")
Back to Journals » Clinical Ophthalmology » Volume 16
Safety and Efficacy of Cataract Surgery Under a Local Infection Control Protocol Before and During a COVID-19 Wave in Thailand for Healthcare Workers and Patients: A Prospective Cohort from a Secondary Center
Authors Rujkorakarn P , Patamatamkul S
Received 14 March 2022
Accepted for publication 25 May 2022
Published 3 June 2022 Volume 2022:16 Pages 1773—1781
DOI https://doi.org/10.2147/OPTH.S366353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ploysai Rujkorakarn,1 Samadhi Patamatamkul2
1Department of Ophthalmology, Suddhavej Hospital, Faculty of Medicine, Mahasarakham University, Mahasarakham, Thailand; 2Department of Internal Medicine, Suddhavej Hospital, Faculty of Medicine, Mahasarakham University, Mahasarakham, Thailand
Correspondence: Ploysai Rujkorakarn, Department of Ophthalmology, Suddhavej Hospital, Faculty of Medicine, Mahasarakham University, 77/99 Talat, Muang, Mahasarakham, 44000, Thailand, Tel +66-4-3021021, Fax +66-4-3722991, Email [email protected]
Purpose: To assess the effectiveness of a local infection control protocol for cataract surgery (CS) during the coronavirus disease (COVID-19) pandemic and determine the trend of CSs and visual outcomes during this period, as compared to the pre-COVID-19 pandemic period.
Methods: This study was conducted at Suddhavej Hospital, Mahasarakham University, Mahasarakham, Thailand, between July 1, 2020, and March 31, 2021. In this two-phase study, we used only a COVID-19-screening questionnaire during the first phase and preoperative nasopharyngeal swab severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing for real-time reverse transcriptase-polymerase chain reaction in the second phase, during Thailand’s second COVID-19 wave. Nasopharyngeal swab SARS-CoV-2 nucleic acid testing, SARS-CoV-2 IgG/IgM, or anti-SARS-CoV-2 spike antibody seroconversion was used to detect COVID-19 infection among healthcare workers. We also compared cataract surgical volume and postoperative visual acuity of CS patients between the pre-COVID-19 period and during the COVID-19 pandemic period.
Results: A total of 947 patients underwent CS. Thirty-two healthcare workers and 275 patients tested negative for SARS-CoV-2 in the second study phase. CSs increased on average by 50.09% month-to-month when the surgery was resumed. The mean postoperative logMAR best-corrected visual acuity was significantly better in the COVID-19 pandemic period than in the pre-pandemic period (difference, 0.1 [95% CI: 0.00– 0.12], p < 0.0001).
Conclusion: CS could be safely performed under an infection control protocol during the COVID-19 pandemic. The cataract surgical volume, with favorable visual outcomes, has an increasing trend after resuming elective surgeries.
Keywords: cataract surgery, cataract surgery trend, COVID-19, pre-operative SARS-CoV-2 screening, visual outcome
Introduction
Approximately 28 million surgeries were postponed globally during the first wave of coronavirus disease (COVID-19) in April 2020, of which more than 80% were elective.1 Global eye surgeries, including cataract surgery, declined by 90% in the US, Europe, and India during the first COVID-19 wave.2–4 Cataract surgery, a common elective surgery in ophthalmology units, including those in Thailand, was also markedly affected.5 The number of cataract surgeries performed in Thailand decreased significantly during the first COVID-19 wave, from a pre-pandemic average of 12,806 cases in January to March 2020 to 2,425 in April 2020 during lockdown (Figure 1).6,7 Consequently, several patients with disabling cataracts were placed on a waiting list. Delaying cataract surgery in patients with disabling visual impairment can cause dementia, depression, falls, and fracture, further reducing quality of life and visual outcomes.8–11 However, resuming cataract surgery safely for both patients and healthcare workers (HCWs) immediately after the lockdown posed a major challenge to Thailand’s healthcare system.
 |
Figure 1 Trends in the volume of cataract surgeries performed according to the Thai national data before and during the COVID-19 pandemic. Large arrow: lockdown phase. Small arrow: after lockdown was lifted. Chevron: start of the second wave. |
During the first COVID-19 wave, all elective surgeries were postponed in Thailand due to the national lockdown, which was announced in April 2020. However, many elective cataract surgeries were performed in Thailand once lockdown was lifted. The number of cataract surgeries slowly increased to 5,658 and 10,254 cases in May and June 2020, respectively (Figure 1).6,7 However, these numbers remained lower than the pre-pandemic values, and many patients were on waiting lists. The delay in cataract surgery after the first COVID-19 wave was similar to that in India, where the number of surgeries gradually increased after the lockdown.4 As most patients with disabling visual impairment were willing to undergo surgery during the pandemic, and as the pandemic is not yet under control, it remains necessary to employ effective protocols to prevent virus transmission during cataract surgery.12
Data regarding an effective protocol for screening for and preventing COVID-19 transmission in hospitals were lacking after the first COVID-19 wave. In Turkey, 10.6% of patients who underwent cataract surgery between November and December 2020 tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by polymerase chain reaction (PCR).13 Additionally, studies from India recommended universal preoperative SARS-CoV-2 testing in patients who underwent cataract surgery to reduce the risk of transmission to HCWs and reported that perioperative SARS-CoV-2 infection carried a higher risk of postoperative morbidity and mortality in patients.14,15 The early guidelines from the Department of Medical Services of Thailand in May 2020 recommended only questionnaire screening for possible SARS-CoV-2 exposure and COVID-19 symptoms among patients who underwent cataract surgery but did not mention the supporting evidence.16 The Infectious Disease Society of America (IDSA) recommended a nucleic acid test preoperatively in non-aerosol-generating procedures (AGPs) in the context of a high COVID-19 prevalence rate.17
Given the uncertainty of these recommendations, we prospectively determined the real-life effectiveness of a preoperative protocol to screen for and prevent COVID-19 transmission to HCWs involved in cataract surgery. We also assessed the trends in patients who underwent cataract surgery and the visual outcomes of such surgery during the COVID-19 pandemic, as compared to the pre-pandemic period, at our center.
Materials and Methods
Study Design and Setting
This prospective study was conducted at a secondary care hospital, Suddhavej Hospital, Mahasarakham University, Mahasarakham, Thailand, between July 1, 2020, and March 31, 2021. The observation period ended on March 31, 2021, because of a planned mass COVID-19 vaccination program for all Mahasarakham’s HCWs, commencing in mid-April 2021, which would complicate the interpretation of seroconversion.
The study was divided into two phases. The first phase occurred immediately after the first COVID-19 wave in Thailand ended, during a period with a low COVID-19 incidence rate (July 1, 2020 to December 31, 2020), while the second phase occurred during the second COVID-19 wave in Thailand (January 1, 2021 to March 31, 2021). At the start of the first phase, the start of the second phase, and the end of the study, there were 3,173, 6,884, and 28,683 confirmed COVID-19 cases in Thailand, with 1, 2, and 22 confirmed cases in Mahasarakham province, respectively.
Mahasarakham University’s Ethics Committee for Research Involving Human Subjects approved the study (No. 183/2020), which adhered to the tenets of the Declaration of Helsinki. All participants provided written informed consent.
Study Participants
The study population included 32 HCWs who worked in the ophthalmology outpatient clinic, inpatient ophthalmology ward, and operating room (Supplementary Material).
Local Infection Control Protocol for Patients and Healthcare Workers
In the first phase, we interviewed patients prospectively, using only a questionnaire, regarding COVID-19 symptoms and SARS-CoV-2 exposure risk during their preoperative outpatient visit and on the pre-admission day. In the second phase, we administered the same questionnaire and performed SARS-CoV-2 testing using nasopharyngeal swabs for real-time reverse transcriptase PCR (rRT-PCR) at 1‒3 days preoperatively. We proceeded to surgery if all swabs were negative and chest radiography showed no COVID-19 pneumonia or suspected pulmonary tuberculosis.
In both phases, patients were asked about typical COVID-19 symptoms and possible COVID-19 contact within the previous month, using a COVID-19 screening questionnaire. Possible COVID-19 contact was defined as 1) recent travel to a hotspot area, ie, a red zone or a strictly-controlled province, 2) exposure to a cluster of at least five cases with unknown pneumonia or respiratory tract infections, or 3) a recent visit to crowded places. The lists of red zones or strictly-controlled provinces changed dynamically with local changes in the COVID-19 incidence rate. If any possible COVID-19 contact or symptoms consistent with COVID-19 were reported, we postponed the patient’s surgery.
Universal surgical masks were used by HCWs in the out- and in-patient wards. Gowns and gloves were worn only in the operating room.
Study Outcomes and Measures
The primary outcome was COVID-19 infection among HCWs, defined as any positive SARS-CoV-2 nucleic acid test from nasopharyngeal swabs, SARS-CoV-2 immunoglobulin G/M (IgG/IgM), or anti-SARS-CoV-2 spike protein (S) antibody seroconversion (Supplementary Material). Nucleic acid tests were performed with the approval of our hospital’s infection control committee based on the epidemiological risk. HCWs were also tested for SARS-CoV-2 IgG/IgM within 4 weeks prior to study commencement and for anti-SARS-CoV-2 S antibody within 3 weeks after study completion.
The secondary outcome included the cataract surgical volume performed by three ophthalmologists during the study period, as compared to the volume during the same length of time in our center pre-pandemic.
We also performed post-hoc analyses comparing the patient’s best-corrected visual acuity (BCVA) improvement, in logMAR, between pre- and post-cataract surgery (measured at 1 month postoperatively in an outpatient clinic). Furthermore, we compared the BCVA improvement obtained postoperatively by the same three surgeons during the pre-COVID-19 pandemic in Thailand (July 1, 2019 to March 31, 2020). All BCVA data were extracted via the Internet from the national database that collected all cataract patient data in the Thai Universal Health Coverage Scheme. Favorable postoperative BCVA was defined as < 0.48 logMAR.
Statistical Analysis
Categorical data are expressed as frequencies and percentages, and continuous variables are expressed as means and standard deviations or medians and ranges based on distribution patterns. Differences between the patients were compared using appropriate statistical tests for continuous and categorical data. We used the Wilcoxon test to compare the paired data and the Kruskal‒Wallis test for differences in changes between the two groups. Statistical significance was set at p < 0.05. Data were analyzed using IBM® SPSS® for Windows version 24 (IBM SPSS, Armonk, NY) and GraphPad Prism version 9 (GraphPad, La Jolla, CA).
Results
Healthcare Worker Outcome
Twenty-six HCWs underwent nasopharyngeal swab and rRT-PCR testing during the study period, at an average of 2.15 times per HCW. Six HCWs did not undergo nasopharyngeal swab testing during the study. The reasons for rRT-PCR testing were linked to exposure to COVID-19 patients, other than cataract patients. All RT-PCR tests were negative for SARS-CoV-2.
All 32 HCWs tested negative for SARS-CoV-2 IgM and IgG at baseline. At the end of the study, 27 HCWs tested negative for anti-SARS-CoV-2 S antibody. Four HCWs did not undergo serological testing at the end of the study, and one HCW had a hemolyzed blood sample. Two HCWs did not undergo any rRT-PCR or serological testing during or at the end of the study period. According to their recalled history, these two HCWs had no illness compatible with COVID-19 during the study period.
Trends in Cataract Surgery
Before the first COVID-19 wave, 74 cataract surgeries on average were performed at our center each month. During the national lockdown, all elective surgeries were postponed in April 2020, and only two cataract patients underwent surgery due to urgency. We resumed cataract surgeries in May 2020 under our local infection control protocol, and the volume increased by 87.21%, as compared to that in May 2019 and continued to increase in the month-to-month (MoM) comparison throughout the study period. The average increase in cataract surgeries performed MoM was 50.09% (Figure 2).
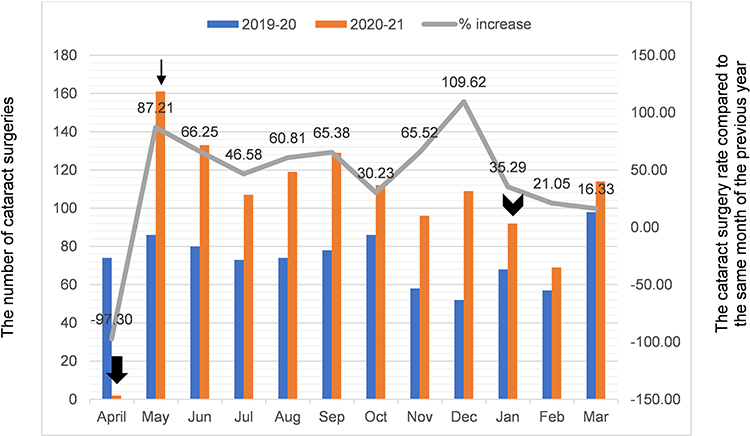 |
Figure 2 Trends in cataract surgery performed during the study period as compared to the pre-pandemic volume. Large arrow: lockdown phase. Small arrow: after lockdown was lifted. Chevron: start of the second wave. |
Patients’ Characteristics and Outcome
Of the 1031 patients scheduled for cataract surgery, 84 did not undergo surgery for the reasons shown in Figure 3. In the final follow-up, 947 patients underwent cataract surgery during the study period (672 and 275 during the first and second periods, respectively). The median age was 67 years (interquartile range, 61–73 years). Phacoemulsification (PE) accounted for 90.39% of cases, followed by manual small-incision cataract surgery (6.76%), extracapsular cataract extraction (ECCE) (2.74%), and intracapsular cataract extraction (0.11%).
 |
Figure 3 Flow diagram of patients who underwent cataract surgery during the study period. |
No COVID-19 contact or COVID-19 symptoms within 1 month were identified using our questionnaire. All 275 patients in the second phase had negative rRT-PCR tests for SARS-CoV-2 within 3 days preoperatively.
Pre- and postoperative BCVA data were available for 813 individuals (89.6%) during the study period. There was a significant difference in baseline BCVA between the two periods, with more advanced visual impairment observed in the pre-COVID-19 pandemic period (difference, 0.18 [95% confidence interval (CI): 0.00–0.18], p < 0.0001) (Figure 4A). Additionally, the postoperative BCVA was significantly lower in the COVID-19 pandemic period than in the pre-pandemic period (difference, 0.1 [95% CI: 0.00–0.12], p < 0.0001) (Figure 4A). However, the change in pre- and postoperative BCVA between the two groups was not significantly different (Figure 4B). BCVA details for each period are shown in Table 1.
 |
Table 1 Best-Corrected Visual Acuity Outcome from COVID-19 Pandemic Period and Pre-COVID-19 Pandemic Period |
 |
Figure 4 (A) Comparison of baseline best-corrected visual acuity (BCVA) and postoperative BCVA between the pre-COVID-19 period and during the COVID-19 pandemic. (B) Comparison of the median difference between pre- and postoperative BCVA between the pre-COVID-19 period and during the COVID-19 pandemic. Triangle: pre-COVID-19 pandemic. Circle: COVID-19 pandemic. Asterisk: p<0.0001. Abbreviation: ns, not significant. |
Postoperative BCVA achieved a favorable outcome < 0.48 logMAR in both periods.
Discussion
This large cohort study revealed the effectiveness of local infection control protocol in preoperative screening for COVID-19 among cataract surgery patients in Thailand. No HCWs in the ophthalmology department working with cataract surgery patients in our center experienced seroconversion of the SARS-CoV-2 S antibody or had positive nucleic acid tests during the study period. Our results are reassuring for HCWs working in the context of a low COVID-19 incidence rate and indicate that local infection control measures, involving multiple aspects, such as verbal screening for COVID-19 exposure risk and symptoms, personal protective equipment (PPE) use, in-hospital physical distancing, and universal nucleic acid test screening during an increasing local COVID-19 incidence rate, are effective in preventing nosocomial COVID-19 infection in HCWs.
Since the beginning of the pandemic, there has been great concern regarding COVID-19 transmission to HCWs, particularly ophthalmologists. Early reports from China stated that three ophthalmologists had contracted COVID-19 from patients and had subsequently died, and the death of an additional 17 ophthalmologists was later reported worldwide.18 Three reports regarding COVID-19 infection among ophthalmology professionals have revealed varying incidence rates during the first COVID-19 wave—16.1% from a single center in Spain, 2.52% from 10 hospitals in Wuhan, and 8.7% from a multinational survey conducted mostly in Saudi Arabia, Pakistan, and Egypt.19–21 Lack of adequate PPE use and lower rates of compliance with infection control measures have been reported among ophthalmology HCWs who acquired COVID-19.19–21 However, these reports could not determine whether the infection was nosocomial or community-acquired due to a lack of detailed epidemiological investigations. A recent study demonstrated that most HCWs acquired COVID-19 from the community.22 There was only a 1.2% risk of nosocomial transmission from patients to HCWs, which increased two-fold to 2.4% during AGPs.22 Most leading ophthalmological societies, including the Royal College of Ophthalmologists and Public Health of England, did not include PE as an AGP, supported by data from a modelling study.23,24 Moreover, no infectivity study has revealed that conjunctival fluid or aqueous humor could transmit SARS-CoV-2, despite reports of positivity of these fluids for SARS-CoV-2 nucleic acid in some symptomatic COVID-19 cases.25,26 Additionally, a large seroprevalence study in the US and Belgium with high community COVID-19 incidence rates revealed that most HCWs acquired the disease from the community rather than in-hospital.27,28 These data suggest that ophthalmology units and ophthalmology HCWs carry a very low risk of acquiring COVID-19 if they adhere to all preventive measures, particularly in low COVID-19 incidence rate areas.
Implementing an optimal COVID-19-screening strategy prior to elective eye surgery requires a thorough assessment of local epidemiologic data. India recommends universal nucleic acid testing due to the high local COVID-19 incidence rate.15 However, the IDSA recommends testing according to epidemiological data.17 After the first and before the second wave, no COVID-19 case was reported in our province. A seroprevalence study conducted among our HCWs and patients visiting our center during the first COVID-19 wave showed a 1.6% seroprevalence rate, in which all cases acquired the disease from an outside community with a higher COVID-19 incidence rate. Moreover, the nucleic tests conducted in our province revealed that hidden community COVID-19 transmission was highly unlikely, with only one positive test among 7,694 nucleic acid tests (0.01%) performed before the second wave and 21 positive tests among 15,471 nucleic tests (0.13%) performed during the second wave, up to the end of our study.
Thailand successfully managed the first COVID-19 wave, which was reflected by a low mortality rate, low local transmission rate, and prompt recovery of most sectors, including social, economic, and healthcare services.29 Therefore, our data supported the Thai recommendation that a universal preoperative nucleic acid test prior to all eye surgeries is unnecessary when the COVID-19 incidence rate is low. Universal nucleic testing should be considered when the number of local COVID-19 cases, particularly the Omicron variant, which has a higher rate of asymptomatic infection, escalates.30
The cataract surgical volume markedly increased immediately after the lockdown was lifted in May 2020 (87% increase in volume MoM) and continued to exceed the pre-pandemic volume (30‒109% increase in volume MoM) even during the second COVID-19 wave (16‒35% increase in volume MoM) (Figure 2). In contrast to our center’s experience, the Thai national data showed a slower increase in the cataract surgery rate, in which the volume started to exceed the pre-pandemic average in August 2020, and the MoM increased by only 4‒8% (Figure 1).
The steep increase in cataract surgeries performed in our center, as compared to the Thai national data, could be explained as follows: 1) Our center was one of only two hospitals to offer cataract surgery in the province. 2) Cataract surgery was the most-performed surgery in our center prior to the pandemic, and resuming this function was necessary to continue the hospital service. 3) Our center was the only center in the province that was able to perform SARS-CoV-2 nucleic acid tests from May to June 2020, which might have influenced the patients’ preference to visit our center. 4) A local infection control committee in our center conducted a surveillance SARS-CoV-2 nucleic acid test for all ophthalmology HCWs when lockdown was lifted in May 2020 to ensure that surgery would be safe for all HCWs. All these data showed that a well-established protocol implemented by local infection control and a readily available PCR laboratory service plays a significant role in ensuring and monitoring safety in continuing medical services during the COVID-19 pandemic.
In the post-hoc results, we demonstrated a slightly better postoperative BCVA during than before the pandemic. This may be because relatively few ECCEs were performed during the pandemic period. ECCE is associated with poor visual outcomes post-cataract surgery.31 ECCE has worse final BCVA than PE, which is the most performed technique due to postoperative astigmatism.32,33 In the pre-pandemic period, more patients with mature and hard cataracts and worse preoperative BCVA were seen. This also resulted in a large difference in the percentage of ECCEs performed in the pre-pandemic period compared to that in the pandemic period (12.89% vs 2.74%), which may have resulted in the worse pre-pandemic postoperative BCVA. However, we were unable to gather complete BCVA data from all the health coverage schemes, which might have affected this finding. Additionally, the cataract pathology in each period was not assessed in detail, which limits further interpretation. A strength of our study was that it gathered 89% of all BCVA data during the study period, and the postoperative BCVA mostly achieved a favorable visual outcome.
Our study had some limitations. First, final serological results were missing for five nurses and assistants. Although no respiratory symptoms were noted among these HCWs during the study, we could not completely exclude asymptomatic COVID-19 infection. Second, some additional ophthalmology HCWs were hired during the study period and were excluded from the study. However, over 95% of HCWs working in ophthalmology units were included in the final analysis. Third, anti-S antibodies might have waned and become undetectable by the final follow-up. Fourth, we did not assess the compliance with using PPE and other preventive measures, such as masks, hand hygiene, and universal precaution, during surgeries. We could not be certain that the lack of infection among HCWs was because there were no occult COVID-19 in the province or whether the preventive strategy was simply highly effective. Fifth, data regarding pre- and post-operative BCVA were available only in cases with the Universal Health Coverage Scheme. Sixth, peri- and postoperative complications were not assessed in our study. Surgeries were performed by three surgeons with more than 25 years, 4 years, and 3 years of ophthalmology practice experience. Surgical experience may have an impact on the complication rate such as the posterior capsular rupture; however, postoperative endophthalmitis was not reported during the study period.
Conclusion
In conclusion, performing cataract surgery during the COVID-19 pandemic is safe for HCWs with well-established infection control measures, even during a surge in new COVID-19 waves. This makes an uninterrupted service possible, which is important given that many patients with disabling cataracts are on long waiting lists during the COVID-19 pandemic. Our findings show that favorable visual outcomes can be achieved for these patients during the pandemic, similar to those in the pre-pandemic era.
Funding
This research project was financially supported by the Faculty of Medicine, Mahasarakham University, Mahasarakham (No. 183/2020).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. COVIDSurg Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg. 2020;107(11):1440–1449. doi:10.1002/bjs.11746
2. Toro MD, Brézin AP, Burdon M, et al. Early impact of COVID-19 outbreak on eye care: insights from EUROCOVCAT group. Eur J Ophthalmol. 2021;31(1):5–9. doi:10.1177/1120672120960339
3. Al-Khersan H, Kalavar MA, Tanenbaum R, et al. Emergent ophthalmic surgical care at a tertiary referral center during the COVID-19 pandemic. Am J Ophthalmol. 2021;222:368–372. doi:10.1016/j.ajo.2020.08.044
4. Das AV, Reddy JC. Year one of COVID-19 pandemic: effect of lockdown and unlock phases on cataract surgery at a multi-tier ophthalmology network. Indian J Ophthalmol. 2021;69(10):2818–2823. doi:10.4103/ijo.IJO_1568_21
5. Yospaiboon Y, Yospaiboon K, Ratanapakorn T, Sinawat S, Sanguansak T, Bhoomibunchoo C. Management of cataract in the Thai population. J Med Assoc Thai. 2012;95(suppl 7):S177–S181.
6. UCINFO. ucinfo.nhso.go.th [Internet]. Available from: https://ucinfo.nhso.go.th/ucinfo/RptRegisPop-1.
7. National Eye Health Data Centre. Vision. 2020thailand.org [Internet]. Available from: http://vision2020thailand.org/home.php.
8. Gimbel HV, Dardzhikova AA. Consequences of waiting for cataract surgery. Curr Opin Ophthalmol. 2011;22(1):28–30. doi:10.1097/ICU.0b013e328341425d
9. Schlenker MB, Thiruchelvam D, Redelmeier DA. Association of cataract surgery with traffic crashes. JAMA Ophthalmol. 2018;136(9):998–1007. doi:10.1001/jamaophthalmol.2018.2510
10. Palagyi A, Rogers K, Meuleners L, et al. Depressive symptoms in older adults awaiting cataract surgery. Clin Exp Ophthalmol. 2016;44(9):789–796. doi:10.1111/ceo.12800
11. Hodge W, Horsley T, Albiani D, et al. The consequences of waiting for cataract surgery: a systematic review. CMAJ. 2007;176(9):1285–1290. doi:10.1503/cmaj.060962
12. Sii SSZ, Chean CS, Sandland-Taylor LE, et al. Impact of COVID-19 on cataract surgery- patients’ perceptions while waiting for cataract surgery and their willingness to attend hospital for cataract surgery during the easing of lockdown period. Eye. 2021;35(11):3156–3158. doi:10.1038/s41433-020-01229-8
13. High prevalence of Sars-Cov-2 infection in patients undergoing cataract surgery.researchsquare.com [Internet]. Available from: https://www.researchsquare.com/article/rs-203185/v1.
14. Goel R, Arora R, Khanam S, Saxena S, Manchanda V, Pumma P. Is it essential to perform COVID-19 testing prior to ophthalmic procedures? Indian J Ophthalmol. 2020;68(11):2335–2337. doi:10.4103/ijo.IJO_3020_20
15. Honavar SG. Nosocomial COVID-19 transmission in routine ophthalmic practice-Is there new evidence? Indian J Ophthalmol. 2020;68(10):2059–2060. doi:10.4103/ijo.IJO_3046_20
16. Department of Medical Services. Guidelines for surgery during COVID-19 pandemic. covid19.dms.go.th [Internet]. Available from: https://covid19.dms.go.th/Content/Select_Landding_page?contentId=70.
17. Hanson KE, Caliendo AM, Arias CA, et al. The Infectious Diseases Society of America guidelines on the diagnosis of COVID-19: molecular diagnostic testing. Clin Infect Dis. 2021;ciab048. doi:10.1093/cid/ciab048
18. American Academy of Ophthalmology. In memoriam: ophthalmologist deaths from COVID-19. aao.org [Internet]. Available from: https://www.aao.org/coronavirus/deaths.
19. Lacorzana J, Ortiz-Perez S, Rubio Prats M. Incidence of COVID-19 among ophthalmology professionals. Med Clin. 2020;155(5):225. doi:10.1016/j.medcli.2020.05.018
20. Qiao C, Zhang H, He M, et al. Symptomatic COVID-19 in eye professionals in Wuhan, China. Ophthalmology. 2020;127(9):1268–1270. doi:10.1016/j.ophtha.2020.04.026
21. Syed AAO, Jahan S, Aldahlawi AA, Alghazzawi EA. Preventive practices of ophthalmologists during COVID-19 pandemic. Clin Ophthalmol. 2021;15:1267–1275. doi:10.2147/OPTH.S295730
22. Shenoy ES, Weber DJ. Routine surveillance of asymptomatic healthcare personnel for severe acute respiratory coronavirus virus 2 (SARS-CoV-2): not a prevention strategy. Infect Control Hosp Epidemiol. 2021;42(5):592–597. doi:10.1017/ice.2020.1428
23. United Kingdom and Ireland Society of Cataract and Refractive Surgeons. Revised joint UKISCRS/RCOphth advice: cataract surgery: protecting patients and professionals during COVID-19. ukiscrs.org.uk [Internet]. Available from: https://www.ukiscrs.org.uk/resource/Final-UKISCRS-comments-re-updated-guidance-on-phaco-as-an-AGP-and-eye-protection.pdf.
24. Kaur S, Kopsachilis N, Zia R. Aerosol generation during phacoemulsification in live patient cataract surgery environment. J Cataract Refract Surg. 2021;47(6):695–701. doi:10.1097/j.jcrs.0000000000000510
25. Azzolini C, Donati S, Premi E, et al. SARS-CoV-2 on ocular surfaces in a cohort of patients with COVID-19 from the Lombardy Region, Italy. JAMA Ophthalmol. 2021;139(9):956–963. doi:10.1001/jamaophthalmol.2020.5464
26. Casagrande M, Fitzek A, Spitzer MS, et al. Presence of SARS-CoV-2 RNA in the cornea of viremic patients with COVID-19. JAMA Ophthalmol. 2021;139(4):383–388. doi:10.1001/jamaophthalmol.2020.6339
27. Jacob JT, Baker JM, Fridkin SK, et al. Risk factors associated with SARS-CoV-2 seropositivity among US health care personnel. JAMA Netw Open. 2021;4(3):e211283. doi:10.1001/jamanetworkopen.2021.1283
28. Steensels D, Oris E, Coninx L, et al. Hospital-wide SARS-CoV-2 antibody screening in 3056 staff in a tertiary center in Belgium. JAMA. 2020;324(2):195–197. doi:10.1001/jama.2020.11160
29. Rajatanavin N, Tuangratananon T, Suphanchaimat R, Tangcharoensathien V. Responding to the COVID-19 second wave in Thailand by diversifying and adapting lessons from the first wave. BMJ Glob Health. 2021;6(7):e006178. doi:10.1136/bmjgh-2021-006178
30. Garrett N, Tapley A, Andriesen J, et al. High rate of asymptomatic carriage associated with variant strain omicron. medRxiv. 2022. doi:10.1101/2021.12.20.21268130
31. Matta S, Park J, Palamaner Subash Shantha G, Khanna RC, Rao GN. Cataract surgery visual outcomes and associated risk factors in Secondary Level Eye Care Centers of L V Prasad Eye Institute, India. PLoS One. 2016;11(1):e0144853. doi:10.1371/journal.pone.0144853
32. Thevi T, Reddy SC, Shantakumar C. Outcome of phacoemulsification and extracapsular cataract extraction: a study in a district hospital in Malaysia. Malays Fam Physician. 2014;9(2):41–47.
33. Minassian DC, Rosen P, Dart JK, et al. Extracapsular cataract extraction compared with small incision surgery by phacoemulsification: a randomised trial. Br J Ophthalmol. 2001;85(7):822–829. doi:10.1136/bjo.85.7.822
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.