")
Back to Journals » Journal of Inflammation Research » Volume 17
Redox Biomarkers – An Effective Tool for Diagnosing COVID-19 Patients and Convalescents
Authors Wolszczak-Biedrzycka B , Dorf J , Matowicka-Karna J , Dymicka-Piekarska V , Wojewódzka-Żeleźniakowicz M, Żukowski P, Zalewska A , Dąbrowski Ł, Maciejczyk M
Received 27 December 2023
Accepted for publication 2 April 2024
Published 26 April 2024 Volume 2024:17 Pages 2589—2607
DOI https://doi.org/10.2147/JIR.S456849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Blanka Wolszczak-Biedrzycka,1 Justyna Dorf,2 Joanna Matowicka-Karna,2 Violetta Dymicka-Piekarska,2 Marzena Wojewódzka-Żeleźniakowicz,3 Piotr Żukowski,4 Anna Zalewska,5 Łukasz Dąbrowski,6 Mateusz Maciejczyk7
1Department of Psychology and Sociology of Health and Public Health, University of Warmia and Mazury in Olsztyn, Olsztyn, Poland; 2Department of Clinical Laboratory Diagnostics, Medical University of Bialystok, Bialystok, Poland; 3Department of Emergency Medicine and Disasters, Medical University of Bialystok, Bialystok, Poland; 4Department of Restorative Dentistry, Croydon University Hospital, London, UK; 5Independent Laboratory of Experimental Dentistry, Medical University of Bialystok, Bialystok, Poland; 6Medical Laboratory, “Diagnostyka” Olsztyn, Olsztyn, Poland; 7Department of Hygiene, Epidemiology and Ergonomics, Medical University of Bialystok, Bialystok, Poland
Correspondence: Blanka Wolszczak-Biedrzycka, Email [email protected]
Aim: COVID-19 triggers the overproduction of reactive oxygen species (ROS) which, in combination with a weakened antioxidant barrier, can lead to protein oxidation and lipid peroxidation. The aim of this study was to evaluate enzymatic and non-enzymatic antioxidants, the overall redox potential, and protein and lipid peroxidation products in COVID-19 patients, convalescents, and healthy subjects, and to the determine the diagnostic applicability of these parameters in COVID-19 patients.
Materials and Methods: The study involved 218 patients with COVID-19, 69 convalescents, and 48 healthy subjects who were selected for the research based on age and sex. The study was conducted between 20 February 2021 and 20 November 2021 in Białystok, Poland. The antioxidant barrier, redox status, and oxidative damage products were assessed in serum/plasma samples with the use of colorimetric and spectrophotometric assays.
Results: Glutathione reductase (GR) activity was higher, whereas total antioxidant capacity (TAC) was lower in COVID-19 patients than in convalescents (p< 0.0001) and the control group (p< 0.0001). The concentrations of advanced glycation end products (AGEs), advanced oxidation protein products (AOPP), 4-hydroxynonenal (4-HNE), and malondialdehyde (MDA) were higher in COVID-19 patients (p< 0.0001) and convalescents (p< 0.0001) than in the control group. AGEs were the most effective diagnostic biomarker for differentiating COVID-19 patients from the control group (AUC=0.9971) and convalescents from the control group (AUC=1.000).
Conclusion: An infection with the SARS-CoV-2 disrupts the redox balance and increases protein oxidation and lipid peroxidation. AGEs fulfill the criteria for a potential diagnostic biomarker in COVID-19 patients and convalescents.
Keywords: oxidative stress, redox biomarkers, antioxidants, COVID-19, SARS CoV-2 virus
Introduction
The pathogenesis of the infection caused by the SARS-CoV-2 has not been fully elucidated to date. The immune response to the infection is complex and highly individualized, which undoubtedly affects the severity of disease symptoms and complications after the infection.1 Research has shown that severe COVID-19 is not directly caused by the SARS-CoV-2, but by the cytokine storm which increases the production of reactive oxygen species (ROS) that induce oxidative stress.2 An infection caused by the SARS-CoV-2 leads to the activation of neutrophils and mononuclear phagocytic cells which are largely responsible for the massive release of ROS in lung tissues.3 In addition, the SARS-CoV-2 reaches lung cells via the angiotensin-converting enzyme 2 (ACE2) receptor, and an imbalance between the rate of ROS production and antioxidant processes may lead to oxidative damage to proteins, lipids, and nucleic acids.4 Glutathione (GSH) is one of the key components of the antioxidant barrier, and it can prevent the S1 subunit of the SARS-CoV-2 spike protein from binding to the ACE2 receptor in the lungs.5 According to the literature, an endogenous deficiency of GSH and other antioxidants, including superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), and glutathione reductase (GR), can affect the severity of COVID-19.6
It is generally known that COVID-19 can lead to post-infection complications and increases the risk of inflammatory,7,8 metabolic, and neurodegenerative diseases which are also caused by an oxidation-reduction (redox) imbalance.9 Therefore, oxidative stress parameters and antioxidant levels should be compared in convalescents vs individuals without a history of SARS-CoV-2 infection and COVID-19 patients.
Oxidative stress exerts a complex influence on the pathogenesis and severity of COVID-19, which is why selected parameters should be evaluated and compared in COVID-19 patients, convalescents, and healthy controls, including in reference to the severity of COVID-19 assessed on the Modified Early Warning Score (MEWS) scale. These parameters include markers of antioxidant capacity (SOD, CAT, GPx, GSH), redox balance (total antioxidant capacity - TAC, total oxidative status - TOS, and oxidative stress index - OSI, calculated as the TOS/TAC ratio), oxidative protein damage (advanced glycation end products - AGEs and advanced oxidation protein products - AOPP), and oxidative lipid damage (4-hydroxynonenal - 4-HNE and malondialdehyde - MDA). The results of the study can improve diagnostic strategies for patients infected with SARS-CoV-2, contribute to effective monitoring of patients, and enable reliable assessments of the risk of severe COVID-19 resulting from a redox imbalance. An evaluation of the diagnostic efficacy of selected parameters based on the area under the receiver operating characteristic (ROC) curve (AUC) in COVID-19 patients and convalescents, as well as assessments of disease severity can also contribute to the development of effective therapeutic strategies.
Materials and Methods
Description of the Study
A single-center study involving COVID-19 patients admitted to the Emergency Department of the Clinical Hospital of the Medical University of Białystok and convalescents was conducted between 20 February 2021 and 20 November 2021. The study was approved by the Bioethics Committee of the Medical University of Białystok (decision No. APK.002.26.2021 of 28 January 2021). All participants gave their written consent to participate in the study.
Characteristics of COVID-19 Patients
The study group consisted of 218 unvaccinated patients (115 men and 103 women aged 26–87) who tested positive for the presence of SARS-CoV-2 genetic material in nasopharyngeal swabs in the PCR assay. Nasal and throat specimens for the analysis were collected upon hospital admission, after the COVID-19 infection had been recognized.
The severity of COVID-19 symptoms was assessed on the MEWS scale.10 The patients were divided into four groups based on the following diagnostic parameters: blood pressure, heart rate, respiratory rate, body temperature, and neurological symptoms: MEWS 1 – asymptomatic and mildly symptomatic infection, MEWS 2 – symptomatic infection with pneumonia without symptoms of respiratory failure, MEWS 3 – symptomatic infection with pneumonia and symptoms of respiratory failure, and MEWS 4 – symptomatic infection with multiple organ failure (Table 1).
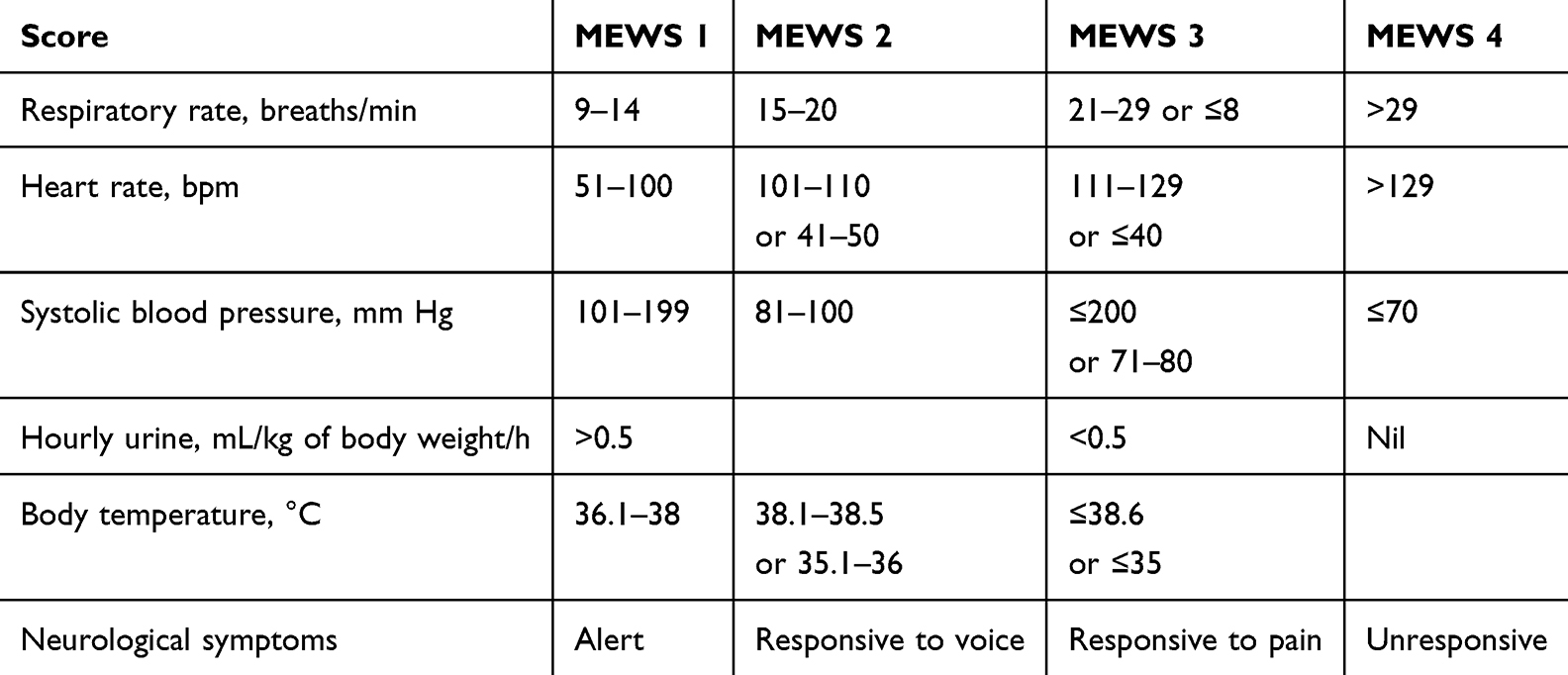 |
Table 1 Modified Early Warning Score (MEWS) |
COVID-19 patients were subjected to the following laboratory tests: hematological analyses (peripheral blood cell morphology), biochemical analyses (CRP, AST, ALT, creatinine, glucose, Na, K), coagulation tests (INR, D-dimers), and imaging tests (radiograph and computed tomography scan of the chest). Patient demographics, time of hospital stay, comorbidities (hematological disorders, diabetes, hypertension, obesity, coronary heart disease, cancer), and clinical symptoms (fever, cough, dyspnea, acute respiratory distress syndrome, gastrointestinal symptoms) were also evaluated.
Characteristics of Convalescents
The group of convalescents consisted of 69 unvaccinated individuals (30 women and 39 men aged 25–68) with a history of COVID-19 and without any comorbidities. Individuals who tested positive for the presence of SARS-CoV-2 genetic material in the PCR assay, had undergone compulsory quarantine, tested negative in the PCR assay at least 14 days prior to the study, and showed no clinical symptoms of COVID-19 were classified as convalescents.11 In this group of participants, biological specimens for analyses were collected 14 to 30 days after a negative result of the PCR test for the SARS-CoV-2.
Characteristics of the Control Group
The control group consisted of 48 healthy unvaccinated individuals of both sexes (28 women and 20 men aged 26–68) without a history of COVID-19 (absence of anti-SARS-CoV antibodies) or comorbidities who had visited the LAB110 laboratory in Białystok for routine tests.
Blood Collection
Oxidative stress parameters were determined in a fasting blood test, where samples of venous blood were collected from all COVID-19 patients, convalescents, and healthy controls with the use of S-Monovette K3 EDTA and S-Monovette® tubes (Sarstedt, Germany) (the participants had not engaged in intensive physical activity for 24 hours before blood collection). Directly after sampling, blood was centrifuged at 4000 × g for 10 minutes at a temperature of 4°C (MPW 351, MPW Med. Instruments, Warsaw, Poland). The plasma and the serum were separated from morphotic blood elements, protected against oxidation (through the addition of 10 µL of 0.5 M BHT/1 mL of serum/plasma), and stored at a temperature of −80°C for less than six months before analysis.
Redox Assay
The reagents for the redox assay were supplied by Sigma-Aldrich (Germany) or St. Louis (MO, USA) (unless indicated otherwise). Absorbance and fluorescence were measured with the Infinite M200 PRO multimode microplate reader (Tecan Group Ltd., Männedorf, Switzerland). Fluorescence was measured in 96-well black microplates. All tests were performed in duplicate, and the results were standardized to 1 mg of total protein. Total protein content was determined with the use of a spectrophotometer (Thermo Scientific PIERCE BCA Protein Assay; Rockford, Illinois, USA).
Antioxidant Enzymes and Non-Enzymatic Antioxidants
The antioxidant barrier was evaluated by measuring the activity of antioxidant enzymes (SOD, CAT, GPx, and GR) and the concentration of GSH as a non-enzymatic antioxidant.
Superoxide dismutase activity was determined in a colorimetric assay by measuring the inhibition of adrenalin oxidation at a wavelength of 480 nm.12.
Catalase activity was determined in a colorimetric assay by measuring the decomposition rate of hydrogen peroxide (H2O2) at a wavelength of 240 nm.13
The activity of GPx was determined in a colorimetric assay by measuring the oxidation rate of NADPH (reduced form of nicotinamide adenine dinucleotide phosphate) at a wavelength of 340 nm.14
Glutathione reductase activity was determined in a colorimetric assay by measuring the oxidation rate of NADPH at a wavelength of 240 nm.15
The concentration of GSH was determined in a colorimetric assay in an enzymatic reaction with 5,5-dithio-bis-(2-nitrobenzoic acid) (DTNB), NADPH, and GR.16
Redox Status
The overall redox status was determined by measuring total antioxidant capacity (TAC) in a colorimetric assay (changes in the absorbance of 2.2’-azino-bis(3-ethylbenzothiazoline-6-sulfonic acid), ABTS+) at a wavelength of 660 nm17 and total oxidative status (TOS) in a colorimetric assay (by measuring the oxidation of the ferrous ion to the ferric ion in the presence of oxidant species).18 The oxidative stress index (OSI) was calculated with the use of the following formula: ( ).19
).19
Oxidative Damage to Proteins and Lipids
The content of AGEs was determined in a fluorescence assay by measuring the fluorescence of AGEs at a wavelength of 350/440 nm. The samples were diluted in 0.02 MPBS (pH 7.4; 1:5, v/v) before analysis.20
The concentration of AOPP was determined in a colorimetric assay by measuring the oxidation of iodide ions at a wavelength of 340 nm. The samples were diluted in 0.02 MPBS (pH 7.4; 1:5, v/v) before analysis.20
Malondialdehyde was quantified in the thiobarbituric acid-reactive-substances (TBARS) assay by reacting MDA with thiobarbituric acid (TBA) in the presence of 1,1,3,3-tetraethoxypropane and measuring the amount of produced MDA at a wavelength of 535 nm.21
The concentration of 4-HNE was determined in the ELISA assay with the use of commercial ELISA kits (Cell Biolabs, Inc., San Diego, CA, USA; Cayman Chemical, Ann Arbor, MI, USA; EIAab, Wuhan, China) according to the manufacturers’ instructions.
Statistical Analyses
Statistical analyses were conducted with the use of GraphPad Prism 9.0 software (GraphPad Software, La Jolla, USA). The Shapiro–Wilk test was used to determine the normality of distribution. The Student’s t-test was applied to test data with a normal distribution, and the Mann–Whitney test was used to analyze data that did not follow a normal distribution. The results were presented as the median (minimum-maximum) at a significance level of p<0.05. The number of subjects was determined based on our previous experiment, assuming that the power of the test = 0.9 and α = 0.05. ClinCalc online calculator was used to estimate the sample size.
Graphics tool license
The figure nr 4 was created using BioRender (number of license: XI26JB4EYF).
Results
Characteristics of COVID-19 Patients
In the group of 218 patients who tested positive for COVID-19 in a PCR assay involving nasopharyngeal swabs (115 men and 103 women), 194 patients were hospitalized for less than 10 days, 13 patients were hospitalized for 10–20 days, and 6 patients were hospitalized for more than 20 days. The presence of comorbidities was determined in 107 patients, including hypertension in 48 patients, coronary heart disease in 29 patients, and diabetes in 24 patients. Based on their MEWS scores, COVID-19 patients were divided into four severity groups (Table 1): MEWS 1–106 patients, MEWS 2–70 patients, MEWS 3–28 patients, and MEWS 4–14 patients. Detailed patient characteristics are presented in Tables 2 and 3.
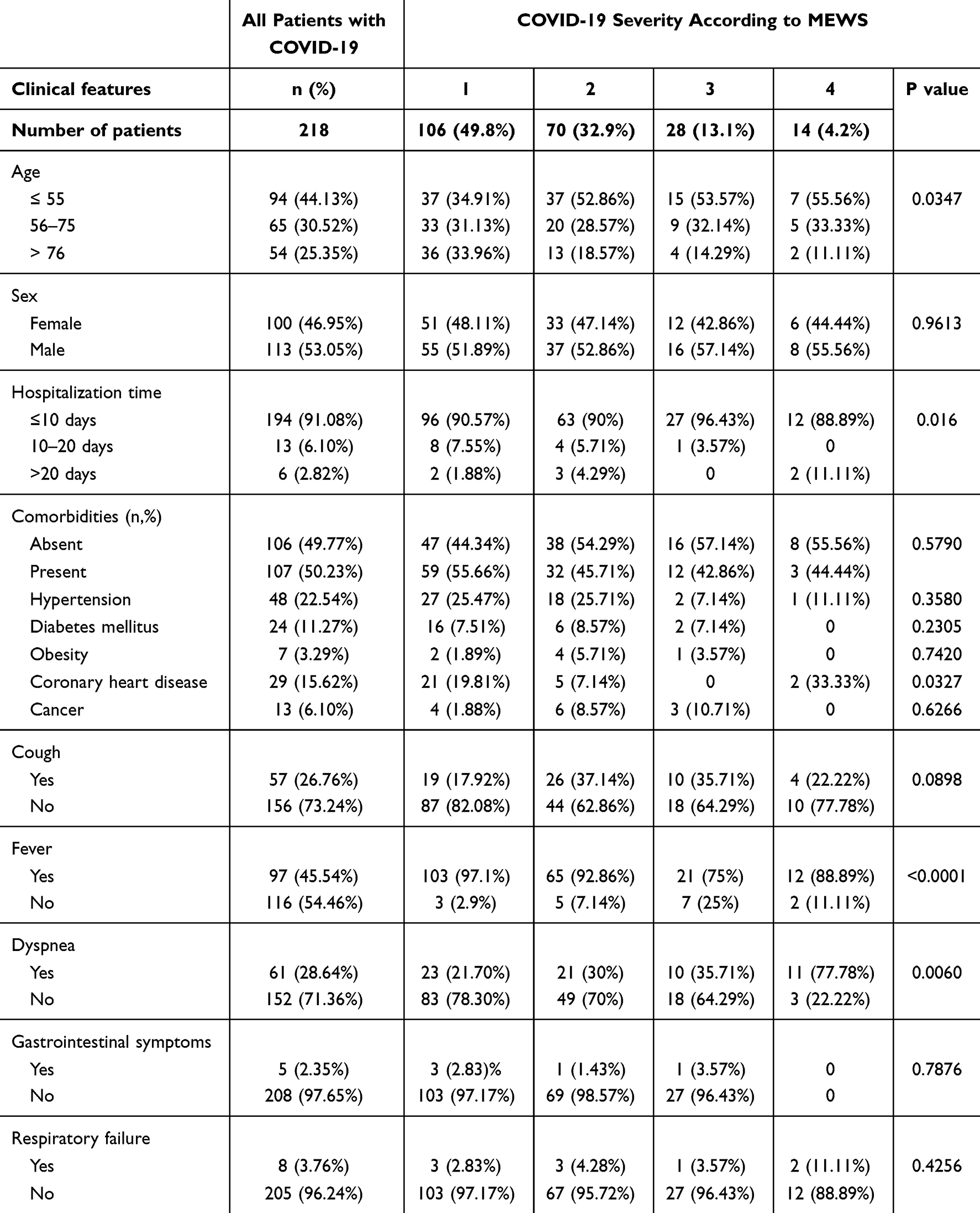 |
Table 2 Characteristics of COVID-19 Patients |
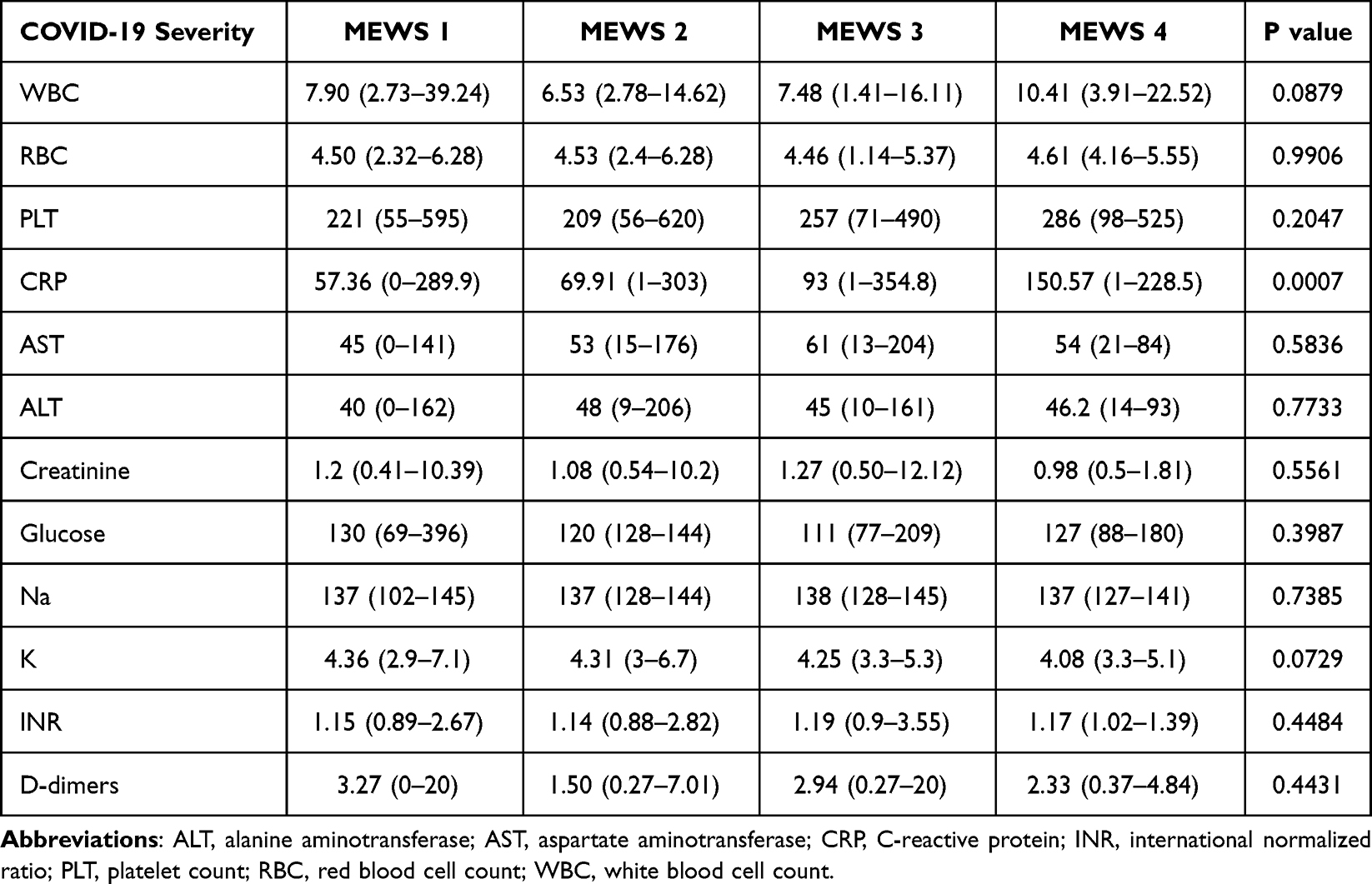 |
Table 3 Comparison of Selected Blood Test Results in COVID-19 Patients with Different MEWS Scores |
A Comparison of the Activity of Enzymatic and Non-Enzymatic Antioxidants in COVID-19 Patients, Convalescents, and Healthy Controls, Including in Reference to the Severity of COVID-19
The activity of SOD (p=0.0156) and GR (p<0.0001) was significantly higher in COVID-19 patients than in the control group. In addition, CAT, GPx and GR activity and GSH concentration were significantly higher in COVID-19 patients than in convalescents (p=0.0280 for CAT, p=0.0027 for GPx, p<0.0001 for GR, and p=0.0431 for GSH) (Table 4, Figure 1). In the group of the analyzed antioxidants, only SOD and GPx activity decreased with an increase in COVID-19 severity assessed on the MEWS scale, but the noted differences were not significant (Table 5).
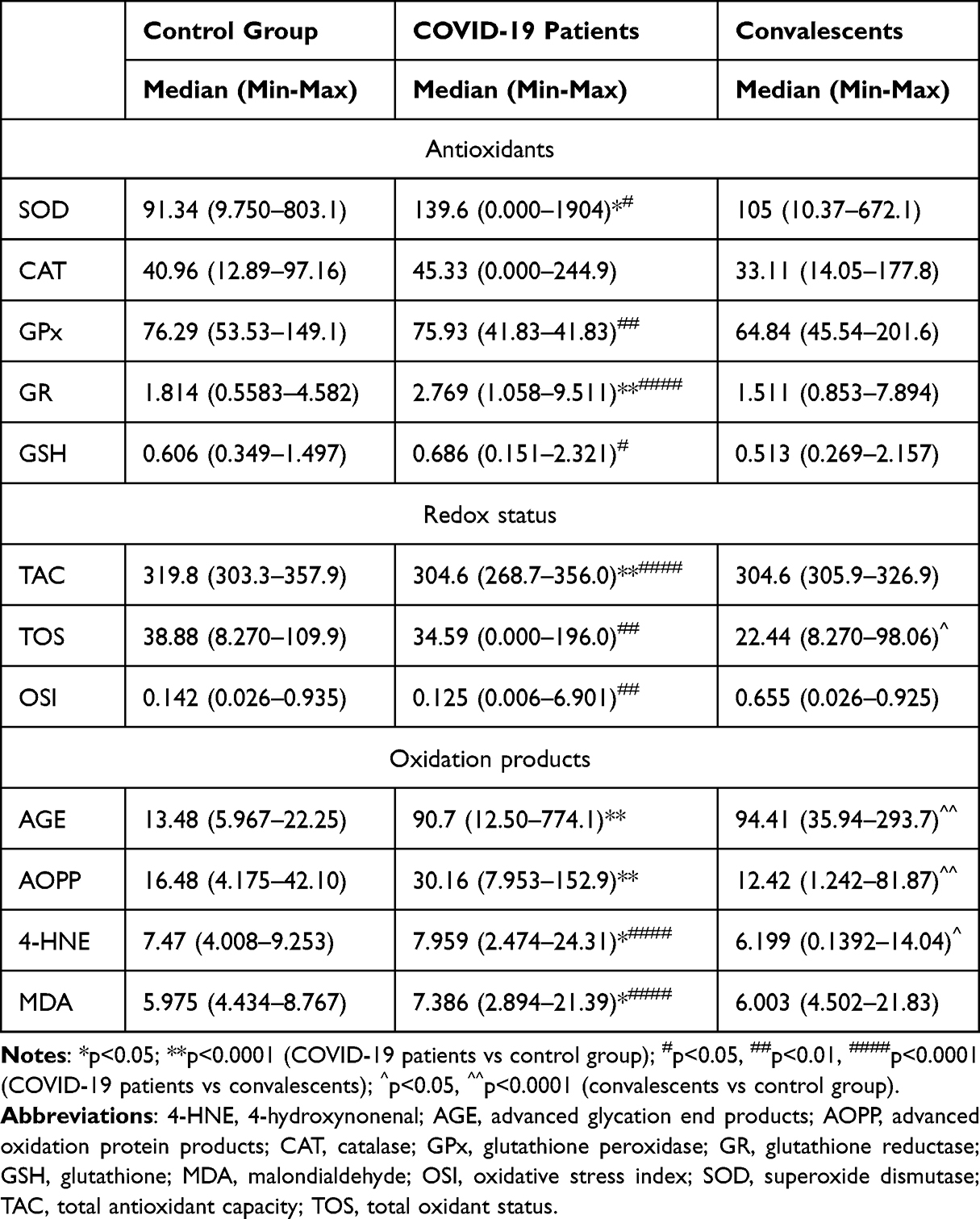 |
Table 4 Comparison of Oxidative Stress Parameters in COVID-19 Patients, Convalescents, and the Control Group |
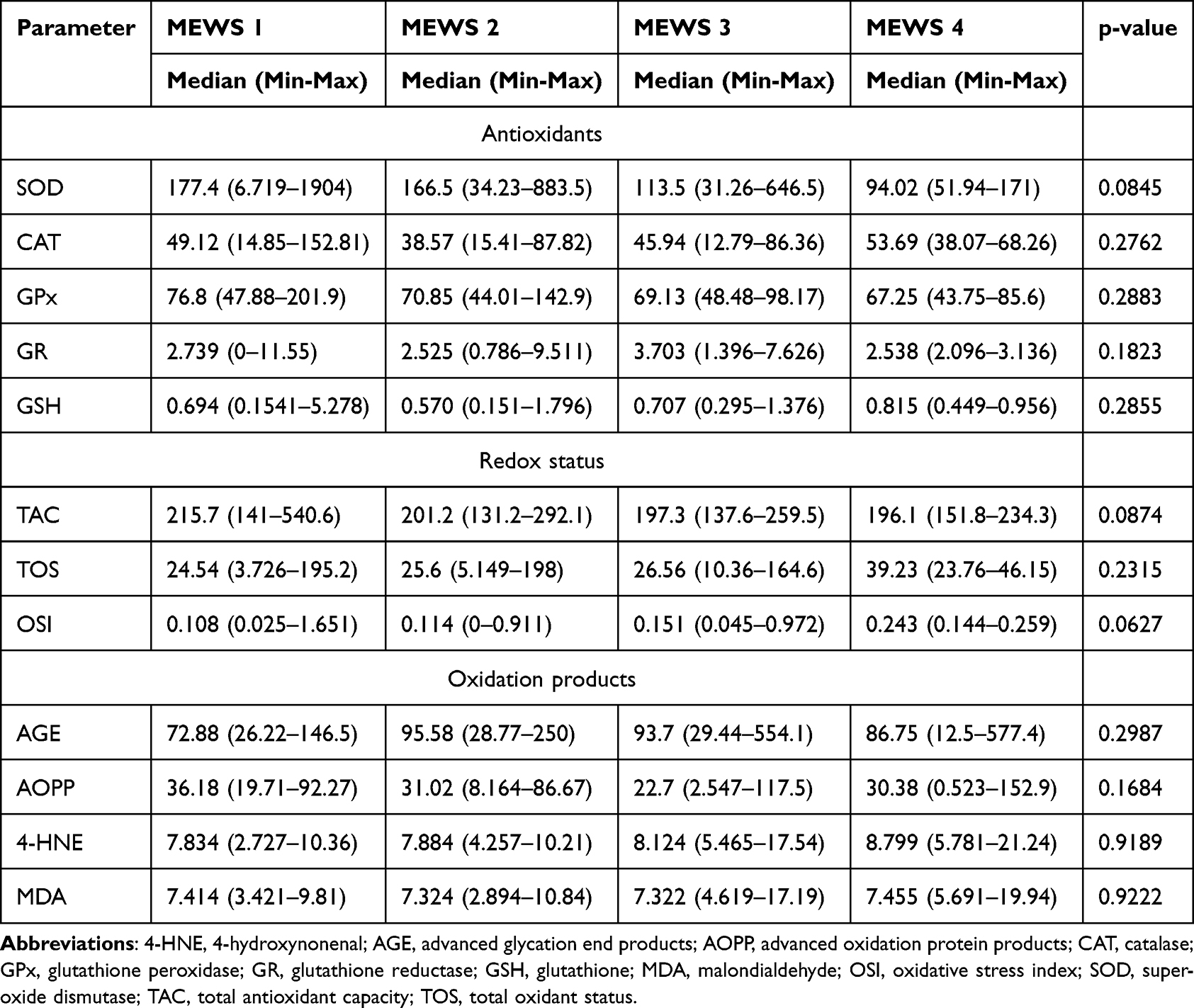 |
Table 5 Oxidative Stress Parameters in COVID-19 Patients Relative to the Severity of Disease Symptoms |
 |
Figure 1 Comparison of the activity of enzymatic (A–D) and non-enzymatic (E) antioxidants in COVID-19 patients, convalescents, and the control group. Abbreviations: CAT, catalase; GPx, glutathione peroxidase; GR, glutathione reductase; GSH, glutathione; SOD, superoxide dismutase. |
Redox Status of Patients Infected with the SARS-CoV-2, Convalescents and the Control Group, Including in Reference to the Severity of COVID-19
The participants’ redox status was determined by measuring TAC and TOS, and calculating the OSI as the TOS/TAC ratio. Plasma TAC was significantly lower in COVID-19 patients than in the control group (p<0.0001) and convalescents (p<0.0001). COVID-19 patients were characterized by significantly higher plasma TOS than convalescents (p < 0.0021), whereas convalescents were characterized by lower plasma TOS than healthy controls (p=0.0450). The values of OSI were significantly lower in COVID-19 patients than in convalescents (p < 0.0080) (Table 4, Figure 2). Total antioxidant capacity decreased and OSI increased with an increase in the severity of COVID-19 symptoms, but the observed differences were not significant (Table 5).
 |
Figure 2 Redox status: TAC (A), TOS (B), OSI (C) of COVID-19 patients, convalescents, and the control group. Abbreviations: OSI, oxidative stress index; TAC, total antioxidant capacity; TOS, total oxidative status. |
A Comparison of the Concentrations of Products of Protein and Lipid Oxidative Damage in Patients Infected with the SARS-CoV-2, Convalescents, and the Control Group, Including in Reference to the Severity of COVID-19
An analysis of the concentrations of products of protein and lipid oxidation revealed that all of the examined biomarkers were significantly higher in COVID-19 patients than in the control group (p<0.0001 for AGEs, p<0.0001 for AOPP, p=0.0405 for 4-HNE, p=0.0233 for MDA), and that 4-HNE (p<0.0001) and MDA (p<0.0001) levels were significantly higher in COVID-19 patients than in convalescents. In turn, the serum levels of AGEs (p<0.0001), AOPP (p<0.0001), and 4-HNE (0=0.0165) were significantly higher in convalescents than in the control group (Table 4, Figure 3). These biomarkers were not significantly correlated with the severity of COVID-19, and 4-HNE was the only parameter that increased with a rise in the MEWS score (Table 5).
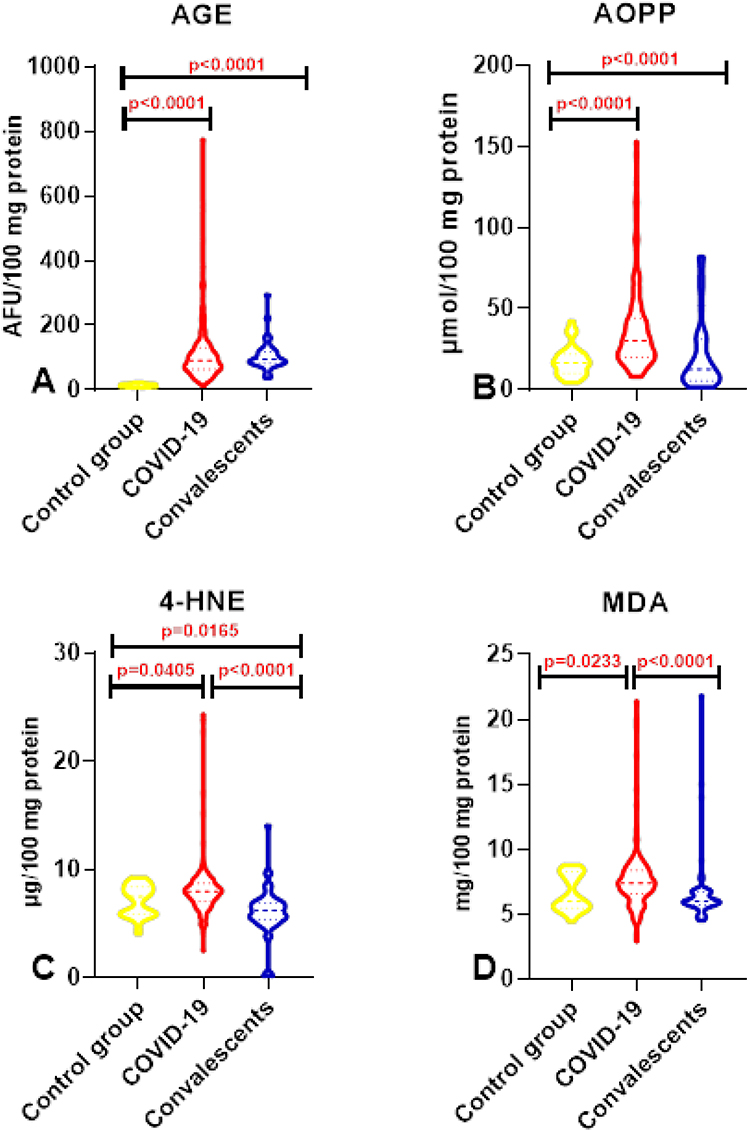 |
Figure 3 A comparison of the concentrations of products of protein (A and B) and lipid (C and D) oxidative damage in patients infected with the SARS-CoV-2 virus, convalescents, and the control group. Abbreviations: 4-HNE, 4-hydroxynonenal; AGE, advanced glycation end products; AOPP, advanced oxidation protein products; MDA, malondialdehyde. |
ROC Analysis
The diagnostic efficacy of oxidative stress biomarkers during an infection caused by the SARS-CoV-2 was evaluated in a ROC analysis. The study demonstrated that oxidative stress biomarkers can be useful for differentiating COVID-19 patients from healthy controls (AUC for SOD=0.6597, for GR=0.8239, for TAC=0.8165, for AGE=0.9971, for AOPP=0.8043, for 4-HNE=0.6327, for MDA=0.6423) (Table 6A, Figure 4) and COVID-19 patients vs convalescents (AUC for GR=0.8365, for AOPP=0.7587, for TAC=0.7775, for TOS=0.7921, for 4-HNE=0.8071, for MDA=0.7407) (Table 6B, Figure 5). In addition, OSI, AGEs, and 4-HNE were also useful diagnostic parameters for differentiating between convalescents and the control group (AUC for OSI=0.7355, for AGE=1.000, for 4-HNE=0.6840) (Table 6C, Figure 6).
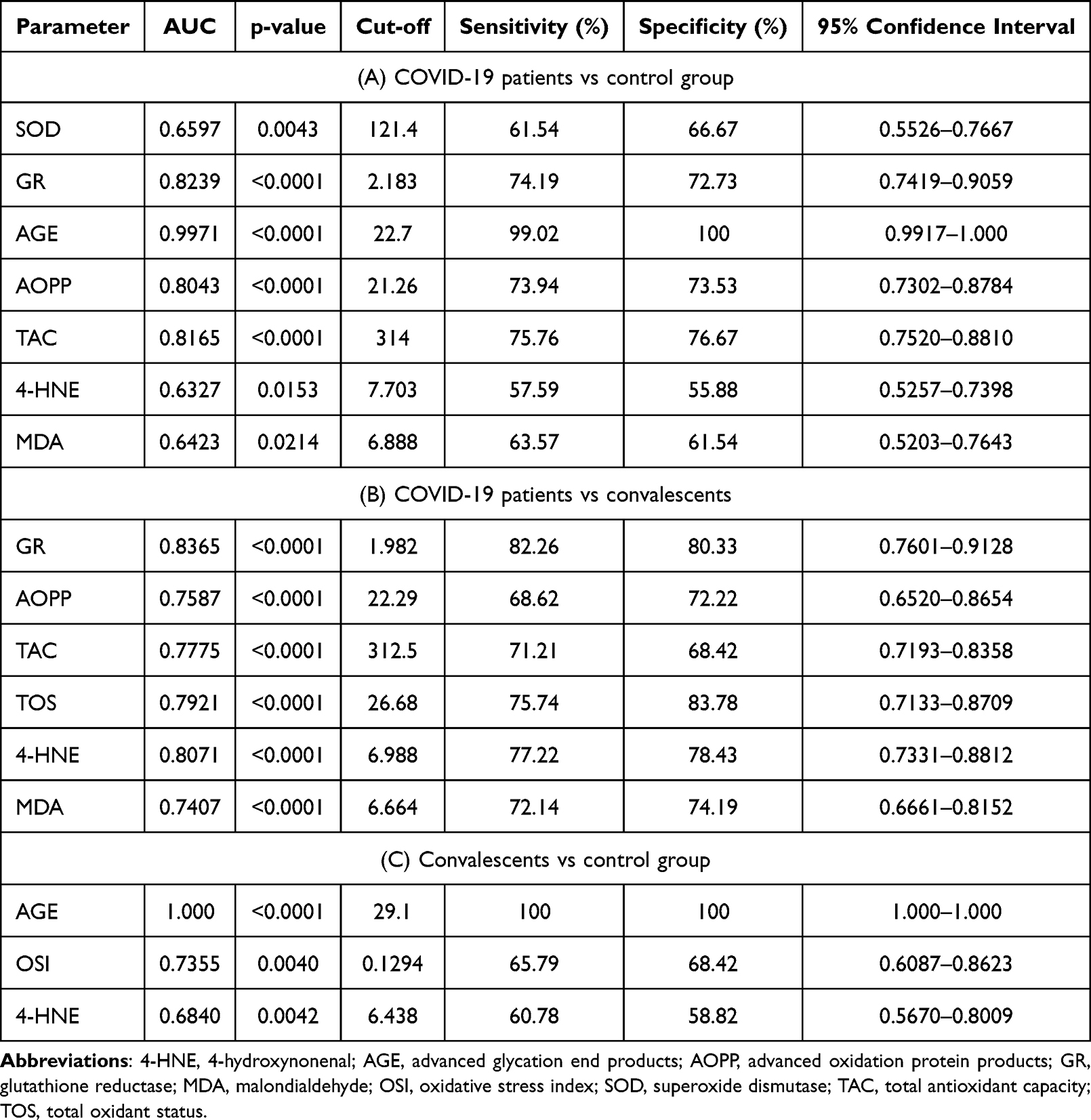 |
Table 6 Area Under the Curve (AUC) Values of Oxidative Stress Biomarkers That Were Used to Differentiate Between COVID-19 Patients and the Control Group (A), Between COVID-19 Patients and Convalescents (B), and Between Convalescents and the Control Group (C) |
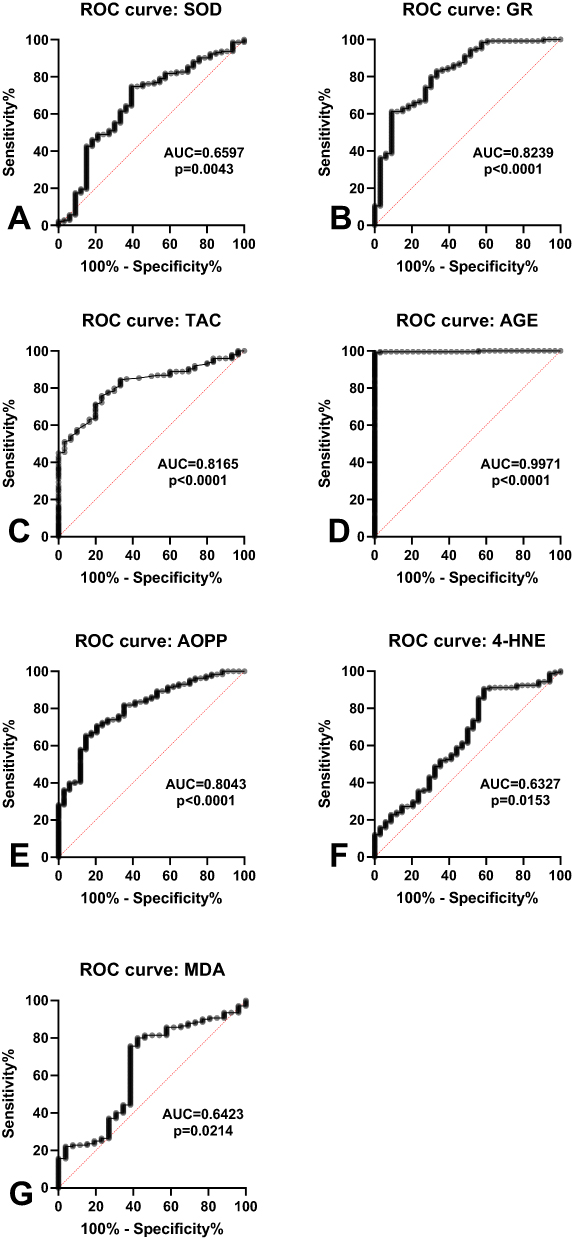 |
Figure 4 Receiver operating characteristic (ROC) curves of antioxidants (A and B), redox balance (C) products of protein (D and E) and lipid (F and G) oxidative damage for differentiating between COVID-19 patients and the control group. |
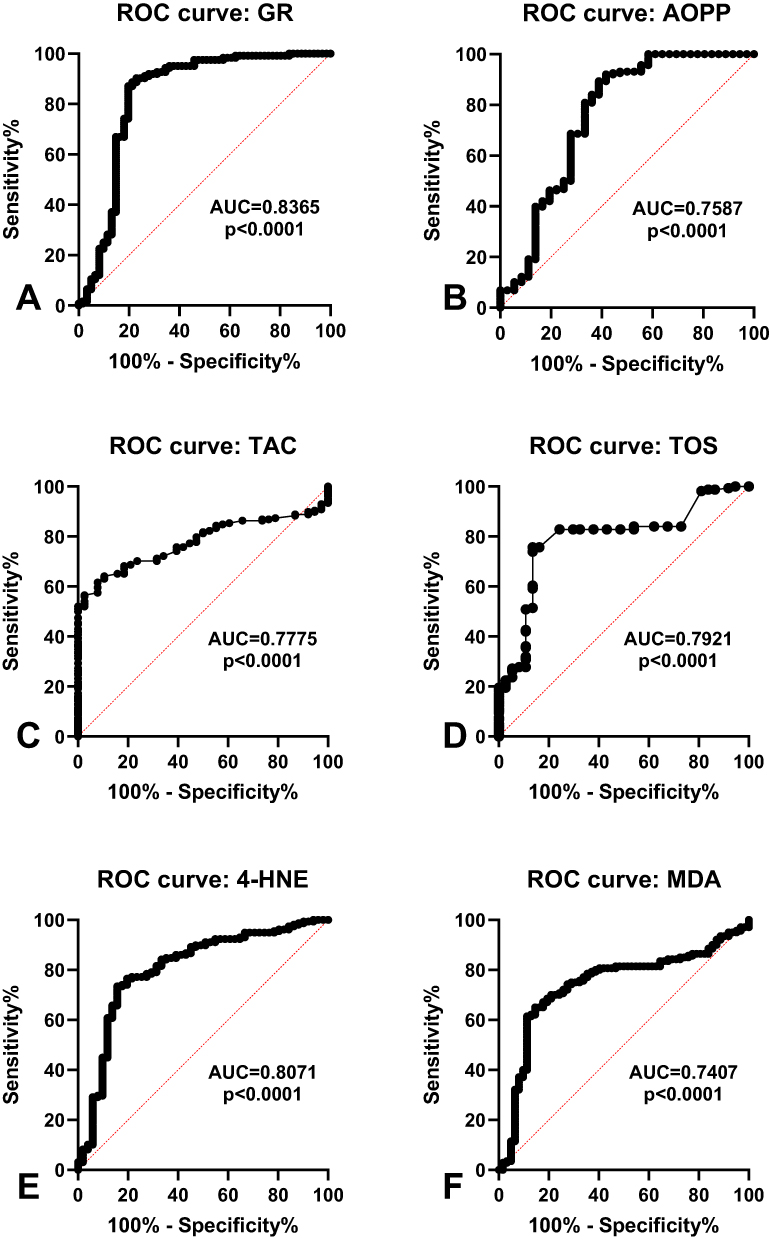 |
Figure 5 Receiver operating characteristic (ROC) curves of antioxidants (A), products of protein oxidative damage (B), redox balance (C and D) products of lipid oxidative damage (E and F) for differentiating between COVID-19 patients and the convalescents. |
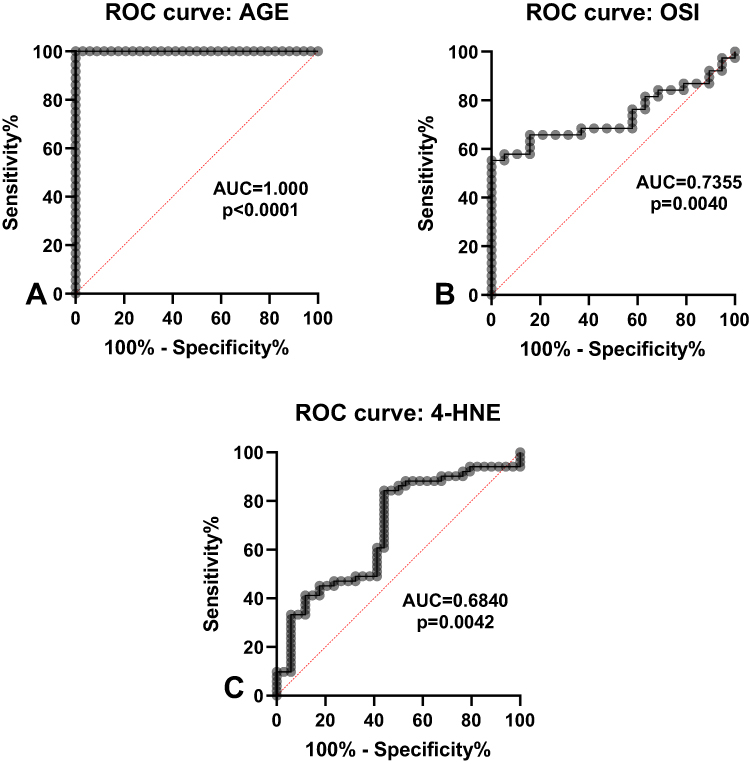 |
Figure 6 Receiver operating characteristic (ROC) curves of products of protein oxidative damage (A), redox balance (B) products of lipid oxidative damage (C) for differentiating between convalescents and the control group. |
Discussion
This is the first study to evaluate the diagnostic applicability of oxidative stress biomarkers during an infection caused by the SARS-CoV-2 (COVID-19 patients) and after COVID-19 (convalescents). COVID-19 can lead to numerous complications, which is why an assessment of redox parameters in the control group and in infected patients can improve diagnosis and predictions of the long-term consequences of COVID-19. An increase in the activity of both enzymatic and non-enzymatic antioxidants, an increase in the values of redox status parameters, as well as an increase in the levels of protein and lipid oxidation products was observed in the blood of COVID-19 patients relative to the control group and convalescents, and in the blood of convalescents relative to the control group (Figure 4). In addition, some markers (SOD, GPx, TAC) decreased, whereas others (OSI, 4-HNE) increased with an increase in COVID-19 severity assessed on the MEWS score.
A redox imbalance in infections caused by the SARS-CoV-2 leads to oxidative stress.22–24 The antioxidant system, including enzymatic (CAT, SOD, GPx, GR)25–27 and non-enzymatic (GSH) antioxidants,28,29 plays a key role in defending the body against excessive ROS production. In the present study, the activity of enzymatic antioxidants SOD and GR was significantly higher in COVID-19 patients than in the control group, and the activity CAT, GPx, and GR and GSH concentration were also higher in COVID-19 patients than in convalescents. These results indicate that the production of these antioxidants is enhanced in response to ROS overproduction during COVID-19.27 However, most of the COVID-19 patients analyzed in the study (82%) had mild and moderate symptoms of the disease. In other reports, a decrease in SOD and GR activity30 and a decrease in GSH concentration were observed in patients with severe COVID-19.31 The present study also demonstrated that the activity of antioxidant enzymes (SOD and GPx) decreased with an increase in disease severity assessed on the MEWS score, which indicates that these enzymes become depleted as a result of prolonged and intensified oxidative stress during an infection with the SARS-CoV-2. The observed decrease in CAT, GPx, GR, and GSH values in convalescents relative to COVID-19 patients indicates that the disease leads to the overstimulation of the antioxidant system and, consequently, a depletion of the antioxidant barrier. The study also revealed that GR is the most useful diagnostic marker (of all analyzed antioxidants) for differentiating COVID-19 patients from healthy subjects (AUC=0.8239) and convalescents (AUC=0.8365). Glutathione reductase is a flavoprotein that maintains the supply of reduced glutathione (GSH)32 during the detoxification of peroxides and free radicals in the mitochondria, which indicates that this enzyme is an important element of the antioxidant defense system that maintains the redox potential of cells.33,34 The response of the antioxidant defense system to ROS overproduction during COVID-19 can be attributed to the function of the main transcription factors, nuclear factor kappa B (NF-κB)35 and nuclear factor erythroid-2-related factor 2 (Nrf2), which are the antioxidant response elements (ARE) of the redox signaling pathway.36 The infection caused by the SARS-CoV-2 intensifies oxidative stress induced by ROS overproduction and, and it also inhibits the translocation of Nrf2 into the nucleus and enhances the activation of NF-κB, which leads to an acute inflammatory response and oxidative damage.37,38 Nrf2 plays a key role in modulating the GSH redox state by regulating GR transcription and protecting cells against oxidative stress.39,40
In the current study, the overall redox potential was evaluated by measuring antioxidant capacity/oxidative stress biomarkers (TAC, TOS, OSI). Total antioxidant capacity was lower in COVID-19 patients than in healthy controls and convalescents (p<0.001). This parameter can be used as a potential diagnostic biomarker for differentiating COVID-19 patients from healthy controls (AUC=0.8165) and convalescents (AUC=0.7775). Total antioxidant capacity denotes the overall content of enzymatic and non-enzymatic antioxidants, and it can be used to assess the body’s antioxidant capacity during diseases and infections, including an infection caused by the SARS-CoV-2.41 Total oxidative status represents the total content of oxidants in the body, and TOS and TAC are used to calculate the OSI (TOS/TAC ratio) which provides information about the ratio of pro-oxidants and antioxidants.42 Total oxidative status was significantly higher in COVID-19 patients than in convalescents (p=0.0021), and this parameter can be used as a potential diagnostic marker to discriminate between these groups of patients (AUC=0.7921). The diagnostic utility of TOS and TAC in infections caused by the SARS-CoV-2 was also recognized by other researchers. Çakırcą et al43 found that TAC and TOS were useful parameters for discriminating between COVID-19 patients who required and did not require treatment in an intensive care unit. In the present study, TOS and TAS measurements revealed a decrease in antioxidant levels in COVID-19 patients assessed on the MEWS score, which indicates that the antioxidant barrier is weakened with an increase in disease severity.
Reactive oxygen species are overproduced during COVID-19, which intensifies oxidative stress.44 Impaired antioxidant defense and ROS overproduction contribute to the oxidation of proteins and DNA and lipid peroxidation, which leads to the loss of their biological activity,45 accelerates aging processes,46 and increases the risk of neurodegenerative diseases,47 diabetes,45 atherosclerosis,48 and carcinogenesis.49 Therefore, ROS levels should be assessed in convalescents to determine the potential risk of these diseases.
In biological systems, ROS act directly on proteins and lead to the oxidation of amino acid side chains, chain fragmentation, and disruptions in the secondary and tertiary structure of proteins.50 In the present study, AGE and AOPP concentrations were significantly higher in both COVID-19 patients and convalescents than in the control group (p<0.0001). In addition, AGEs were a highly useful diagnostic parameter for differentiating COVID-19 patients from healthy controls (AUC=0.9971) and convalescents from healthy controls (AUC=1.000). In the group of the analyzed biomarkers, AGEs were also characterized by the highest sensitivity and specificity (>99%) in discriminating between the study groups. AGEs bind to the soluble receptor for advanced glycation end-products (sRAGE) that is found on the surface of endothelial cells, smooth muscle cells, monocytes/macrophages, T cells, podocytes in renal glomeruli, cardiomyocytes, dendritic cells, neurons in the central and peripheral nervous systems, and transforming cells, and they trigger intracellular production of ROS and the activation of transcription factors.51 The above leads to the activation of the pro-inflammatory NF-κB and signaling pathways, including MAP-kinase, JAK, and p21RAS pathways.52,53 The production of many cytokines and growth factors is also intensified.2 The activation of aldose reductase accelerates the formation of AGEs and intensifies carbonyl stress.54 The expression of intracellular adhesion molecules (ICAM) and vascular cell adhesion molecules (VCAM) is also intensified.55,56 According to many researchers, sRAGE is a useful biomarker for predicting damage to pulmonary alveoli in COVID-19 patients with pneumonia that is not associated with ARDS.57 In COVID-19 patients with pneumonia, high initial plasma levels of sRAGE have been found to be linked with disease severity, antigen levels, and short- and long-term outcomes.58 The present study demonstrated that AOPP can be regarded as a potential diagnostic biomarker for differentiating COVID-19 patients from healthy subjects (AUC=0.8043) and convalescents (AUC=0.7583). Advanced oxidation protein products contain tyrosine and are modified mainly through the oxidation of albumins, fibrinogen, and lipoproteins.59 Changes in AOPP levels may provide information about disease severity, including monocyte and neutrophil activation during an infection caused by the SARS-CoV-2.60 During lung injury, the accumulation of AOPP can prevent the removal of edema fluid, which contributes to the progression of disease, including COVID-19.61 It should also be noted that AOPP activate neutrophils, monocytes, and T cells, regulate dendritic cells, activate the NF-κB signaling pathway, promote the secretion of proinflammatory cytokines, and increase the production of free radicals.62
An analysis of the concentrations of lipid peroxidation products revealed that MDA and 4-HNE levels were significantly higher in COVID-19 patients than in the control group (MDA p=0.0233; 4-HNE p=0.0405) and convalescents (MDA p<0.0001; 4-HNE p<0.0001). 4-HNE (AUC=0.8071) and MDA (AUC=0.7407) were most useful for discriminating between COVID-19 patients and convalescents. Elevated levels of lipid peroxidation products in patients infected with the SARS-CoV-2 were also reported in other studies.6,63,64 Some researchers found correlations between the concentrations of lipid peroxidation products and disease severity,65 and between 4-HNE levels and the risk of mortality in COVID-19 patients.6 The peroxidation of lipids, mainly unsaturated fatty acids, leads to the production of peroxides and, in subsequent reactions, aldehydes such as MDA and HNE66,67 which were analyzed in this study. Lipid peroxidation products are potentially mutagenic and carcinogenic.68 4-HNE is highly toxic,69 whereas MDA is the most mutagenic compound.70 Malondialdehyde is also a marker of ferroptosis, an iron-dependent form of cell death.71 Lipid peroxidation products increase the risk of numerous diseases, including cardiovascular diseases,72 cancer,73 Alzheimer’s disease,74 and chronic diseases such as non-alcoholic fatty liver disease (NAFLD),75 chronic obstructive pulmonary disease (COPD),76 and diabetes.77 In the current study, the concentrations of protein and lipid peroxidation products were lower in convalescents than in COVID-19 patients, which suggests that oxidative stress is reduced after infection, thus decreasing the risk of long-term complications.
The pathogenesis of the infection caused by the SARS-CoV-2 has not been fully elucidated to date,78,79 but studies confirmed that the pathogenesis and severity of COVID-19 are closely linked with the overproduction of ROS and the depletion of the antioxidant barrier, and these processes promote oxidation and contribute to protein and lipid damage.80 Similar observations were made in this study which demonstrated that TAC was lower and TOS was higher in COVID-19 patients, and that antioxidant levels (SOD, GPx) decreased with an increase in disease severity. COVID-19 patients were also characterized by higher concentrations of protein oxidation products (AOPP, AGEs) and lipid peroxidation products (4-HNE, MDA). Redox parameters were lower in convalescents than in COVID-19 patients, which indicates that biomarker levels decrease after the infection, but remain higher than in persons without a history of COVID-19, which may significantly affect short- and long-term complications after infection. In the present study, these parameters did not increase with an increase in COVID-19 severity evaluated on the MEWS score, but this result could be attributed to differences in the size of the studied population groups. The study demonstrated that AGEs supported the differentiation of COVID-19 patients from healthy subjects and convalescents with the highest sensitivity and specificity (>99%). The results of the study pave the way for further research into the diagnostic utility of redox biomarkers in larger populations of patients infected with the SARS-CoV-2 and convalescents. Studies conducted on larger populations of similar sizes can provide valuable insights about redox parameters that are particularly useful for identifying COVID-19 patients with different disease severity. It should be noted that redox biomarkers show high diagnostic utility in many diseases, for example in cardiovascular disease81 and neurodegenerative diseases,82 but they are not yet routinely used in diagnosis and treatment.
The study had certain limitations. COVID-19 patients were divided into groups based on their MEWS scores, and the resulting groups were unequal in size. In the future, a similar study should be conducted on COVID-19 patients with a wider range of MEWS scores. In addition, the redox parameters evaluated in this study are not specific to COVID-19 only; therefore, they are more useful for monitoring disease progression than for diagnosing an infection. The strength of this study was that redox parameters in COVID-19 patients were compared not only with the control group, but also with convalescents who did not have any comorbidities. The enzymatic and non-enzymatic antioxidant barrier was evaluated, and the redox balance and protein and lipid oxidation products were also analyzed to describe systemic oxidative stress in COVID-19 patients and convalescents. The present findings can be used in clinical trials to evaluate the diagnostic efficacy of redox biomarkers in larger populations of patients infected with the SARS-CoV-2 and convalescents.
Conclusions
An infection with the SARS-CoV-2 disrupts the redox balance and increases protein oxidation and lipid peroxidation. AGEs fulfill the criteria for a potential diagnostic biomarker in COVID-19 patients and convalescents.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of the Medical University of Białystok (decision No. APK.002.26.2021 of 28 January 2021). All participants gave their written consent to participate in the study for studies involving humans and were informed about the purpose of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by grants from the Medical University of Bialystok, Poland (grant numbers: SUB/1/DN/22/001/2209; SUB/1/DN/22/005/2209).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Dymicka-Piekarska V, Dorf J, Milewska A, et al. Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – risk of death inflammatory biomarkers in patients with COVID-19. J Inflamm Res. 2023;16:2209–2222. doi:10.2147/jir.s409871
2. Pum A, Ennemoser M, Adage T, Kungl AJ. Cytokines and chemokines in SARS-CoV-2 infections—therapeutic strategies targeting cytokine storm. Biomolecules. 2021;11(1):91. doi:10.3390/biom11010091
3. Ramezani M, Nemati H, Najafi F, Sayad B, Sadeghi M. A systematic review and meta-analysis on blood levels of cytokines/chemokines in COVID-19 cases. Gulhane Med J. 2022;64(3):208–216. doi:10.4274/gulhane.galenos.2021.25733
4. Hanson QM, Wilson KM, Shen M, et al. Targeting ACE2-RBD interaction as a platform for COVID-19 therapeutics: development and drug-repurposing screen of an AlphaLISA proximity assay. ACS Pharmacol Transl Sci. 2020;3(6):1352–1360. doi:10.1021/ACSPTSCI.0C00161/SUPPL_FILE/PT0C00161_SI_002.XLSX
5. Silvagno F, Vernone A, Pescarmona GP. The role of glutathione in protecting against the severe inflammatory response triggered by covid-19. Antioxidants. 2020;9(7):624. doi:10.3390/antiox9070624
6. Žarković N, Jastrząb A, Jarocka-Karpowicz I, et al. The impact of severe COVID-19 on plasma antioxidants. Molecules. 2022;27(16):5323. doi:10.3390/molecules27165323
7. Kosidło JW, Wolszczak-Biedrzycka B, Dymicka-Piekarska V, Dorf J, Matowicka-Karna J. Clinical significance and diagnostic utility of NLR, LMR, PLR and SII in the course of COVID-19: a literature review. J Inflamm Res. 2023;16:539–562. doi:10.2147/JIR.S395331
8. Wolszczak-Biedrzycka B, Dorf J, Milewska A, et al. The diagnostic value of inflammatory markers (CRP, IL6, CRP/IL6, CRP/L, LCR) for assessing the severity of COVID-19 symptoms based on the MEWS and predicting the risk of mortality. J Inflamm Res. 2023;16:2173–2188. doi:10.2147/jir.s406658
9. Raveendran AV, Jayadevan R, Sashidharan S. Long COVID: an overview. Diabetes Metabolic Syndr. 2021;15(3):869–875. doi:10.1016/j.dsx.2021.04.007
10. Flisiak R, Parczewski M, Horban A, et al. Management of SARS-CoV-2 infection: recommendations of the Polish association of epidemiologists and infectiologists. Annex no. 2 as of October 13, 2020. Pol Arch Intern Med. 2020;130(10):915–918. doi:10.20452/PAMW.15658
11. District Sanitary and Epidemiological Station in Wałbrzych Zaświadczenia o statusie ozdrowieńca [Certificates of recovery status] Available from: https://www.gov.pl/web/psse-walbrzych/zaswiadczenia-o-statusie-ozdrowienca.
12. Misra HP, Fridovich I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J Biol Chem. 1972;247(10):3170–3175. doi:10.1016/s0021-9258(19)45228-9
13. Enzymology HAM. Catalase in vitro. Elsevier; 1984. Available from: https://www.sciencedirect.com/science/article/pii/S0076687984050163.
14. Paglia DE, Valentine WN. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J Lab Clin Med. 1967;70(1):158–169.
15. Mize CE, Langdon RG. Hepatic glutathione reductase. I. Purification and general kinetic properties. J Biol Chem. 1962;237(5):1589–1595. doi:10.1016/S0021-9258(19)83745-6
16. Griffith OW. Determination of glutathione and glutathione disulfide using glutathione reductase and 2-vinylpyridine. Anal Biochem. 1980;106(1):207–212. doi:10.1016/0003-2697(80)90139-6
17. Erel O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin Biochem. 2004;37(4):277–285. doi:10.1016/j.clinbiochem.2003.11.015
18. Erel O. A new automated colorimetric method for measuring total oxidant status. Clin Biochem. 2005;38(12):1103–1111. doi:10.1016/j.clinbiochem.2005.08.008
19. Knaś M, Maciejczyk M, Daniszewska I, et al. Oxidative damage to the salivary glands of rats with streptozotocin-induced diabetes-temporal study: oxidative stress and diabetic salivary glands. J Diabetes Res. 2016;2016:1–13. doi:10.1155/2016/4583742
20. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/12511184/.
21. Buege JA, Aust SD. Microsomal lipid peroxidation. Methods Enzymol. 1978;52. doi:10.1016/S0076-6879(78)52032-6
22. Mingoti MED, Bertollo AG, Simões JLB, Francisco GR, Bagatini MD, Ignácio ZM. COVID-19, oxidative stress, and neuroinflammation in the depression route. J Mol Neurosci. 2022;72(6):1166–1181. doi:10.1007/s12031-022-02004-y
23. Vollbracht C, Kraft K. Oxidative stress and hyper-inflammation as major drivers of severe COVID-19 and Long COVID: implications for the benefit of high-dose intravenous vitamin C. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.899198
24. Schönrich G, Raftery MJ, Samstag Y. Devilishly radical NETwork in COVID-19: oxidative stress, neutrophil extracellular traps (NETs), and T cell suppression. Adv Biol Regul. 2020;77. doi:10.1016/j.jbior.2020.100741
25. Trujillo-Mayol I, Guerra-Valle M, Casas-Forero N, et al. Western dietary pattern antioxidant intakes and oxidative stress: importance during the SARS-CoV-2/COVID-19 pandemic. Adv Nutr. 2021;12(3):670–681. doi:10.1093/advances/nmaa171
26. Yaghoubi N, Youssefi M, Jabbari Azad F, Farzad F, Yavari Z, Zahedi Avval F. Total antioxidant capacity as a marker of severity of COVID-19 infection: possible prognostic and therapeutic clinical application. J Med Virol. 2022;94(4):1558–1565. doi:10.1002/jmv.27500
27. Mehri F, Rahbar AH, Ghane ET, Souri B, Esfahani M. Changes in oxidative markers in COVID-19 patients. Arch Med Res. 2021;52(8):843–849. doi:10.1016/j.arcmed.2021.06.004
28. Kumar P, Osahon O, Vides DB, Hanania N, Minard CG, Sekhar RV. Severe glutathione deficiency, oxidative stress and oxidant damage in adults hospitalized with covid-19: implications for glynac (glycine and n-acetylcysteine) supplementation. Antioxidants. 2022;11(1). doi:10.3390/antiox11010050
29. Glassman I, Le N, Mirhosseini M, et al. The role of glutathione in prevention of COVID-19 immunothrombosis: a review. Front Biosci. 2023;28(3):59. doi:10.31083/j.fbl2803059
30. Dikshit N, Kant S, Verma AK, Ansari KM. Study to estimate levels of oxidative stress biomarkers in long COVID patients. Lung India. 2022;39(Suppl 1):S137–S138.
31. Labarrere CA, Kassab GS. Glutathione deficiency in the pathogenesis of SARS-CoV-2 infection and its effects upon the host immune response in severe COVID-19 disease. Front Microbiol. 2022;13. doi:10.3389/fmicb.2022.979719
32. Moron MS, Depierre JW, Mannervik B. Levels of glutathione, glutathione reductase and glutathione S-transferase activities in rat lung and liver. BBA General Subjects. 1979;582(1). doi:10.1016/0304-4165(79)90289-7
33. Zhu Z, Du S, Du Y, Ren J, Ying G, Yan Z. Glutathione reductase mediates drug resistance in glioblastoma cells by regulating redox homeostasis. J Neurochem. 2018;144(1):93–104. doi:10.1111/jnc.14250
34. Couto N, Wood J, Barber J. The role of glutathione reductase and related enzymes on cellular redox homoeostasis network. Free Radic Biol Med. 2016;95:27–42. doi:10.1016/j.freeradbiomed.2016.02.028
35. Amini-Farsani Z, Yadollahi-Farsani M, Arab S, Forouzanfar F, Yadollahi M, Asgharzade S. Prediction and analysis of microRNAs involved in COVID-19 inflammatory processes associated with the NF-kB and JAK/STAT signaling pathways. Int Immunopharmacol. 2021;100:108071. doi:10.1016/j.intimp.2021.108071
36. Lee J, Kwon KH. Development of customized inner beauty products and customized cosmetics apps according to the use of NRF2 through DTC genetic testing after the COVID-19 pandemic. J Cosmet Dermatol. 2022;21(6):2288–2297. doi:10.1111/jocd.14467
37. Carcaterra M, Caruso C. Alveolar epithelial cell type II as main target of SARS-CoV-2 virus and COVID-19 development via NF-Kb pathway deregulation: a physio-pathological theory. Med Hypotheses. 2021;146:110412. doi:10.1016/j.mehy.2020.110412
38. Banchini F. Covid-19 and nf-kb: the hepcidin paradox and the iron storm – reply. Acta Biomed. 2020;91(4). doi:10.23750/abm.v91i4.10904
39. Gümüş H, Erat T, Öztürk İ, Demir A, Koyuncu I. Oxidative stress and decreased Nrf2 level in pediatric patients with COVID-19. J Med Virol. 2022;94(5):2259–2264. doi:10.1002/jmv.27640
40. Muchtaridi M, Amirah SR, Harmonis JA, Ikram EHK. Role of nuclear factor Erythroid 2 (Nrf2) in the recovery of long COVID-19 using natural antioxidants: a systematic review. Antioxidants. 2022;11(8):1551. doi:10.3390/antiox11081551
41. Al-Mamouri SRK, Al-Kufaishi AMA. Evaluation of total antioxidant capacity and total oxidant status in patients with COVID-19. J Pharm Negat Results. 2022;13(4). doi:10.47750/pnr.2022.13.04.016
42. Karkhanei B, Talebi Ghane E, Mehri F. Evaluation of oxidative stress level: total antioxidant capacity, total oxidant status and glutathione activity in patients with COVID-19. New Microbes New Infect. 2021;42:100897. doi:10.1016/j.nmni.2021.100897
43. Çakırca G, Damar Çakırca T, Üstünel M, Torun A, Koyuncu İ. Thiol level and total oxidant/antioxidant status in patients with COVID-19 infection. Ir J Med Sci. 2022;191(4):1925–1930. doi:10.1007/s11845-021-02743-8
44. Sengupta P, Dutta S, Roychoudhury S, D’souza UJA, Govindasamy K, Kolesarova A. COVID-19, oxidative stress and male reproduction: possible role of antioxidants. Antioxidants. 2022;11(3):548. doi:10.3390/antiox11030548
45. Paul AK, Hossain MK, Mahboob T, et al. Does oxidative stress management help alleviation of COVID-19 symptoms in patients experiencing diabetes? Nutrients. 2022;14(2):321. doi:10.3390/nu14020321
46. Ebert T, Tran N, Schurgers L, Stenvinkel P, Shiels PG. Ageing – oxidative stress, PTMs and disease. Mol Aspects Med. 2022;86:101099. doi:10.1016/j.mam.2022.101099
47. Shandilya S, Kumar S, Kumar Jha N, Kumar Kesari K, Ruokolainen J. Interplay of gut microbiota and oxidative stress: perspective on neurodegeneration and neuroprotection. J Adv Res. 2022;38:223–244. doi:10.1016/j.jare.2021.09.005
48. Wadhwa N, Mathew BB, Jatawa SK, Tiwari A. Lipid peroxidation: mechanism, models and significance. Int J Curr Sci. 2012;3:29–38.
49. Dorf J, Pryczynicz A, Matowicka-Karna J, et al. Could circulating biomarkers of nitrosative stress and protein glycoxidation be useful in patients with gastric cancer? Front Oncol. 2023;13. doi:10.3389/fonc.2023.1213802
50. Davies MJ. Protein oxidation and peroxidation. Biochem J. 2016;473(7):805–825. doi:10.1042/BJ20151227
51. Yalcin Kehribar D, Cihangiroglu M, Sehmen E, et al. The receptor for advanced glycation end product (RAGE) pathway in COVID-19. Biomarkers. 2021;26(2):114–118. doi:10.1080/1354750X.2020.1861099
52. Muhammad M, Hassan TM, Baba SS, et al. Exploring NFκB pathway as a potent strategy to mitigate COVID-19 severe morbidity and mortality. J Public Health Afr. 2022;13(3). doi:10.4081/jphia.2022.1679
53. Goel S, Saheb Sharif-Askari F, Saheb Sharif Askari N, et al. SARS-CoV-2 Switches ‘on’ MAPK and NFκB Signaling via the reduction of nuclear DUSP1 and DUSP5 expression. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.631879
54. Anvari E, Fred RG, Welsh N. The H1-receptor antagonist cetirizine protects partially against cytokine- and hydrogen peroxide-induced β-TC6 cell death in vitro. Pancreas. 2014;43(4):624–629. doi:10.1097/MPA.0000000000000076
55. Tong M, Yan X, Jiang Y, et al. Endothelial biomarkers in patients recovered from COVID-19 one year after hospital discharge: a cross-sectional study. Mediterr J Hematol Infect Dis. 2022;14(1):e2022033. doi:10.4084/MJHID.2022.033
56. Singh V, Kaur R, Kumari P, Pasricha C, Singh R. ICAM-1 and VCAM-1: gatekeepers in various inflammatory and cardiovascular disorders. Clin Chim Acta. 2023;548:117487. doi:10.1016/j.cca.2023.117487
57. Salehi M, Amiri S, Ilghari D, Hasham LFA, Piri H. The remarkable roles of the Receptor for Advanced Glycation End Products (RAGE) and its soluble isoforms in COVID-19: the importance of RAGE pathway in the lung injuries. Indian J Clin Biochem. 2023;38(2):159–171. doi:10.1007/s12291-022-01081-5
58. Spadaro S, Fogagnolo A, Campo G, et al. Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients. Crit Care. 2021;25(1). doi:10.1186/s13054-021-03499-4
59. Dorf J, Zaręba K, Pryczynicz A, et al. Diagnostic significance and utility of circulating redox biomarkers in patients with gastric cancer–preliminary study. Ann Med. 2023;55(2). doi:10.1080/07853890.2023.2241472
60. Kosanovic T, Sagic D, Djukic V, et al. Time course of redox biomarkers in covid-19 pneumonia: relation with inflammatory, multiorgan impairment biomarkers and ct findings. Antioxidants. 2021;10(7):1126. doi:10.3390/antiox10071126
61. Ducastel M, Chenevier‐gobeaux C, Ballaa Y, et al. Oxidative stress and inflammatory biomarkers for the prediction of severity and ICU admission in unselected patients hospitalized with covid‐19. Int J Mol Sci. 2021;22(14):7462. doi:10.3390/ijms22147462
62. Satała J, Woźniak A, Fabiś M, et al. Severe COVID-19 classified by simple covid risk index is associated with higher levels of advanced oxidation protein products and 8-hydroxy 2 deoxyguanosine. Epidemiol Infect. 2023;151. doi:10.1017/S0950268823001280
63. Šķesters A, Lece A, Kustovs D, Zolovs M. Selenium status and oxidative stress in SARS-CoV-2 patients. Medicina. 2023;59(3):527. doi:10.3390/medicina59030527
64. Žarković N, Orehovec B, Milković L, et al. Preliminary findings on the association of the lipid peroxidation product 4-hydroxynonenal with the lethal outcome of aggressive covid-19. Antioxidants. 2021;10(9):1341. doi:10.3390/antiox10091341
65. de Morais Batista F, Puga MAM, da Silva PV, et al. Serum biomarkers associated with SARS-CoV-2 severity. Sci Rep. 2022;12(1):1–9. doi:10.1038/s41598-022-20062-5
66. Żebrowska E, Maciejczyk M, Żendzian-Piotrowska M, Zalewska A, Chabowski A. High protein diet induces oxidative stress in rat cerebral cortex and hypothalamus. Int J Mol Sci. 2019;20(7):1547. doi:10.3390/ijms20071547
67. Maciejczyk M, Żebrowska E, Zalewska A, Chabowski A. Redox balance, antioxidant defense, and oxidative damage in the hypothalamus and cerebral cortex of rats with high fat diet-induced insulin resistance. Oxid Med Cell Longev. 2018;2018:1–11. doi:10.1155/2018/6940515
68. Bokhari MM, Khurshid R, Jabbar U, et al. Is there an association between thyroid dysfunction and breast cancer? Pak J Med Health Sci. 2022;16(4):252–255. doi:10.53350/pjmhs22164252
69. Eskelinen M, Saimanen I, Koskela R, Holopainen A, Selander T, Eskelinen M. Plasma Concentration of the Lipid Peroxidation (LP) biomarker 4-Ηydroxynonenal (4-HNE) in benign and cancer patients. In Vivo. 2022;36(2):773–779. doi:10.21873/INVIVO.12764
70. Haroun M, Elsewedy HS, Shehata TM, et al. Significant of injectable brucine PEGylated niosomes in treatment of MDA cancer cells. J Drug Deliv Sci Technol. 2022;71. doi:10.1016/j.jddst.2022.103322
71. Wang H, Wang P, Zhu BT. Mechanism of erastin-induced ferroptosis in MDA-MB-231 human breast cancer cells: evidence for a critical role of protein disulfide isomerase. Mol Cell Biol. 2022;42(6). doi:10.1128/mcb.00522-21
72. Abbaszadeh S, Javidmehr A, Askari B, Janssen PML, Soraya H. Memantine, an NMDA receptor antagonist, attenuates cardiac remodeling, lipid peroxidation and neutrophil recruitment in heart failure: a cardioprotective agent? Biomed Pharmacother. 2018;108:1237–1243. doi:10.1016/j.biopha.2018.09.153
73. Barrera G. Oxidative stress and lipid peroxidation products in cancer progression and therapy. ISRN Oncol. 2012;2012:1–21. doi:10.5402/2012/137289
74. Kim GH, Kim JE, Rhie SJ, Yoon S. The role of oxidative stress in neurodegenerative diseases. Exp Neurobiol. 2015;24(4):325–340. doi:10.5607/en.2015.24.4.325
75. Martín-Fernández M, Arroyo V, Carnicero C, et al. Role of oxidative stress and lipid peroxidation in the pathophysiology of NAFLD. Antioxidants. 2022;11(11):2217. doi:10.3390/antiox11112217
76. Tsubouchi K, Araya J, Yoshida M, et al. Involvement of GPx4-regulated lipid peroxidation in idiopathic pulmonary fibrosis pathogenesis. J Immunol. 2019;203(8):2076–2087. doi:10.4049/jimmunol.1801232
77. Yoshikawa T, Mifune Y, Inui A, et al. Influence of diabetes-induced glycation and oxidative stress on the human rotator cuff. Antioxidants. 2022;11(4):743. doi:10.3390/antiox11040743
78. Yang L, Wang Z. Bench-to-bedside: innovation of small molecule anti-SARS-CoV-2 drugs in China. Eur J Med Chem. 2023;257:115503. doi:10.1016/J.EJMECH.2023.115503
79. Wang Z, Yang L. Post-acute sequelae of SARS-CoV-2 infection: a neglected public health issue. Front Public Health. 2022;10. doi:10.3389/FPUBH.2022.908757
80. Smail SW, Babaei E, Amin K. Hematological, inflammatory, coagulation, and oxidative/antioxidant biomarkers as predictors for severity and mortality in COVID-19: a prospective cohort-study. Int J Gen Med. 2023;16:565–580. doi:10.2147/IJGM.S402206
81. Galougahi KK, Antoniades C, Nicholls SJ, Channon KM, Figtree GA. Redox biomarkers in cardiovascular medicine. Eur Heart J. 2015;36(25):1576–1582. doi:10.1093/EURHEARTJ/EHV126
82. Pastore A, Petrillo S, Piermarini E, Piemonte F. Systemic redox biomarkers in neurodegenerative diseases. Curr Drug Metab. 2015;16(1):46–70. doi:10.2174/138920021601150702161250
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.