")
Back to Journals » Integrated Blood Pressure Control » Volume 17
Resistance Training in Cardiovascular Diseases: A Review on Its Effectiveness in Controlling Risk Factors
Authors Nazir A , Heryaman H, Juli C, Ugusman A, Martha JW, Moeliono MA, Atik N
Received 9 November 2023
Accepted for publication 6 March 2024
Published 18 March 2024 Volume 2024:17 Pages 21—37
DOI https://doi.org/10.2147/IBPC.S449086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Turgay Celik
Arnengsih Nazir,1,2 Henhen Heryaman,1,3 Cep Juli,4 Azizah Ugusman,5 Januar Wibawa Martha,6 Marina Annette Moeliono,2 Nur Atik3
1Doctoral Program, Faculty of Medicine, Padjadjaran University, Bandung, WJ, Indonesia; 2Department of Physical and Rehabilitation Medicine, Dr. Hasan Sadikin General Hospital/Faculty of Medicine, Padjadjaran University, Bandung, WJ, Indonesia; 3Department of Biomedical Sciences, Faculty of Medicine, Padjadjaran University, Bandung, WJ, Indonesia; 4Department of Neurology, Dr. Hasan Sadikin General Hospital/Faculty of Medicine Padjadjaran University, Bandung, WJ, Indonesia; 5Department of Physiology, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 6Department of Cardiology and Vascular Medicine, Faculty of Medicine, Padjadjaran University, Bandung, WJ, Indonesia
Correspondence: Nur Atik, Department of Biomedical Sciences, Faculty of Medicine, Padjadjaran University, Jl. Prof. Eijkman No. 38, Bandung, WJ, 40161, Indonesia, Tel +62 81280956825, Email [email protected]
Abstract: Cardiovascular Disease (CVD), a term encompassing various disorders affecting the heart and blood vessels, includes coronary artery disease (CAD). CAD is primarily due to the development of atherosclerotic plaques that disrupt blood flow, oxygenation, and nutrient delivery to the myocardium. Risk factors contributing to CAD progression include smoking, hypertension, diabetes mellitus (DM), dyslipidaemia, and obesity. While aerobic exercise (AE) has shown promising results in controlling CVD risk factors, the impact of resistance training (RT) has not been extensively investigated. This review aims to describe the effects of RT on CVD risk factors based on studies retrieved from PubMed and Google Scholar databases. Both isometric and isotonic RT have been found to decrease systolic blood pressure (SBP), diastolic blood pressure, or mean arterial pressure, with SBP showing a more significant reduction. Hypertensive patients engaging in RT alongside a calorie-restricted diet demonstrated significant improvements in blood pressure. RT is associated with increased nitric oxide bioavailability, sympathetic modulation, and enhanced endothelial function. In type-2 DM patients, 8– 12 weeks of RT led to improvements in fasting blood glucose levels, insulin secretion, metabolic syndrome risk, and glucose transporter numbers. Combining AE with RT had a more significant impact in reducing insulin resistance and enhancing blood glucose compared to performing exercises separately. It also significantly decreased total cholesterol, triglycerides, and low-density lipoprotein levels while increasing high-density lipoprotein within 12 weeks of application. However, improvements are considered insignificant when lipid levels are already low to normal at baseline. The administration of RT resulted in weight loss and improved body mass index, with more pronounced effects seen when combining AE with RT and a calorie-restricted diet. Considering these results, the administration of RT, either alone or in combination with AE, proves beneficial in rehabilitating CAD patients by improving various risk factors.
Keywords: coronary artery disease, dyslipidaemia, exercise, Hypertension, obesity, type 2 diabetes mellitus
Introduction
Cardiovascular Disease (CVD) is a broad term that encompasses various disorders affecting the heart and blood vessels. One prominent condition within this category is coronary artery disease (CAD), which plays a significant role in CVD-related mortality. 1,2 CAD occurs due to disruption of blood supply, oxygenation, and nutrients to the heart muscles, primarily caused by the accumulation of fatty deposits within the walls of the coronary artery, a condition known as atherosclerosis. Several key risk factors contribute to the formation of atherosclerosis, including smoking, hypertension, diabetes mellitus (DM), dyslipidaemia, obesity, physical inactivity, and stress.3–7
Previous studies had reported the detrimental impact of a sedentary lifestyle on the prevalence of CAD and the associated risk factors for CVD.4,7,8 In particular, Type 2 DM and obesity are recognized as significant indicators to initiate exercise-based cardiac rehabilitation (CR) programs, which serve as strategies to effectively manage CVD risk factors.9,10
Aerobic exercise (AE) is the primary modality employed in CR, as it induces physiological changes in cardiovascular, respiratory, and metabolic systems.11,12 A large body of literature has been produced to investigate the role of AE in effectively managing CVD risk factors, yielding satisfactory outcomes.8,13–16 Aerobic exercise has been proven effective in lowering CVD risk factors by reducing resting blood pressure (BP), increasing insulin sensitivity and glycaemic control, improving lipid profile, decreasing body weight, and improving body composition.13,16
Resistance training (RT) is another modality employed in CR, which can be given as a single exercise or in combination with AE. This combination has been found to produce better results compared to the single application of AE.17–21 It was demonstrated in a study by Chen et al to have a positive effect on body mass index (BMI), body fat, triglycerides, low-density lipoprotein (LDL), and total cholesterol in school-age children who were obese or overweight.21 Schroeder et al found that the combination of AE-RT decreased diastolic blood pressure (DBP) and increased lean body mass.17 Previous reviews mostly synthesized data related to the effects of resistance training (RT) on hypertension risk factors.22–25 Another review examined the impact of RT on blood pressure (BP) and cholesterol.26 Only one review assessed the effects of RT on various cardiovascular disease (CVD) risk factors, including hypertension, diabetes mellitus (DM), and dyslipidaemia.27 Major CVD risk factors often coexist, and in developing countries like Indonesia, hypertension, DM, hyperlipidaemia, obesity, and smoking are major CVD risk factors with continuously increasing prevalence.28–30 Therefore, this review aims to describe the effects of RT on CVD risk factors, focusing on hypertension, DM, dyslipidaemia, and obesity, to enrich previous reviews on this topic.
Methods
Articles published in the last ten years were searched using PubMed and Google Scholar databases. Original articles and systematic reviews and meta-analyses were included. Keywords used were “cardiovascular diseases”, “coronary artery disease”, “hypertension”, “diabetes mellitus”, “dyslipidaemia”, “obesity” or “overweight”, “blood pressure”, “blood glucose”, “lipid profile”, “cholesterol”, “trygliseride”, “low-density lipoprotein” or “LDL”, “high-density lipoprotein” or “HDL”, “weight loss”, “body mass index”, “cardiac rehabilitation”, “exercise”, “exercise-based cardiac rehabilitation”, “resistance exercise”, “resistance training”, and “weight training”. Articles were excluded if did not publish in English language and not available in full text.
Results and Discussion
The database search retrieved 13 articles consisting of seven original articles and six systematic reviews and meta-analysis (Figure 1). These articles were extracted and presented in the form of text and table.
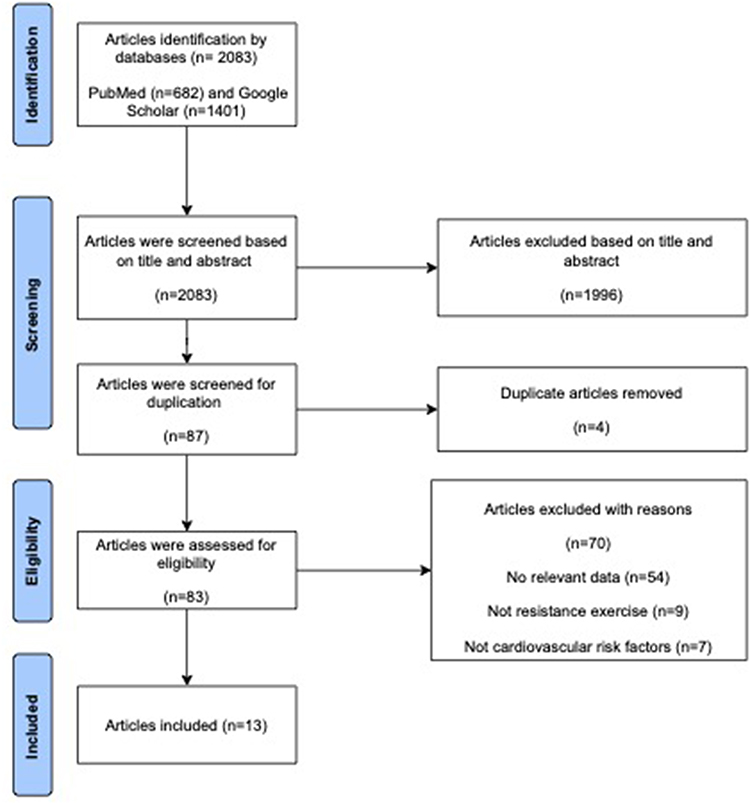 |
Figure 1 PRISMA Flow Chart. Schematic representation of the identification process for studies through databases and registers. |
RT in CVD
Objective of RT
The overall objectives of RT programs for healthy adults across all age groups include: 1) improving performance in activities of daily living, such that it can be conducted without causing physiological stress; and 2) managing or preventing chronic disease and conditions such as type 2 DM, osteoporosis, and obesity.31 In the CR program, the primary purpose of providing RT, especially strength training, is to optimize muscle mass and strength. This is usually achieved through high-intensity muscle strength training.32
Contraindications
RT can be given as a single exercise or in combination with AE. The absolute and relative contraindications of RT in CVD patients are described in Table 1.31,33–35 Several studies have considered that RT should be avoided in CVD or CAD patients when conditions such as complex ventricular arrhythmias, myocardial infarction or percutaneous coronary intervention in the past month, left ventricular ejection fraction <40%, history of ventricular aneurysms or aortic conditions, and comorbidities such as lung or chronic kidney disease.33,36 Therefore, the administration of RT in this group of patients needs further investigation.
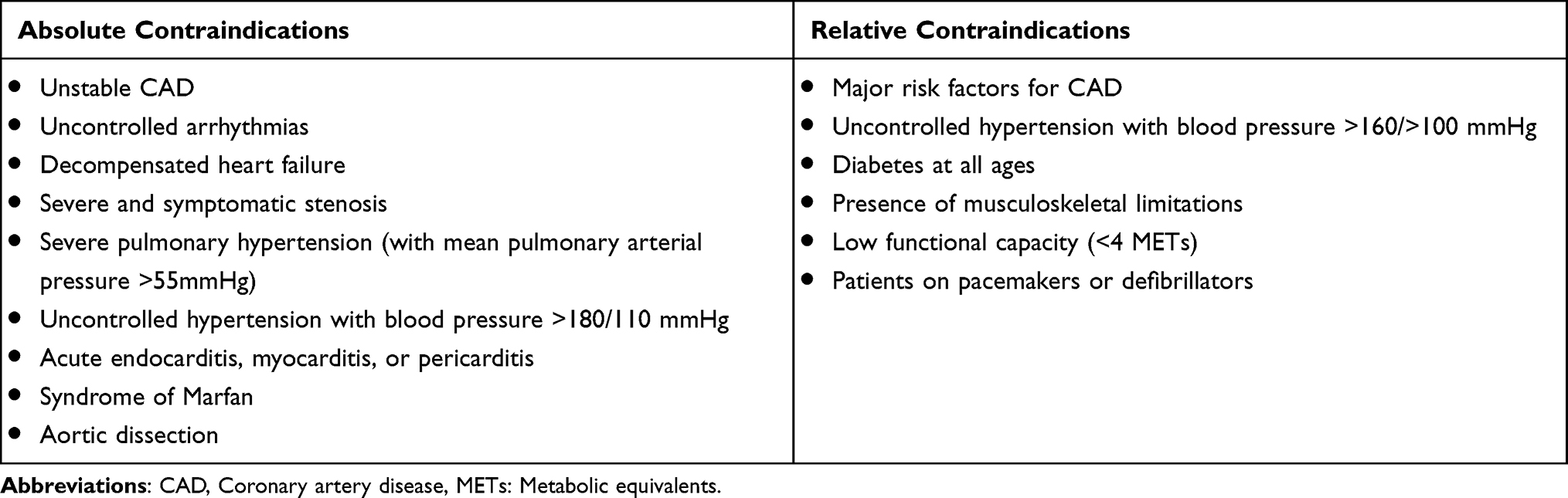 |
Table 1 Absolute and Relative Contraindications Aerobic and Resistance Exercises in Cardiovascular Diseases |
Recommendation of RT Prescription
The American College of Sports Medicine (ACSM) provides recommendations for RT prescription. Specific parameters in patients with heart failure, sternotomy, and peripheral arterial disease are also described (Table 2). 31 Previous studies were given RT in the form of single exercise or in combination with AE for 4–12 weeks (Table 3).
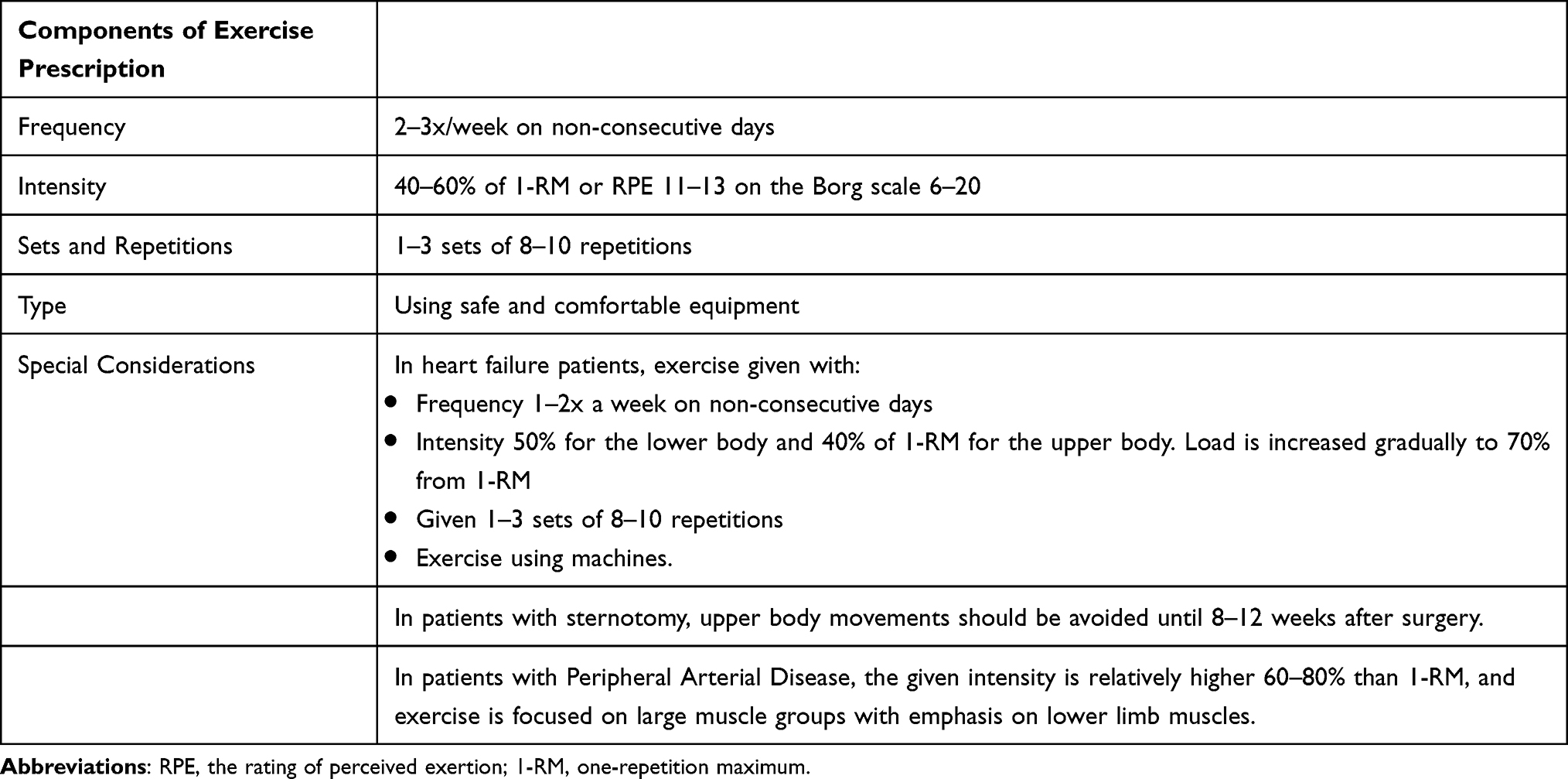 |
Table 2 Recommendation of Resistance Training Prescription in Cardiovascular Diseases Patients |
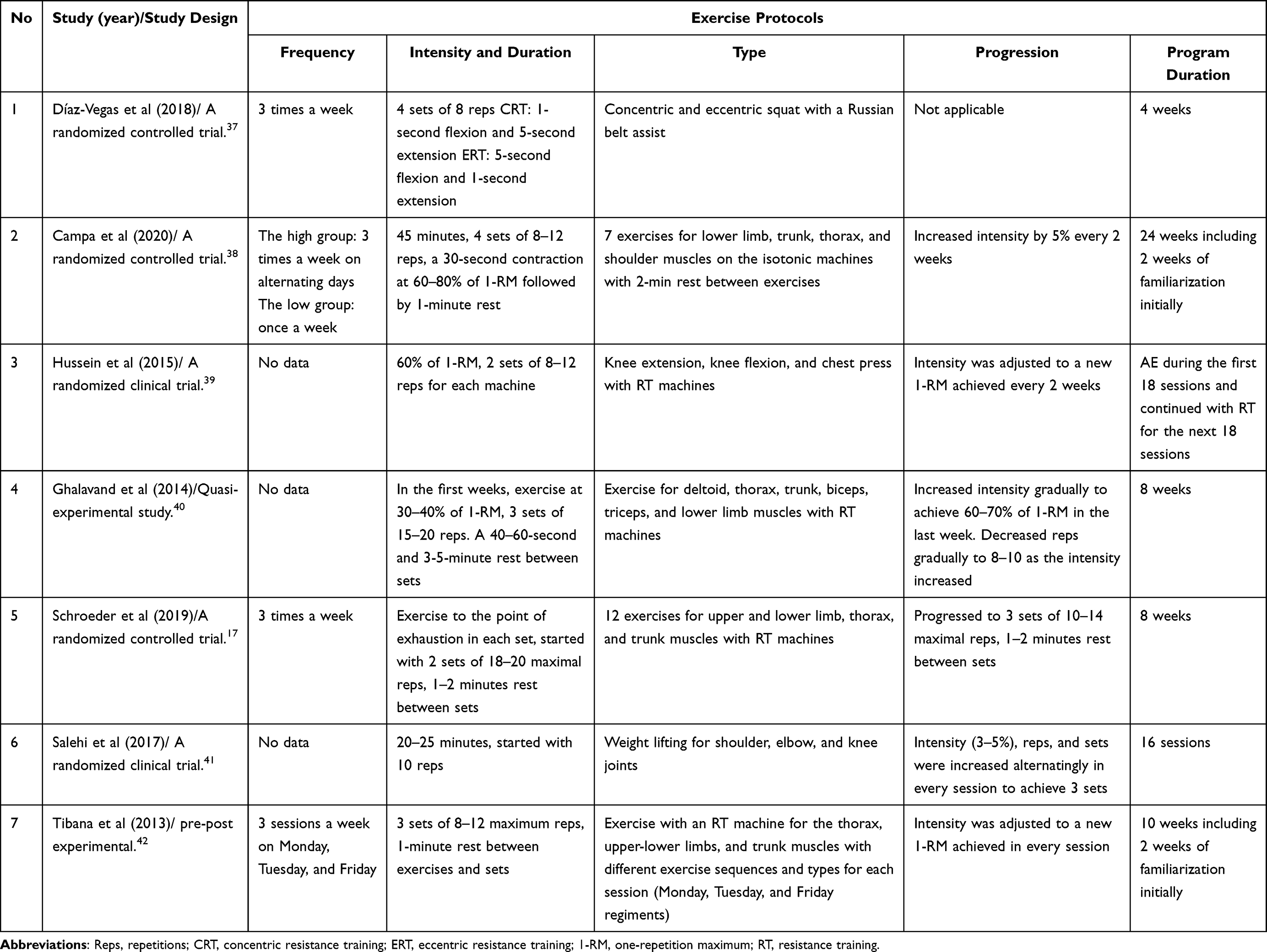 |
Table 3 Exercise Protocols Used in Previous Studies |
Safety Issues in Providing RT in CVD Patients
Previous studies showed that the administration of RT alone or in combination with AE, even at high intensity did not cause significant adverse events. The primary concern when providing RT to CVD patients is the potential for excessive changes in BP, heart rate, and symptoms that could lead to loss of consciousness.32,43–46 Based on several studies, safety issues or exercise side effects that have been reported in CVD patients include 1) light headedness for a few seconds, without vertigo or loss of consciousness, muscle fatigue, and shortness of breath that disappears before starting the next set, 2) musculoskeletal discomforts such as lower back pain, elbow tendonitis, shoulder pain, and hypotension, as well as 3) musculoskeletal complications such as exacerbation of knee arthritis.43–45 The risk of cardiac events was not found in light- or even high-intensity RT.32,45
To prevent adverse events when prescribing exercise, several measures can be taken, including appropriate exercise preparation, prevention of the Valsalva maneuver, adequate exercise supervision, and consideration of functional capacity or muscle strength.31,36,44,47,48 Preparations before starting RT include: 1) refraining from consuming caffeinated or alcoholic beverages and other stimulants; 2) abstaining from intense physical activity for 24 hours before the test or exercise; 3) ensuring adequate sleep the night before exercise, and 4) eating at least 2 hours before exercise.36
Valsalva maneuver during RT can lead to an elevation in intra-thoracic pressure and subsequently affect BP. A study found that during knee extension exercise at a 100% intensity of one-repetition maximum (1-RM), BP reached 311/284 mmHg. However, when it is performed at the same intensity but with slow expiration, the increase in BP was limited to 198/175 mmHg.48 To prevent the occurrence of the Valsalva maneuver, subjects can be instructed to exhale and inhale during the concentric and eccentric phases, respectively, execute slow movements, and ensure a sufficient warm-up is performed.35,36
Supervision of RT can be conducted by various professionals, including exercise specialists, physical therapists, cardiac nurses, and rehabilitation staff.49 The primary objective is to determine the right type of exercise, guide patients during their workouts, enable them to progressively enhance their tolerance levels without compromising safety, and ensure the achievement of exercise goals.44,50 Before starting RT, it is recommended to have a minimum level of cardiorespiratory fitness of 5 metabolic equivalents (METs) as determined through exercise testing or 4 METs based on a questionnaire.47,51
Effect of RT on CVD Risk Factors
Effect of RT on BP in Hypertensive Patients
Previous studies that investigated the effect of RT on BP had generally shown a reduction in BP.22,23,25,27 This decrease depends on the type and prescription of exercise. Dynamic RT affects BP acutely, but the chronic influence of its eccentric counterpart on CVD risk factors has not been studied (Table 4). 37
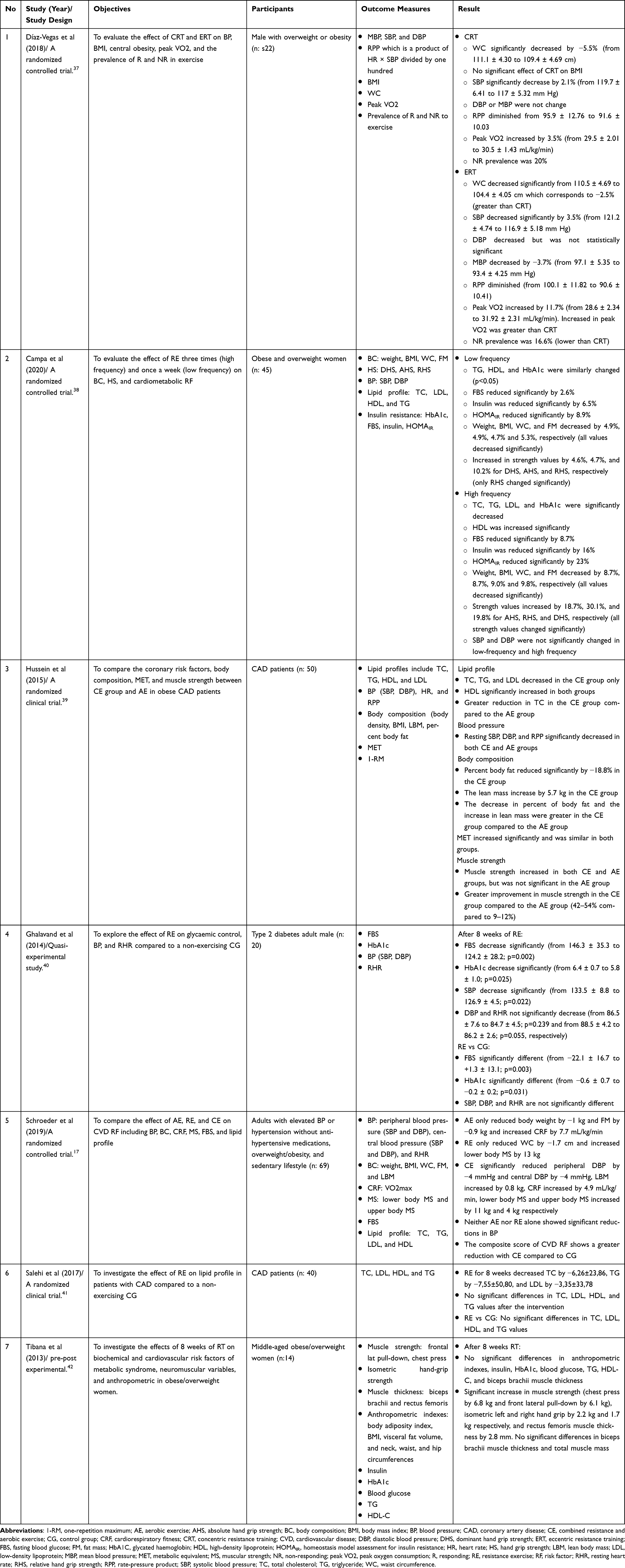 |
Table 4 Studies Related to the Effect of Resistance Training on Cardiovascular Risk Factors |
In a systematic review and meta-analysis conducted by Carlson et al the effect of isometric exercise on systolic BP (SBP), DBP, and mean arterial pressure (MAP) in subclinical patients was examined. According to the study, isometric RT resulted in a reduction in BP that was comparable to, or possibly even greater than, reductions observed with other exercise modalities. This decrease was observed not only in patients with hypertension who are receiving treatment but also in subjects with normal BP. Furthermore, the reduction in MAP and DBP was greater in the group of patients with hypertension who were receiving treatment.25
Inder et al conducted a study to explore the effect of isometric RT on changes in SBP, DBP, and MAP in adult patients. The results showed that it led to a decrease in SBP, DBP, and MAP, aligning with previous studies. The decrease in BP was greater in male hypertensive patients aged >45 years old.22 In a systematic review and meta-analysis conducted by Smart et al it was suggested that isometric exercise lowered BP, especially SBP, DBP, and MAP.23
The mechanism of BP reduction due to isometric RT remains unclear.23,25,27,42 One of the mechanisms is a decreased in arterial stiffness. Primary hypertension is caused by various factors such as arterial stiffness and impaired vasomotor activity such as the Renin-Angiotensin-Aldosterone System (RAAS) and nitric oxide (NO) secretion.27,52–54 Arterial stiffness refers to the resistance of the arterial walls and is affected by factors such as kidney failure, age, smoking, and obesity. When the left ventricle contracts, blood is pumped through the aorta, leading to dilation of the aortic wall, which is a determinant of SBP. As the left ventricle relaxes, blood flows back towards the heart until the aortic valve closes, marking the end of SBP. The maintenance of SBP requires an adequate degree of aortic stiffness. The degree of arterial stiffness is determined by the tunica intima and tunica adventitia which are formed from elastin, smooth muscle, collagen, and mucopolysaccharides. This is attributed to collagen deposits which occur in the connective tissue and calcification of blood vessel walls due to aging and high intraluminal BP. High BP leads to endothelial dysfunction, resulting in reduced NO production, thereby causing further arterial wall stiffness.54
The RAAS is a key regulator of arterial BP and plays a crucial role in maintaining fluid and electrolyte balance within the body. Aldosterone, as one of its components, increases vascular smooth muscle hypertrophy and stimulates the synthesis of fibronectin and endothelin 1. These processes can lead to elevated arterial stiffness and hypertension.54 Renin, which is produced by kidney cells maintain the electrolyte body balance and BP regulation. The RAAS in the process of atherosclerosis is determined by the angiotensin II (Ang II) enzyme. In atherosclerosis formation, this enzyme regulates smooth muscles and endothelial cells and has been shown to induce inflammation and oxidative stress. Its increase aggravates the process by promoting adhesion molecule expression on endothelium, leading to enhanced recruitment of macrophages and the formation of plaques.53
Hypertension is known to cause endothelial dysfunction, leading to subsequent oxidative stress. One significant aspect of this process is the role of NO as a potent antioxidant in regulating peripheral vascular resistance. This was achieved by promoting relaxation and vasodilation of vascular smooth muscle. However, due to oxidative stress, NO deficit in blood vessels emerges as a primary contributor to hypertension.55
Previous studies support the role of isometric RT in enhancing vascular vasodilation through increased NO bioavailability. This leads to peripheral vasodilation and decreases systemic peripheral resistance.23,25,27,39 Specifically, isometric exercise has been reported to augment vascular NO-mediated vasodilation in response to reactive hyperemia in patients receiving antihypertensive medication. This effect was observed solely in the trained lower limb and not in patients with normal BP.25 A systematic review by Ashton et al found that improvements in endothelial function were obtained after RT for 7–23 weeks through adaptation of NO metabolism produced by shear stress resulting from muscle contraction during exercise and changes in BP and resting heart rate.27
Following the administration of isometric exercise, SBP decreased by about 7 mmHg.25 Isometric RT can lower BP by reducing total peripheral resistance similar to AE. Anti-hypertensive effect of RT becomes evident after 12 weeks of intervention. However, there is a scarcity of studies examining the impact of RT for 12 weeks.23
Sympathetic modulation and increased endothelial function are thought to be associated with BP reduction. However, there is limited evidence to support the notion that isometric RT is linked to decreased vascular sympathetic modulation. Isometric exercise improves endothelial function, leading to an increase in the diameter of lower limb arteries, enhanced blood flow, and reduced vascular resistance. Additionally, it has also been reported to increase the concentration of antioxidants.25
Certain isometric RT regimens, such as unilateral arm for more than 8 weeks, led to a greater reduction in BP. In line with this, Inder et al found that SBP decreased by almost 6 mmHg, following isometric exercise. However, it is worth noting that the decrease in DBP and MAP was smaller compared to that of SBP.22
A greater reduction in BP was observed in patients at greater risk of hypertension. Hypertensive patients who are men aged 45 years old or older showed a greater reduction in BP. This may be attributed to the deconditioning tendency observed, which provides a greater opportunity for improvement. The decrease in BP was not dependent on weight loss. To optimize the antihypertensive benefits, it is recommended to administer isometric RT for 8 weeks or more. Longer training periods are needed to initiate regional changes in ventricular function.22
Dynamic, isotonic RT is another type of exercise that has been employed to impact BP (Table 4). 38,40 Ghalavand et al conducted a study and observe a decrease in SBP in the intervention group following 8 weeks of exercise. It was suggested that isotonic RT can improve ventricular contractility, stroke volume, left ventricular diastolic function, and endothelial function, ultimately contributing to a reduction in BP.40
Another study was found that concentric RT led to a decrease in BP of 2.1%, while its eccentric counterpart resulted in a 3.5% reduction. However, changes in DBP could not be obtained due to the small number of subjects. Another study reported that 12 weeks of concentric RT led to a reduction of 3.1% in SBP.37
A combination of AE and RT significantly causes changes in BP with a better reduction in SBP than when they are administered separately. The intervention provided was effective in triggering adaptation. AE contributes to improved cardiorespiratory endurance, while RT enhances muscle strength. Their combination, increased cardiorespiratory fitness, despite not being statistically significant.17 The decrease in BP that occurred in administering RT is the same as AE and adheres to the principle of a dose-response relationship, with variable duration of intervention (Table 4). 39
An eight-week program was considered insufficient to detect the expected BP response to exercise. Previous studies have shown that a minimum duration of 12 weeks is required to achieve a significant reduction in BP, either through AE, RT, or a combination of both. It is worth noting that baseline BP can influence this decrease. For example, in one study, 15 of the 69 participants had a baseline BP of <120/80 mmHg, making it challenging to detect exercise-induced reduction. Despite SBP not change, there was a decrease in DBP in this study. Additionally, exercise coupled with changes in body composition, showed a reduction in BP and a better decrease in CVD risk. Changes in body composition were more significant after giving AE compared to RT. The combination of these two therapies causes a slight change with an increase in lean body mass (Table 4). 17
According to a literature review and meta-analysis conducted by Jewiss et al no difference in SBP between the group given a combination of AE-RT and the control group. Despite the decrease in SBP in the intervention group, the reduction may not be clinically significant, averaging around 2 mmHg. The decrease in SBP resulted from an increase in cardiac output due to an increase in peak heart rate.24
Compared to a decrease in SBP and DBP, a reduction in MAP was less statistically significant. A study found that the effect of RT on resting heart rate and MAP was not statistically significant. The lack of data regarding its impact on MAP could be due to studies assessing BP as being less frequent than SBP and DBP.39 Since MAP is affected more by DBP rather than SBP, a lesser effect of RT on DBP caused a lesser effect on MAP.27 In a study by Campa et al no changes in BP were observed after the intervention in the group given RT. The absence of a decrease in BP was presumed because there was no implementation of a calorie restriction program.38 One study explored the impact of calorie restriction on effect of RT in hypertensive patients. It was found that this therapy without calorie restriction was associated with lower BP reductions.42
Effect of RT on Type 2 DM
RT has been associated with various beneficial effects on individuals with type 2 DM. These include a decrease in fasting blood glucose levels, insulin secretion, and protein glycation are haemoglobin A1c (HbA1c), as well as an increase in the number of glucose transporter (GLUT)-4, and improved glucose transport into cells.38,40,56
Insulin resistance occurs when peripheral tissues fail to respond adequately to insulin, leading to hyperglycaemia and dysfunction of pancreatic beta-cell.57,58 In the context of type 2 DM, insulin resistance primarily contributed to the development and progression of the condition, particularly in the liver and muscle. Furthermore, it is risk factors that promote the emergence of dyslipidaemia and hypertension.7
Glucose is a hydrophilic monosaccharide that circulates widely in the bloodstream. It enters the cell through an active co-transporter sodium-dependent mechanism or by carrier-mediated transport. The carriers on the cell surface are known as GLUT, and they consist of 14 types, ranging from GLUT-1 to GLUT-14. Those that play an important role in maintaining blood glucose balance are GLUT-1 to GLUT-4. Among these, GLUT-1 to GLUT-3 located in hepatocytes, pancreatic beta cells, and basolateral membranes of renal tubular and intestinal cells. Meanwhile, GLUT-4 is situated in adipose tissue and cardiac or skeletal muscle cells. Insulin hormone secretion enhances the function of GLUT, facilitating the movement of extracellular glucose into the cells.57
Several factors that contribute to the development of DM include 1) abnormal secretion of the inflammatory mediator, 2) dysregulated secretion of adipokines, cytokines produced by adipocytes, 3) interference with insulin regulation and GLUT receptors by free radicals in the blood, 4) rapid insulin degradation due to autoimmune reactions or abnormal insulin structure, 5) dysfunction of mitochondrial, 6) decreased capacity of cell receptors to bind insulin, and 7) mutation of GLUT-4, leading to impaired glucose transport into cells.57,58 Diabetic macroangiopathy can give rise to atherosclerotic diseases, namely cerebrovascular disorders, peripheral artery disease, and other vascular diseases. Two primary factors that worsen vascular disease in DM are insulin resistance and hyperglycaemia.7,58
Glucose can non-enzymatically bind to proteins within the body, resulting in the formation of glycated proteins. This process is expedited under conditions of oxidative stress, hyperglycaemia, and inflammatory reactions. The initial products of HbA1c and glyco-albumin, which subsequently give rise to advanced glycation end product (AGE). In the atherosclerosis process, AGE contributes by accelerating the migration of monocyte to the sub-endothelial space and promoting the transformation of macrophage. This is achieved through the increase of adhesion molecules on endothelial cells.7
Endothelial cells play a crucial role in maintaining the function and structure of blood vessels by producing a range of bioactive substances. These substances help to maintain a balance between oxidation and anti-oxidation, inflammation and anti-inflammation within the vascular wall, proliferation and anti-proliferation of smooth muscle, dilation and contraction of blood vessels, as well as blood coagulation and fibrinolysis.7 However, various factors such as oxidative stress, dyslipidaemia, hyperglycaemia, and smoking can lead to endothelial dysfunction, ultimately contributing to the development of atherosclerosis.7,53
Shiroma et al assessed the longitudinal effect of strength training on the incidence of type 2 DM or CVD. The results showed a reduction in the incidence of these diseases.56 Ghalavand et al conducted a study to examine the impact of regular RT on resting heart rate, glucose control, and BP in men with type 2 DM. The results showed that 8 weeks of the therapy led to a significant reduction in fasting blood glucose levels and HbA1C.40
Twenty-four weeks of RT was proven to be beneficial in controlling risk factors associated with metabolic syndrome, including HbA1c level. RT increased insulin resistance in young obese people, but the improvement was not significant compared to when it is combined with AE. Additionally, a study found that single contraction RT affects glucose and insulin levels for 18–24 hours post-exercise.38
Eccentric RT led to greater metabolic changes compared to its concentric counterpart.37 A review by Schroeder et al stated that baseline blood glucose levels at the beginning of the program resulted in minor changes in glucose levels after being given a combination of AE and RT.17
Previous studies found an inverse relationship between dose response, duration of RT, and the incidence of type 2 DM in men, with a variation of 12–34% decrease. Similarly, women that engaged in strengthening exercises experienced a decreased risk, with a reduction of 23–35%. Those that received RT had lower CVD risk factors such as body fat, fasting glucose levels, and total cholesterol.56
The mechanism of blood sugar level improvement after RT administration is largely due to the accumulation effect from each training session. Studies showed that muscle contractions enhanced the diffusion of glucose from the blood into the cells, where it is used for energy production. It also caused an elevation in the permeability of the membrane to glucose due to an increase in GLUT-4. Through exercise, the amount of GLUT-4 in the muscles increases, leading to enhanced glucose metabolism and resulting in lower fasting blood glucose and HbA1C.40,42
Exercise could also inhibit fatty acid accumulation in muscle cells by increasing their oxidation, thereby reducing impaired GLUT-4 transport. Improvements in glucose metabolism also occur due to increased insulin action and signalling. Furthermore, the change in glucose control was caused by exercise which increases the protein content of the insulin receptor. The protein kinase B, a relay to send insulin signals activity also improved, ultimately leading to lower blood glucose levels.40
Exercise, either performed alone or in combination with weight reduction programs, indirectly improved the function of the beta cell. This improvement was achieved through the action of biochemical mediators or peptide hormones that influence gene expression in pancreatic cells, subsequently leading to a decrease in blood sugar levels. Following exercise, muscle cells restore glycogen, helping to maintain low blood glucose concentrations for several hours. With increasing muscle mass, RT raised glucose uptake by muscle cells and facilitates blood sugar control. Since the skeletal muscle is an important factor in fatty acid, insulin resistance, and basal metabolism, the increase in muscle mass through strengthening exercise could assist in improving insulin resistance and several other metabolic syndrome assessment indices.40 Additionally, RT-mediated improvements in fasting blood glucose, insulin levels, and insulin resistance result from changes in body composition such as decrease fat mass and increased muscle mass that results in improvement in glucose transport and insulin sensitivity. These have clinical implications for the management of metabolic syndrome, type 2 DM, and CVD.27
Effect of RT on Dyslipidaemia
Atherosclerosis is a condition that arises from the metabolism of fat and lipoprotein, consisting of triglycerides, phospholipids, and cholesterol. This process triggers the activation of macrophage, leading to the formation of foam cells.5 Hyperlipidaemia produces highly reactive oxygen species (ROS) that can damage the endothelium and contribute to the development of atherosclerosis.53 In the context of dyslipidaemia, high fatty acids along with high triglycerides and low-density lipoprotein (LDL), render them more susceptible to oxidation. The oxidation process causes oxidative stress, which in turn plays a role in endothelial and vascular dysfunction leading to inflammation and atherogenesis.5,53
Dyslipidaemia control could be attained either through RT or in combination with AE.17,26,38,39,41,42 A study found that a single application of RT did not affect high density lipoprotein (HDL) triglycerides (TG) significantly.47 However, combination of RT with AE effectively increased HDL and decreased LDL.56 Hussein et al compared the effect of the combination and the single application of AE on CVD risk factors including lipids and body composition in CAD patients. The results showed that AE and RT in combined form resulted in a significant decrease in total cholesterol, triglyceride, and LDL, as well as an increase in HDL. Another study also identified similar outcomes in patients with heart disease after 12 weeks of intervention. Total cholesterol and HDL were significantly associated with body fat percentage.39
The initial lipid profile affects the improvement after the administration of RT, but studies have not found any correlation between relative muscle strength and a decrease in triglyceride levels.17,41,42 In a study conducted by Schroeder et al it was concluded that there was no change in lipid profile in both groups given a combination of AE-RT and the control. This was attributed to the normal range of lipid profile at the beginning of the exercise.17 Salehi et al conducted a study to explore effect of RT on lipid profiles in CAD patients. The results showed a decrease in triglyceride, cholesterol, and LDL levels, but it was not significant. Changes in the average lipid profiles observed in the RT group were the same as in the control group who received regular AE. This could be explained by the initial low level of total cholesterol, triglyceride, and LDL (Table 4). 41
Mann et al found that pre-menopausal women administered 14 weeks of RT experienced a reduction in cholesterol, LDL levels, and body fat ratio. In untrained men, low-intensity RT yielded better outcomes compared to high-intensity. The decrease in cholesterol level was attributed to the improvement in the exchange of its esters between tissues and lipoproteins, particularly with HDL.26
Several studies explored effect of RT on the improvement of dyslipidaemia.26,27,38 According to the recommendations of the ACSM, performing whole-body RT 2–3 days per week led to enhancement in lipid profiles, including LDL and total cholesterol. In a group receiving this exercise 3 times weekly, lipid profiles improved significantly compared to those exercised once a week. The result of this study showed that exercise with a higher frequency had a more positive effect on the health of obese and overweight individuals.38 Compared to high-intensity RT (80–90% 1-RM), moderate-intensity (45–55% 1-RM) resulted in a greater reduction in LDL and total cholesterol. However, in the group given high-intensity RT, there was a significant increase in HDL.26 The improvement in LDL and TG were most pronouncing with 7–23 weeks of intervention.27
Effect of RT on Obesity
Obesity occurs when there is a disruption in fat storage, leading to the accumulation of triglycerides and cholesterol in adipose tissue and atherosclerotic plaques, respectively. This disorder alongside atherosclerosis, is considered a chronic inflammatory disease.5,59 Their pathogenesis has similarities, as they both involve an inflammatory process triggered by factors such as fat, oxidized LDL, and free fatty acids. Adipose tissue secretes adipocytokines in the form of tumor necrotizing factor-α, interleukin 6, leptin, and resistin, which can contribute to endothelial dysfunction, insulin resistance, systemic inflammation, and hypercoagulability. Systemic inflammation leads to an increased level of C-reactive protein (CRP) and adiposity, further elevating the risk of peripheral vascular disease, myocardial infarction, and DM.59,60 Previous systematic review found that RT decreased CRP, LDL, and TG levels through improvement of muscle mass and fat mass.27 An increase of 10 kg of body weight can raise the risk of CAD, SBP, and BP by up to 12%, 3 mm Hg, and 2.3 mm Hg. Additionally, every increase in BMI can elevate the risk of haemorrhagic and ischemic stroke by 6 and 4%, respectively.59
Anthropometric changes and cardiometabolic risk factors are important factors for improving the health outcomes of obese patients.38 In a study by Hussein et al a negative correlation was found between lean mass and total cholesterol levels, while a positive correlation was observed with LDL levels.39 Campa et al conducted a study comparing effect of RT given 3 times and once a week on body composition, cardiometabolic risk factors, and hand grip strength in obese and overweight women. It was found that this exercise decreased body weight, BMI, and fat mass.38
Diaz-Vegas et al conducted a study to evaluate the effect of concentric or eccentric RT on CVD risk factors including central obesity and BMI. It was found that they both decreased waist circumference but no impact on BMI.37 Another study showed that the combination of AE and RT along with a calorie restriction diet improved the anthropometric index of obese patients. However, this improvement was not observed when RT was administered alone (Table 4). 42
Conclusion
This review found that administering RT either in the form of a single exercise or in combination with aerobic exercise or a calorie-restricted diet in an average of 8 to 12 weeks improved BP, DM-related parameters, lipid profile, and body compositions.
Abbreviations
1-RM, One-repetition maximum; ACSM, American College of Sports Medicine; AE, Aerobic exercise; AGE, Advance glycation end; Ang II, Angiotensin II; BMI, Body mass index; BP, Blood pressure; CAD, Coronary Artery Disease; CR, Cardiac rehabilitation; CVD, Cardiovascular Disease; DBP, Diastolic blood pressure; DM, Diabetes Mellitus; GLUT, Glucose transporter; HbA1c, Hemoglobin A1c; HDL, High-density lipoprotein; LDL, Low-density lipoprotein; MAP, Mean arterial pressure; METs, Metabolic equivalents; NO, Nitric oxide; RAAS, Renin-angiotensin Aldosterone System; RT, Resistance training; SBP, Systolic blood pressure.
Acknowledgment
The authors would like to acknowledge Padjadjaran University for awarding an internal research grant to Nur Atik for conducting and publishing this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Cardiovascular diseases; 2023. Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1.
2. Zhao D. Epidemiological features of cardiovascular disease in Asia. JACC Asia. 2021;1(1):1–13. doi:10.1016/j.jacasi.2021.04.007
3. Libby P, Buring JE, Badimon L, et al. Atherosclerosis. Nat Rev Dis Primers. 2019;5(1):56. doi:10.1038/s41572-019-0106-z
4. Joseph P, Leong D, McKee M, et al. Reducing the global burden of cardiovascular disease, part 1: the epidemiology and risk factors. Circ Res. 2017;121(6):677–694. doi:10.1161/CIRCRESAHA.117.308903
5. Wengrofsky P, Lee J, Makaryus AN. Dyslipidemia and Its Role in the Pathogenesis of Atherosclerotic Cardiovascular Disease: Implications for Evaluation and Targets for Treatment of Dyslipidemia Based on Recent Guidelines. Dyslipidemia: Intech Open; 2019.
6. Pelliccia A, Sharma S, Gati S, et al. ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease: the task force on sports cardiology and exercise in patients with cardiovascular disease of the European society of cardiology (ESC). Rev Esp Cardiol. 2021;74(6):545. doi:10.1016/j.rec.2021.05.003
7. Katakami N. Mechanism of development of atherosclerosis and cardiovascular disease in diabetes mellitus. J Atheroscler Thromb. 2018;25(1):27–39. doi:10.5551/jat.RV17014
8. Lavie CJ, Ozemek C, Carbone S, Katzmarzyk PT, Blair SN. Sedentary behavior, exercise, and cardiovascular health. Circ Res. 2019;124(5):799–815. doi:10.1161/CIRCRESAHA.118.312669
9. Kemps H, Kränkel N, Dörr M, et al. Exercise training for patients with type 2 diabetes and cardiovascular disease: what to pursue and how to do it. a position paper of the European Association of preventive cardiology (EAPC). Eur J Prev Cardiol. 2019;26(7):709–727. doi:10.1177/2047487318820420
10. Heinl RE, Dhindsa DS, Mahlof EN, et al. Comprehensive cardiovascular risk reduction and cardiac rehabilitation in diabetes and the metabolic syndrome. Can J Cardiol. 2016;32(10 Suppl 2):S349–S357. doi:10.1016/j.cjca.2016.07.507
11. Lindgren M, Börjesson M. The importance of physical activity and cardiorespiratory fitness for patients with heart failure. Diabet Res Clin Pract. 2021;176:108833. doi:10.1016/j.diabres.2021.108833
12. Patel PN, Zwibel H. Physiology, Exercise. StatPearls [Internet]: StatPearls Publishing; 2021.
13. Nystoriak MA, Bhatnagar A. Cardiovascular effects and benefits of exercise. Front Cardiovasc Med. 2018;5(135):1–11. doi:10.3389/fcvm.2018.00001
14. Joseph JJ, Deedwania P, Acharya T, et al. Comprehensive management of cardiovascular risk factors for adults with type 2 diabetes: a scientific statement from the American heart association. Circulation. 2022;145(9):e722–e59. doi:10.1161/CIR.0000000000001040
15. Fernandes T, Baraúna VG, Negrão CE, Phillips MI, Oliveira EM. Aerobic exercise training promotes physiological cardiac remodeling involving a set of microRNAs. Am J Physiol Heart Circ Physiol. 2015;309(4):H543–H552. doi:10.1152/ajpheart.00899.2014
16. Wang B, Gan L, Deng Y, et al. Cardiovascular disease and exercise: from molecular mechanisms to clinical applications. J Clin Med. 2022;11(24):7511. doi:10.3390/jcm11247511
17. Schroeder EC, Franke WD, Sharp RL, D-c L. Comparative effectiveness of aerobic, resistance, and combined training on cardiovascular disease risk factors: a randomized controlled trial. PLoS One. 2019;14(1):e0210292. doi:10.1371/journal.pone.0210292
18. Liang M, Pan Y, Zhong T, Zeng Y, Cheng AS. Effects of aerobic, resistance, and combined exercise on metabolic syndrome parameters and cardiovascular risk factors: a systematic review and network meta-analysis. Rev Cardiovasc Med. 2021;22(4):1523–1533. doi:10.31083/j.rcm2204156
19. Yavari A, Najafipoor F, Aliasgarzadeh A, Niafar M, Mobasseri M. Effect of aerobic exercise, resistance training or combined training on glycaemic control and cardio-vascular risk factors in patients with type 2 diabetes. Biol Sport. 2012;29(2):135–143. doi:10.5604/20831862.990466
20. Sousa N, Mendes R, Silva A, Oliveira J. Combined exercise is more effective than aerobic exercise in the improvement of fall risk factors: a randomized controlled trial in community-dwelling older men. Clin Rehabil. 2017;31(4):478–486. doi:10.1177/0269215516655857
21. Chen T, Lin J, Lin Y, et al. Effects of aerobic exercise and resistance exercise on physical indexes and cardiovascular risk factors in obese and overweight school-age children: a systematic review and meta-analysis. PLoS One. 2021;16(9):1.
22. Inder JD, Carlson DJ, Dieberg G, McFarlane JR, Hess NC, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis to optimize benefit. Hypertens Res. 2016;39(2):88–94. doi:10.1038/hr.2015.111
23. Smart NA, Way D, Carlson D, et al. Effects of isometric resistance training on resting blood pressure: individual participant data meta-analysis. J Hypertens. 2019;37(10):1927–1938. doi:10.1097/HJH.0000000000002105
24. Jewiss D, Ostman C, Smart N. The effect of resistance training on clinical outcomes in heart failure: a systematic review and meta-analysis. Int J Cardiol. 2016;221:674–681. doi:10.1016/j.ijcard.2016.07.046
25. Carlson DJ, Dieberg G, Hess NC, Millar PJ, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis. Mayo Clin Proc. 2014;89(3):327–334. doi:10.1016/j.mayocp.2013.10.030
26. Mann S, Beedie C, Jimenez A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: review, synthesis and recommendations. Sports Med. 2014;44(2):211–221. doi:10.1007/s40279-013-0110-5
27. Ashton R, Tew G, Aning J, et al. Effects of short-, medium and long-term resistance exercise training on cardiometabolic health outcomes in adults: systematic review and meta-analysis. Br J Sports Med. 2020;54(6):341–348. doi:10.1136/bjsports-2017-098970
28. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
29. Arsyad DS, Westerink J, Cramer MJ, et al. Modifiable risk factors in adults with and without prior cardiovascular disease: findings from the Indonesian national basic health research. BMC Public Health. 2022;22(1):660. doi:10.1186/s12889-022-13104-0
30. Harmadha WSP, Muharram FR, Gaspar RS, et al. Explaining the increase of incidence and mortality from cardiovascular disease in Indonesia: a global burden of disease study analysis. PLoS One. 2023;18(12):e0294128. doi:10.1371/journal.pone.0294128
31. ACSM. ACSM’s Guidelines for Exercise Testing and Prescription. Philadelphia: Wolters Kluwer; 2018.
32. Hansen D, Abreu A, Doherty P, Völler H. Dynamic strength training intensity in cardiovascular rehabilitation: is it time to reconsider clinical practice? A systematic review. Eur J Prev Cardiol. 2019;26(14):1483–1492. doi:10.1177/2047487319847003
33. Laukkanen JA, Khan H, Kunutsor S. Cardiorespiratory fitness, muscle strength and risk of cardiovascular outcomes. J Public Health Emerg. 2017;1(6):60–64. doi:10.21037/jphe.2017.05.10
34. Helgerud J, Karlsen T, Kim W, et al. Interval and strength training in CAD patients. Int J Sports Med. 2011;32(1):54–59. doi:10.1055/s-0030-1267180
35. Schoenfeld BJ, Grgic J, Van Every DW, Plotkin DL. Loading recommendations for muscle strength, hypertrophy, and local endurance: a re-examination of the repetition continuum. Sports. 2021;9(2):32–57. doi:10.3390/sports9020032
36. Caruso FR, Bonjorno JC, Arena R, et al. Hemodynamic, autonomic, ventilatory, and metabolic alterations after resistance training in patients with coronary artery disease: a randomized controlled trial. Am J Phys Med Rehabil. 2017;96(4):226–235. doi:10.1097/PHM.0000000000000568
37. Díaz-Vegas A, Espinoza A, Cofré C, Sánchez-Aguilera P. Eccentric resistance training reduces both non-response to exercise and cardiovascular risk factors in adult with overweight or obesity. Sci Sports. 2018;33(4):245–252. doi:10.1016/j.scispo.2017.12.002
38. Campa F, Maietta Latessa P, Greco G, et al. Effects of different resistance training frequencies on body composition, cardiometabolic risk factors, and handgrip strength in overweight and obese women: a randomized controlled trial. J Funct Morphol Kinesiol. 2020;5(3):51. doi:10.3390/jfmk5030051
39. Hussein N, Thomas M, Prince D, Zohman L, Czojowski P. Effect of combined resistive and aerobic exercise versus aerobic exercise alone on coronary risk factors in obese coronary patients. J Clin Exp Cardiolog. 2015;6(361):2.
40. Ghalavand A, Shakeriyan S, Monazamnezhad A, Delaramnasab M. The effect of resistance training on cardio-metabolic factors in males with type 2 diabetes. Jundishapur J Chronic Dis Care. 2014;3(4):e23346. doi:10.17795/jjcdc-23346
41. Salehi Z, Salehi K, Moeini M, Kargarfard M, Sadeghi M. The effect of resistance exercise on lipid profile of coronary artery disease patients: a randomized clinical trial. Iran J Nurs Midwifery Res. 2017;22(2):112–116. doi:10.4103/ijnmr.IJNMR_385_14
42. Tibana RA, Navalta J, Bottaro M, et al. Effects of eight weeks of resistance training on the risk factors of metabolic syndrome in overweight/obese women-“A Pilot Study”. Diabetol Metab Syndr. 2013;5(1):11. doi:10.1186/1758-5996-5-11
43. Marzolini S, Oh PI, Brooks D. Effect of combined aerobic and resistance training versus aerobic training alone in individuals with coronary artery disease: a meta-analysis. Eur J Prev Cardiol. 2012;19(1):81–94. doi:10.1177/1741826710393197
44. Hollings M, Mavros Y, Freeston J, Singh MF. The effect of progressive resistance training on aerobic fitness and strength in adults with coronary heart disease: a systematic review and meta-analysis of randomised controlled trials. Eur J Prev Cardiol. 2017;24(12):1242–1259. doi:10.1177/2047487317713329
45. Kambic T, Hadžić V, Lainscak M. Hemodynamic response to high-and low-load resistance exercise in patients with coronary artery disease: a randomized, crossover clinical trial. Int J Environ Res Public Health. 2021;18(8):3905. doi:10.3390/ijerph18083905
46. Xanthos PD, Gordon BA, Kingsley MI. Implementing resistance training in the rehabilitation of coronary heart disease: a systematic review and meta-analysis. Int J Cardiol. 2017;230:493–508. doi:10.1016/j.ijcard.2016.12.076
47. Fidalgo ASF, Farinatti P, Borges JP, de Paula T, Monteiro W. Institutional guidelines for resistance exercise training in cardiovascular disease: a systematic review. Sports Med. 2019;49(3):463–475. doi:10.1007/s40279-019-01059-z
48. Lamotte M, Chimenti S. Resistive training and hemodynamics in cardiac rehabilitation. J Cardiopulm Rehabil. 2017;1(2):1000111.
49. Grafe K, Bendick P, Burr M, Boura J, Franklin BA. Effects of resistance training on vascular and hemodynamic responses in patients with coronary artery disease. Res Q Exerc Sport. 2018;89(4):457–464. doi:10.1080/02701367.2018.1519385
50. Adams J, Cline M, Reed M, Masters A, Ehlke K, Hartman J. Importance of resistance training for patients after a cardiac event. Proc. 2006;19(3):246–248. doi:10.1080/08998280.2006.11928172
51. Williams MA, Haskell WL, Ades PA, et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American heart association council on clinical cardiology and council on nutrition. Phy Act Metab Cir. 2007;116(5):572–584.
52. Ziegler T, Abdel Rahman F, Jurisch V, Kupatt C. Atherosclerosis and the capillary network; pathophysiology and potential therapeutic strategies. Cells. 2019;9(1):50. doi:10.3390/cells9010050
53. Hurtubise J, McLellan K, Durr K, Onasanya O, Nwabuko D, Ndisang JF. The different facets of dyslipidemia and hypertension in atherosclerosis. Curr Atheroscler Rep. 2016;18(12):82. doi:10.1007/s11883-016-0632-z
54. Ecobici M, Stoicescu C. Arterial stiffness and hypertension–which comes first? Maedica. 2017;12(3):184–190.
55. Larsen MK, Matchkov VV. Hypertension and physical exercise: the role of oxidative stress. Medicina (Kaunas). 2016;52(1):19–27. doi:10.1016/j.medici.2016.01.005
56. Shiroma EJ, Cook NR, Manson JE, et al. Strength training and the risk of type 2 diabetes and cardiovascular disease. Med Sci Sports Exerc. 2017;49(1):40–46. doi:10.1249/MSS.0000000000001063
57. Yaribeygi H, Farrokhi FR, Butler AE, Sahebkar A. Insulin resistance: review of the underlying molecular mechanisms. J Cell Physiol. 2019;234(6):8152–8161. doi:10.1002/jcp.27603
58. Zeadin MG, Petlura CI, Werstuck GH. Molecular mechanisms linking diabetes to the accelerated development of atherosclerosis. Can J Diabetes. 2013;37(5):345–350. doi:10.1016/j.jcjd.2013.06.001
59. Csige I, Ujvárosy D, Szabó Z, et al. The impact of obesity on the cardiovascular system. J Diabetes Res. 2018;2018:3407306. doi:10.1155/2018/3407306
60. Henning RJ. Obesity and obesity-induced inflammatory disease contribute to atherosclerosis: a review of the pathophysiology and treatment of obesity. Am J Cardiovasc Dis. 2021;11(4):504–529.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.