")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 15
Safety Aspects and Rational Use of Testosterone Undecanoate in the Treatment of Testosterone Deficiency: Clinical Insights
Authors Campbell K, Muthigi A, Ghomeshi A, Schuppe K, Sandler MD , Ramasamy R
Received 3 December 2022
Accepted for publication 16 March 2023
Published 31 March 2023 Volume 2023:15 Pages 73—84
DOI https://doi.org/10.2147/DHPS.S383130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rajender R Aparasu
Katherine Campbell,1 Akhil Muthigi,1 Armin Ghomeshi,2 Kyle Schuppe,3 Max D Sandler,4 Ranjith Ramasamy1
1Desai Sethi Urology Institute, University of Miami, Miami, Fl, 33136, USA; 2Herbert Wertheim College of Medicine, Florida International University, Miami, FL, 33199, USA; 3Washington State University Elson S. Floyd College of Medicine, Spokane, WA, 99202-2131, USA; 4University of Miami Miller of Medicine, Miami, Fl, USA
Correspondence: Ranjith Ramasamy, Desai Sethi Urology Institute, University of Miami, 1120 NW 14th St, Miami, Fl, 33136, USA, Tel +1 305-243-6090, Email [email protected]
Abstract: Testosterone deficiency is diagnosed by a serum total testosterone level below 300 ng/dL in combination with symptoms such as decreased energy and libido. These symptoms can be ameliorated by restoring serum testosterone to the physiologic range with testosterone therapy (TT). There are numerous forms of testosterone therapy, such as injectable, transdermal, nasal, and subcutaneous applications. There are also multiple formulations of injection, such as testosterone cypionate, testosterone enanthate, and testosterone undecanoate. Testosterone undecanoate (TU) is a long-acting ester formulation of testosterone that can be provided in an injectable or oral form. Oral testosterone undecanoate is marketed as Andriol, Jatenzo, Tlando, and Kyzatrex. Oral TU provides a convenient option for many patients, which may increase compliance with TT. Injectable testosterone undecanoate is marketed as Aveed and Nebido. Injectable TT remains the most cost-effective therapeutic option and is appropriate for most patients as an initial therapy. This review describes the pharmacokinetics of these testosterone undecanoate products and provides a guide for prescribers using these medications. While many forms of testosterone are appropriate for TT, a patient-centered discussion focused on goals of care should best guide physician prescription of these medications.
Keywords: testosterone, testosterone deficiency, testosterone therapy, hypogonadism in male
Introduction
Testosterone deficiency is recognized as the deficiency of testosterone (T) production by the testes. This deficiency results in a pathologically low systemic testosterone concentration, as well as the concentrations of its bioactive metabolites dihydrotestosterone (DHT) and estradiol (E2).1 Testosterone deficiency may affect up to 10% of men worldwide and 40% of men over the age of 45.2,3 Signs and symptoms of testosterone deficiency include characteristic physical changes such as regression of secondary sex characteristics, decreased lean muscle mass, and cognitive changes.3–5 The restoration of serum testosterone to physiologic, or eugonadal, levels has been shown to alleviate some of the symptoms of testosterone deficiency and provide significant improvement in quality of life.6 Multiple treatment options for testosterone deficiency exist, most commonly consisting of testosterone therapy (TT) with exogenous testosterone. Specifically, testosterone undecanoate (TU) is an 11-carbon long androgen ester derivative of testosterone that comes in an injectable or oral formulation. Recently, we have seen a rapid increase in the available FDA-approved TU forms of T. Herein, we present a focused review on testosterone undecanoate and its various formulations, as well as a practical guide for prescribers.
What is Testosterone Deficiency
As per American Urologic Association guidelines, testosterone deficiency is diagnosed with a serum testosterone level below 300 ng/dL on two separate occasions, with both conducted in the early morning in combination with symptoms.7 Recent studies suggest that 300 ng/dL may not be an appropriate cutoff for diagnosis of testosterone deficiency, and thus the diagnosis should be made by a trained physician based on serum biochemical (testosterone and sex hormone binding globulin) and clinical symptoms given the specific patient’s concomitant medical conditions.8 Regardless of primary or secondary etiology, testosterone deficiency is associated with characteristic physical changes, including gynecomastia, regression of secondary sex characteristics, and sexual dysfunction.5,7 Testosterone deficiency is also associated with musculoskeletal changes such as decreased bone mineral density and muscle mass.5 In addition, obese or overweight men have been shown to have higher rates of secondary testosterone deficiency than their normal weight counterparts.9 Psychological disturbances such as low motivation, poor concentration, and diminished energy are also frequent concerns of men with low T.5,10 Of the symptoms, diminished energy is the most reported hypogonadal symptom in men younger than 40 years old.11
Why Do We Treat Testosterone Deficiency?
Testosterone therapy can improve mood, libido, sexual function, as well as increase muscle mass and bone density, elevate hematocrit from anemic levels, and reduce body fat.7,12,13 Despite less conclusive evidence, many patients also report significant improvements in their energy level and cognitive function with TT.14 Currently, studies have shown conflicting results as to the reproducibility and mechanism of these improvements in energy and cognition, and, as such, the 2018 AUA Guidelines do not recognize improvements in energy and cognition as known benefits of TT.7
Treating patients with testosterone deficiency not only improves immediate symptoms, but also minimizes long-term sequelae of T deficiency itself. T deficiency is a known risk for cardiovascular disease, and is associated with hypertension, dyslipidemia, obesity, and diabetes.7,12 A 2018 meta-analysis of seven observational studies indicated that men with testosterone deficiency have an increased risk of myocardial infarction and pooled analysis of 12 studies demonstrated an increased risk of cerebrovascular accidents compared to men with normal T levels.7
Due to lack of long-term prospective studies, it is unclear whether testosterone therapy in deficient patients will ameliorate all these risks, and prescribers must balance the potential benefits against risks of TT, including the well-described effects of polycythemia, hypertension, and a decrease in sperm count. This is especially true in those at high risk of these adverse events and those with baseline poor health status. Patients with elevated hemoglobin/hematocrit (>50%) should delay testosterone therapy to avoid further polycythemia.15 Patients wishing to conceive must also be informed that 10% of men failed to recover sperm in their ejaculate until two years after stopping TT and some may become permanently oligospermic or azoospermic after treatment with TT.16 Ironically, despite the association between testosterone deficiency and cardiovascular risk, exogenous T may have cardiovascular risks of its own. The 2018 AUA Guidelines recognized this risk but, since then, a systematic review of over 50 trials showed that testosterone therapy was not associated with an increased risk of cardiovascular events.17 Due to this conflicting evidence, an individualized and patient-centered approach must include a discussion of these risks, alongside the benefits, before testosterone therapy is to be prescribed.
Common Treatment Options for Testosterone Deficiency
Many formulations and modalities of testosterone therapy exist. Exogenous testosterone modalities include injections, subcutaneous pellets, topical, and mucosal (nasal and buccal) applications (Table 1). Testosterone Undecanoate (TU) is a testosterone ester that has a long half-life compared to other esters.18 TU is also the only available formulation of oral TT (Table 2). Pharmacokinetic studies demonstrate that TU injections (Table 3) can return serum T levels to the eugonadal range 7–14 days after injection with a slow decline back to hypogonadal range by 10 weeks.19–21 Compared to testosterone enanthate and cypionate, TU is a longer acting form of testosterone and therefore requires less frequent administration to achieve clinical benefits.22 As a result, patients experience more stable T levels between injections and report significantly fewer fluctuations in mood and sexual function.23 Furthermore, a prospective study showed maximal TU effect on erectile function after 9 years of therapy, suggesting continued benefits over a long period of time.24
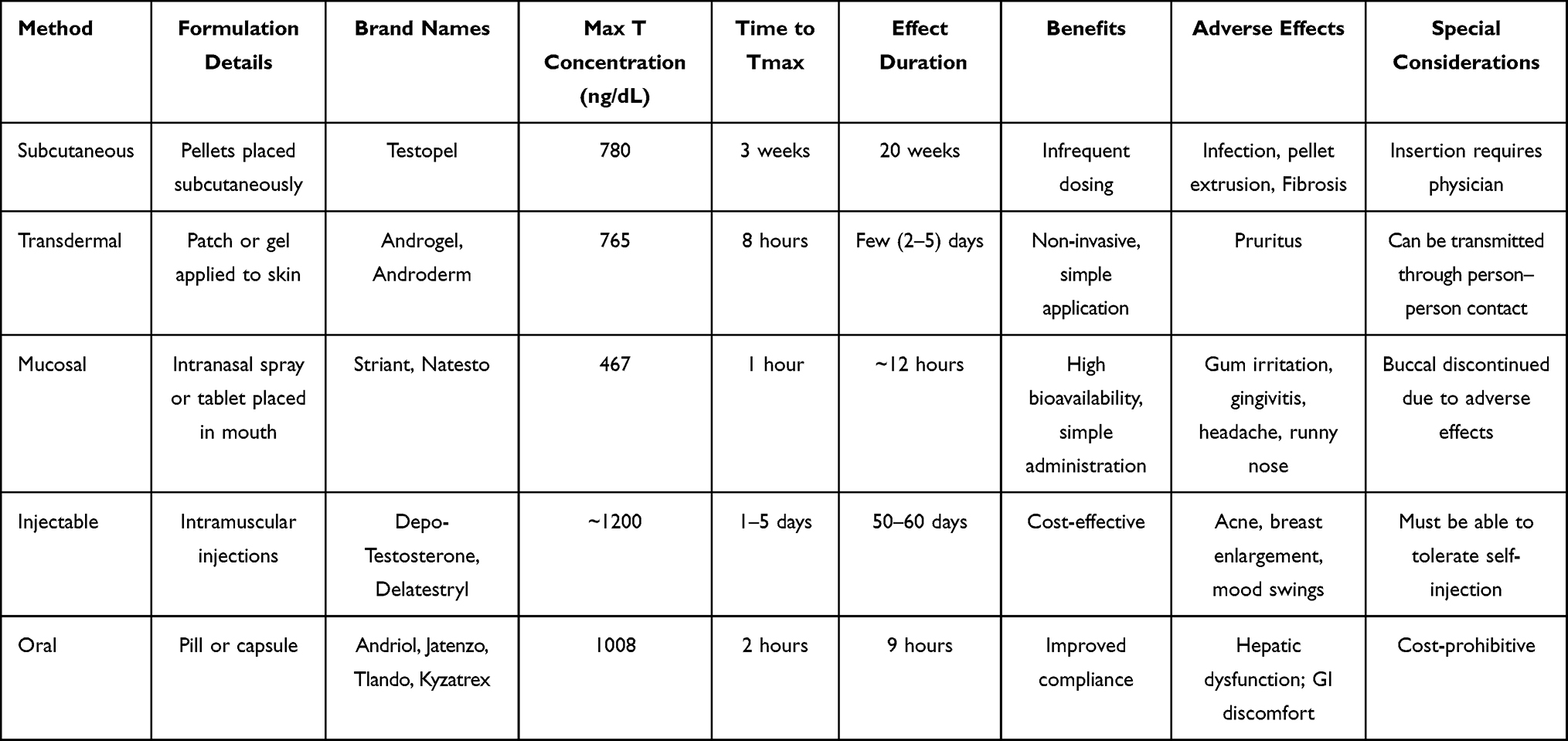 |
Table 1 Comparison of Modalities of Exogenous Testosterone |
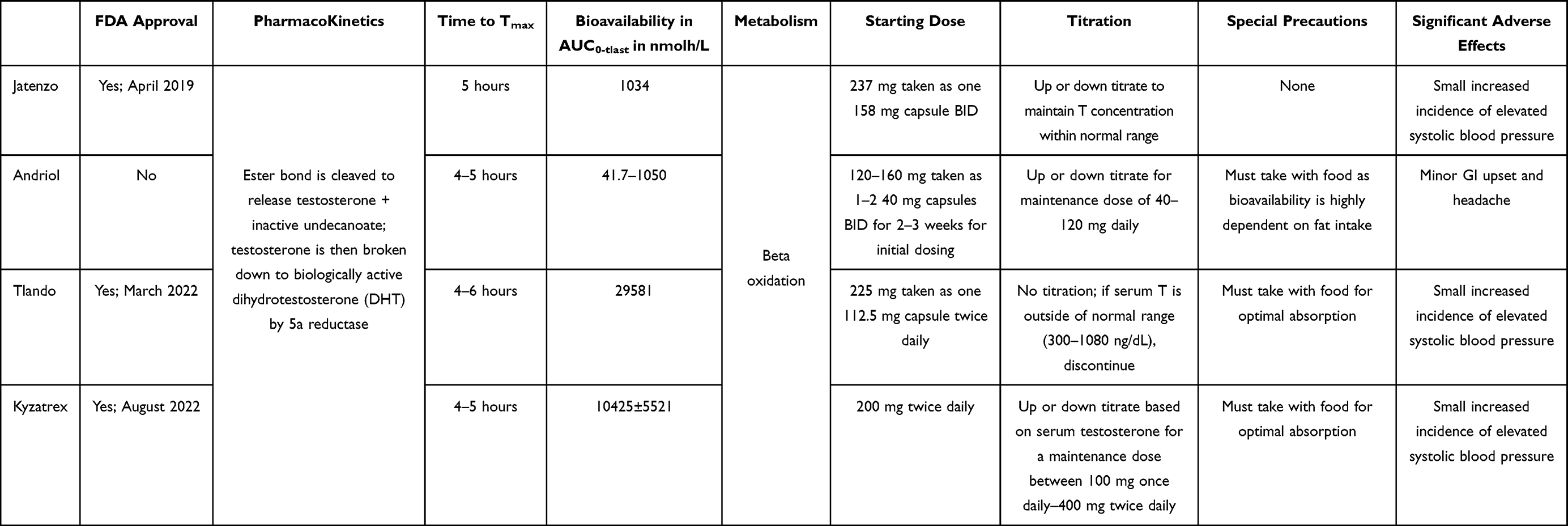 |
Table 2 Pharmacokinetic Properties of Oral TU Formulations |
 |
Table 3 Pharmacokinetic Properties of Injectable TU Formulations |
Oral Testosterone Undecanoate Formulations
Andriol
History and Development
In the 1970s, when it was found that the esterification of testosterone allowed for its intestinal lymphatic absorption via chylomicrons, oral TT became a possibility.25 The first oral TU formulation has been marketed for use outside the United State as Andriol, and is available in more than 80 countries around the world.26
Efficacy
Initial studies of Andriol showed a modest rise in plasma testosterone levels and a substantial rise in dihydrotestosterone when compared with placebo and non-esterified oral testosterone, which established efficacy of the formulation as early as 1975.27,28 Additional randomized controlled trials confirmed improvement in quality of life scores as compared with placebo.29,30 Few adverse events were found in the trials, and those that did were considered minor, such as headache and gastrointestinal upset.26,29
Dosing
Dosing of Andriol is simple, with 40 and 80 mg capsules available and a starting dose of 120–160 mg divided into a twice-daily administration.31
Adverse Effects
Despite initial positive results with Andriol, there were three major concerns with the drug. First, serum testosterone levels vary widely throughout the day and despite reaching the normal range within hours following ingestion, serum testosterone rapidly falls back to the hypogonadal range.27,28,32 As a result, the average serum testosterone level may not be within the physiologic range of normal for the majority of men using the drug.33 Second, the bioavailability of Andriol has been shown to be highly impacted by a patient’s dietary habits. Similar lipophilic formulations of drugs have been shown to have enhanced absorption and bioavailability with food.34 Taking the drug after an overnight fast led to serum concentrations of testosterone and its downstream metabolites below the limit of quantification.26 Additionally, meals with a higher fat content led to elevated serum concentrations of testosterone and its downstream metabolites.35 Though these studies used small sample sizes and heterogenous study techniques, these results suggest that unintentionally elevated serum testosterone levels may occur in patients who consume more fat. Overall, the necessity of combining Andriol with a meal may impact patient satisfaction and compliance with the drug, which make it a less ideal choice for TT. Lastly, Andriol undergoes metabolism in the liver, which decreases the bioavailability of the drug.36 As a consequence, higher doses may be required for the action of the drug and it is important to note that this formulation may not be a suitable choice for those with liver disease. Despite concern, data has not shown change in liver function while on Andriol,36 though caution should still be applied when prescribing this drug for those with comorbid liver conditions.
Jatenzo
History and Development
In 2019, the United States Food and Drug Administration approved the first oral testosterone ester prodrug – Jatenzo.37 As with all exogenous androgens, Jatenzo exerts its effect through suppressing FSH/LH and therefore endogenous testosterone function and production.38 Jatenzo was developed with a unique self-emulsifying drug delivery system (SEDDS) consisting of hydrophilic and lipophilic components that facilitate intestinal lymphatic absorption. In addition, this formulation allows absorption with a typical meal (15–45 g fat) as opposed to high fat-containing meals required for prior formulations.39 Jatenzo quickly leads to a serum testosterone concentration peak at two to four hours after ingestion, which slowly decreases to sub-physiologic levels near hour 9, thus requiring twice-daily dosing.36,40
Efficacy
Long-term and short-term phase III clinical trials confirmed efficacy of the oral TU formulation, as 84 and 87%, respectively, of patients enrolled in the trials became eugonadal during treatment as compared to topical testosterone gel.36,40 This oral formulation of TT also significantly improved subjective quality of life and metabolic parameters across varied diets, suggesting that Jatenzo absorption is not dependent on consumption of fats and therefore could be beneficial for diverse patient populations.36
Dosing
Dosing of Jatenzo is straightforward, with the usual adult dosage ranging from 158–396 mg.41 Based on the results of the clinical trials, the recommended starting dose is 237 mg taken as one 158 mg capsule twice daily.40 Dosing can be up or down titrated based on the individual’s testosterone concentration drawn 6 hours after morning dose.41
Adverse Effects
In initial trials of this oral TU formulation, adverse effects were consistent with other TT including polycythemia as well as a small, but statistically significant, increase in systolic blood pressure when compared to topical testosterone.36 Other side effects included transient and minor gastrointestinal concerns such as nausea, diarrhea, and burping, which may be associated with any oral medication. Importantly, and unlike other oral TU, Jatenzo partially avoids liver metabolism and has not been associated with liver toxicity. It has also not been shown to elevate markers of prostate cancer such as PSA and prostate volume specifically when compared with topical testosterone formulations. Overall, these adverse effects indicate the need for routine monitoring of hematocrit and blood pressure, as is consistent with AUA guidelines for any patient receiving TT.
Tlando
History and Development
In 2014, a clinical trial comparing a novel TU formulation against topical testosterone gel began, and in 2022 this product, marketed as Tlando, was approved for use in the United States. This capsule contains 112.5 mg of TU in a unique predigested triglyceride lipid formulation.42 Consistent with all other TU products, this lipid emulsification is designed to optimize absorption of TU through the intestinal lymphatic system. This formulation was hypothesized to avoid dose titration when used as twice daily TT.
Efficacy
Initial trials showed efficacy of Tlando in returning the majority of participants to a eugonadal testosterone range.42 Further, early results of a small, single-arm, open-label multicenter study (NCT03242590) presented at the Annual Meeting of the Endocrine Society showed that dose titration of Tlando did not alter pharmacokinetics.43 That same year, presented at the American Urologic Association, results of a year-long, open-label, active-controlled multicenter study confirmed that dose titration had an insignificant impact on pharmacokinetics.44 A final, open-label, multicenter study (NCT03242590) confirmed these results and suggested that adverse effects related to elevated serum testosterone, thus requiring dose titration, can be avoided with the new formulation.42
Dosing
Dosing of Tlando is straightforward, with a starting dose of 225 mg daily split into two equal doses of one, 112.5 mg pill, twice daily.45
Adverse Effects
Adverse effects of Tlando are similar to other forms of TT, including a minor increase in hematocrit and PSA.42 A unique adverse effect of the early trials, an elevated blood prolactin, was the most commonly reported side effect.42 Minor increases in systolic blood pressure along with elevated hematocrit were found to be clinically significant in a small, but significant number of patients.46 Further studies into long-term effects, both positive and negative, will be needed to elucidate side effects of this formulation.
Kyzatrex
History and Development
The most recently approved TT is Kyzatrex, which received FDA approval in August 2022.47 Unique to Kyzartrex is a TU formulation of phytosterols contained in a softgel capsule with the intent of maximizing lymphatic absorption and minimizing liver toxicity.48
Efficacy
A phase III open-label, active-controlled clinical trial (NCT03198728) showed efficacy of the formulation, with 88% (95% CI 82–93) of male patients with an average serum testosterone level in the eugonadal range, which led to FDA approval.49
Dosing
Dosing of Kyzatrex is more variable than Tlando, with 100 mg, 150 mg, and 200 mg softgel capsules available and a recommended starting dose of 200 mg orally twice daily with food, followed by titration up or down based on serum testosterone concentration 7 days after starting treatment.49
Adverse Effects
The initial study was extended (NCT04467697) to further assess blood pressure effects of the formulation. The results of this safety study showed small but significant increases in systolic blood pressure, especially in men already taking antihypertensive therapy and those with type 2 diabetes, which follows trends previously reported with TT.50 Importantly, the clinical relevance of these small increases in systolic blood pressure is unclear, and requires further long-term studies. Other adverse effects of Kyzatrex include rare instances of headache, GI upset, elevated hemoglobin and PSA, anxiety, and peripheral edema.49
Patient Selection for Oral Testosterone Undecanoate
American Urologic Association guidelines do not specify which modality of testosterone therapy is most appropriate, therefore physicians should take a patient-centered approach to the prescription of TT. Oral formulations provide a convenient and easy to use option for patients with T deficiency. Though these drugs are newer, studies have shown that patients with chronic conditions impacting mobility such as rheumatoid arthritis and multiple sclerosis prefer oral medications and demonstrate improved compliance with oral T when compared to other forms of TT.51,52 Clearly, patients with dysphagia or other impediments to use of an oral medication are not good candidates for oral TT. Additionally, patients who cannot take oral medications twice per day are poor candidates for treatment with Jatenzo, Tlando, or Kyzatrex.
Injectable Testosterone Undecanoate Formulations
As early as 1995, preclinical, animal studies were performed to investigate the potential role of TU as an alternative injectable form of TT.53 Subsequent pharmokinetic studies in humans showed that mean serum T levels reached or exceeded the eugonadal range within the first week after injection and slowly returned to the patient’s hypogonadal baseline over the following 8 weeks, accompanied by improvement in quality of life scores.54 This is likely due to the slow metabolism of the saturated aliphatic fatty acid undecanoic acid.20,55 Unlike TE and TC, which require injection every 2 weeks, TU showed a favorable pharmokinetic profile and allowed a longer duration between injections, thus decreasing yearly injections from 26–52 to only 5–10 and increasing patient satisfaction.
Unique to the intramuscular (IM) injection of testosterone esters in an oil medium, is a concerning but non-life-threatening adverse effect pulmonary oil microembolism (POME). In contrast to a life-threatening venous thromboembolism, POME is defined by the acute onset of a non-productive cough sometimes accompanied by a sensation of flushing, faintness, or anxiety which resolves in minutes after the injection.56 These events are rare but did lead to a black box warning on the US formulation of the drug. The mechanism for these events is unclear and may be related to improper injection technique, therefore patients require monitoring after each injection.57
Aveed
History and Development
In 2014, the United States FDA approved the first injectable TU formulation, marketed as Aveed. An initial pharmacokinetic and safety trial established efficacy of the formulation with minimal side effects, suggesting that it would be an appropriate alternative to transdermal TT, and the drug received approval a few years later.19 Further clinical studies after FDA approval suggested patient satisfaction to complement the pharmacologic results.
Efficacy
The initial, multicenter, open-label clinical trial investigated the 750 mg TU in 3 mg castor oil (250 mg/mL) formulation. This study showed that serum total testosterone reached eugonadal range within the first week after injection, with a peak around 7 days, and then slowly decreased to low eugonadal or hypogonadal range in the following 10 weeks, with an average serum testosterone concentration of 890.6.19 Further, the majority of patients experienced symptomatic improvement, with one-third experiencing return of hypogonadal symptoms between injections, though a not insubstantial proportion (20.4%) discontinued treatment due to dissatisfaction.58 Some of these men who experienced return of symptoms received a TC injection for symptom relief.58
Dosing
Since Aveed is an IM injection, dosage titration is not performed. Rather, 3 mL of solution (750 mg) is injected, followed by an identical injection after 4 weeks, at which point the same dose can be injected every 10 weeks.59 Similar to most IM injections, the patient must prepare the drug for injection by drawing the appropriate amount into the syringe, therefore it may not be appropriate in someone who cannot perform this action.
Adverse Effects
The initial clinical trial of the formulation marketed as Aveed reported mild adverse effects. Most commonly, patients experienced a mild cough or adverse effects expected with injectable medications such as injection site soreness.19 Mild elevations in PSA and serum hemoglobin concentration were noted, but no prostate cancer was diagnosed during the trial.19 The results from Morgentaler et al were corroborated by Krakowsky et al, who showed few instances of cough and injection site bruising. Their study also confirmed a mild elevation in hematocrit and PSA in participants, but experienced no new diagnoses or progression of prostate cancer or cardiovascular incidents.58 In a post-marketing analysis of Aveed, the rate of POME was <0.1%.
Nebido
History and Development
Outside of the United States, Nebido has been available as a high dose TU injection since 2003. Today, Nebido is available in 80 countries worldwide, including in Europe, Australia, and Canada. In an initial pharmacokinetic study, serum testosterone concentration reached a peak at or above eugonadal range by two weeks after injection and slowly decreased during the following 12 weeks for both subcutaneous and intramuscular injections of the formulation. However, IM injections are generally preferred by patients due to lower pain and thus it is marketed as an IM injection.60
Efficacy
In an open-label, randomized, prospective trial, when compared with testosterone enanthate injections, participants receiving TU maintained a significantly higher serum testosterone level within the normal range.61 After an initial loading dose, most patients remain in the physiologic range and only need an injection every 12 weeks, therefore allowing them to receive 4 injections each year. Though individualization is beneficial, and men may receive injections every 10–14 weeks, serum trough levels at the time of injection are generally still found in the low normal range, which suggests adequate length of coverage.62 Long-term clinical studies have shown that testosterone concentrations are maintained within the normal range, which is accompanied by subjective improvement in symptoms.24,61,63 Importantly, men using Nebido do not report significant fluctuations in their symptoms, especially at the end of the dosing interval, as has been reported with TC, TE, and Aveed.24
Dosing
Two loading doses of 1000 mg TU separated by 6 weeks can then be followed by injections every 12 weeks, with sufficient maintenance of the serum testosterone level within the physiologic range.
Adverse Effects
In none of the initial or long-term clinical studies did a participant experience a significant adverse effect leading to them leaving the study. Mild side effects can be seen, but few local adverse reactions were seen. As is consistent with other TT, elevated plasma hemoglobin and hematocrit are seen during treatment but, in long-term studies, these values did not reach the upper limit of normal.61,63 PSA was also elevated but no new diagnoses of prostate cancer or progression of the disease were seen.24,61,63 It is hypothesized that the excellent safety profile of Nebido is secondary to the continuous normalization of plasma testosterone level.
Patient Selection for Injectable Testosterone Undecanoate
Intramuscular injections of testosterone have been the most commonly prescribed form of TT since their development in the 1930s.64 IM formulations of TT remain the most cost-effective and most frequently covered by insurance, making them an ideal option for those wishing for cost-effective treatment. IM injections of T often require dose optimization based on body habitus and individual metabolism; therefore, dosing may vary and should be guided by an individual’s serologic and symptomatic response. Though IM injections are commonly used, and generally safe, this formulation may not be a suitable option for patients who are averse to self-injecting the medication. Additionally, those with physical or cognitive impairment that prevents them from drawing up testosterone from a small vial and then injecting it may not be candidates for IM TT.
Conclusions
Low testosterone is an ongoing problem for men and can cause detrimental physiological and psychological effects. Various pharmacological interventions exist, and TU is currently a promising treatment modality. TU has increased compliance due to the option of oral intake and a pharmacokinetic profile that allows for far less frequent dosing compared to other exogenous testosterone compounds. While oral formulations provide a promising new option to expand access to TT, potential liver toxicity and fat consumption necessary for absorption of these drugs must be taken into consideration before prescription. Traditional injectable formulations of TU continue to provide a cost-effective strategy for TT. The decision to start treatment with oral or injectable TU must be the result of an individualized conversation between a patient and their physician. Overall, clinicians may offer TU as part of a personalized treatment regimen based on patient goals and preferences.
Disclosure
Dr Ranjith Ramasamy reports grants from NIH, grants from ACS, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Trabado S, Maione L, Salenave S, et al. Estradiol levels in men with congenital hypogonadotropic hypogonadism and the effects of different modalities of hormonal treatment. Fertil Steril. 2011;95(7):2324–2329.e3. doi:10.1016/j.fertnstert.2011.03.091
2. Anaissie J, DeLay KJ, Wang W, Hatzichristodoulou G, Hellstrom WJ. Testosterone deficiency in adults and corresponding treatment patterns across the globe. Transl Androl Urol. 2017;6(2):183–191. doi:10.21037/tau.2016.11.16
3. Cohen J, Nassau DE, Patel P, Ramasamy R. Low testosterone in adolescents & young adults. Front Endocrinol Lausanne. 2019;10:916. doi:10.3389/fendo.2019.00916
4. Vartolomei MD, Kimura S, Vartolomei L, Shariat SF. Systematic review of the impact of testosterone replacement therapy on depression in patients with late-onset testosterone deficiency. Eur Urol Focus. 2020;6(1):170–177. doi:10.1016/j.euf.2018.07.006
5. Kumar P, Kumar N, Thakur DS, Patidar A. Male hypogonadism: symptoms and treatment. J Adv Pharm Technol Res. 2010;1(3):297–301. doi:10.4103/0110-5558.72420
6. Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of testosterone treatment in older men. N Engl J Med. 2016;374(7):611–624. doi:10.1056/NEJMoa1506119
7. Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200(2):423–432. doi:10.1016/j.juro.2018.03.115
8. Rochira V. Hypogonadism in systemic diseases. In: Vitti P, Hegedus L, editors. Thyroid Diseases. Endocrinology. Springer International Publishing; 2017:1–51. doi:10.1007/978-3-319-29456-8_28-1
9. Gurayah AA, Mason MM, Masterson JM, Kargi AY, Ramasamy R. U-shaped association between prevalence of secondary hypogonadism and body mass index: a retrospective analysis of men with testosterone deficiency. Int J Impot Res. 2022. doi:10.1038/s41443-022-00533-z
10. Dhingra OP, Bernstein J, Barnes SD, VanLaanen H, Wadlington N, Chang J. Novel oral testosterone formulation improves male well being without compromising international prostate symptom scores. In: © The Author(s) 2021. Vol. 5. Published by Oxford University Press on behalf of the Endocrine Society.; 2021:A760. doi:10.1210/jendso/bvab048.1546
11. Scovell JM, Ramasamy R, Wilken N, Kovac JR, Lipshultz LI. Hypogonadal symptoms in young men are associated with a serum total testosterone threshold of 400 ng/dL. BJU Int. 2015;116(1):142–146. doi:10.1111/bju.12970
12. Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pr. 2010;64(6):682–696. doi:10.1111/j.1742-1241.2010.02355.x
13. Valancy D, Blachman-Braun R, Kuchakulla M, Nackeeran S, Ramasamy R. Association between low testosterone and anaemia: analysis of the National Health and Nutrition Examination Survey. Andrologia. 2021;53(11):e14210. doi:10.1111/and.14210
14. Straftis AA, Gray PB. Sex, energy, well-being and low testosterone: an exploratory survey of U.S. men’s experiences on prescription testosterone. Int J Env Res Public Health. 2019;16(18):3261. doi:10.3390/ijerph16183261
15. Wheeler KM, Smith RP, Kumar RA, Setia S, Costabile RA, Kavoussi PK. A comparison of secondary polycythemia in hypogonadal men treated with clomiphene citrate versus testosterone replacement: a multi-institutional study. J Urol. 2017;197(4):1127–1131. doi:10.1016/j.juro.2016.10.068
16. Liu PY, Swerdloff RS, Anawalt BD, et al. Determinants of the rate and extent of spermatogenic suppression during hormonal male contraception: an integrated analysis. J Clin Endocrinol Metab. 2008;93(5):1774–1783. doi:10.1210/jc.2007-2768
17. Hudson J, Cruickshank M, Quinton R, et al. Adverse cardiovascular events and mortality in men during testosterone treatment: an individual patient and aggregate data meta-analysis. Lancet Healthy Longev. 2022;3(6):e381–e393. doi:10.1016/S2666-7568(22)00096-4
18. Buvat J, Maggi M, Guay A, Torres LO. Testosterone deficiency in men: systematic review and standard operating procedures for diagnosis and treatment. J Sex Med. 2013;10(1):245–284. doi:10.1111/j.1743-6109.2012.02783.x
19. Morgentaler A, Dobs AS, Kaufman JM, et al. Long acting testosterone undecanoate therapy in men with hypogonadism: results of a pharmacokinetic clinical study. J Urol. 2008;180(6):2307–2313. doi:10.1016/j.juro.2008.08.126
20. von Eckardstein S, Nieschlag E. Treatment of male hypogonadism with testosterone undecanoate injected at extended intervals of 12 weeks: a Phase II study. J Androl. 2002;23(3):419–425. doi:10.1530/eje.0.1400414
21. Corona G, Vignozzi L, Sforza A, Maggi M. Risks and benefits of late onset hypogonadism treatment: an expert opinion. World J Mens Health. 2013;31(2):103–125. doi:10.5534/wjmh.2013.31.2.103
22. Shoskes JJ, Wilson MK, Spinner ML. Pharmacology of testosterone replacement therapy preparations. Transl Androl Urol. 2016;5(6):834–843. doi:10.21037/tau.2016.07.10
23. Jockenhövel F, Minnemann T, Schubert M, et al. Comparison of long-acting testosterone undecanoate formulation versus testosterone enanthate on sexual function and mood in hypogonadal men. Eur J Endocrinol. 2009;160(5):815–819. doi:10.1530/EJE-08-0830
24. Saad F, Kamischke A, Yassin A, et al. More than eight years’ hands-on experience with the novel long-acting parenteral testosterone undecanoate. Asian J Androl. 2007;9(3):291–297. doi:10.1111/j.1745-7262.2007.00275.x
25. Horst HJ, Höltje WJ, Dennis M, Coert A, Geelen J, Voigt KD. Lymphatic absorption and metabolism of orally administered testosterone undecanoate in man. Klin Wochenschr. 1976;54(18):875–879. doi:10.1007/BF01483589
26. Bagchus WM, Hust R, Maris F, Schnabel PG, Houwing NS. Important effect of food on the bioavailability of oral testosterone undecanoate. Pharmacotherapy. 2003;23(3):319–325. doi:10.1592/phco.23.3.319.32104
27. Skakkebaek NE, Bancroft J, Davidson DW, Warner P. Androgen replacement with oral testosterone undecanoate in hypogonadal men: a double blind controlled study. Clin Endocrinol. 1981;14(1):49–61. doi:10.1111/j.1365-2265.1981.tb00364.x
28. Nieschlag E, Mauss J, Coert A, Kićović P. Plasma androgen levels in men after oral administration of testosterone or testosterone undecanoate. Acta Endocrinol. 1975;79(2):366–374. doi:10.1530/acta.0.0790366
29. Park NC, Yan BQ, Chung JM, Lee KM. Oral testosterone undecanoate (Andriol) supplement therapy improves the quality of life for men with testosterone deficiency. Aging Male. 2003;6(2):86–93. doi:10.1080/tam.6.2.86.93
30. Emmelot-Vonk MH, Verhaar HJJ, Nakhai Pour HR, et al. Effect of testosterone supplementation on functional mobility, cognition, and other parameters in older men: a randomized controlled trial. JAMA. 2008;299(1):39–52. doi:10.1001/jama.2007.51
31. Jungwirth A, Plas E, Geurts P. Clinical experience with Andriol Testocaps--the first Austrian surveillance study on the treatment of late-onset hypogonadism. Aging Male. 2007;10(4):183–187. doi:10.1080/13685530701495088
32. Wittert GA, Chapman IM, Haren MT, Mackintosh S, Coates P, Morley JE. Oral testosterone supplementation increases muscle and decreases fat mass in healthy elderly males with low-normal gonadal status. J Gerontol a Biol Sci Med Sci. 2003;58(7):618–625. doi:10.1093/gerona/58.7.m618
33. Yin AY, Htun M, Swerdloff RS, et al. Reexamination of pharmacokinetics of oral testosterone undecanoate in hypogonadal men with a new self-emulsifying formulation. J Androl. 2012;33(2):190–201. doi:10.2164/jandrol.111.013169
34. Frey H, Aakvaag A, Saanum D, Falch J. Bioavailability of oral testosterone in males. Eur J Clin Pharmacol. 1979;16(5):345–349. doi:10.1007/BF00605634
35. Schnabel PG, Bagchus W, Lass H, Thomsen T, Geurts TBP. The effect of food composition on serum testosterone levels after oral administration of Andriol Testocaps. Clin Endocrinol (Oxf). 2007;66(4):579–585. doi:10.1111/j.1365-2265.2007.02781.x
36. Swerdloff RS, Wang C, White WB, et al. A new oral testosterone undecanoate formulation restores testosterone to normal concentrations in hypogonadal men. J Clin Endocrinol Metab. 2020;105(8):dgaa238. doi:10.1210/clinem/dgaa238
37. Meyer L. FDA approves new oral testosterone capsule for treatment of men with certain forms of hypogonadism. FDA NEWS RELEASE; 2019. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-oral-testosterone-capsule-treatment-men-certain-forms-hypogonadism.
38. Khodamoradi K, Khosravizadeh Z, Parmar M, Kuchakulla M, Ramasamy R, Arora H. Exogenous testosterone replacement therapy versus raising endogenous testosterone levels: current and future prospects. FS Rev. 2021;2(1):32–42. doi:10.1016/j.xfnr.2020.11.001
39. Patel M, Muthigi A, Ramasamy R. JATENZO®: challenges in the development of oral testosterone. Int J Impot Res. 2022;34(7):721–724. doi:10.1038/s41443-021-00461-4
40. Swerdloff RS, Dudley RE. A new oral testosterone undecanoate therapy comes of age for the treatment of hypogonadal men. Ther Adv Urol. 2020;12:1756287220937232. doi:10.1177/1756287220937232
41. Clarus Therapeutics, Inc. JATENZO- testosterone undecanoate capsule, liquid filled. Package insert; 2021. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/206089s000lbl.pdf.
42. DelConte A, Papangkorn K, Kim K, et al. A new oral testosterone (TLANDO) treatment regimen without dose titration requirement for male hypogonadism. Andrology. 2022;10(4):669–676. doi:10.1111/andr.13153
43. DelConte A, Patel MV, Papangkorn K, et al. SAT-052 A Novel Oral Testosterone Therapy (TLANDO) safely restores testosterone to eugonadal levels with fixed dose treatment. J Endocr Soc. 2020;4(Supplement_1):SAT–052. doi:10.1210/jendso/bvaa046.684
44. Anthony D, Nachiappan C, Kongnara P, et al. MP45-15 a novel oral testosterone therapy restores testosterone to eugonadal levels without dose titration. J Urol. 2020;203(Supplement4):e670–e670. doi:10.1097/JU.0000000000000900.015
45. Antares Pharma, Inc. TLANDO- testosterone undecanoate capsule, liquid filled. Package insert; 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/208088s000lbl.pdf.
46. White WB, Dobs A, Carson C, et al. Effects of a novel oral testosterone undecanoate on ambulatory blood pressure in hypogonadal men. J Cardiovasc Pharmacol Ther. 2021;26(6):630–637. doi:10.1177/10742484211027394
47. Globe Newswire. CORRECTION -- Marius pharmaceuticals receives FDA approval of KYZATREXTM, an oral testosterone replacement therapy; 2022. Available from: https://www.globenewswire.com/en/news-release/2022/09/21/2520385/0/en/CORRECTION-Marius-Pharmaceuticals-Receives-FDA-Approval-of-KYZATREX-an-Oral-Testosterone-Replacement-Therapy.html.
48. Marius Pharma. Marius pharmaceuticals completes efficacy Phase 3 study; 2018. Available from: https://www.mariuspharma.com/.
49. Marius Pharmaceuticals. KYZATREX- testosterone undecanoate capsule, liquid filled. Package insert; 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/213953s000lbl.pdf.
50. White WB, Bernstein JS, Rittmaster R, Dhingra O. Effects of the oral testosterone undecanoate KyzatrexTM on ambulatory blood pressure in hypogonadal men. J Clin Hypertens Greenwich Conn. 2021;23(7):1420–1430. doi:10.1111/jch.14297
51. Edel Y, Sagy I, Pokroy-Shapira E, et al. A cross-sectional survey on the preference of patients with rheumatoid arthritis for route of administration of disease-modifying anti-rheumatic drugs: oral target-specific versus parenteral biologic. Isr Med Assoc J. 2020;22(3):154–159.
52. Sánchez Martínez I, Cerdán Sánchez M, López Román J, et al. Possible influence of the route of treatment administration on treatment adherence in patients with multiple sclerosis. Clin Ther. 2020;42(5):e87–e99. doi:10.1016/j.clinthera.2020.03.005
53. Partsch CJ, Weinbauer GF, Fang R, Nieschlag E. Injectable testosterone undecanoate has more favourable pharmacokinetics and pharmacodynamics than testosterone enanthate. Eur J Endocrinol. 1995;132(4):514–519. doi:10.1530/eje.0.1320514
54. Zhang GY, Gu YQ, Wang XH, Cui YG, Bremner WJ. A pharmacokinetic study of injectable testosterone undecanoate in hypogonadal men. J Androl. 1998;19(6):761–768.
55. Behre HM, Abshagen K, Oettel M, Hübler D, Nieschlag E Intramuscular injection of testosterone undecanoate for the treatment of male hypogonadism: phase I studies. European Journal of Endocrinology. 1999 May;140(5):414–419. doi: 10.1530/eje.0.1400414.
56. Middleton T, Turner L, Fennell C, et al. Complications of injectable testosterone undecanoate in routine clinical practice. Eur J Endocrinol. 2015;172(5):511–517. doi:10.1530/EJE-14-0891
57. Adam JA, Pastuszak AW, Christensen MB, et al. Occurrence of pulmonary oil microembolism (POME) with intramuscular testosterone undecanoate injection: literature review. Int J Impot Res. 2022. doi:10.1038/s41443-022-00585-1
58. Krakowsky Y, Conners W, Davidson E, Rawji A, Morgentaler A. Initial clinical experience with testosterone undecanoate therapy (AVEED) in men with testosterone deficiency in the United States. Urology. 2017;109:27–31. doi:10.1016/j.urology.2017.07.007
59. Endo Pharmaceuticals. AVEED (testosterone undecanoate) injection, for intramuscular use. Package insert; 2014. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022219s000lbl.pdf.
60. Turner L, Ly LP, Desai R, et al. Pharmacokinetics and acceptability of subcutaneous injection of testosterone undecanoate. J Endocr Soc. 2019;3(8):1531–1540. doi:10.1210/js.2019-00134
61. Schubert M, Minnemann T, Hübler D, et al. Intramuscular testosterone undecanoate: pharmacokinetic aspects of a novel testosterone formulation during long-term treatment of men with hypogonadism. J Clin Endocrinol Metab. 2004;89(11):5429–5434. doi:10.1210/jc.2004-0897
62. Yassin AA, Saad F. Treatment of sexual dysfunction of hypogonadal patients with long-acting testosterone undecanoate (Nebido). World J Urol. 2006;24(6):639–644. doi:10.1007/s00345-006-0120-0
63. Moon DG, Park MG, Lee SW, et al. The efficacy and safety of testosterone undecanoate (Nebido(®)) in testosterone deficiency syndrome in Korean: a multicenter prospective study. J Sex Med. 2010;7(6):2253–2260. doi:10.1111/j.1743-6109.2010.01765.x
64. Rostom M, Ramasamy R, Kohn TP. History of testosterone therapy through the ages. Int J Impot Res. 2022;34(7):623–625. doi:10.1038/s41443-021-00493-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.