")
Back to Journals » Research and Reports in Urology » Volume 15
Refractory Bladder Neck Contracture (BNC) After Radical Prostatectomy: Prevalence, Impact and Management Challenges
Authors Uguzova S, Beisland C, Honoré A , Juliebø-Jones P
Received 28 July 2023
Accepted for publication 2 November 2023
Published 7 November 2023 Volume 2023:15 Pages 495—507
DOI https://doi.org/10.2147/RRU.S350777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Sabine Uguzova,1 Christian Beisland,2,3 Alfred Honoré,2,3 Patrick Juliebø-Jones2,3
1Department of Urology, Stepping Hill Hospital, Manchester, UK; 2Department of Urology, Haukeland University Hospital, Bergen, Norway; 3Department of Clinical Medicine, University of Bergen, Bergen, Norway
Correspondence: Patrick Juliebø-Jones, Email [email protected]
Abstract: Bladder neck contracture is a recognised complication associated with radical prostatectomy. The management can be challenging, especially when refractory to initial intervention strategies. For the patient, the burden of disease is high and continence status cannot be overlooked. This review serves to provide an overview of the management of this recognised clinical pathology. Consideration needs to be given to minimally invasive approaches such as endoscopic incision, injectables, implantable devices as well as major reconstructive surgery where the condition persists. For the latter, this can involve open and robotic surgery as well as use of grafts and artificial sphincter surgery. These elements underline the need for a tailored and a patient centred approach.
Keywords: prostate cancer, bladder neck contracture, radical prostatectomy
Introduction
Prostate cancer (PCa) is the second most common cancer with an estimated 1.41 million new cases diagnosed in 2020.1 Among these new cases, approximately 40% will have clinically significant PCa2,3 and within this group approximately 38% of patients will undergo radical prostatectomy (RP).4,5 One of the late complications is bladder neck contracture (BNC) and based on the Cancer of the Prostate Strategic Urological Research Endeavor (CaPSURE) database, the risk is estimated between 1% and 8.4%.6 In the context of RP, this can also be referred to as vesicourethral anastomotic stenosis (VUAS). The commonest cause is healing by secondary intention, often precipitated by ischemia, wound distraction and/or poor apposition associated with post-operative complications.7 When occurring after RP as opposed to radiotherapy (RTx), the onset of BNC is typically more rapid such as 6 months.8 First-line treatment for BNC post RP is currently dilatation or endoscopic incision of the fibrotic tissue.9–11 Reported success rates range between 80% and 100%.12 Where initial treatments fail, patients are left with refractory BNC (rBNC), which can be difficult to manage. The aim of this article was to summarise the available evidence on the treatment options of rBNC after RP.
Methods
A comprehensive but non-systematic review of the literature was performed on surgical management options for refractory BNC after RP. Search was performed of bibliographic databases including PubMed/MEDLINE, Scopus and Google Scholar. Reference lists of studies were also searched as well as relevant grey literature eg, conference abstracts. Search terms included the following: “refractory”, “recurrent”, “recalcitrant”, “vesicourethral anastomotic”, “bladder neck”, “posterior urethral”, “stenosis”, “stricture”, “contracture”, “radical prostatectomy” and “devastated bladder outlet”. All study types were considered eligible for inclusion, and there were no time limits applied. Articles reporting bladder neck stenosis with prostate in-situ were excluded. Only articles in the English language were considered. The findings were evaluated and have been evaluated and summarised in a narrative fashion, which has been grouped according to the following key areas: (1) Definition, prevalence, and socioeconomic impact, (2) Treatment options and challenges, (3) Minimally invasive options, and (4) Surgical reconstruction.
Refractory BNC: Definition, Prevalence, and Socioeconomic Impact
In 2007, Elliott et al reported one of the largest published series on BNC post RP and determined the incidence was 8.4%.6 With the advent of robotic surgery, new operative techniques and advances in peri-operative care, the risk of BNC has decreased to 0–2%.13–17 However, the risk increases to 22–40% in patients who undergo salvage prostatectomy after initial RTx.15 Selvi et al18 studied initial treatment success rates and reported the risk of recalcitrant disease to be approximately 20% of all BNC cases. At present, there is also no universal definition on when BNC can be defined as refractory. Reported definitions range between failure after one to >3 procedures.19–24 The treatment carries an economic burden. It is estimated that in the UK, an elective bladder neck incision (BNI) procedure costs £1204-2987 in the elective setting and this cost rises threefold if it is performed in the emergency setting.25
Treatment Options and Challenges
Given that following RP, the posterior urethra is shorter, there is less tissue to either incise or augment without risking further complications. Therefore, treatment options and their outcomes for BNC post RP differ when compared to BNC where the prostate is still in situ. The majority of BNC patients will be treated with minimally invasive approaches. However, the small proportion of patients who develop a recurrence pose a major challenge, especially when long-term intermittent self-dilatation (ISD) is not an option. Currently, there are three main guidelines that outline the treatment rationale and options for patients with BNC post RP: American Urology Association (AUA, 2023), European Association of Urology (EAU, 2023) and Société Internationale d’Urologie (SIU, 2010).11 The consensus among these guidelines is that most patients can be successfully treated with simple measures such as dilatation and scar incision or resection. However, for more severe and recalcitrant cases, or cases of complete loss of patency (often referred to as ´devastated bladder outlet´), these should be offered open or robotic surgical reconstruction. Outcomes of both minimally invasive and surgical procedures are summarised in Table 1 and Table 2.
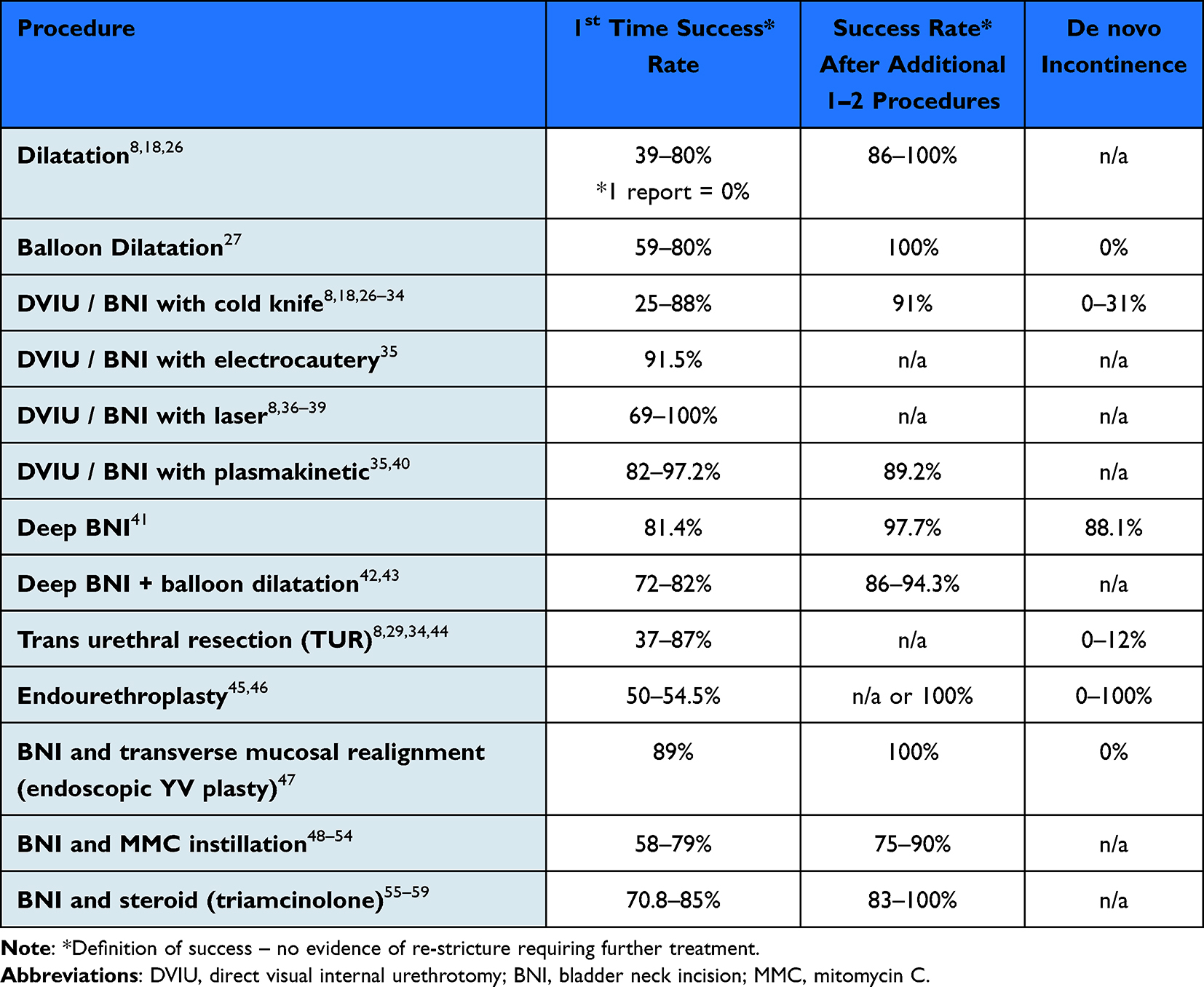 |
Table 1 Comparative Summary of Minimally Invasive Techniques for VUAS Repair |
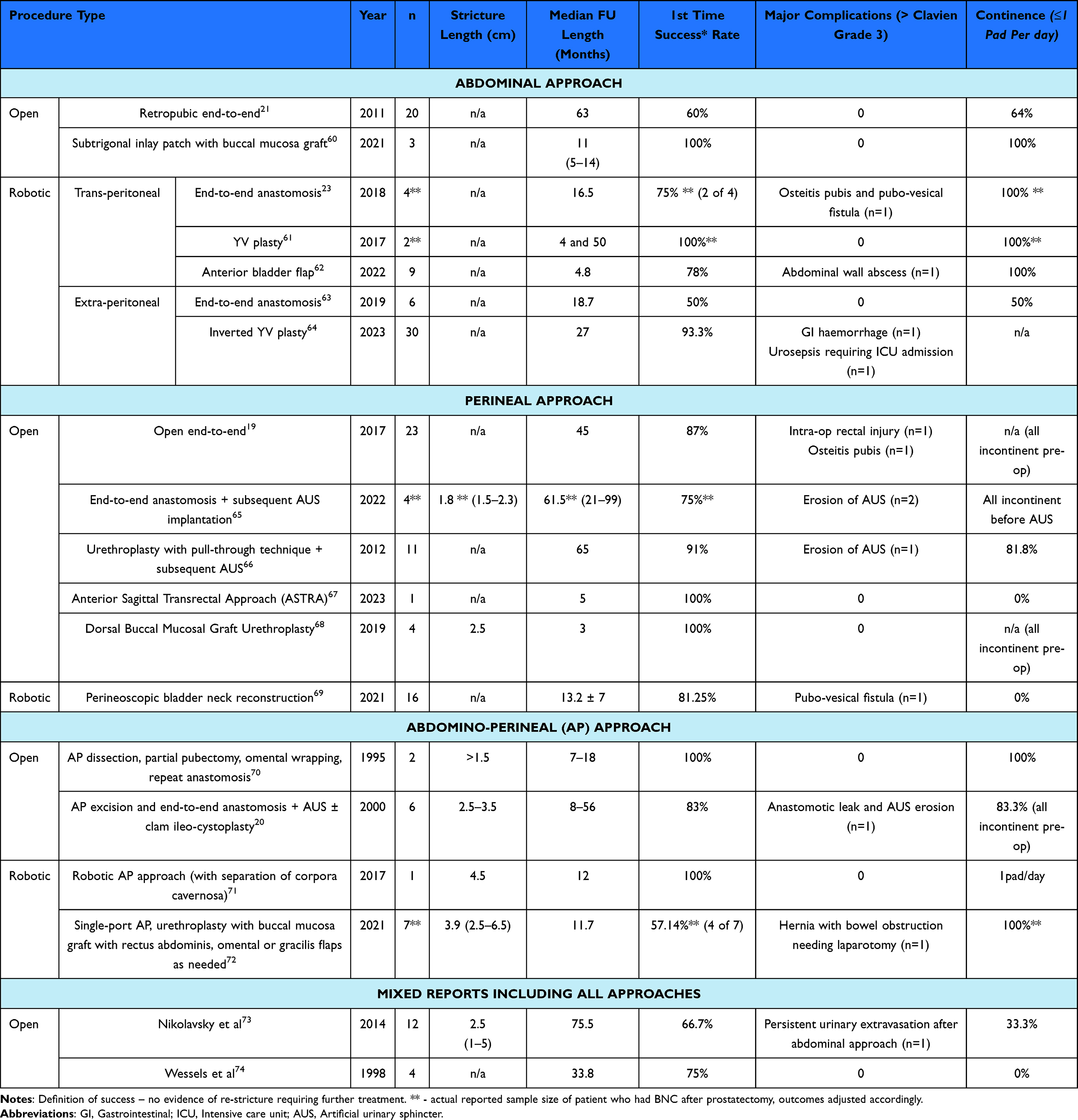 |
Table 2 Comparative Summary of Surgical Reconstructive Techniques for VUAS Repair |
There is no set number of procedures that patients should undergo before proceeding with major surgery. Ultimately, it is dependent on the scar morphology (length, extent and surrounding tissue involvement, degree of obliteration), patient factors (performance status and patient wishes), surgeon experience and available resources. Overall, patients usually need two procedures to resolve BNC8 or at least, achieve a greater than 80% chance of improving their functional status. Mean time to stricture recurrence is approximately 6 months. Multiple previous attempts and tobacco use are associated with a higher risk of procedural failure.8,12 De novo incontinence is one of the major risks of any BNC treatment. EAU guidelines highlight rates of 0–11%; however, some studies have reported it to be as high as 88%.41 Therefore, patient expectations need to be managed prior to the initiation of any treatment. Appropriate counselling regarding the risks of recurrence, potential complications and multiple procedures is key.
Minimally Invasive Approaches
Given the definition of rBNC varies as well as the need for a tailored approach, minimally invasive techniques can be attempted initially.
Endoscopic Procedures
Dilatation can be attempted but recurrence rates are high. Following failure of initial dilatation, the next step is usually BNI, which is also referred to as direct visual internal urethrotomy (DVIU). This can be performed with either a cold or a hot knife as well as various other energy sources (electrocautery with monopolar or bipolar, laser, or plasmakinetic systems). Similar to dilatation, the initial and secondary success rates with BNI have been reported at 74% and 98%,27–33 respectively. Outcomes between cold and hot knife methods appear comparable. Lasers that have been employed for this purpose include Nd: YAG, Thulium: YAG and Holmium: YAG systems. Their properties allow for effective cutting power while maintaining good haemostasis and lower risk of scar formation.8,36–39,75 DVIU with the plasmakinetic energy source has reported patency rates from 82% to 97.2%, although only two studies have been performed to date.35,40 The latter technique uses bipolar energy with axipolar electrode in an electro-conductive solution causing formation of ionized plasma corona and ultimately vaporisation or resection of the tissue.76
Irrespective of the energy source, incisions are made at 3 and 9 o’clock. Incisions at 6 and 12 o’clock are discouraged in order to avoid injury to the rectum and/or pubic symphysis.9 The depth of incision depends on the thickness and extent of the scar but must be generous enough to establish a lumen of reasonable size. Shinchi et al reported the first-time success rate of deep BNI approach as 81.4%, but this was matched by an equally high percentage of de novo incontinence.41 As such, albeit there is evidence to support performing deep BNI down to fat it does not increase the success rate significantly enough to justify the additional risks.41 These outcomes are also not further improved by combination of simultaneous balloon dilatation, as patency rates for this are similar, and range from 72% to 81% after a single procedure.42,43 More extensive intervention with transurethral resection (TUR) yields success rates between 37% and 87%.8,21,34,44 Similar to hot knife DVIU/BNI, various energy sources can be employed. However, success rates are similar to simple incision, but the associated risks can be higher. In 2004, Kropfl et al reported on a trial of endoscopic incision or resection followed by brachytherapy delivered over 3 days at 4Gy x3 or x4 scheme with the aim to prevent recurrence. The principle behind the technique is considered to be like that of endovascular radiotherapy to prevent hypertrophic scar formation. Two of 15 patients in the cohort had BNC post RP and even though the overall cohort success rate was 46%, the two BNC post RP patients were free of recurrence at 22 months follow-up.77
Finally, there have been attempts at reconstructing the scar endoscopically with endourethroplasty. Chiou et al described a two-step technique carried out in a series of two patients. The patients underwent scar incision at 2, 4, 8 and 10 o’clock followed by creation of a grafting bed with a paediatric resectoscope a few days later. This was achieved by pulling through a tubulised preputial skin graft via a suprapubic tract and fixing it with two perineal sutures. One patient had good patency at 25 months follow-up, but the second required one more dilatation.45 This technique was further modified and tested by Kuyumcuoglu et al; however, the first-time success rate in 11 patients was only 54.5% and graft necrosis occurred in two patients.46 A more recent study by Abramowitz et al had also described a technique of BNI combined with transverse mucosal realignment. In this procedure, the scar was incised, and healthy bladder mucosa brought over the defect and fixed with laparoscopic suturing device in a Y-V plasty technique. Their success rate was 89% after the first treatment and 100% following two procedures.47
Injectables (Scar Modulators)
Intralesional injections serve to prevent re-fibrosis of the incision or resection site and thereby stabilise the scar. It is used primarily as an adjunct following primary surgical scar treatment. There have been a multitude of injectables trialled in urethral stricture disease.78 However, specifically for BNC there are two main scar stabilisers that are used most commonly: triamcinolone and mitomycin C (MMC). The former is a glucocorticosteroid, and the usual dosages are 40–80mg without any significant difference in outcomes. Its first-time success rate ranges between 70% and 85%.55–59 MMC gives a first-time success rate between 45% and 79%.48–54 An anti-fibrinogenic DNA alkylating agent, it prevents DNA replication and therefore cell growth.79 Concentrations are usually 0.1 to 1 mg/mL with up to 10mg diluted in saline. MMC extravasation into perivesical fat following bladder instillations for bladder cancer is known for its potentially devastating effect.52 Similarly, potential side-effects of MMC injections at VUAS can include osteitis pubis, rectourethral fistula, chronic bladder pain and tissue necrosis.52 As such, EAU guidelines advise against MMC injections for posterior urethral strictures outside the context of clinical trials.9 In recent years, there has been research on use of stem cells and their role in mitigating tissue hypoxia. Wiafe et al reported that bone-marrow derived stem cells co-cultured with human bladder smooth muscle cells resulted in the inhibition of inflammation and fibrosis.80 However, human trials are still awaited.
Implantable Devices / Stents
Several stents have been employed in the setting of rBNC including the Allium Round Posterior Stent. This is a temporary nitinol stent coated with a co-polymer and can be left in position for up to 1 year.81,82 An alternative is Memokath®045, which is a thermo-expandable tightly knit nitinol alloy stent, available in 3 and 7cm lengths, and is designed to prevent urothelial ingrowth83 Overall, success rates are low, and they carry a high risk of ingrowth and de novo incontinence. The former can worsen the fibrotic changes of an already dense stricture, which renders extraction and repeat treatment more difficult. This can be further compounded by stent encrustation, which McNamar et al reported to occur in 23% of their series.84 Given the posterior urethra shortens post RP, stent incontinence rates have been reported from 19% up to 100%. This can be mitigated by subsequent artificial urinary sphincter (AUS) placement. However, this can be complicated by sphincter device erosion in up to 19.5% of patients.84 To this end, EAU guidelines advise against their use in the setting of posterior urethral strictures.9
Surgical Reconstruction
Surgical reconstruction of rBNC post RP can be technically challenging. However, it represents the mainstay treatment when minimally invasive treatments have failed. Tissue viability is invariably further compromised following repeated attempts at minimally invasive procedures, as well as adjuvant or salvage RTx. There are three main elements that are important to consider when planning surgical approach: first-time treatment success, continence and risk of a serious adverse event.
Regarding how to surgically expose the defect, there are 3 main choices: abdominal, perineal or abdomino-perineal. This can be achieved either open or robotically. When deciding upon how to approximate the anastomosis after scar excision, numerous methods have been described in the literature. These range from simple end-to-end anastomosis to variety of augmentations, grafts and flaps. In terms of continence, this can be challenging, as apart from the risk of sphincter injury, it can also unmask an already incompetent sphincter which has been compensated by the scarring.12,85 It is thus important to perform a thorough pre-operative work up in order to determine the length of obliteration and involvement of the membranous urethra/external sphincter so as to appropriately counsel patients regarding the need for additional incontinence surgery. Comparisons between the different surgical reconstructive techniques are summarised in Table 2.
Access to Defect
One of the earliest reports of posterior urethra repair was in the setting of pelvic fractures by Young in 1929. Later in 1953, he described a technique of retropubic reconstruction of the bladder neck in a paediatric population.86,87 It was not until 1995 when Schlossberg et al70 published one of the first case series on open reconstruction of BNC post RP and this was followed by a further series by Wessels et al in 1998.74
Transabdominal approach is the most described approach and can represent a preferred choice where longer segments are involved.73 Both trans/extraperitoneal techniques have been described and the first reports of robotic cases were reported in 2018.23,61,88 Fibrotic changes within the Retzius space, hypertrophy of the bladder muscle, potentially short urethral segment often adherent to the urogenital diaphragm and variable depth of the pelvis can all deliver challenges. As described by Schlossberg et al, “the easy plane is the wrong plane” and as such, an open approach may be accompanied by vertical partial pubectomy to facilitate the view.70 The anterior bladder wall can be adherent to the pubic bone and dissection must be delicate so as to avoid shredding of the tissue. After dissection of the Retzius space, the bladder neck is then freed beneath the pubic symphysis and dropped from the anterior abdominal wall. Therein it allows for identification of the proximal extent of the stricture via opening the anterior bladder wall. This should preferably be done with cold scissors to avoid further compromise of blood supply to the scar. The posterior bladder wall is mobilised from the anterior rectal wall via the Pouch of Douglas. Scarring can then be excised completely or a Y-V plasty can be used to avoid dissection of the posterior bladder wall in cases where rectal injury is a concern. If there is any doubt about the proximity of the ureteric orifices to the resection site, it is important to protect them by inserting small calibre feeding tubes or catheters to delineate their location.12,21,24,60
With robotic surgery, while the anatomy remains challenging, the flexibility of the instruments and tissue magnification allows the surgeon to avoid performing pubectomy, which reduces the morbidity usually associated with the open transabdominal approach. The patient is placed in a Trendelenburg ± dorsal lithotomy position and the robotic arms are most commonly set up in a similar way to the approach used for robotic RP. On-table flexible cystoscopy can be used to map the distal extent of the stricture and a “cut-to-the-light” technique can be performed. However, it is advised to reserve this for short strictures (<0.5cm) only.17,23,61–63,70,88–93 The majority of robotic reports are transperitoneal, but Lavolle et al94 and Diamant et al64 also trialed extraperitoneal access with end-to-end anastomosis. However, outcomes were worse when compared to the transperitoneal approach and first-time treatment success was only 50% and continence rates ranged from 37.5% to 50%. In 2023, Youssef et al65 reported superior outcomes with the extraperitoneal approach and inverted Y-V plasty. The authors reported a success rate of 83.3% in a 30-patient series.
Of note, if the patient is incontinent pre-operatively or develops de-novo incontinence at a later stage then the abdominal approach could improve durability of an AUS due to the lack of perineal scarring.12,17
Perineal dissection is similar to radical perineal prostatectomy. Although it is mainly preferred for more distal strictures, it has been used as an alternative to avoid entering rigid perivesical tissue. Extensive urethral mobilisation can result in a high risk of devascularising and injuring the external sphincter, which is reflected by high incontinence rates associated with this approach in the literature (Table 2). To this end, a high proportion of these patients ultimately require artificial sphincter surgery at some stage.22,95 The patient is usually placed in an exaggerated lithotomy position and a simple vertical, “Y”, “lambda” or “half-moon” perineal incision is used. The proximal bulbo-membranous urethra is mobilised, similar to a trans-perineal bulbar urethroplasty with division of the bulbospongiosus muscle and central perineal tendon with or without division of corpus spongiosum. The distal extent of the scar tissue is identified, with or without the aid of a flexible ureteroscope and the urethra is transected at that level. To identify the proximal extent of the scar, the vesicourethral wall and bladder base must be dissected away from surrounding tissue including the rectal wall. The crura often needs to be divided or inferior partial pubectomy performed to facilitate surgical access and to re-create an adequate bladder neck with a tension-free anastomosis. In cases of complete obliteration, access can be facilitated by use of a flexible cystoscope via a supra-pubic catheter tract. Opening of the bladder neck can then be done with the aid of endoscopic visualisation.19,22,24,63,67,68,91,95,96
A modified perineal approach has been recently described by Pinto et al69 and is referred to as the Anterior Sagittal Transrectal Approach (ASTRA). The authors described a technique where the patient is placed in a Jackknife position. A vertical incision is made through the perineum with extension into the anterior border of the rectum, which allows for an improved access to the bladder neck and avoiding a pubectomy. The authors reported that 92 such ASTRA procedures have been performed with no incidence of fecal incontinence, similar rates of urinary incontinence to the conventional perineal approach and two cases of rectourethral fistula in previously irradiated patients.
Finally, a robotic approach has also been described for perineal dissection in 2021 by Simsek et al.71 The robot is used more as an adjunct for tissue visualisation with the camera arm rather than the traditional dissection with working robot arms. This can allow for extended dissection with corporal separation and pubectomy to be avoided and facilitates creation of the anastomosis and facilitates ergonomic operating. A success rate of 81.3% was reported.
For the abdomino-perineal approach, patients are often not placed in an exaggerated lithotomy position. Anatomical landmarks can be more challenging to identify during perineal dissection, especially between the bladder anastomosis and anterior rectal wall. This combined approach is best utilised in longer strictures (>3cm) and especially in those with prior RTx to the pelvis.70,73,74 With this method, maximal scar excision is allowed for as well as a higher success rate for creating a patent lumen. However, this is arguably most extensive of the approaches and can result in a longer post-operative recovery for the patients. However, bearing this in mind, there have been two robotic approaches described including a “single port” access.72,97
Closure of Defect and Anastomosis
Following excision of the stricture, a tension-free and water-tight anastomosis with a wide enough lumen must be fashioned. The most commonly described technique is an end-to-end anastomosis following mobilisation of the urethra and bladder base, with or without spatulation of the healthy urethra. This is the preferred option if the tissue is malleable.12,85,96 However, if the defect is larger than expected and the primary anastomosis would be under tension then the gap can be bridged with variety of autologous grafts, flaps or augmentation techniques.
Grafts
Since early 1990s, the most popular graft material has been buccal mucosa. This was first described by Sepezhko et al in 1894 and re-investigated by Burger et al in 1992.98,99 It is primarily used in anterior urethral strictures with good success rates. However, it has also been applied by Shahrour et al in 201767 via a perineal approach, Bozkurt et al in 202260 via a trans-abdominal onlay technique and Liu et al in 202297 via the abdomino-perineal approach with reports showing success rates between 89% and 100%. However, Orandi et al in 1968100 reported that any part of the genital skin can be used as a patch with a dartos pedicle. As such, there are several reports with the use of penile skin grafts being employed in the context of rBNC.73,74,101 There are a multitude of options for graft orientations (dorsal or ventral onlay, double inlay, subtrigonal inlay, etc.), but there is no data to support the superiority of one particular technique.
Flaps
Following approximation of the tissue for the anastomosis, it can be further reinforced by numerous flaps with a goal to improve tissue vascularity and promote healing. For abdominal procedures, it is often the omental pedicle flap,102 peritoneal or rectus abdominis muscle flap based on inferior epigastric artery that is chosen. For those with perineal access, gracilis, penile fasciocutaneous flap or dartos pedicle flaps can be used.73,74,97
Augmentation
In cases where complete scar excision is not feasible, various augmentations can be used as an alternative. Most known is the YV-plasty, first described by Young in 1953103 and involves identification of the contracture, division of anterior bladder wall in an inverted “Y” incision and then reconstruction of the bladder neck into a “V” shaped incision.88 Although this procedure is more commonly described in rBNC following surgery for bladder outflow obstruction with the prostate still in situ, it has been described after RP with success rates between 83.3% and 100%.61,65,88 Recently, a modification, the T-plasty, has also been described by Reiss et al.103 However, it is yet to be applied in the setting of a rBNC post RP patient sample.
Another alternative is an anterior bladder flap (also known as tubularisation of the bladder neck) which was first described in 1972 by Tanagho for treatment of urinary incontinence.104 Its aim is to imitate the urethral sphincter by tubulising the circularly oriented muscle fibers of the anterior bladder wall.105 It was trialed by Boccan-Giddon in 198566 in a mixed group of 10 patients with incontinence after both simple retropubic or transurethral prostatectomy. Although only 3 patients in the cohort had bladder neck stenosis, the success rate was 80% and of note, the two failures were in patients after suprapubic prostatectomy with a fibrotic anterior bladder wall. Most recently, Zhao et al in 2022,62 have reported their experience with trans-abdominal robotic VUAS reconstruction using the anterior bladder flap technique Although a series of only nine patients, the success rate was 78% for patency and 100% for continence.
Finally, Simonato et al26 have a described a “pull-through urethroplasty” approach, performed via combined suprapubic and perineal approach where the scar is resected perineally and healthy urethra is gently pulled through the suprapubic tract, placed under traction and sutured to the pelvic diaphragm with interrupted sutures. This is then followed by delayed insertion of AUS with an overall success rate of 91%.
Conclusion
rBNC post RP is relatively uncommon but the associated functional burden for patients is clinically significant and the surgical management can present many challenges. While endoscopic and minimally invasive methods can be attempted initially, open or robotic surgical reconstruction is usually required. A tailored surgical plan is required that takes into consideration the most appropriate access and method for vesicourethral anastomotic reconstruction. Consideration needs to be made for the continence status. Given the complexity and associated risks, thorough patient counselling is essential.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: Https://GcoIarcFr/Today.
2. Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet. 2017;389(10071):815–822. doi:10.1016/S0140-6736(16)32401-1
3. Valerio M, Anele C, Bott SRJ, et al. The Prevalence of Clinically Significant Prostate Cancer According to Commonly Used Histological Thresholds in Men Undergoing Template Prostate Mapping Biopsies. J Urol. 2016;195(5):1403–1408. doi:10.1016/J.JURO.2015.11.047
4. Chen J, Oromendia C, Halpern JA, Ballman KV. National trends in management of localized prostate cancer: a population based analysis 2004-2013. Prostate. 2018;78(7):512–520. doi:10.1002/PROS.23496
5. Hamdy FC, Donovan JL, Lane JA, et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N Eng J Med. 2016;375(15):1415–1424. doi:10.1056/NEJMoa1606220
6. Elliott SP, Meng MV, Elkin EP, McAninch JW, Duchane J, Carroll PR. Incidence of Urethral Stricture After Primary Treatment for Prostate Cancer: data From CaPSURE. J Urol. 2007;178(2):529–534. doi:10.1016/j.juro.2007.03.126
7. Nicholson HL, Al-Hakeem Y, Maldonado JJ, Tse V. Management of bladder neck stenosis and urethral stricture and stenosis following treatment for prostate cancer. Transl Androl Urol. 2017;6:S92–102. doi:10.21037/tau.2017.04.33
8. LaBossiere JR, Cheung D, Rourke K. Endoscopic Treatment of Vesicourethral Stenosis after Radical Prostatectomy: outcomes and Predictors of Success. J Urol. 2016;195(5):1495–1500. doi:10.1016/j.juro.2015.12.073
9. Lumen N, Campos-Juanatey F, Dimitropoulos K, Greenwell T. European Association of Urology Guidelines on Urethral Strictures. EAU Guidelines. 2023.
10. Wessells H, Morey A, Souter L, Rahimi L, Vanni A. Urethral Stricture Disease Guideline Amendment (2023). J Urol. 2023;210(1):64–71. doi:10.1097/JU.0000000000003482
11. Abbasi B, Shaw NM, Lui JL, et al. Posterior urethral stenosis: a comparative review of the guidelines. World J Urol. 2022;40(11):2591–2600. doi:10.1007/s00345-022-04131-y
12. Rocco NR, Zuckerman JM. An update on best practice in the diagnosis and management of post-prostatectomy anastomotic strictures. Ther Adv Urol. 2017;9(5):99–110. doi:10.1177/1756287217701391
13. Parihar JS, Ha Y-S, Kim IY. Bladder neck contracture-incidence and management following contemporary robot assisted radical prostatectomy technique. Prostate Int. 2014;2:12–18. doi:10.12954/PI.13034
14. Erickson BA, Meeks JJ, Roehl KA, Gonzalez CM, Catalona WJ. Bladder neck contracture after retropubic radical prostatectomy: incidence and risk factors from a large single-surgeon experience. BJU Int. 2009;104:1615–1619. doi:10.1111/j.1464-410X.2009.08700.x
15. Rosenbaum CM, Fisch M, Vetterlein MW. Contemporary Management of Vesico-Urethral Anastomotic Stenosis After Radical Prostatectomy. Front Surg. 2020;7. doi:10.3389/fsurg.2020.587271
16. Modig KK, Godtman RA, Bjartell A, et al. Vesicourethral Anastomotic Stenosis After Open or Robot-assisted Laparoscopic Retropubic Prostatectomy—Results from the Laparoscopic Prostatectomy Robot Open Trial. Eur Urol Focus. 2021;7(2):317–324. doi:10.1016/j.euf.2019.10.012
17. Branche B, Crocerossa F, Carbonara U, et al. Management of Bladder Neck Contracture in the Age of Robotic Prostatectomy: an Evidence-based Guide. Eur Urol Focus. 2022;8(1):297–301. doi:10.1016/j.euf.2021.01.007
18. Selvi I, Arik AI, Basay MS, Basar H. The effect of proliferative hypertrophic scars on determining treatment options for preventing recurrence of vesicourethral anastomotic stenosis after radical prostatectomy: a single-center cross-sectional study. Sao Paulo Medical Journal. 2021;139(3):241–250. doi:10.1590/1516-3180.2020.0349.r1.28012021
19. Schuettfort VM, Dahlem R, Kluth L, et al. Transperineal reanastomosis for treatment of highly recurrent anastomotic strictures after radical retropubic prostatectomy: extended follow-up. World J Urol. 2017;35(12):1885–1890. doi:10.1007/s00345-017-2067-8
20. Theodorou C, Katsifotis C, Stournaras P, Moutzouris G, Katsoulis A, Floratos D. Abdomino–Perineal Repair of Recurrent and Complex Bladder Neck–Prostatic Urethra Contractures. Eur Urol. 2000;38(6):734–741. doi:10.1159/000020371
21. Pfalzgraf D, Beuke M, Isbarn H, et al. Open Retropubic Reanastomosis for Highly Recurrent and Complex Bladder Neck Stenosis. J Urol. 2011;186(5):1944–1947. doi:10.1016/j.juro.2011.07.040
22. Simonato A, Ennas M, Benelli A, et al. Comparison between Two Different Two-Stage Transperineal Approaches to Treat Urethral Strictures or Bladder Neck Contracture Associated with Severe Urinary Incontinence that Occurred after Pelvic Surgery: report of Our Experience. Adv Urol. 2012;2012:1–6. doi:10.1155/2012/481943
23. Kirshenbaum EJ, Zhao LC, Myers JB, et al. Patency and Incontinence Rates After Robotic Bladder Neck Reconstruction for Vesicourethral Anastomotic Stenosis and Recalcitrant Bladder Neck Contractures: the Trauma and Urologic Reconstructive Network of Surgeons Experience. Urology. 2018;118:227–233. doi:10.1016/j.urology.2018.05.007
24. Giúdice CR, Lodi PE, Olivares AM, et al. Safety and effectiveness evaluation of open reanastomosis for obliterative or recalcitrant anastomotic stricture after radical retropubic prostatectomy. Int Braz j Urol. 2019;45(2):253–261. doi:10.1590/s1677-5538.ibju.2017.0681
25. The National Health Service England. 2022/23 National Tariff Payment System documents 2022. Available from: https://www.england.nhs.uk/publication/national-tariff-payment-system-documents-annexes-and-supporting-documents/.
26. Simonato A, Gregori A, Lissiani A, Varca V, Carmignani G. Use of Solovov-Badenoch principle in treating severe and recurrent vesico-urethral anastomosis stricture after radical retropubic prostatectomy: technique and long-term results. BJU Int. 2012;110:E456–60. doi:10.1111/j.1464-410X.2012.11132.x
27. Ramchandani P, Banner MP, Berlin JW, Dannenbaum MS, Wein AJ. Vesicourethral anastomotic strictures after radical prostatectomy: efficacy of transurethral balloon dilation. Radiology. 1994;193(2):345–349. doi:10.1148/radiology.193.2.7972741
28. Yurkanin JP, Dalkin BL, Cui H. Evaluation of cold knife urethrotomy for the treatment of anastomotic stricture after radical retropubic prostatectomy. J Urol. 2001;165(5):1545–1548. doi:10.1016/S0022-5347(05)66345-8
29. Pfalzgraf D, Worst T, Kranz J, et al. Vesico-urethral anastomotic stenosis following radical prostatectomy: a multi-institutional outcome analysis with a focus on endoscopic approach, surgical sequence, and the impact of radiation therapy. World J Urol. 2021;39(1):89–95. doi:10.1007/s00345-020-03157-4
30. Dalkin BL. Endoscopic evaluation and treatment of anastomotic strictures after radical retropubic prostatectomy. J Urol. 1996;155(1):206–208. doi:10.1016/S0022-5347(01)66595-9
31. Surya BV, Provet J, Johanson K-E, Brown J. Anastomotic Strictures Following Radical Prostatectomy: risk Factors and Management. J Urol. 1990;143(4):755–758. doi:10.1016/S0022-5347(17)40082-6
32. Veerman H, Vis AN, Hagens MJ, et al. Surgical and Functional Outcomes of Bladder Neck Incision for Primary Vesico-Urethral Anastomosis Stricture after Robot-assisted Radical Prostatectomy are Influenced by the Presence of Pre- or Postoperative Radiotherapy. Urology. 2022;166:216–222. doi:10.1016/j.urology.2022.03.015
33. Giannarini G, Manassero F, Mogorovich A, et al. Cold-Knife Incision of Anastomotic Strictures after Radical Retropubic Prostatectomy with Bladder Neck Preservation: efficacy and Impact on Urinary Continence Status. Eur Urol. 2008;54(3):647–656. doi:10.1016/j.eururo.2007.12.013
34. Popken G, Sommerkamp H, Schultze-Seemann W, Wetterauer U, Katzenwadel A. Anastomotic Stricture after Radical Prostatectomy. Eur Urol. 1998;33(4):382–386. doi:10.1159/000019620
35. Geavlete B, Moldoveanu C, Iacoboaie C, Geavlete P. Bipolar plasma vaporization versus standard transurethral resection in secondary bladder neck sclerosis: a prospective, medium-term, randomized comparison. Ther Adv Urol. 2013;5(2):75–83. doi:10.1177/1756287212470695
36. Bader MJ, Tilki D, Gratzke C, Sroka R, Stief CG, Reich O. Ho:YAG-laser: treatment of vesicourethral strictures after radical prostatectomy. World J Urol. 2010;28(2):169–172. doi:10.1007/s00345-010-0520-z
37. Bach T, Herrmann TRW, Cellarius C, Gross AJ. Bladder neck incision using a 70 W 2 micron continuous wave laser (RevoLix). World J Urol. 2007;25:263–267. doi:10.1007/s00345-007-0169-4
38. Lagerveld BW, Laguna MP, Debruyne FMJ, De La Rosette JJMCH. Holmium:YAG Laser for Treatment of Strictures of Vesicourethral Anastomosis after Radical Prostatectomy. J Endourol. 2005;19(4):497–501. doi:10.1089/end.2005.19.497
39. Hayashi T, Asushi Y, Ohno R, et al. Successful treatment of recurrent vesicourethral stricture after radical prostatectomy with holmium laser: report of three cases. Int J Urol. 2005;12(4):414–416. doi:10.1111/j.1442-2042.2005.01053.x
40. Öztürk H. Treatment of recurrent vesicourethral anastomotic stricture after radical prostatectomy using plasma-button vaporization. Scand J Urol. 2015;49(5):371–376. doi:10.3109/21681805.2015.1012115
41. Shinchi M, Horiguchi A, Ojima K, et al. Deep lateral transurethral incision for vesicourethral anastomotic stenosis after radical prostatectomy. Int J Urol. 2021;28(11):1120–1126. doi:10.1111/iju.14650
42. Ramirez D, Simhan J, Hudak SJ, Morey AF. Standardized Approach for the Treatment of Refractory Bladder Neck Contractures. Urologic Clinics of North America. 2013;40(3):371–380. doi:10.1016/j.ucl.2013.04.012
43. Nealon SW, Bhanvadia RR, Badkhshan S, Sanders SC, Hudak SJ, Morey AF. Transurethral Incisions for Bladder Neck Contracture: comparable Results without Intralesional Injections. J Clin Med. 2022;11(15):4355. doi:10.3390/jcm11154355
44. Mobilio G, Cosciani Cunico S, Petracco S. Guided Dilatation and Transurethral Resection in One Session for the Treatment of the Postprostatectomy Obstructive Complications above the Verumontanum. Endoscopy. 1977;9(01):13–19. doi:10.1055/s-0028-1098478
45. Chiou RK, Howe S, Morton JJ, Grune MT, Taylor RJ. Treatment of recurrent vesicourethral anastomotic stricture after radical prostatectomy with endourethroplasty. Urology. 1996;47(3):422–425. doi:10.1016/S0090-4295(99)80465-8
46. Kuyumcuoglu U, Eryildirim B, Tarhan F, Faydaci G, Ozgül A, Erbay E. Antegrade Endourethroplasty with Free Skin Graft for Recurrent Vesicourethral Anastomotic Strictures After Radical Prostatectomy. J Endourol. 2010;24(1):63–67. doi:10.1089/end.2009.0076
47. Abramowitz DJ, Balzano FL, Ruel NH, Chan KG, Warner JN. Transurethral Incision with Transverse Mucosal Realignment for the Management of Bladder Neck Contracture and Vesicourethral Anastomotic Stenosis. Urology. 2021;152:102–108. doi:10.1016/j.urology.2021.02.035
48. Vanni AJ, Zinman LN, Buckley JC. Radial Urethrotomy and Intralesional Mitomycin C for the Management of Recurrent Bladder Neck Contractures. J Urol. 2011;186(1):156–160. doi:10.1016/j.juro.2011.03.019
49. Hacker EC, Maganty A, Pere MM, Rusilko PJ. Outcomes of Vesicourethral Anastomotic Stenosis and Bladder Neck Contracture With Direct Visual Internal Urethrotomy With Mitomycin-C After Prostate Cancer Treatment. Urology. 2022;165:331–335. doi:10.1016/j.urology.2022.01.041
50. Rozanski AT, Zhang LT, Holst DD, Copacino SA, Vanni AJ, Buckley JC. The Effect of Radiation Therapy on the Efficacy of Internal Urethrotomy With Intralesional Mitomycin C for Recurrent Vesicourethral Anastomotic Stenoses and Bladder Neck Contractures: a Multi-Institutional Experience. Urology. 2021;147:294–298. doi:10.1016/j.urology.2020.09.035
51. Sourial MW, Richard PO, Bettez M, Jundi M, Tu LM. Mitomycin-C and urethral dilatation: a safe, effective, and minimally invasive procedure for recurrent vesicourethral anastomotic stenoses. Urol Oncol. 2017;35(12):672.e15–672.e19. doi:10.1016/j.urolonc.2017.07.031
52. Redshaw JD, Broghammer JA, Smith TG, et al. Intralesional Injection of Mitomycin C at Transurethral Incision of Bladder Neck Contracture May Offer Limited Benefit: TURNS Study Group. J Urol. 2015;193(2):587–592. doi:10.1016/j.juro.2014.08.104
53. Lyon TD, Ayyash OM, Ferroni MC, Rycyna KJ, Chen ML. Bipolar Transurethral Incision of Bladder Neck Stenoses with Mitomycin C Injection. Adv Urol. 2015;2015:1–5. doi:10.1155/2015/758536
54. Yao HH, Sengupta S, Chee J. Incorporating intra-lesional injection of mitomycin C in the management algorithm for bladder neck contractures and vesicourethral anastomotic strictures. J Clin Urol. 2022;15(1):46–53. doi:10.1177/2051415820961901
55. Eltahawy E, Gur U, Virasoro R, Schlossberg SM, Jordan GH. Management of recurrent anastomotic stenosis following radical prostatectomy using holmium laser and steroid injection. BJU Int. 2008;102(7):796–798. doi:10.1111/j.1464-410X.2008.07919.x
56. Neu S, Vigil H, Locke JA, Herschorn S. Triamcinolone acetonide injections for the treatment of recalcitrant post-radical prostatectomy vesicourethral anastomotic stenosis: a retrospective look at efficacy and safety. Canadian Urol Assoc J. 2020;15. doi:10.5489/cuaj.6644
57. Shaw NM, Marhamati S, Friedman A, Sussman R, Venkatesan K. Recurrent vesicourethral anastomotic stenosis following treatment for prostate cancer: an effective endoscopic treatment using bipolar plasma button and triamcinolone. Int Urol Nephrol. 2022;54(5):1001–1008. doi:10.1007/s11255-022-03153-0
58. Kravchick S, Lobik L, Peled R, Cytron S. Transrectal Ultrasonography-Guided Injection of Long-Acting Steroids in the Treatment of Recurrent/Resistant Anastomotic Stenosis After Radical Prostatectomy. J Endourol. 2013;27(7):875–879. doi:10.1089/end.2012.0661
59. Farah RN, DiLoreto RR, Cerny JC. Transurethral resection combined with steroid injection in treatment of recurrent vesical neck contractures. Urology. 1979;13(4):395–397. doi:10.1016/0090-4295(79)90338-8
60. Bozkurt O, Sen V, Demir O, Esen A. Subtrigonal Inlay Patch Technique with Buccal Mucosa Graft for Recurrent Bladder Neck Contractures. Urol Int. 2022;106(3):256–260. doi:10.1159/000517894
61. Musch M, Hohenhorst JL, Vogel A, Loewen H, Krege S, Kroepfl D. Robot-assisted laparoscopic Y-V plasty in 12 patients with refractory bladder neck contracture. J Robot Surg. 2018;12:139–145. doi:10.1007/s11701-017-0708-y
62. Zhao CC, Shakir NA, Zhao LC. Robotic bladder flap posterior urethroplasty for recalcitrant bladder neck contracture and vesicourethral anastomotic stenosis. Urol Video J. 2022;13:100133. doi:10.1016/j.urolvj.2022.100133
63. Vitarelli A, Vulpi M, Divenuto L, Papapicco G, Pagliarulo V, Ditonno P. Prerectal-transperineal approach for treatment of recurrent vesico-urethral anastomotic stenosis after radical prostatectomy. Asian J Urol. 2021. doi:10.1016/j.ajur.2021.05.009
64. Diamant E, de la Taille A, Lavolle A, et al. Urethro-vesical anastomosis reconstruction using extra-peritoneal robot-assisted laparoscopy for anastomotic stenosis after radical prostatectomy. Progrès En Urologie. 2021;31:591–597. doi:10.1016/j.purol.2020.12.014
65. Abo Youssef N, Obrecht F, Padevit C, Brachlow J, John H. Short and Intermediate-Term Outcome of Robot-Assisted Inverted YV-Plasty for Recurrent Bladder Neck Stenosis - a Single Centre Study. Urology. 2023;175:196–201. doi:10.1016/j.urology.2023.02.011
66. Boccon-Gibod L, Benoit G, Steg A. Bladder Neck Reconstruction Using an Anterior Bladder Flap in Post-Prostatectomy Incontinence. Eur Urol. 1985;11:150–151. doi:10.1159/000472480
67. Shahrour W, Hodhod A, Kotb A, Prowse O, Elmansy H. Dorsal Buccal Mucosal Graft Urethroplasty for Vesico-Urethral Anastomotic Stricture Postradical Prostatectomy. Urology. 2019;130:210. doi:10.1016/j.urology.2019.04.022
68. Reiss CP, Pfalzgraf D, Kluth LA, Soave A, Fisch M, Dahlem R. Transperineal reanastomosis for the treatment for highly recurrent anastomotic strictures as a last option before urinary diversion. World J Urol. 2014;32(5):1185–1190. doi:10.1007/s00345-013-1180-6
69. Pinto LOAD, Westin LA, Kietzer KS, Teloken PE, Favorito LA. ASTRA – an alternative approach for the posterior urethra. Int Braz j Urol. 2023;49:161–162. doi:10.1590/s1677-5538.ibju.2022.0164
70. Schlossberg S, Jordan G, Schellhammer P. Repair of obliterative vesicourethral stricture after radical prostatectomy: a technique for preservation of continence. Urology. 1995;45(3):510–513. doi:10.1016/S0090-4295(99)80025-9
71. Simsek A, Danacioglu YO, Arikan Y, et al. Perineoscopic vesicourethral reconstruction: a novel surgical technique for anastomotic stricture following radical prostatectomy. Türk Üroloji Dergisi/Turkish Journal of Urology. 2021;47(1):51–57. doi:10.5152/tud.2020.20372
72. Dinerman BF, Hauser NJ, Hu JC, Purohit RS. Robotic-Assisted Abdomino-perineal Vesicourethral Anastomotic Reconstruction for 4.5 Centimeter Post-prostatectomy Stricture. Urol Case Rep. 2017;14:1–2. doi:10.1016/j.eucr.2017.05.005
73. Nikolavsky D, Blakely SA, Hadley DA, et al. Open reconstruction of recurrent vesicourethral anastomotic stricture after radical prostatectomy. Int Urol Nephrol. 2014;46(11):2147–2152. doi:10.1007/s11255-014-0816-9
74. Wessells H, Morey AF, McAninch JW. Obliterative vesicourethral strictures following radical prostatectomy for prostate cancer: reconstructive armamentarium. J Urol. 1998;160(4):1373–1375. doi:10.1016/S0022-5347(01)62540-0
75. Salant RL, Cohen MS, Warner RS. Neodymium: YAG laser treatment of postoperative bladder neck contractures. Urology. 1990;35(5):385–387. doi:10.1016/0090-4295(90)80077-Z
76. Wang K, Li Y, Teng J-F, Zhou H-Y, Xu D-F, Fan Y. Transurethral plasmakinetic resection of the prostate is a reliable minimal invasive technique for benign prostate hyperplasia: a meta-analysis of randomized controlled trials. Asian J Androl. 2015;17(1):135. doi:10.4103/1008-682X.138191
77. Kropfl D, Olschewski T, Seegenschmiedt MH. Endoluminale Brachytherapie zur Vorbeugung von rezidivierenden Strikturen nach Urethrotomia interna. Der Urologe, Ausgabe A. 2004;43:1254–1261. doi:10.1007/s00120-004-0630-6
78. Pang KH, Chapple CR, Chatters R, et al. A Systematic Review and Meta-analysis of Adjuncts to Minimally Invasive Treatment of Urethral Stricture in Men. Eur Urol. 2021;80(4):467–479. doi:10.1016/j.eururo.2021.06.022
79. Verweij PHM. Mitomycin C: mechanism of action, usefulness and limitations. Anticancer Drugs. 1990;1(1):5–13. doi:10.1097/00001813-199010000-00002
80. Wiafe B, Adesida A, Churchill T, Metcalfe P. Mesenchymal stem cells inhibit hypoxia-induced inflammatory and fibrotic pathways in bladder smooth muscle cells. World J Urol. 2018;36(7):1157–1165. doi:10.1007/s00345-018-2247-1
81. Bahouth Z, Moskovitz B, Halachmi S. Allium Stents: a Novel Solution for the Management of Upper and Lower Urinary Tract Strictures. Rambam Maimonides Med J. 2017;
82. Teke K, Bosnali E, Kara O, Ustuner M, Avci IE, Culha MM. Minimal invasive management of bladder neck contracture using Allium round posterior stent: the long-term results. Prostate Int. 2021;9(4):203–207. doi:10.1016/j.prnil.2021.05.004
83. de Graaf GW, Stijns PEF, Scheepens WA, van Moorselaar RJA, Hendrikx AJM. The Use of a Memokath Prostatic Stent for Obstructive Voiding Symptoms after Brachytherapy. Curr Urol. 2013;7(1):19–23. doi:10.1159/000343547
84. McNamara ER, Webster GD, Peterson AC. The UroLume Stent Revisited: the Duke Experience. Urology. 2013;82(4):933–936. doi:10.1016/j.urology.2013.06.017
85. Abbosov S, Sorokin N, Shomarufov A, et al. Bladder neck contracture as a complication of prostate surgery: alternative treatment methods and prospects (literature review). Urol Sci. 2022;33(2):49. doi:10.4103/UROS.UROS_127_21
86. Young HH. Treatment of Complete Rupture of the Posterior Urethra, Recent or Ancient, by Anastomosis. J Urol. 1929;21(4):417–450. doi:10.1016/S0022-5347(17)73112-6
87. Young BW, Niebel JD. Vesico-Urethroplasty for Congenital Vesical Neck Obstruction in Children. J Urol. 1958;79(5):838–843. doi:10.1016/S0022-5347(17)66353-5
88. Granieri MA, Weinberg AC, Sun JY, Stifelman MD, Zhao LC. Robotic Y-V Plasty for Recalcitrant Bladder Neck Contracture. Urology. 2018;117:163–165. doi:10.1016/j.urology.2018.04.017
89. Capibaribe DM, Avilez ND, Sacomani CAR, Lucena ASP, Reis LO. Robotic approach to vesicourethral anastomotic stenosis and resection of remaining prostate after radical prostatectomy. Int Braz j Urol. 2023;49:158–160. doi:10.1590/s1677-5538.ibju.2022.0249
90. Shakir NA, Alsikafi NF, Buesser JF, et al. Durable Treatment of Refractory Vesicourethral Anastomotic Stenosis via Robotic-assisted Reconstruction: a Trauma and Urologic Reconstructive Network of Surgeons Study. Eur Urol. 2022;81(2):176–183. doi:10.1016/j.eururo.2021.08.013
91. Savun M, Ozdemir H, Keskin ET, Colakoglu Y, Canat HL, Simsek A. Open Vs. Robotic-Assis Reconstruction Vesicourethral Anastomotic Stenosis. AUA Journals. 2023. doi:10.1097/JU.0000000000003333.04
92. Bearrick EN, Findlay BL, Maciejko LA, Hebert KJ, Anderson KT, Viers BR. Robotic Urethral Reconstruction Outcomes in Men With Posterior Urethral Stenosis. Urology. 2022;161:118–124. doi:10.1016/j.urology.2021.11.035
93. Grosso AA, Di Maida F, Lambertini L, et al. Robotic reconstruction of vesico-urethral anastomosis stenosis: a descriptive technique and short-term results. Cent European J Urol. 2022;75:227. doi:10.5173/ceju.2022.0048
94. Lavollé A, de la Taille A, Chahwan C, et al. Extraperitoneal Robot-Assisted Vesicourethral Reconstruction to Manage Anastomotic Stricture Following Radical Prostatectomy. Urology. 2019;133:129–134. doi:10.1016/j.urology.2019.07.027
95. Ojima K, Horiguchi A, Shinchi M, et al. Transperineal bulbovesical anastomosis for extensive posterior urethral stenoses after treatment of prostatic disease. Int J Urol. 2022;29(12):1511–1516. doi:10.1111/iju.15029
96. Mundy AR, Andrich DE. Posterior urethral complications of the treatment of prostate cancer. BJU Int. 2012;110:304–325. doi:10.1111/j.1464-410X.2011.10864.x
97. Liu W, Shakir N, Zhao LC. Single-Port Robotic Posterior Urethroplasty Using Buccal Mucosa Grafts: technique and Outcomes. Urology. 2022;159:214–221. doi:10.1016/j.urology.2021.07.049
98. Korneyev I, Ilyin D, Schultheiss D, Chapple C. The First Oral Mucosal Graft Urethroplasty Was Carried Out in the 19th Century: the Pioneering Experience of Kirill Sapezhko (1857–1928). Eur Urol. 2012;62(4):624–627. doi:10.1016/j.eururo.2012.06.035
99. Bürger RA, Müller SC, El-Damanhoury H, Tschakaloff A, Riedmiller H, Hohenfellner R. The Buccal Mucosal Graft For Urethral Reconstruction: a Preliminary Report. J Urol. 1992;147:662–664. doi:10.1016/S0022-5347(17)37340-8
100. Orandi A. One-Stage Urethroplasty. Br J Urol. 1968;40(6):717–719. doi:10.1111/j.1464-410X.1968.tb11872.x
101. Özgök Y, Tan MÖ, Kilciler M, Tahmaz L, Erduran D. Use of bladder mucosal graft for urethral reconstruction. Int J Urol. 2000;7(10):355–360. doi:10.1046/j.1442-2042.2000.00210.x
102. Wein AJ, Malloy TR, Greenberg SH, Carpiniello VL, Murphy JJ. Omental Transposition as an Aid in Genitourinary Reconstructive Procedures. J Trauma. 1980;20(6):473–477. doi:10.1097/00005373-198006000-00007
103. Reiss CP, Rosenbaum CM, Becker A, et al. The T-plasty: a modified YV-plasty for highly recurrent bladder neck contracture after transurethral surgery for benign hyperplasia of the prostate: clinical outcome and patient satisfaction. World J Urol. 2016;34(10):1437–1442. doi:10.1007/s00345-016-1779-5
104. Tanagho EA, Smith DR, Meyers FH, Fisher R. Mechanism of Urinary Continence. II. Technique for Surgical Correction of Incontinence. J Urol. 1969;101(3):305–313. doi:10.1016/S0022-5347(17)62333-4
105. Beck PH, Mcaninch JW, Stutzman RE. Anterior Bladder Tube Flap Reconstruction of the Urethrovesical Neck After Radical Retropubic Prostatectomy. J Urol. 1979;121(3):379–381. doi:10.1016/S0022-5347(17)56795-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.