached in Appendix B. This guide was created collaboratively between the PI (DM), one physical therapy student (LSA), and the ISP team (TW, LVT). The review meeting was conducted in Spanish, but for the purpose of this article, quotes from the review sessions have been translated to English.
A total of 3 sessions were held to review the educational materials. All review sessions were held via Zoom platform due to the continued need for social distancing due to the COVID-19 pandemic. The meeting identification code and password were provided directly to all participants to ensure privacy of information. The first session was made up of 5 CRB members and was facilitated by two bilingual PT students (LSA, ACA), a bilingual research specialist, and the PI (DM) for the TEMPO study and lasted 2 hours. During this session, the bilingual research specialist and PT students facilitated discussion using prompts from the guide, and the PT students took notes. While the PI was not fluent in Spanish, she was available for the participants and facilitators to ask clarifying questions throughout all review sessions. Following the initial session, it was clear that additional input regarding gender-inclusive language and brainstorming around parent-friendly language would be beneficial, and another review session was planned with research specialists with expertise in these areas.
The next review session included 3 of the original 5 CRB members, two bilingual review session facilitators (LVT and TW) and the PI (DM) and lasted 2 hours. The two bilingual PT students who originally translated the written materials (LSA, ACA) were not present, reducing the potential for bias and conflict of interest. Overall discussion was animated and extensive, and the members were able to complete feedback for the Early Parent Education pamphlet but were unable to complete feedback on the Discharge Parent Education pamphlet within the first session alone. Thus, a third, 1 hour session was scheduled for the following week to resume and complete feedback on the second document.
During the review sessions, primary facilitator (LVT) utilizing open-ended questions from the above guide; and then proceeded to lead CRB members through each document from beginning to end, soliciting input for each session in chronological order. Another facilitator (JTW) provided facilitation support, discussion prompts regarding gendered language, and live document revision via use of screen sharing and track changes. The review sessions were audio recorded through the Zoom platform. Audio recordings and chat transcripts were uploaded for the study team to analyze results (Figure 1).
Data Analysis and Feedback Integration
Following the review sessions, ISP staff (JTW, LVT) reviewed discussion notes, as well as audio files where helpful, to organize and summarize group feedback according to predetermined topics (per interview guide) and applicable content areas/sections of the materials. Additional points of feedback that emerged during the review discussions were categorized by subject area and summarized. The PI, in consultation with ISP staff, integrated the summarized feedback into the translated documents (Figure 1).
Readability Analysis
The educational materials were originally written in English. Investigators applied the Coleman-Liau Index26 to the English versions of the Early Parent Education pamphlet, which resulted in a score of grade level 10 and the Discharge Parent Education pamphlet scored grade level 8. Therefore, the educational materials in English did not reach the AMA recommended 6th grade reading level. The PI and research team did not feel that the English language text should be adjusted to a lower reading levelbecause the pamphlet’s medical and developmental terminology in the written materials was intended to be reviewed with the parent to enable them to participate in and understand a variety of medical interactions during the NICU stay. The parent education pamphlets were designed to be used alongside hands-on and verbal education from the therapist. In order to assess translated materials for readability and grade level equivalence, we used Legible,27 an online readability Spanish text analyzer to determine the Crawford grade-level equivalent,28 at the end of the translation process (Figure 1).
Results
Overall Impressions and Need for Educational Materials
To gain overall impressions of the educational materials, the CRB members were asked if they would recommend these materials to a family member or friend who had an infant admitted to the NICU, and all 5 members agreed that they would recommend this program and its educational materials. The two CRB members with previous exposure to the NICU setting reported witnessing Spanish-speaking families not having a way to communicate with providers and these families would often request their assistance to speak with their infant’s nurse. One participant said, “There are no providers that speak Spanish. All the signage on the floor is in English, and all the information they were given was always in English”, and expressed frustration about the lack of resources available to Spanish-speaking patients and families.
Parent-Friendly Language
First, the CRB members expressed appreciation for the simplicity and friendly language used in the materials. Despite a diversity in dialect exposures among members ranging from Venezuela, Mexico, and Honduras, all participants agreed that the language presented in the materials was appropriate and easily understood. Additionally, members expressed familiarity and/or understanding of the activities presented in the materials. Not only did they express a general understanding of the activities based on the name of the game (eg, “bicycles” and “hug-the-baby”), they reported that even though they may not know exactly what the phrase means, that the activity name being in quotation marks indicated to them that it would be an activity that was taught by the therapist. This was a correct interpretation of the information, as all activities are intended to be reviewed hands-on with the parents when the materials were presented.
Gender Inclusive Language
In most cases during the review meetings, language revisions that were suggested by one CRB member or another were quickly and unanimously confirmed by all members as appropriate corrections or improvements to improve readability in Spanish language; however, discussion was lengthier with respect to the selection of gendered noun options (ie, feminine singular, feminine plural, masculine singular, masculine plural, and other options such as indicative of non-binary persons) referring to the infant and/or the reader or presumed caregiver. The facilitated discussion of this topic solicited participants’ consideration of multiple options and responded to PI input where requested. With the goal of creating written materials that were both easily read and understood, as well as to reflect and include gender diverse birthing parents and caregivers, CRB reviewers determined to utilize the plural masculine form as a means of maintaining readability for a range of literacy levels (plural masculine form is traditional) while also not as broadly misgendering post-partum parents who are men and/or non-binary via an explicitly feminine plural form. Similarly, the reviewers determined to reference the infant without using gendered language by consistently referring to the infant as “your baby”, which does not require the use of a gendered article.
Direct Translation Challenges
Several revisions focused on more clearly describing a physical movement, condition, or developmental status that did not have a direct, common use Spanish language translation. For example, the term “swaddle” in English does not exist in Spanish, so researchers and CRB members came up with various terms to describe the action of swaddling. In these instances, clarification from the PI was helpful in achieving group understanding of the exact movement or state that the material was attempting to reference. It was suggested that these final translated materials may provide the interpreters, too, with helpful language for describing movements, conditions, and developmental statuses. Participants suggested using various “and” and “or” language to allow for multiple terms to be used so that individuals from different backgrounds could understand the intended meaning.
Using Written Materials to Supplement Hands-on Education
CRB members suggested that due to the depth and breadth of the material covered that the therapists should review the information and practice the activities in the materials with the parents in a hands-on manner, using the written materials to supplement the training session. They felt that this structure would help alleviate any stress or feelings of being overwhelmed that parents might feel when learning new information about their preterm infant. Additionally, CRB members appreciated the use of pictures and images to aid in comprehension of materials and provide visual context to many of the instructions.
Readability Analysis
After all edits had been made based on professional translator and CRB members feedback, the written materials were analyzed using “legible.es”, an online text readability analyzer for Spanish text. Based on the Crawford grade-level index,28 the Early Parent Education pamphlet was approximately at grade level 5.8 (eg, number of school years needed to understand) and the Discharge Parent Education pamphlet at grade level 5.1.27
Discussion
Our team developed, translated, and successfully adapted written education materials for parents of preterm infants into Spanish. This multi-step process that involved students, professional translators, researchers, and Spanish-speaking community members resulted in written educational materials that Spanish-speaking parents from a variety of backgrounds and dialects can read and understand. Based on CRB feedback and readability analysis, the translated and culturally adapted caregiver education materials appear to be comprehensible and useful. The review meetings also reinforced the need for Spanish materials in the healthcare setting. Further assessment of these materials with Spanish-speaking families in the NICU setting is needed.
Overall, CRB members expressed a significant need for accessible written educational materials in the US healthcare setting. CRB members also expressed the need to use more descriptive language to better explain concepts that are not easily translatable. CRB members felt that using the plural masculine form to be inclusive of all caregivers (eg, mother, father, caregiver) and gender identities. Another important theme that emerged was the importance of using these written materials to supplement hands-on education. Finally, grade-level analysis revealed that the translation and adaptations made during this process resulted in Spanish grade-level equivalencies within the NIH recommendations for patient education materials.
Despite a lack of robust research in this area, it is well understood that not only is there a dearth of accessible translated patient education materials throughout the health care system, but of what does exist, there is often a mismatch between the level of knowledge necessary to understand the materials and the health literacy of the patients receiving the information.13,29 While Spanish is the leading non‐English language in the US, the Latinx/ Hispanic population has one of the lowest health literacy rates in the country; therefore, among Spanish speakers, limited English proficiency contributes to a lower quality of care and ultimately, to worse health outcomes.29 In an effort to offset the challenges faced by low health literacy in the Latinx/ Hispanic community, the process we used resulted in higher readability and lower grade level equivalence in Spanish translated texts. Use of patient education materials written in patient-friendly language can also support medical interpreters and bilingual family members in communicating important concepts provided by the medical team.
In a study by Olenik et al, Spanish-speaking interviewees expressed overall frustration about how lack of medical insurance perceived negative attitudes from hospital personnel, and limited Spanish-speaking healthcare providers create intimidating and uncomfortable situations when trying to receive medical care.30 They also expressed this frustration around lack of verbal and written educational information. One participant said:
A lot of things that you read, which are not related to medications, the information is in English, Spanish, and other languages. But for medications, which are much more important than a blender or coffee pot, I would think it would be better like that.30
Parents of infants in the NICU must learn and assume care for the complex medical needs of their infant which may include a specialized feeding plan, medication administration, and/or supplemental oxygen needs in addition to normal infant care needs (eg, holding and diapering). Additionally, parents are expected to continue or initiate therapeutic activities as recommended by the physical, occupational, or speech therapist to optimize their infant’s development post discharge;31 therefore, we recommend that best practice for educating Spanish-speaking parents during the NICU stay and when preparing for discharge is to provide hands-on education at the infant’s bedside with a medical interpreter, supplemented by using translated written materials for review after the session.
The readability analysis from our study aligned with previous work by Villa Camacho et al, who found that online Spanish-language materials for breast cancer patients were more significantly more likely than English-language materials to meet AMA recommendations of a 6th grade reading level.28 As of 2018, 54% of Latino US residents had completed a high-school degree, as compared to more than 90% of the general US population.32 While the rate of high-school completion rate in the Latinx/ Hispanic population has increased significantly in the 25–29 year age group (88.5%), ensuring readability for a wide range of backgrounds and language exposure in this population is crucial, especially when considering that most verbal instruction may be completed through an interpreter in the medical setting.
Limitations
This study had various limitations. While the CRB members were all native Spanish-speaking mothers, none had experience birthing a preterm infant who required a NICU stay; therefore, the results are most generalizable to Latinx/ Hispanic mothers living in the Southeastern US. The familiarity of the NICU setting with two CRB members provided greater context to the particular challenges facing Spanish-speaking families in the health care setting. This study was intended for the purpose of outlining the process for preparing translated materials in clinical trials. Future studies are necessary to assess the effectiveness of these materials in Spanish-speaking families in the NICU.
Practice Implications
As Spanish-speaking and Latinx/ Hispanic populations in the United States continue to increase, the need for accessible, comprehensive, and relevant healthcare education materials remains critical. This study demonstrates that community review and readability analysis meaningfully improve the linguistic accuracy and cultural relevancy of translated materials, and thus the quality of patient care, for Spanish-speaking, Latinx/ Hispanic populations.
Conclusion
The multi-step, interdisciplinary Spanish translation and cultural adaptation approach used in this study produced patient education materials that were acceptable to CRB members representing Spanish-speaking families in the healthcare setting. These materials provide comprehensible information and are appropriately adapted to be congruent with Latinx/Hispanic cultures but will need additional assessment in Spanish-speaking families.
Data Sharing Statement
Data from review meetings are available on request from the authors.
Acknowledgments
The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Numbers UL1TR002489 and UM1TR004406. The primary study was funded by National Center for Advancing Translational Sciences, National Institutes of Health, under Grant KL2TR002490. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Matricardi S, Agostino R, Fedeli C, Montirosso R. Mothers are not fathers: differences between parents in the reduction of stress levels after a parental intervention in a NICU. Acta Paediatr. 2013;102(1):8–14. doi:10.1111/apa.12058
2. Ivashchuk A, Guillen U, Mackley A, Locke R, Sturtz W. Parental protective factors and stress in NICU mothers and fathers. J Perinatol. 2021;41(8):2000–2008. doi:10.1038/s41372-020-00908-4
3. Xie J, Zhu L, Zhu T, et al. Parental engagement and early interactions with preterm infants reduce risk of late postpartum depression. J Nerv Ment Dis. 2019;207(5):360–364. doi:10.1097/NMD.0000000000000971
4. Pineda R, Bender J, Hall B, Shabosky L, Annecca A, Smith J. Parent participation in the neonatal intensive care unit: predictors and relationships to neurobehavior and developmental outcomes. Early Hum Dev. 2018;117:32–38. doi:10.1016/j.earlhumdev.2017.12.008
5. White-Traut R, Wink T, Minehart T, Holditch-Davis D. Frequency of premature infant engagement and disengagement behaviors during two maternally administered interventions. Newborn Infant Nurs Rev. 2012;12(3):124–131. doi:10.1053/j.nainr.2012.06.005
6. Hofheimer JA, Smith LM, McGowan EC, et al. Psychosocial and medical adversity associated with neonatal neurobehavior in infants born before 30 weeks gestation. Pediatr Res. 2020;87(4):721–729. doi:10.1038/s41390-019-0607-1
7. Kadivar M, Seyedfatemi N, Mokhlesabadi Farahani T, Mehran A, Pridham KF. Effectiveness of an internet-based education on maternal satisfaction in NICUs. Patient Educ Couns. 2017;100(5):943–949. doi:10.1016/j.pec.2016.11.005
8. Shorey S, Ng YPM, Ng ED, et al. Effectiveness of a technology-based supportive educational parenting program on parental outcomes (part 1): randomized controlled trial. J Med Internet Res. 2019;21(2):e10816. doi:10.2196/10816
9. Anwar Siani S, Dol J, Campbell-Yeo M. Impact of parent-targeted eHealth on parent and infant health outcomes: a scoping review. J Perinat Neonatal Nurs. 2017;31(4):332–340. doi:10.1097/JPN.0000000000000265
10. Davis SH, Rosenberg J, Nguyen J, et al. Translating discharge instructions for limited English-proficient families: strategies and barriers. Hosp Pediatr. 2019;9(10):779–787. doi:10.1542/hpeds.2019-0055
11. Beasley LO, Silovsky JF, Espeleta HC, et al. A qualitative study of cultural congruency of legacy for childrenTM for Spanish-speaking mothers. Child Youth Serv Rev. 2017;79:299–308. doi:10.1016/j.childyouth.2017.06.022
12. Nitsos A, Estrada RD, Messias DKH. Tummy time for latinos with limited English proficiency: evaluating the feasibility of a cultural and linguistically adapted parent education intervention. J Pediatr Nurs. 2017;36:31–36. doi:10.1016/j.pedn.2017.04.004
13. Hall ML, Reidies JA. Measuring receptive ASL skills in novice signers and nonsigners. J Deaf Stud Deaf Educ. 2021;26(4):501–510. doi:10.1093/deafed/enab024
14. Fernández A, Pérez-Stable EJ. ¿Doctor, habla español? Increasing the supply and quality of language-concordant physicians for Spanish-speaking patients. J Gen Intern Med. 2015;30(10):1394–1396. doi:10.1007/s11606-015-3436-x
15. Witt RE, Colvin BN, Lenze SN, et al. Lived experiences of stress of black and Hispanic mothers during hospitalization of preterm infants in neonatal intensive care units. J Perinatol. 2022;42(2):195–201. doi:10.1038/s41372-021-01241-0
16. Holditch-Davis D, White-Traut RC, Levy JA, O’Shea TM, Geraldo V, David RJ. Maternally administered interventions for preterm infants in the NICU: effects on maternal psychological distress and mother-infant relationship. Infant Behav Dev. 2014;37(4):695–710. doi:10.1016/j.infbeh.2014.08.005
17. Khurana S, Kane AE, Brown SE, Tarver T, Dusing SC. Effect of neonatal therapy on the motor, cognitive, and behavioral development of infants born preterm: a systematic review. Dev Med Child Neurol. 2020;62(6):684–692. doi:10.1111/dmcn.14485
18. Dusing SC, Burnsed JC, Brown SE, et al. Efficacy of supporting play exploration and early development intervention in the first months of life for infants born very preterm: 3-arm randomized clinical trial protocol. Phys Ther. 2020;100(8):1343–1352. doi:10.1093/ptj/pzaa077
19. Waddington C, van Veenendaal NR, O’Brien K, Patel N. International steering committee for family integrated care. Family integrated care: supporting parents as primary caregivers in the neonatal intensive care unit. Pediatr Investig. 2021;5(2):148–154. doi:10.1002/ped4.12277
20. Dusing SC, Murray T, Stern M. Parent preferences for motor development education in the neonatal intensive care unit. Pediatr Phys Ther. 2008;20(4):363–368. doi:10.1097/PEP.0b013e31818add5d
21. North Carolina’s Hispanic community: 2021 snapshot | Carolina Demography. Available from: https://www.ncdemography.org/2021/10/18/north-carolinas-hispanic-community-2021-snapshot/#:~:text=Statewide%2C%2010.7%25%20of%20North%20Carolina’s,over%20the%20past%2030%20years.
22. Loomba L, Bonanno S, Arellano D, Crossen S, Glaser N. Disparities in insulin pump use among Spanish-speaking children with type 1 diabetes compared to their non-Hispanic white peers: mixed methods study. JMIR Diabetes. 2023;8:e45890. doi:10.2196/45890
23. McCarty DB, Dusing SC, Thorpe D, et al. A feasibility study of a physical and occupational therapy-led and parent-administered program to improve parent mental health and infant development. Phys Occup Ther Pediatr. 2023:1–20. doi:10.1080/01942638.2023.2271102
24. McCarty DB, Dusing SC, Gilbert A, LeBlond KD, Soucie M, O’Shea TM. Parent and therapist perceptions of the feasibility, acceptability, and benefits of a weekly therapist-led massage program for extremely preterm infants in neonatal intensive care. Children. 2023;10(9):1453. doi:10.3390/children10091453
25. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348(mar07 3):g1687. doi:10.1136/bmj.g1687
26. Miguéns-Vila R, Ledesma-Ludi Y, Rodríguez-Lozano F, Varela-Centelles P, Seoane-Romero JM, Castelo-Baz P. Disparities between English and Spanish in readability of online endodontic information for laypeople. J Am Dent Assoc. 2018;149(11):960–966. doi:10.1016/j.adaj.2018.07.003
27. Analizador de legibilidad de texto | legible. Available from: https://legible.es.
28. Villa Camacho JC, Pena MA, Flores EJ, et al. Addressing linguistic barriers to care: evaluation of breast cancer online patient educational materials for Spanish-speaking patients. J Am Coll Radiol. 2021;18(7):919–926. doi:10.1016/j.jacr.2021.02.001
29. Novin SA, Huh EH, Bange MG, Hui FK, Yi PH. Readability of Spanish-language patient education materials from radiologyInfo.org. J Am Coll Radiol. 2019;16(8):1108–1113. doi:10.1016/j.jacr.2018.12.036
30. Olenik NL, Gonzalvo JD, Snyder ME, Nash CL, Smith CT. Perceptions of Spanish-speaking clientele of patient care services in a community pharmacy. Res Social Adm Pharm. 2015;11(2):241–252. doi:10.1016/j.sapharm.2014.07.001
31. McCarty DB, Letzkus L, Attridge E, Dusing SC. Efficacy of therapist supported interventions from the neonatal intensive care unit to home: a meta-review of systematic reviews. Clin Perinatol. 2023;50(1):157–178. doi:10.1016/j.clp.2022.10.004
32. Census bureau releases new educational attainment data. Available from: https://www.census.gov/newsroom/press-releases/2022/educational-attainment.html#:~:text=The%20high%20school%20completion%20rate,10.5%25%20between%202011%20and%202021.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.