")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 15
Review of the Safety, Efficacy and Tolerability of Palivizumab in the Prevention of Severe Respiratory Syncytial Virus (RSV) Disease
Authors O'Hagan S, Galway N, Shields MD , Mallett P, Groves HE
Received 5 May 2023
Accepted for publication 6 September 2023
Published 11 September 2023 Volume 2023:15 Pages 103—112
DOI https://doi.org/10.2147/DHPS.S348727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender R Aparasu
Shaun O’Hagan,1,2 Niamh Galway,3 Michael D Shields,3,4 Peter Mallett,1,4 Helen E Groves1,2
1Paediatric Infectious Diseases, Royal Belfast Hospital for Sick Children, Belfast, Northern Ireland; 2Wellcome-Wolfson Institute for Experimental Medicine, Queen’s University Belfast, Belfast, Northern Ireland; 3Paediatric Respiratory Medicine, Royal Belfast Hospital for Sick Children, Belfast, Northern Ireland; 4Centre for Medical Education, Queen’s University Belfast School of Medicine, Belfast, Northern Ireland
Correspondence: Helen E Groves, Email [email protected]
Abstract: Respiratory Syncytial Virus (RSV) is a major global cause of childhood morbidity and mortality. Palivizumab, a monoclonal antibody that provides passive immunity against RSV, is currently licensed for prophylactic use in specific “high-risk” populations, including congenital heart disease, bronchopulmonary dysplasia and prematurity. Available research suggests palivizumab use in these high-risk populations can lead to a reduction in RSV-related hospitalization. However, palivizumab has not been demonstrated to reduce mortality, adverse events or length of hospital stay related to RSV. In this article, we review the management of RSV, indications for palivizumab prophylaxis, the safety, cost-effectiveness and efficacy of this preventative medication, and emerging therapeutics that could revolutionize future prevention of this significant pathogen.
Keywords: RSV, palivizumab, efficacy, safety, future directions
Scale of the Problem of RSV Disease
Respiratory Syncytial Virus (RSV) is the leading cause of acute lower respiratory tract infection (LRTI) in infants and young children worldwide.1 RSV infection is associated with a wide clinical spectrum of disease, ranging from mild coryzal symptoms to severe bronchiolitis and pneumonia requiring hospitalization. In 2019, there were over 33 million global RSV infections and 3 million RSV-associated hospital admissions in children under five.2 RSV also commonly affects adults; usually manifesting with mild symptoms, such as a head-cold. However, more severe presentations may occur in adults with significant cardiac or respiratory disease, in immunocompromised individuals and in the elderly.3 This review will primarily focus on the impact of RSV disease in infants and the current role of palivizumab therapy in this group.
Risk factors for severe RSV disease and hospitalization in infants include: prematurity; comorbidities such as Bronchopulmonary Dysplasia (BPD), Congenital Heart Disease (CHD), Immunosuppression, Cystic Fibrosis and Down Syndrome; younger age at time of infection (<six months); low birth weight; low socio-economic status and viral co-infection.4–7 Infants in the first 6 months of life are disproportionately affected by RSV disease; representing 20% of RSV infection and 46% of RSV mortality.2 Very premature infants, born at less than 29 weeks gestation, are especially vulnerable to adverse outcomes and infants with CHD have an estimated 5% mortality with RSV infection.8–10 Although the highest rates of RSV-related hospitalization are seen within high-risk groups, it is important to recognize the vast majority of infection occurs in otherwise healthy infants born at term.11 Virtually all children will have had at least one RSV infection by two years old.12
Socio-economic status greatly impacts RSV morbidity and mortality, with 95% of the global disease burden and greater than 97% of RSV deaths occurring in low- and middle-income countries.2,4,13 In this setting, for every in-hospital RSV death, there are approximately three within the community.2,13 Additionally, RSV infection carries a significant global economic burden, costing an estimated €4.82 billion for inpatient and outpatient management in 2017.14 Sixty-five percent of this economic burden falls onto developing countries.14 Hospitalization accounts for the majority of this cost, with very preterm infants and those with haemodynamically significant CHD (hs-CHD) representing the highest cost per-patient.14–16
Currently, RSV treatment is limited to respiratory and nutritional support; with the exception of the antiviral drug, ribavirin, which lacks widespread use. For over half a century, prevention of infection has remained the most effective strategy in reducing RSV-related mortality.17 In 2015, after almost 70 years of RSV vaccine research, RSV vaccine development was highlighted by the World Health Organization (WHO) as a high-priority global health goal.18
In early May 2023, the United States Food and Drug Administration (US FDA) approved the world’s first-ever RSV vaccine, Arexvy, for the prevention of RSV-related lower respiratory tract infection amongst those aged 60 years or older.19 This landmark approval was quickly followed, in July 2023, by Pfizer’s Abrysvo vaccine which received approval from the European Medicines Agency (EMA) and FDA for active immunisation against RSV-LRTI in adults aged 60 years or older.20,21 Additionally, the EMA granted Abrysvo approval for passive protection against RSV-LRTI in infants from birth to 6 months of life, through maternal immunisation in pregnancy.20
Background to Previously Licensed RSV-Specific Therapies and Prophylaxis
Ribavirin
Ribavirin is a synthetic nucleoside analogue, which inhibits RSV replication and is the only licensed antiviral for RSV infection. However, due to limited supporting evidence and toxicity concerns, in practice it is infrequently prescribed for the management of RSV disease, with use limited to those receiving immunosuppressive medications or with other serious co-morbidities. In relation to potential toxicity issues, pre-clinical research in pregnant rodents using doses below and within the human therapeutic range, demonstrated a dose- and time-dependent teratogenic effect of ribavirin exposure.22–24 It is unknown if ribavirin can lead to teratogenicity in humans. Three studies investigating the potential effects of aerosolized ribavirin exposure concluded that secondary ribavirin absorption by health care workers, if it occurs, is minimal.25–27 Despite these findings, staff anxiety and perception of teratogenic risk are often high. Efficacy studies for ribavirin have been challenging, with an early controlled trial of aerosolized ribavirin use in ventilated infants with severe RSV infection criticized for the use of nebulized water, not saline, as the placebo which is known to induce bronchospasm and cause hypoxaemia.28,29 Furthermore, compared to supportive care, meta-analysis demonstrated no difference in mortality for those receiving aerosolized or oral ribavirin.30 Indeed, ribavirin has only been found to be efficacious when used in RSV-positive children with haematological malignancy or haemopoietic stem cell transplant recipients, where it was shown to reduce progression from upper- to lower-respiratory-tract infection and all-cause mortality.31
RSV-IGIV - RespiGam®
In 1996, RSV immune globulin (RSV-IGIV (RespiGam®)) was the first FDA-licensed immunoprophylactic agent for the prevention of severe RSV bronchiolitis in children.32,33 Established to provide passive RSV-immunity in preterm infants <35 weeks and infants <24 months with BPD, RSV-IGIV is a polyclonal hyperimmune globulin developed from healthy donors with high serum RSV-neutralizing antibody titres.32 The seminal PREVENT trial, studying the use of RSV-IGIV in premature infants, demonstrated a 41% reduction in RSV hospitalization and 53% reduction in total days of hospitalization per 100 children versus placebo.34 However, significant clinical and practical limitations lead to a decline in its use. Administration of the monthly intravenous 3–4 hour infusion proved time-consuming and challenging, particularly in the ex-preterm population where intravenous access difficulties are common. Additionally, infusions were associated with significantly increased cyanotic episodes, risk of fluid overload and worsened post-operative mortality in cyanotic CHD patients receiving RSV-IGIV.35,36 Furthermore, RespiGam® was also expensive; in 1996, per infant, the average cost of prophylaxis per season was $4000–5000 USD.37 In 2003, it was withdrawn from the market, following the successful licensing of palivizumab in 1998.38
The Role of Palivizumab (Synagis®) in RSV Disease Prophylaxis
Palivizumab is the first monoclonal antibody successfully developed and licenced for RSV prophylaxis and has been in use since 1998.38,39 Produced in mouse myeloma host cells, via recombinant DNA technology, palivizumab provides short-term passive immunity by preventing RSV uptake into host cells through fusion-inhibitory activity against antigenic site II of the RSV F-protein.40,41
Presently, palivizumab is licenced for prophylactic use in specific “high-risk” populations under expert supervision. In the United Kingdom (UK), these “high-risk” groups include:
- Infants under 6 months old and born at less than 35 weeks’ gestation.
- Children under 2 years old who have received treatment for BPD within the last 6 months.
- Children under 2 years old with haemodynamically significant CHD (hs-CHD).
- Should also be considered in infants with Severe Combined Immunodeficiency (SCID) and those requiring long-term ventilation.42
Palivizumab Administration Considerations
Palivizumab remains prohibitively expensive and, with a half-life in the range of 18–21 days, requires monthly intramuscular administration during the RSV season (to a maximum of five months per season).40 The recommended dose of palivizumab is 15mg/kg and the 100mg/mL solution for injection is supplied as either 0.5mL or 1 mL vials; necessitating practical considerations to reduce wastage.40 In the Northern hemisphere, the RSV seasonal peak typically occurs between October and March, with the majority of infections occurring within a relatively short timeframe of approximately six weeks.40 Where possible, the first dose should be administered prior to the start of the RSV season, which can pose challenges due to inter-seasonal variation in RSV circulation. Palivizumab immunisation programmes are thus timed to coincide with the onset of the RSV seasonal epidemic wave. This requires surveillance data to monitor levels of RSV activity, such as that performed by Public Health England (PHE), which collects RSV surveillance data from hospital microbiology laboratory reports across England and Wales.40
Palivizumab Use and Overall Efficacy
Palivizumab has no demonstrated treatment benefit in symptomatic RSV disease; however, its use prophylactically has been shown in “high-risk” populations to mitigate serious RSV disease. A recent Cochrane review suggests palivizumab leads to a 56% reduction in RSV hospitalization (RSVH) amongst premature infants, a 22% reduction in hospitalization from any respiratory illness, reduced number of wheezing days at one year follow-up and a 67% reduction in RSV infection rates at two-year follow-up.43 However, there is little to no difference in RSV mortality, adverse events or length of hospital stay with palivizumab prophylaxis.43 A more recent systematic review and network meta-analysis of 14 randomised controlled trials, conducted to compare the outcomes of four monoclonal antibodies (palivizumab, motavizumab, nirsevimab and suptavumab), found that palivizumab, motavizumab and nirsevimab were all associated with similar reduced rates of RSV infection and hospitalisation compared to placebo.44
Efficacy of Palivizumab on RSV-Related Hospitalization (RSVH)
Palivizumab is highly effective in preventing RSVH in preterm infants with or without chronic lung disease, both in controlled trials and real-world studies.38 The safety and efficacy of palivizumab for preventing RSVH was first established in the IMpact-RSV study, demonstrating a 55% reduction in RSVH with palivizumab prophylaxis versus placebo, in patients with prematurity (≤35 wGA) or Bronchopulmonary Dysplasia (BPD).39 A recent systematic review of Phase 3 clinical trials, demonstrated significantly lower RSVH rates following palivizumab prophylaxis versus placebo in children with BPD (7.9% vs 12.8%) and in premature infants (1.8% vs 8.1%).43 Similar RSVH rates were seen in real-world settings; 0–5.5% in patients with BPD (10 studies) and 0.7–4.0% in premature infants (16 studies).45
Amongst otherwise healthy moderate-to-late preterm infants (29–35 weeks) a number of studies have demonstrated benefit of prophylactic palivizumab in reducing RSVH. Real-world studies have demonstrated a four-fold reduction in RSV hospitalization in those receiving palivizumab.46 These results are comparable to randomised controlled trial findings. Additionally, a recent multicentre Italian study conducted before and after health policy changes to discontinue palivizumab eligibility for moderate-to-late preterm infants, demonstrated a significant increase in RSVH in the season post-policy change compared to pre-policy change (5.1% and 1.9% respectively).47
Efficacy of Palivizumab on Oxygen Requirement of Hospitalized RSV Patients
The effect of palivizumab on supplemental oxygen requirement is not well described in current research. A recent systematic review demonstrated a statistically significant reduction in the duration of supplemental oxygen required in those receiving palivizumab prophylaxis, within two Phase 3 trials.45 However, analysis of real-world studies has shown a heterogenous range in supplemental oxygen requirement amongst hospitalized premature infants with RSV infection, following palivizumab prophylaxis.48–51
Palivizumab Efficacy in “High Risk” Groups
Amongst children with congenital heart disease, bronchopulmonary dysplasia and prematurity, palivizumab is associated with a 53%, 65% and 68% reduction in RSV hospitalization respectively.38 A phase 3 trial conducted in hs-CHD patients, however, found no significant difference in intensive care unit (ICU) admission between palivizumab and placebo groups (38.2% versus 38.1%).52 Recent systematic review evidence suggests palivizumab may also be associated with reduced RSVH in children aged under 2 years with Cystic Fibrosis.53 Further research is necessary to establish palivizumab impact amongst other ‘high-risk groups’, including vulnerable neuro-disability patients, those with immunodeficiency and Down Syndrome (DS).38,42 Interestingly, recent expansion of the Japanese palivizumab prophylaxis program, to include children with DS, was not associated with a reduction in RSVH in these children.54 However, up to 90% of DS children in Japan, with varying RSV-risk, were already receiving palivizumab prophylaxis prior to the 2013 policy expansion, which may account for the lack of impact following the policy introduction.54
Palivizumab Impact on Rates of ICU Admission and Length of Stay
In 1998, the IMpact-RSV trial included 1502 children with prematurity (≤35 weeks) or bronchopulmonary dysplasia, randomised to receive palivizumab or placebo.39 This study showed reduced ICU admission (1.3 vs 3.0%; P = 0.026), shorter respiratory-related hospital days per 100 children (124 vs 180 days; P = 0.004) and a reduction in all respiratory hospitalizations (16 vs 22%; P = 0.008) amongst those receiving palivizumab.39 Of note, there was no significant reduction in ICU length of stay.39 Amongst hs-CHD patients, a more recent Phase 3 trial demonstrated no significant difference in RSV-related ICU admission rates, but did report a 78% reduction in ICU length of stay amongst those receiving palivizumab compared to placebo (15.9 vs 71.2 days per 100 children; P = 0.08).52
Palivizumab Impact on Rates and Duration of Mechanical Ventilation
The IMpact-RSV trial found no significant difference in rates or duration of mechanical ventilation amongst palivizumab and placebo groups.39 Likewise, a systematic review of six observational studies found no significant difference in requirement for mechanical ventilation amongst premature infants hospitalized with RSV who received palivizumab.45 Additionally, no significant difference in mechanical ventilation requirement was found amongst hs-CHD patients; however, palivizumab was associated with an 88% reduction in mechanical ventilation duration in this “high risk” group (6.5 vs 54.7 days per 100 children; P = 0.224).52
RSV-Related Mortality in Patients Receiving Palivizumab Prophylaxis
Thankfully, deaths from RSV infection are uncommon. Systematic review of palivizumab safety highlights RSV-related mortality rates within two controlled trials were 0.2% in premature infants and 0.3% in infants with hs-CHD.37, 50 Current evidence demonstrates little to no difference in mortality or adverse events amongst those receiving RSV prophylaxis with palivizumab.43
Impact of Palivizumab on RSV-Related Long-Term Outcomes
Research has shown that RSV infection in infancy may lead to long-term respiratory issues, including recurrent wheeze and reactive airway disease.55 A 2020 WHO report on the association between RSV and asthma was inconclusive in demonstrating whether this relationship represents causation or correlation due to a shared predisposition.11
Recent interventional studies have demonstrated a reduced risk of wheezing in the first years of life among healthy preterm infants who received palivizumab.43,56 However, no significant different in lung function parameters in adolescents born very prematurely (<29 weeks), has been found when comparing those who received palivizumab with those who did not.57
In summary, palivizumab prophylaxis has demonstrated efficacy for a number of RSV-disease outcomes across a range of at risk patient groups as summarised in Table 1.
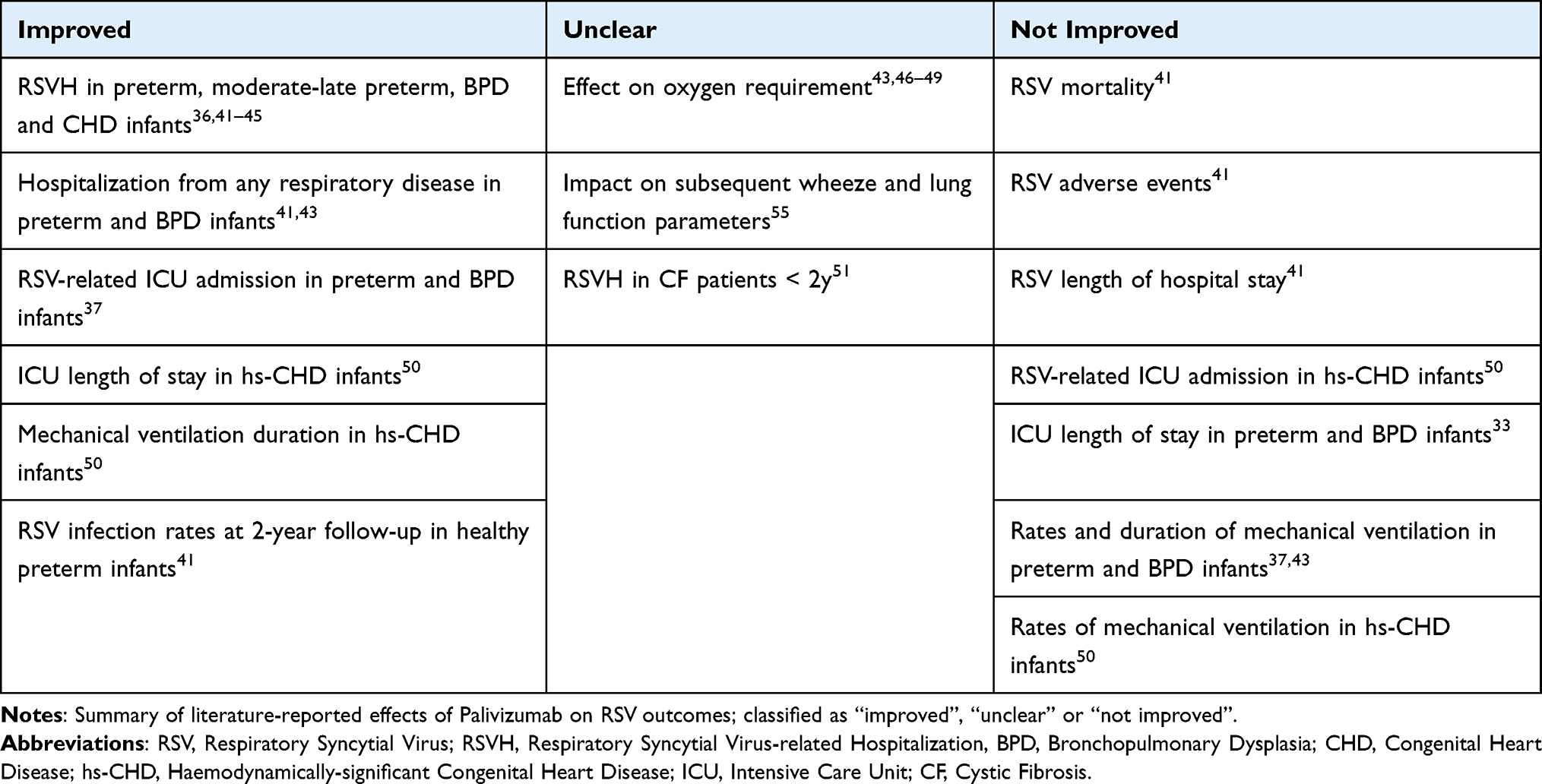 |
Table 1 Effect of Palivizumab on RSV Outcomes |
Palivizumab Cost-Effectiveness
The cost effectiveness of palivizumab remains under debate, with significant uncertainties due to limited availability and quality of health economic studies.58 In the UK, unselected use of palivizumab in all children meeting licensed indication fails to meet UK convention for cost-effectiveness, based on a threshold of £30,000 per Quality Adjusted Life Year.58,59 Economic sub-group analysis of “high-risk” populations demonstrated palivizumab prophylaxis may be cost-effective in some subgroups.58 These include children without CLD or CHD but at least two other risk-factors (apart from gestational age or birth age) and children with CLD or CHD did not necessarily need to have other risk factors for palivizumab prophylaxis to be considered cost-effective.58
Palivizumab Safety/Side-Effects and Tolerability
The frequency of adverse events associated with palivizumab is low in both clinical trial and real-world studies (1–12% and 0–7% of patients, respectively).45 The IMpact-RSV trial reported no significant difference in adverse events between palivizumab and placebo groups (11% and 10% respectively).39 The most common adverse events consisted of fever (3% placebo vs 2.8% palivizumab), nervousness (2.6% placebo vs 2.5% palivizumab), injection site reactions – including erythema, pain, swelling and bruising – (1.8% placebo vs 2.7% palivizumab) and mild-moderate derangement of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) (1.6% placebo vs 3.6% palivizumab and 2% placebo vs 2.3% palivizumab, respectively).39 Discontinuation of injections due to adverse events were rare (0.3%).39 These adverse events were predominantly mild and of short duration. Amongst observational studies, the most commonly reported adverse events were fever, rhinitis and pain at the injection site.45
The Role of Motavizumab in RSV Disease Prophylaxis
Motavizumab is a monoclonal antibody derivative of palivizumab that was developed with the aim of offering higher RSV affinity and a longer half-life. Pre-clinical studies using rodent lung models of RSV infection were promising, showing between 50 and 100 times reduced viral titres compared to palivizumab.60 Motavizumab was also found to be effective in reducing RSV hospitalization amongst high-risk term infants in the United States.61 However, in December 2010, its further development was discontinued following two FDA licensing rejections related to concerns of lacking non-inferiority to palivizumab and safety issues regarding serious side-effects (anaphylactic and allergic skin reactions).61
The Role of Suptavumab in RSV Disease Prophylaxis
Suptavumab is another human monoclonal antibody developed for RSV-disease prophylaxis. However, in August 2017 Regeneron Pharmaceuticals discontinued ongoing clinical development, after the phase 3 trial evaluating its use in preterm infants failed to meet the primary endpoint of preventing medically attended RSV infections.62,63
The Future of RSV Disease Prevention
Next Generation Monoclonal Antibodies
Presently, therapeutic options for treatment of RSV disease remain limited. However, a large number of novel therapeutic and prophylactic candidates are being developed and tested in clinical trials. One notable new preventative monoclonal antibody therapy, nirsevimab, has shown great promise in recent clinical trials. Like palivizumab, nirsevimab is a humanized monoclonal antibody; however, it has been engineered with a triple amino acid substitution (YTE modification) that provides a much longer half-life of 150 days.64 Thus, a single injection has the potential to protect against RSV for an entire season; possibly improving treatment compliance and lowering costs.17 Additionally, by targeting the Ø site of the RSV fusion (F) protein, nirsevimab has the ability to neutralize both A and B strains of RSV, with a potency greater than 50 times that of palivizumab.65
In 2022, the UK Medicines and Healthcare Products Regulatory Agency (MHRA) and the European Medicines Agency (EMA) both granted approval for nirsevimab in the prevention of RSV disease in infants during their first RSV season.66,67 This approval came following the success of the MEDLEY and MELODY clinical trials. The phase 2b MEDLEY trial evaluated the safety and tolerability of nirsevimab in healthy preterm infants (29–35 weeks’ gestation) approaching their first RSV season. Compared to placebo, nirsevimab was found to lower medically attended RSV LRTI by 70.1% (2.6% vs 9.5%; P =<0.001) and RSVH by 78.4% (0.8% vs 4.1%; P =<0.001).68 The phase 3 MELODY trial, conducted in 1490 healthy late-preterm (≥35 weeks’ gestation) and full-term infants randomised to receive nirsevimab or placebo, also demonstrated a 74.5% reduction in medically attended RSV LRTI.69 RSV disease in preterm and other “high-risk” infants represents only a small proportion of the overall disease burden. This research highlights the potential for nirsevimab to have a significant impact on the prevention of serious RSV disease not only in preterm “high-risk” groups, but also in healthy term babies. Further study of the role of nirsevimab in prevention of RSV hospitalization in all babies is currently being conducted as part of the HARMONIE trial, which aims to recruit more than 20,000 infants across the United Kingdom, Germany and France.70 Preliminary trial data was presented at the European Society for Paediatric Infectious Diseases (ESPID) conference earlier this year. With 8058 infants randomized at the time of primary analysis; 4037 in the nirsevimab group and 4021 in the no intervention group, nirsevimab showed an efficacy of 83.2% (95% CI: 67.77–92.04%) against RSV LRTI hospitalisation and 75.71% (95% CI: 32.75–92.91%) against very severe RSV LRTI.71
Another promising monoclonal antibody undergoing clinical trial is clesrovimab. In-vitro studies of clesrovimab have demonstrated an extended half-life and similar potency and efficacy to nirsevimab.72 Trial simulations predict a single dose could provide greater than 75% efficacy against RSV LRTI, with preventative effects lasting for more than 150 days.73
RSV Vaccines
As of January 2023, there are 34 RSV disease preventatives currently undergoing clinical trial; targeting maternal, elderly and paediatric populations.74 Four vaccine development strategies are being explored, including live-attenuated vaccines, nucleic acid vaccines, protein-based vaccines and recombinant vectors.74 It is estimated that an RSV vaccine with 80% efficacy could, annually, prevent up to 1.1 million hospitalizations and 22,000 RSV deaths globally.13
As previously noted, the first-ever RSV vaccine for the prevention of RSV-LRTI amongst adults aged 60 years or older, Arexvy, was approved by the US FDA in May 2023.19 This approval came following trial data demonstrating a statistically significant overall vaccine efficacy of 82.6% (96.95% CI, 57.9 to 94.1) against RSV-related LRTI; meeting the primary research endpoint.75 In July 2023, Pfizer’s Abrysvo vaccine also received EMA and FDA approval for prevention of RSV-LRTI in adults over 60 years old.20,21 This approval came on the basis of data from the ongoing global phase 3 clinical trial, RENOIR (RSV vaccine Efficacy study iN Older adults Immunized against RSV disease). The EMA also granted Abrysvo approval for passive protection against RSV-LRTI in infants from birth to 6 months of life, through maternal immunisation in late second or third trimester of pregnancy.20 This approval comes after the phase 3 randomised placebo-controlled trial, MATISSE (Maternal Immunization Study for Safety and Efficacy), was stopped early due to meeting the primary outcome after enrolment of approximately 7400 pregnant women. The MATISSE study demonstrated a vaccine efficacy of 81.8% for the primary outcome of prevention of severe medically attended LRTI during the first 90 days of life, as well as 69.4% efficacy over the first 6 months of life.76 However, of note, a safety concern in a similar maternal RSV vaccine candidate, developed by GSK, has prompted some experts to call for further analysis of Pfizer’s trial data and post-approval monitoring.77 Development of the similar GSK maternal RSV vaccine was halted in a phase 3 trial in February 2023, due to safety concerns relating to a rise in preterm births and neonatal deaths.78 Specifically, GSK data demonstrated preterm birth in 6.8% of the maternal vaccine cohort and 4.9% in the placebo; equating to around one extra preterm delivery for every 54 vaccinated mothers and, additionally, there were 13 neonatal deaths in the vaccine cohort with 3 in the placebo cohort.79 Phase 3 interim analysis results for Pfizer’s Abrysvo maternal RSV vaccine candidate did show a difference in preterm births for vaccinated compared to unvaccinated mothers (5.6% versus 4.7%); however, this difference was not statistically significant.76
Conclusion
Palivizumab is the first licensed monoclonal antibody therapy against RSV and has an established safety and tolerability profile as well as demonstrated efficacy in the prevention of severe-RSV related disease in certain high-risk groups. However, with the advent of new monoclonal antibody therapies, such as nirsevimab and novel anti-RSV vaccines, the future prevention of this significant pathogen is likely to rapidly develop, with the potential to significantly alter the current role of palivizumab therapy in prevention of severe RSV disease.
Disclosure
HEG previously received honoraria for presenting at an RSV-educational event sponsored by an AstraZeneca Educational grant and for presenting at an RSV-educational event sponsored by AbbVie. MS reports personal fees from Sanofi Pharmaceutical, outside the submitted work. All other authors declare no conflicts of interest in this work.
References
1. Meng J, Stobart CC, Hotard AL, Moore ML. An overview of respiratory syncytial virus. PLoS Pathog. 2014;10(4):e1004016.
2. Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340):2047–2064. doi:10.1016/S0140-6736(22)00478-0
3. Haber N. Respiratory syncytial virus infection in elderly adults. Med Mal Infect. 2018;48(6):377–382. doi:10.1016/j.medmal.2018.01.008
4. Anderson J, Oeum M, Verkolf E, et al. Factors associated with severe respiratory syncytial virus disease in hospitalised children: a retrospective analysis. Arch Dis Child. 2021;107:359–364. doi:10.1136/archdischild-2021-322435
5. Bloemers BL, van Furth AM, Weijerman ME, et al. Down syndrome: a novel risk factor for respiratory syncytial virus bronchiolitis—a prospective birth-cohort study. Pediatrics. 2007;120:e1076–e1081. doi:10.1542/peds.2007-0788
6. Murray J, Bottle A, Sharland M, et al. Risk factors for hospital admission with RSV bronchiolitis in England: a population-based birth cohort study. PLoS One. 2014;9:e89186. doi:10.1371/journal.pone.0089186
7. Kristensen K, Hjuler T, Ravn H, Simões EA, Stensballe LG. Chronic diseases, chromosomal abnormalities, and congenital malformations as risk factors for respiratory syncytial virus hospitalization: a population-based cohort study. Clin Infect Dis. 2012;54:810–817. doi:10.1093/cid/cir928
8. Igueras-Aloy J, Manzoni P, Paes B, et al. Defining the risk and associated morbidity and mortality of severe respiratory syncytial virus infection among preterm infants without chronic lung disease or congenital heart disease. Infect Dis Ther. 2016;5(4):417–452. doi:10.1007/s40121-016-0130-1
9. Haerskjold A, Kristensen K, Kamper-Jorgensen M, Nybo Andersen AM, Ravn H, Graff Stensballe L. Risk factors for hospitalization for respiratory syncytial virus infection: a population-based cohort study of Danish children. Pediatr Infect Dis J. 2016;35(1):61–65. doi:10.1097/INF.0000000000000924
10. Nguyen-van-tam J, Wyffels V, Smulders M, et al. Cumulative incidence of post-infection asthma or wheezing among young children clinically diagnosed with respiratory syncytial virus infection in the United States: a retrospective database analysis. Influenza Other Respir Viruses. 2020;14:730–738. doi:10.1111/irv.12770
11. Driscoll AJ, Arshad SH, Bont L, et al. Does respiratory syncytial virus lower respiratory illness in early life cause recurrent wheeze of early childhood and asthma? Critical review of the evidence and guidance for future studies from a World Health Organization-sponsored meeting. Vaccine. 2020;38(11):2435–2448. doi:10.1016/j.vaccine.2020.01.020
12. Esteban I, Stein RT, Polack FP. A durable relationship: respiratory syncytial virus bronchiolitis and asthma past their golden anniversary. Vaccines. 2020;8(2):201. doi:10.3390/vaccines8020201
13. Shi T, McAllister DA, O’Brien KL, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958. doi:10.1016/S0140-6736(17)30938-8
14. Zhang S, Akmar LZ, Bailey F, et al. Cost of respiratory syncytial virus-associated acute lower respiratory infection management in young children at the regional and global level: a systematic review and meta-analysis. J Infect Dis. 2020;222(7):680–687. doi:10.1093/infdis/jiz683
15. Bozzola E, Ciarlitto C, Guolo S, et al. Respiratory syncytial virus bronchiolitis in infancy: the acute hospitalization cost. Front Pediatr. 2021;8:594898. doi:10.3389/fped.2020.594898
16. Brusco NK, Alafaci A, Tuckerman J, et al. The 2018 annual cost burden for children under five years of age hospitalised with respiratory syncytial virus in Australia. Commun Dis Intell. 2018;2022:46.
17. Messina A, Germano C, Avellis V, et al. New strategies for the prevention of respiratory syncytial virus (RSV). Early Hum Dev. 2022;174:105666. doi:10.1016/j.earlhumdev.2022.105666
18. Modjarrad K, Giersing B, Kaslow DC, Smith PG, Moorthy VS. WHO consultation on respiratory syncytial virus vaccine development report from a World Health Organization meeting held on 23–24 March 2015. Vaccine. 2016;34(2):190–197. doi:10.1016/j.vaccine.2015.05.093
19. U.S Food and Drug Administration. FDA news release, FDA approves first Respiratory Syncytial Virus (RSV) vaccine, arexvy approved for individuals 60 years of age and older; 2023. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine.
20. European Medicines Agency. First RSV vaccine to protect infants up to 6 months of age and older adults; 2023. Available from: https://www.ema.europa.eu/en/news/first-rsv-vaccine-protect-infants-6-months-age-older-adults.
21. Pfizer. Pfizer press release, U.S. FDA approves ABRYSVO™, Pfizer’s vaccine for the prevention of Respiratory Syncytial Virus (RSV) in older adults; 2023. Available from: https://www.pfizer.com/news/press-release/press-release-detail/us-fda-approves-abrysvotm-pfizers-vaccine-prevention.
22. Johnson EM. The effects of ribavirin on development and reproduction: a critical review of published and unpublished studies. Endocrinology. 1990;131:1149–1156.
23. Kilham L, Ferm VH. Congenital anomalies induced in hamster embryos with ribavirin. Science. 1977;195(4276):413–414. doi:10.1126/science.401547
24. Ferm VH, Willhite C, Kilham L. Teratogenic effects of ribavirin on hamster and rat embryos. Teratology. 1978;17(1):93–102. doi:10.1002/tera.1420170117
25. Linn WS, Gong H Jr, Anderson KR, Clark KW, Shamoo DA. Exposures of health-care workers to ribavirin aerosol: a pharmacokinetic study. Arch Environ Health. 1995;50(6):445–451. doi:10.1080/00039896.1995.9935981
26. Rodriguez WJ, Bui RH, Connor JD. Environmental exposure of primary care personnel to ribavirin aerosol when supervising treatment of infants with respiratory syncytial virus infections. Antimicrob Agents Chemother. 1987;31(7):1143–1146. doi:10.1128/AAC.31.7.1143
27. Bortolussi RA, Gold R. Ribavirin aerosol therapy: safety for staff. Can Med Assoc J. 1988;138:204.
28. Smith DW, Frankel LR, Mathers LH, Tan ATS, Ariagno RL, Prober CG. A controlled trial of aerosolized ribavirin in infants receiving mechanical ventilation for severe respiratory syncytial virus infection. N Engl J Med. 1991;325(1):24–29. doi:10.1056/NEJM199107043250105
29. Moler FW, Bandy KP, Custer JR. Ribavirin therapy for acute bronchiolitis: need for appropriate controls. J Pediatr. 1991;119(3):509–510. doi:10.1016/S0022-3476(05)82091-8
30. Tejada S, Martinez-Reviejo R, Karakoc HN, Peña-López Y, Manuel O, Rello J. Ribavirin for treatment of subjects with respiratory syncytial virus-related infection: a systematic review and meta-analysis. Adv Ther. 2022;39(9):4037–4051. doi:10.1007/s12325-022-02256-5
31. Anak S, Atay D, Unuvar A, et al. Respiratory syncytial virus infection outbreak among pediatric patients with oncologic diseases and/or BMT. Pediatr Pulmonol. 2010;45(3):307–311. doi:10.1002/ppul.21184
32. Smyth RL, Brearey SP. Bronchiolitis. In: Laurent GJ, Shapiro SD, editors. Encyclopedia of Respiratory Medicine. Academic Press; 2006:268–275.
33. Stiehm RE, Keller MA. Chapter 256 – passive Immunisation. In: Feigin RD, Cherry JD, Demmler-Harrison GJ, Kaplan SL, editors. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases.
34. The PREVENT Study Group. Reduction of respiratory syncytial virus hospitalization among premature infants and infants with bronchopulmonary dysplasia using respiratory syncytial virus immune globulin prophylaxis. Pediatrics. 1997;99(1):93–99. doi:10.1542/peds.99.1.93
35. Junge S, Nokes DJ, Simões EAF, Weber MW. Respiratory syncytial virus. In: Stella R, editor. Quah. International Encyclopedia of Public Health.
36. Simoes EA, Sondheimer HM, Top FH, et al.; The Cardiac Study Group. Respiratory syncytial virus immune globulin for prophylaxis against respiratory syncytial virus disease in infants and children with congenital heart disease. J Pediatr. 1998;133:492–499.
37. Oertel MD. RespiGam: an RSV immune globulin. Pediatr Nurs. 1996;22(6):525.
38. Simões EAF, Bont L, Manzoni P, et al. Past, present and future approaches to the prevention and treatment of respiratory syncytial virus infection in children. Infect Dis Ther. 2018;7(1):87–120. doi:10.1007/s40121-018-0188-z
39. The IMpact-RSV Study Group. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics. 1998;102(3):531–537. doi:10.1542/peds.102.3.531
40. Public Health England. Chapter 27a: respiratory Syncytial Virus. In: Immunisation Against Infectious Disease (Green Book). London: Department of Health; 2015.
41. Harkensee C, Brodlie M, Embleton ND, Mckean M. Passive immunisation of preterm infants with palivizumab against RSV infection. J Infect. 2006;52(1):2–8. doi:10.1016/j.jinf.2005.08.003
42. Paediatric Formulary Committee. BNF for Children. London: BMJ Group, Pharmaceutical Press, and RCPCH Publications; 2022.
43. Garegnani L, Styrmisdóttir L, Roson Rodriguez P, Escobar Liquitay CM, Esteban I, Franco JVA. Palivizumab for preventing severe respiratory syncytial virus (RSV) infection in children. Cochrane Database Syst Rev. 2021;11(11):CD013757. doi:10.1002/14651858.CD013757.pub2
44. Sun M, Lai H, Na F, et al. Monoclonal antibody for the prevention of respiratory syncytial virus in infants and children: a systematic review and network meta-analysis. JAMA Netw Open. 2023;6(2):e230023. doi:10.1001/jamanetworkopen.2023.0023
45. Gonzales T, Bergamasco A, Cristarella T, et al. Effectiveness and safety of palivizumab for the prevention of serious lower respiratory tract infection caused by respiratory syncytial virus: a systematic review. Am J Perinatol. 2023. doi:10.1055/a-1990-2633
46. Manzoni P, Baraldi E, Luna MS, Tzialla C. Real-world studies of respiratory syncytial virus hospitalizations among moderate/late preterm infants exposed to passive immunoprophylaxis with palivizumab. Am J Perinatol. 2022;39(1):7–13. doi:10.1055/s-0042-1757279
47. Priante E, Tavella E, Girardi E, et al. Restricted palivizumab recommendations and the impact on RSV hospitalizations among infants born at > 29 weeks of gestational age: an Italian multicenter study. Am J Perinatol. 2019;36(2):77–82. doi:10.1055/s-0039-1691771
48. Paes B, Mitchell I, Li A, Lanctôt KL. A comparative study of respiratory syncytial virus (RSV) prophylaxis in premature infants within the Canadian Registry of Palivizumab (CARESS). Eur J Clin Microbiol Infect Dis. 2012;31(10):2703–2711. doi:10.1007/s10096-012-1617-7
49. Paes B, Mitchell I, Li A, Lanctôt KL. Respiratory hospitalizations and respiratory syncytial virus prophylaxis in special populations. Eur J Pediatr. 2012;171(5):833–841. doi:10.1007/s00431-011-1654-8
50. Resch B, Bramreiter VS, Kurath-Koller S, et al. Respiratory syncytial virus associated hospitalizations in preterm infants of 29 to 32 weeks gestational age using a risk score tool for palivizumab prophylaxis. Eur J Clin Microbiol Infect Dis. 2017;36(6):1057–1062. doi:10.1007/s10096-016-2891-6
51. Groothuis JR. Safety of palivizumab in preterm infants 29 to 32 weeks’ gestational age without chronic lung disease to prevent serious respiratory syncytial virus infection. Eur J Clin Microbiol Infect Dis. 2003;22(7):414–417. doi:10.1007/s10096-003-0961-z
52. Feltes TF, Cabalka AK, Meissner HC, et al.; Cardiac Synagis Study Group. Palivizumab prophylaxis reduces hospitalization due to respiratory syncytial virus in young children with hemodynamically significant congenital heart disease. J Pediatr. 2003;143(4):532–540. doi:10.1067/S0022-3476(03)00454-2
53. Kua KP, Lee SWH. Systematic review of the safety and efficacy of palivizumab among infants and young children with cystic fibrosis. Pharmacotherapy. 2017;37(6):755–769. doi:10.1002/phar.1936
54. Takeuchi M, Kawakami K. Universal palivizumab prophylaxis for children with Down syndrome in Japan: analysis with interrupted time-series. Hum Vaccin Immunother. 2021;17(4):1235–1238. doi:10.1080/21645515.2020.1809265
55. Sharland M, Cant A, Dagan R, et al. Manual of Childhood Infections (Oxford Specialist Handbooks in Paediatrics): The Blue Book.
56. Blanken MO, Rovers MM, Molenaar JM, et al; Dutch RSV Neonatal Network. Respiratory syncytial virus and recurrent wheeze in healthy preterm infants. N Engl J Med. 2013;368(19):1791–1799. doi:10.1056/NEJMoa1211917
57. Amitai N, Stafler P, Blau H, et al. Palivizumab following extremely premature birth does not affect pulmonary outcomes in adolescents. Chest. 2020;158(2):660–669. doi:10.1016/j.chest.2020.02.075
58. Wang D, Bayliss S, Meads C. Palivizumab for immunoprophylaxis of respiratory syncytial virus (RSV) bronchiolitis in high-risk infants and young children: a systematic review and additional economic modelling of subgroup analyses. Health Technol Assess. 2011;15(5):1–124. doi:10.3310/hta15050
59. Wang D, Cummins C, Bayliss J, Sandercock J, Burls A. Immunoprophylaxis against RSV with palivizumab in children—a systematic review and economic evaluation. Health Technol Assess. 2008;12(36):1–86. doi:10.3310/hta12360
60. Wu H, Pfarr DS, Johnson S, et al. Development of motavizumab, an ultra-potent antibody for the prevention of respiratory syncytial virus infection in the upper and lower respiratory tract. J Mol Biol. 2007;368(3):652–665. doi:10.1016/j.jmb.2007.02.024
61. O’Brien KL, Chandran A, Weatherholtz R, et al. Efficacy of motavizumab for the prevention of respiratory syncytial virus disease in healthy Native American infants: a phase 3 randomised double-blind placebo-controlled trial. Lancet Infect Dis. 2015;15(12):398–1408.
62. Simões EAF, Forleo-Neto E, Geba GP, et al. Suptavumab for the prevention of medically attended respiratory syncytial virus infection in preterm infants. Clin Infect Dis. 2021;73(11):e4400–e4408. doi:10.1093/cid/ciaa951
63. Regeneron. Press Release: Regeneron to discontinue development of suptavumab for respiratory syncytial virus; 2017. Available from: https://investor.regeneron.com/news-releases/news-release-details/regeneron-discontinue-development-suptavumab-respiratory.
64. Domachowske JB, Khan AA, Esser MT, et al. Safety, tolerability and pharmacokinetics of MEDI8897, an extended half-life single-dose respiratory syncytial virus prefusion F-targeting monoclonal antibody administered as a single dose to healthy preterm infants. Pediatr Infect Dis. 2018;37(9):886–892. doi:10.1097/INF.0000000000001916
65. Zhu Q, McLellan JS, Kallewaard NL, et al. A highly potent extended half-life antibody as a potential RSV vaccine surrogate for all infants. Sci Transl Med. 2017;9(388):1928. doi:10.1126/scitranslmed.aaj1928
66. Sandofi. Press Release: European Commission grants first approval worldwide of Beyfortus® (nirsevimab) for prevention of RSV disease in infants; 2022. Available from: https://investor.regeneron.com/news-releases/news-release-details/regeneron-discontinue-development-suptavumab-respiratory.
67. GOV.UK. Independent report. Respiratory Syncytial virus (RSV) immunisation programme: JCVI advice; 2023. Available from: https://www.gov.uk/government/publications/rsv-immunisation-programme-jcvi-advice-7-june-2023/respiratory-syncytial-virus-rsv-immunisation-programme-jcvi-advice-7-june-2023.
68. Griffin MP, Yuan Y, Takas T, et al.; Nirsevimab Study Group. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med. 2020;383(5):415–425. doi:10.1056/NEJMoa1913556
69. Hammitt LL, Dagan R, Yuan Y, et al.; MELODY Study Group. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med. 2022;386(9):837–846. doi:10.1056/NEJMoa2110275
70. St George’s Vaccine Institute (SGVI). Harmonie RSV Study. A Phase IIIb randomised open-label study of nirsevimab (versus no intervention) in preventing hospitalizations due to respiratory syncytial virus in infants (HARMONIE); 2023. Available from: https://vaccine.ac.uk/research/harmonie-study/.
71. Sandofi. Press release: nirsevimab delivers 83% reduction in RSV infant hospitalizations in a real-world clinical trial setting; 2023. Available from: https://www.sanofi.com/en/media-room/press-releases/2023/2023-05-12-08-50-00-2667568.
72. Tang A, Chen Z, Cox KS, et al. A potent broadly neutralizing human RSV antibody targets conserved site IV of the fusion glycoprotein. Nat Commun. 2019;10(1):4153. doi:10.1038/s41467-019-12137-1
73. Maas BM, Lommerse J, Plock N, et al. Forward and reverse translational approaches to predict efficacy of neutralizing respiratory syncytial virus (RSV) antibody prophylaxis. eBioMedicine. 2021;73:6. doi:10.1016/j.ebiom.2021.103651
74. RSV vaccine and mAb snapshot; 2022. Available from: https://www.path.org/resources/rsv-vaccine-and-mab-snapshot/.
75. Papi A, Ison MG, Langley JM, et al; AReSVi-006 Study Group. Respiratory syncytial virus prefusion F Protein vaccine in older adults. N Engl J Med. 2023;388(7):595–608. doi:10.1056/NEJMoa2209604
76. Kampmann B, Madhi SA, Munjal I, et al.; MATISSE Study Group. Bivalent prefusion F vaccine in pregnancy to prevent RSV illness in infants. N Engl J Med. 2023;388(16):1451–1464. doi:10.1056/NEJMoa2216480
77. Boytchev H. Maternal RSV vaccine: further analysis is urged on preterm births. BMJ. 2023;381:1021. doi:10.1136/bmj.p1021
78. GSK. GSK provides further update on Phase III RSV maternal vaccine candidate programme; 2022. Available from: www.gsk.com/en-gb/media/press-releases/gsk-provides-further-update-on-phase-iii-rsv-maternal-vaccine-candidate-programme.
79. FDA. Sponsor briefing document vaccines and related biological products advisory committee meeting date: February 28-March 1, 2023. Available from: www.fda.gov/media/165621/download#page=42.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.