")
Back to Journals » Clinical Ophthalmology » Volume 18
Retrospective Analysis of Factors Related to the Long-Term Recovery of Third, Fourth, and Sixth Cranial Nerve Palsy with Etiologies and Clinical Course in a Tertiary Hospital
Authors Srimanan W , Panyakorn S
Received 11 November 2023
Accepted for publication 5 February 2024
Published 9 February 2024 Volume 2024:18 Pages 441—450
DOI https://doi.org/10.2147/OPTH.S449127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Worapot Srimanan, Somboon Panyakorn
Ophthalmology Division, Phramongkutklao Hospital, Bangkok, Thailand
Correspondence: Worapot Srimanan, Ophthalmology division, Phramongkutklao hospital, 315 Ratchawithi Road, Thung Phayathai Subdistrict, Ratchathewi, Bangkok, Thailand, Tel +662-763-9300, Fax +662-354-9309, Email [email protected]
Purpose: Although various studies have explored the causes and clinical aspects of cranial nerve palsies, there remains a significant gap in understanding the prognostic factors that influence outcomes. In this study, we sought to address this gap by investigating the incidence, etiologies, clinical courses, and factors associated with long-term recovery, with the aim of enhancing the knowledge base in this field and providing valuable insights for improved patient care.
Patients and Methods: This retrospective study evaluated the data gathered from subjects who had third, fourth, and sixth cranial nerve palsy at the ophthalmology outpatient clinic of Phramongkutklao Hospital between April 1, 2012, and April 30, 2022.
Results: Among the three nerves, abducens nerve palsy was the most prevalent finding by most commonly involved. Our study revealed that ischemic and compressive lesions were the most common etiology of oculomotor nerve palsy, comprising 24.6% each. In addition, the most common etiology of trochlear and abducens nerve palsy was trauma, at 31.6% and 27.1%, respectively. Compared with the other nerves, oculomotor nerve palsy was associated with a shorter duration onset of symptoms and recovery period. The best recovery outcomes among the various etiologies were inflammation, ischemic events, and trauma in oculomotor, trochlear, and abducens nerve palsy, respectively. Logistic regression revealed that an onset of < 7 days and isolated nerve involvement were significantly associated with good long-term outcomes, with an adjusted odds ratio of 1.73 (95% confidence interval, 1.03– 2.89) and 2.56 (95% confidence interval, 1.21– 5.39) adjusted for the type of cranial nerve palsy, aged at 50 years, sex, diabetes mellitus, hypertension, dyslipidemia, onset at 7 days, and number of cranial nerves involved, respectively.
Conclusion: The onset of symptoms in less than 1 week and isolated nerve involvement were associated with better prognosis in subjects with third, fourth, and sixth cranial nerve palsy.
Plain Language Summary: This study aimed to fill a gap in our understanding of cranial nerve palsies, which affects eye movements and coordination. We investigated the causes, clinical courses, and factors influencing long-term recovery in patients with third, fourth, and sixth cranial nerve palsy. We studied the data obtained from patients at an ophthalmology clinic over a 10-year period.
Abducens nerve palsy was the most common among these conditions. Ischemia and compression were observed to be the leading causes of oculomotor nerve palsy, whereas trauma was the primary cause of trochlear and abducens nerve palsy. Oculomotor nerve palsy had the shortest onset and recovery time compared with other nerves. The best recovery outcomes were observed in cases of inflammation, ischemic events, and trauma for oculomotor, trochlear, and abducens nerve palsy, respectively.
The study also found that a rapid onset of symptoms in less than 7 days and involvement of only one nerve were associated with better long-term outcomes. This information can help doctors provide better care and more accurate prognoses to patients with cranial nerve palsies.
Keywords: oculomotor, trochlear, abducens, nerve palsy, outcome, prognosis
Introduction
Cranial nerve palsy is a complex neurologic disorder that is characterized by the dysfunction of one or more cranial nerves, and it can vary in clinical presentation and course. Three cranial nerves, namely, oculomotor, trochlear, and abducens nerves, are vital in controlling eye movements. Their dysfunction can result in an imbalance in ocular control, resulting in binocular diplopia. As evidenced by various reports in the literature, the incidence of cranial nerve palsy varies among different regions.1–18 Recent reports have indicated that the incidence rates of third, fourth, and sixth cranial nerve palsy among the Korean population are 3.71, 5.73, and 4.66 per 100,000 per year, respectively.12,14,15 These rates exhibit an age-dependent increase, accelerating notably after individuals reach 60 years of age. It is also noteworthy that these incidence rates are comparatively lower than those reported in the United States.13,18 The causes of these nerve palsies are diverse, encompassing ischemic events, trauma, aneurysms, and compressive lesions.1–18 Intriguingly, the distribution of etiological factors can vary, even within the same institution across different time frames.1–4 Moreover, the underlying etiology of these palsies is notably influenced by their clinical course, leading to a spectrum of outcomes that range from complete recovery to a lack of improvement.1,4–6
Recent population-based studies have provided valuable insights into the etiologies of cranial nerve palsies. Oculomotor nerve palsy is predominantly attributed to microvascular causes, particularly in older adults.12,13 Pupillary involvement, although not specific to compressive lesions, is relatively rare.12,13 In the case of trochlear nerve palsy, evidence has revealed a bimodal distribution, with congenital factors prevalent in early childhood and vascular etiology more common in adults.14 In younger and adolescent patients, cranial nerve palsy typically has nonvascular origins. A retrospective series highlighted the prevalence of tumor-related causes in this demographic.8 However, the population-based literature often highlights a primarily congenital basis.16 High-resolution neuroimaging is pivotal in pathology demonstration and diagnostic support.8,17 Treatment modalities are tailored to the specific etiologies and are aimed at alleviating sequelae through interventions such as prism glasses, botulinum toxin, or strabismus surgery.
Understanding the natural progression of these conditions is vital for guiding clinical decisions and providing appropriate patient care. However, there is a current gap in the literature on the prognostic factors that affect the recovery rate.10 Investigating these factors allows for a comprehensive assessment of patient outcomes and provides valuable insights into optimizing management strategies for these neuro-ophthalmologic conditions.
In this study, we aim to report the etiologies, clinical courses, and factors associated with good prognosis in a tertiary referral hospital. Furthermore, we conducted a literature review to compare our study with previous reports.
Materials and Methods
Study Participants
We analyzed the data/hospital records of patients who underwent treatment for cranial palsy in an inpatient/outpatient clinic at Phramongkutklao Hospital between April 1, 2012 and April 30, 2022. We included subjects who visited the ophthalmology clinic at least four times in a year with all recorded data available, and we excluded subjects who visited the clinic fewer than four times in a year and who had incompletely recorded data.
We recruited 297 subjects with oculomotor nerve palsy, 152 cases of trochlear nerve palsy, and 338 cases of abducens nerve palsy. After excluding patients with incomplete data, the overall numbers of subjects included in the analysis were 65 cases of oculomotor nerve palsy, 57 cases of trochlear nerve palsy, and 176 cases of abducens nerve palsy, respectively.
This study was retrospective in nature and approved by the Institutional Review Board of the Royal Thai Army (approval No. S027h/66_Exp).
Disease Definition
Oculomotor nerve palsy is defined as any presentation resulting from weakness of the oculomotor nerve, including exotropia, vertical misalignment, and ptosis with or without pupillary involvement. Trochlear nerve palsy is defined as any presentation that results from a weakness of the trochlear nerve, including vertical or torsional diplopia. Abducens nerve palsy is defined as any presentation resulting from weakness of the abducens nerve, including incomitant esotropia. The onset of symptoms refers to the duration between the onset of symptoms and the initial visit to the hospital. Oral corticosteroids are prescribed for treating inflammatory causes at our institution at a dose of 1 mg/kg per day for at least 2 weeks and a slower taper, depending on the case. There is no given treatment for ischemic etiology. Complete recovery is defined as the resolution of presenting signs and symptoms of the affected subjects. The entire ocular duction with orthotropia in the primary position is reserved for complete recovery of an ocular sign. An absence of clinical double vision was the favorable endpoint of symptoms. Partial recovery is defined as residual signs and symptoms at the endpoint.
Data Gathered
We conducted a search of outpatient and inpatient data using the following ICD-10 codes: H49.0 for oculomotor nerve palsy, H49.1 for trochlear nerve palsy, and H49.2 for abducens nerve palsy. The data gathered included patient sex, age, underlying condition, laterality, number of involvements, etiologies, symptoms, manifestation, onset, neuroimaging, recovery period, and surgical treatment. We initially extracted imaging parameters from official radiologic reports that were subsequently reviewed by a single neuroradiologist.
Statistical Analysis
We used descriptive statistics for the basic data on the sample group obtained from the general data. The group data were also analyzed in terms of the amount and percentage of quantitative data. For a normal distribution, the mean was measured along with the mean and standard deviation. For irregular distribution, the average value was summed with the median. Numbers and percentages represent clustered data. The two-proportion z-test is a statistical procedure used to compare the proportions of two independent groups.
We used logistic regression to estimate the independent factors associated with good recovery. The subjects were categorized into two age groups: younger (<50 years) and older (≥50 years). The onset was classified as early (<7 days) and late (≥7 days) clinical symptoms. In the multivariate logistic regression, we adjusted type of cranial nerve palsy, age at 50 years, sex, diabetes mellitus, hypertension, dyslipidemia, onset at 7 days, and number of cranial nerve involvement as potential factors for favorable outcomes.
The information was validated and recorded in a data file in the STATA/MP 12 program and then analyzed. We used SPSS for all statistical analyses. For all tests, p< 0.05 was considered significant.
Results
Patient Demographics
Our study included 65 patients with oculomotor nerve palsy, 58 subjects with trochlear nerve palsy, and 177 with abducens nerve palsy. Table 1 presents the demographic data.
 |
Table 1 Demographic Data of Cranial Nerve Palsy |
Oculomotor Nerve Palsy
Subjects with oculomotor nerve palsy had a mean age of 50.34 years. The onset of palsy was approximately 14 days. Most subjects had unilateral and isolated nerve palsy. The most common etiologies were ischemic and compressive. The complete recovery rate of oculomotor nerve palsy was 35.4% and for those receiving strabismus surgery was 10.8%. In cases with full recovery, the average duration was 4.74 months.
Trochlear Nerve Palsy
The average age of patients with trochlear nerve palsy was 54.75 years, with a median onset of 90 days. Most subjects had unilateral and isolated involvement. The rate of acquired trochlear nerve palsy was 73.7%. Trauma was the most common etiology in this set of patients. Idiopathic etiology was ranked second. In this group, 26.3% had complete recovery and 21.1% received strabismus surgery due to inferior oblique muscle weakening. Among these groups, the average duration of recovery was 5.39 months.
Abducens Nerve Palsy
Abducens nerve palsy was the most common palsy among the three groups. The average age of the subjects was 48.71 years, with a mean onset of 84.25 days. Most subjects had unilateral and isolated involvement. Traumatic causes were the most common etiology in this population. The second and third most common etiologies were inflammation and ischemic, respectively. In our population, 44.1% had complete recovery and 14.3% received strabismus surgery. The average recovery time was 4.76 months.
Etiologies Correlation with Recovery Rate
Among the various etiologies of nerve palsy, our study showed that inflammation had the best recovery rate in oculomotor nerve palsy as shown in Table 2, patients experiencing ischemic events had the best recovery in trochlear nerve palsy and trauma in abducens nerve palsy. Among the groups, the two proportions revealed traumatic causes in trochlear nerve palsy, which had a statistically significant difference compared with abducens nerve (p = 0.00). Comparatively, there was a considerable difference in idiopathic etiology between trochlear nerve palsy and oculomotor and abducens nerve, with p values of 0.001 and 0.026, respectively.
 |
Table 2 Recovery Rates by Etiology |
As shown in Table 3, we combined the three nerve palsy groups for logistic regression analysis. Our study revealed that an early onset of <7 days and isolated cranial nerve palsy were significantly associated with complete recovery at an adjusted odds ratio of 1.73 (95% confidence interval, 1.03–2.89) and 2.56 (95% confidence interval, 1.21–5.39), respectively.
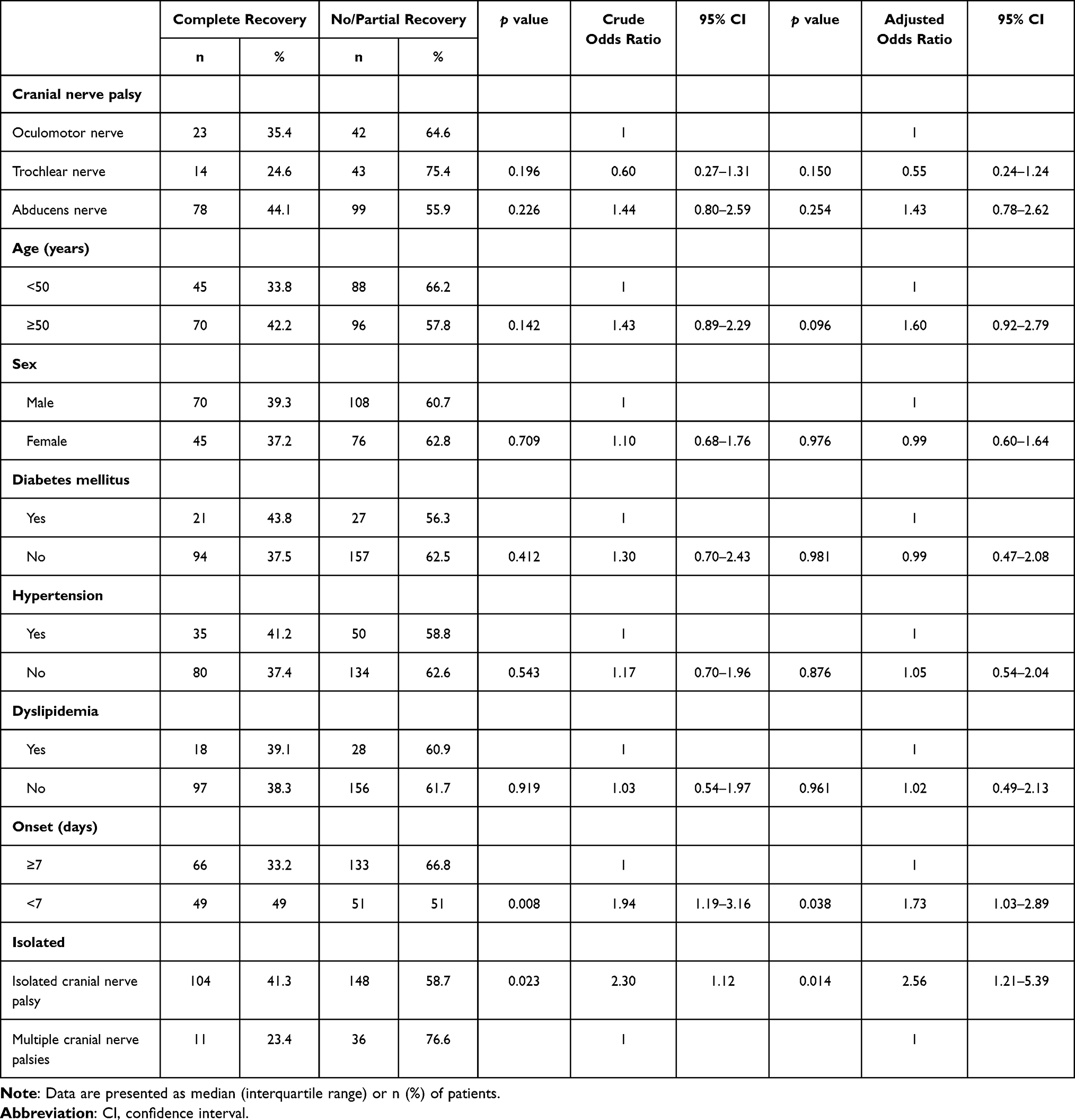 |
Table 3 Logistic Regression of Factors Associated with Complete Recovery of Cranial Nerve Palsy |
Discussion
Cranial nerves 3, 4, and 6 supply extraocular muscle movement. Their pathology affects both the motor and autonomic nervous systems. In an analysis of existing research on the long-term outcomes of third, fourth, and sixth cranial nerve palsy, we found a diverse landscape of research findings.1–18
Our data corroborates those of previous studies, indicating that abducens nerve palsy is the most frequently encountered among the three nerves,1–6,8,10,11,18 whereas trochlear nerve palsy exhibits a lower prevalence.1–6,8,10 However, recently reported incidence rates in the Korean population present a different perspective, with trochlear nerve palsy being the most common and oculomotor nerve palsy the least common.12,14 These regional disparities underscore the significance of geographic factors in the distribution of cranial nerve palsies and emphasize the need for clinical evaluations and research to consider such variations.12,14
We conducted a literature review on the etiologies of oculomotor, trochlear, and abducens nerve palsy, categorized according to the most extensive literature reviews of 4278 subjects from the previous study1 (Table 4). The etiologies varied across the studies for many reasons. First, the evolution in investigation lessens the undetermined etiology. Second, studies in different regions may reflect other disease distributions. Finally, even at the same institution, different data collection times led to various etiologies,1–4 implying an actual change.
 |
Table 4 Compared Etiologies of Isolated Third, Fourth, and Sixth Cranial Nerve Palsy (%) |
Our data showed that the overall recovery rate was 38.5%, which is comparable with previous reports (range, 38–80%).1,4–6 The recovery rate varied across studies due to data collection methods. Moreover, the rate depended on the criteria used for recovery measurement. Some studies used follow-up letters or telephone calls to collect data,1,4 which might not accurately reflect total recovery. In our research, ophthalmologists evaluated all patients, asked for symptoms, and measured ocular deviation at every visit, which might have resulted in excellent reliability regarding accurate recovery.
According to the etiology of cranial nerve palsy, microvascular had a good recovery rate,1,4,6,7 whereas compressive lesions, especially tumors, had the worst prognosis in the previous studies.1,4,7 Our results support the good recovery in ischemic cases, which had a >50% chance of recovery. In addition, the best prognosis was observed for the inflammatory cause of trochlear nerve palsy, among other reasons, and the traumatic cause had the most remarkable recovery rate in abducens nerve palsy. Among the groups, the two proportions with a traumatic cause in abducens nerve palsy had a better prognosis than those with a trochlear nerve cause. In comparison, idiopathic etiology was associated with a better prognosis in trochlear nerve palsy than others.
With regard to underlying conditions, controversy exists as to whether diabetes mellitus and hypertension are associated with cranial nerve palsy. Several studies have supported that these underlying conditions are risk factors of acquired nerve palsies.18–22 Despite the increased risks, they were not associated with outcomes.19,22 Our study demonstrated no correlation between the rate of cranial nerve palsy recovery and diabetes and hypertension.
Only a few studies identified factors associated with good prognosis. Park et al10 retrospectively reviewed 206 subjects with acquired cranial third, fourth, and sixth palsy from July 1998 to February 2005 at Seoul National University Hospital. They found that sixth cranial nerve palsy was affected most frequently in 52.4% of cases. Vascular disease was the most common etiology at 31.1%, whereas 85.2% of patients showed overall (at least partial) recovery and 67.6% complete recovery. In the study, multivariate logistic regression indicated that minor initial ocular deviation and treatable etiologies were associated with good recovery. The objective measurement of ocular deviation was key in determining recovery from palsy, as in our research.
Kim et al7 retrospectively reported on 153 patients diagnosed with paralytic strabismus, showing that vascular-related causes were the most common at 54.9%. The idiopathic cause had the best recovery rate of 50% within 3 months, and the Cox proportional hazard analysis revealed a significant association between baseline prism diopter and recovery rate.
Many reasons support the association between a short onset of presentation and good prognosis. First, it may reflect the cause of abrupt changes in nerve function, such as inflammation, ischemia, or infection, which can be reversible or treatable. Second, early onset may reflect early detection and subsequent intervention, leading to significant improvement or complete resolution of symptoms. Third, early intervention may improve neural plasticity, which offers a better chance of function regeneration and restoration. Fourth, a short onset may lower the risk of complications arising from chronic or long-standing conditions, such as muscle contracture. Finally, patients with recent onset may be more motivated to adhere to treatment plans and follow-up appointments, resulting in a positive influence on prognosis. In this study, early onset before 7 days was significantly associated with good recovery (odds ratio 1.73; 95% confidence interval, 1.03–2.89). Urgent visits and prompt treatment of these conditions may affect the excellent recovery rate.
For various reasons, involvement of multiple cranial nerves can result in poor outcomes. At first, multiple cranial nerve palsy resulted from a wide range of complicated etiologies, such as systemic diseases, autoimmunity, infection, or tumor.23 The complexity of addressing these underlying conditions can make management challenging and influence prognosis. Second, multiple cranial nerve palsies often signify more extensive nerve damage or a lesion affecting multiple nerve pathways. The extent of neurologic involvement can lead to more profound and lasting deficits. Finally, the simultaneous involvement of multiple cranial nerves may reduce the likelihood of complete recovery, especially if the underlying cause is severe or not readily treatable. Our study indicated that isolated cranial nerve involvement led to good outcomes (odds ratio 2.56; 95% confidence interval, 1.21–5.39). Extensive etiologies might require complicated treatment, affecting unfavorable clinical outcomes.
Limitations
This study has several limitations. First, this study had a retrospective design. The neuroimaging protocol was inconsistent across all subjects, with variations based on clinical presentations. Second, a selection bias may exist. The patient source primarily consisted of referrals to a tertiary hospital, potentially leading to an overrepresentation of severe underlying pathologies in our research. Due to differences in referral patterns, this might influence the prevalence of specific etiologies related to third, fourth, and sixth cranial nerve palsies, such as those resulting from trauma. Third, because all data were collected from a single center, predominantly from patients with one ethnicity, it is crucial to exercise caution when applying these findings directly to other racial or ethnic groups.
Future research should focus on uncovering additional prognostic factors for cranial nerve palsies. Exploring advanced neuroimaging and biomarkers may refine our understanding of etiological subtypes and therapies. Collaborative, multicenter studies can enhance the applicability of the findings, ultimately optimizing patient care and long-term recovery for those with cranial nerve palsies.
Conclusion
Abducens nerve palsy was the most common palsy, and oculomotor nerve palsy had the shortest onset and recovery period. Complete recovery was associated with an onset of <7 days and isolated cranial nerve palsy. Further research may identify additional factors influencing good outcomes, ultimately improving patient care and recovery prospects.
Abbreviations
ICD, International Classification of Diseases; STATA/MP, Multiprocessor Version of Statistic and Data; SPSS, Statistical Package for the Social Sciences.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of Royal Thai Army (No. S027h/66_Exp). This study was performed in accordance with the principles stated in the Declaration of Helsinki. Because this was a retrospective study, the Institutional Review Board waived the need for informed consent. We confirm that the data were anonymized and maintained with confidentiality.
Acknowledgments
We extend our foremost gratitude to our supervisor, Dr. Ornwasee Jatuthong, whose invaluable guidance and unwavering support profoundly influenced our research trajectory. Dr. Jatuthong’s expertise and insights played a pivotal role in shaping the direction and emphasis of our study. Furthermore, we express our appreciation to the ophthalmology division of Phramongkutklao Hospital for their generous provision of resources and unyielding support, which proved indispensable in the successful completion of our project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval to the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Richards BW, Jones FR, Younge BR. Causes and prognosis in 4278 cases of paralysis of the oculomotor, trochlear, and abducens cranial nerves. Am J Ophthalmol. 1992;113(5):489–496. doi:10.1016/S0002-9394(14)74718-X
2. Rucker CW. Paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol. 1958;46(6):787–794. doi:10.1016/0002-9394(58)90989-9
3. Rucker CW. The causes of paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol. 1966;61(5 Pt 2):1293–1298. doi:10.1016/0002-9394(66)90258-3
4. Rush JA, Younge BR. Paralysis of cranial nerves III, IV, and VI. Cause and prognosis in 1000 cases. Arch Ophthalmol. 1981;99(1):76–79. doi:10.1001/archopht.1981.03930010078006
5. Tiffin PA, MacEwen CJ, Craig EA, Clayton G. Acquired palsy of the oculomotor, trochlear and abducens nerves. Eye. 1996;10(3):377–384. doi:10.1038/eye.1996.77
6. Berlit P. Isolated and combined pareses of cranial nerves III, IV and VI a retrospective study of 412 patients. J Neurol Sci. 1991;103(1):10–15. doi:10.1016/0022-510X(91)90276-D
7. Kim K, Noh SR, Kang MS, Jin KH. Clinical course and prognostic factors of acquired third, fourth, and sixth cranial nerve palsy in Korean patients. Korean J Ophthalmol. 2018;32(3):221–227. doi:10.3341/kjo.2017.0051
8. Park KA, Oh SY, Min JH, Kim BJ, Kim Y. Acquired onset of third, fourth, and sixth cranial nerve palsies in children and adolescents. Eye. 2019;33(6):965–973. doi:10.1038/s41433-019-0353-y
9. de Camargo GB, Hida WT, Goldchmit M, Uesugui CF, de Souza-Dias CR. Estrabismo paralítico: revisão de 24 anos da Santa Casa de São Paulo [Paralytic strabismus: review of 24 years at “Santa Casa de São Paulo”]. Arq Bras Oftalmol. 2007;70(4):585–587. Portuguese. doi:10.1590/S0004-27492007000400005
10. Park UC, Kim SJ, Hwang JM, Yu YS. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye. 2008;22(5):691–696. doi:10.1038/sj.eye.6702720
11. Tamhankar MA, Biousse V, Ying GS, et al. Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: a prospective study. Ophthalmology. 2013;120(11):2264–2269. doi:10.1016/j.ophtha.2013.04.009
12. Jung EH, Kim SJ, Lee JY, Cho BJ. The incidence and etiologies of third cranial nerve palsy in Koreans: a 10-year nationwide cohort study. Ophthal Epidemiol. 2020;27(6):460–467. doi:10.1080/09286586.2020.1773870
13. Fang C, Leavitt JA, Hodge DO, Holmes JM, Mohney BG, Chen JJ. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135(1):23–28. doi:10.1001/jamaophthalmol.2016.4456
14. Jung EH, Kim SJ, Lee JY, Cho BJ. The incidence and presumed aetiologies of fourth cranial nerve palsy in Korea: a 10-year nationwide cohort study. Eye. 2021;35(11):3012–3019. doi:10.1038/s41433-020-01374-0
15. Jung EH, Kim SJ, Lee JY, Cho BJ. The incidence and etiology of sixth cranial nerve palsy in Koreans: a 10-year nationwide cohort study. Sci Rep. 2019;9(1):18419. doi:10.1038/s41598-019-54975-5
16. Holmes JM, Mutyala S, Maus TL, Grill R, Hodge DO, Gray DT. Pediatric third, fourth, and sixth nerve palsies: a population-based study. Am J Ophthalmol. 1999;127(4):388–392. doi:10.1016/S0002-9394(98)00424-3
17. Park KA, Oh SY, Min JH, Kim BJ, Kim Y. Cause of acquired onset of diplopia due to isolated third, fourth, and sixth cranial nerve palsies in patients aged 20 to 50 years in Korea: a high resolution magnetic resonance imaging study. J Neurol Sci. 2019;407:116546. doi:10.1016/j.jns.2019.116546
18. Patel SV, Holmes JM, Hodge DO, Burke JP. Diabetes and hypertension in isolated sixth nerve palsy: a population-based study. Ophthalmology. 2005;112(5):760–763. doi:10.1016/j.ophtha.2004.11.057
19. Sanders SK, Kawasaki A, Purvin VA. Long-term prognosis in patients with vasculopathic sixth nerve palsy. Am J Ophthalmol. 2002;134(1):81–84. doi:10.1016/S0002-9394(02)01439-3
20. Choung HK, Chang BL. Clinical features of ischemic ophthalmoplegia caused by diabetes mellitus or hypertension. J Korean Ophthalmol Soc. 2002;43:131–135.
21. Jacobson DM, McCanna TD, Layde PM. Risk factors for ischemic ocular motor nerve palsies. Arch Ophthalmol. 1994;112(7):961–966. doi:10.1001/archopht.1994.01090190109029
22. Ho TH, Lin HS, Lin MC, Sheu SJ. Acquired paralytic strabismus in Southern Taiwan. J Chin Med Assoc. 2013;76(6):340–343. doi:10.1016/j.jcma.2013.03.003
23. Keane JR. Multiple cranial nerve palsies: analysis of 979 cases. Arch Neurol. 2005;62(11):1714–1717. doi:10.1001/archneur.62.11.1714
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.