")
Back to Journals » Clinical Ophthalmology » Volume 15
Real-World Outcomes in Diabetic Macular Edema for the 0.2 μg/Day Fluocinolone Acetonide Implant: Case Series from the Midlands, UK
Authors Mushtaq B, Bhatnagar A, Palmer H
Received 25 December 2020
Accepted for publication 9 February 2021
Published 7 July 2021 Volume 2021:15 Pages 2935—2943
DOI https://doi.org/10.2147/OPTH.S283561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bushra Mushtaq,1 Ajay Bhatnagar,2 Helen Palmer3
1Birmingham Midland Eye Centre, City Hospital SWBH NHS Trust, Birmingham, UK; 2Department of Ophthalmology, New Cross Hospital, The Royal Wolverhampton NHS Trust, Wolverhampton, UK; 3Ophthalmology Department, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK
Correspondence: Bushra Mushtaq
Birmingham Midland Eye Centre, City Hospital SWBH NHS Trust, Dudley Road, B18 7QH, UK
Tel +44 7976416571
Email [email protected]
Aim: To investigate real-world effectiveness and safety of fluocinolone acetonide (FAc) implant over three years of treatment in eyes with diabetic macular edema (DME) in a population with large ethnic diversity.
Methods: This audit of three large treatment centres in the UK involved retrospective collection of outcome data (best recorded visual acuity [BRVA] by Early Treatment Diabetic Retinopathy Study [ETDRS] letters, central retinal thickness [CRT], intraocular pressure [IOP] and use of supplementary treatments) from patients with DME treated with 0.2 μg/day FAc intravitreal implant with three-year follow-up expected.
Results: A total of 96 eyes were included. Ninety (93.8%) eyes had received prior intravitreal treatment. Increases in mean BRVA were significant at one, two and three years (p< 0.05). Overall, 78.1% of eyes gained or maintained BRVA; just over 50% gained ≥ 5 letters, representing a functional response. Eleven (11.6%) patients lost ≥ 10 letters by year three. Decreases in central retinal thickness (CRT) nearing 200 μm in the first year were sustained to three years (p < 0.0001). Patients with baseline VA ≥ 60 letters maintained their BRVA throughout follow-up, while significant improvements at month 12 (p< 0.0001) in those with baseline BRVA < 60 letters were maintained through month 36 (p < 0.005). Fifty-three (55.2%) eyes required no supplementary therapy during follow-up. Increases in IOP to ≥ 30 mmHg and ≥ 25 mmHg were seen in 12 (12.5%) and 23 (24.0%) eyes, respectively.
Conclusion: This study confirms the effectiveness and tolerability of FAc implant up to 36 months in a real-world setting, highlighting the importance of early treatment for sustaining functional vision for patients.
Keywords: fluocinolone acetonide, DME, diabetic macular edema, real-world, observational, case series
Introduction
Vision loss from diabetic retinopathy (DR) results primarily from proliferative retinopathy and diabetic macular edema (DME).1 Current treatments for DME include laser therapy, intravitreal anti-vascular endothelial growth factor (VEGF) injections and corticosteroid therapies.2–5 Anti-VEGF therapy is first line in the UK;6 however, 40% of patients are insufficiently responsive to these drugs.2,7
Intravitreal corticosteroid implants, including dexamethasone and fluocinolone acetonide (FAc), are effective in this setting.8 ILUVIEN® (0.2 µg/day FAc intravitreal implant) is indicated for treatment of vision impairment associated with chronic DME considered insufficiently responsive to available therapies.9 Its effectiveness and safety have been demonstrated in numerous studies.3,8,10–12 In UK clinical practice, many patients with DME who insufficiently respond to anti-VEGFs still continue to receive them, which is one of the major reasons for a discrepancy between clinical and real-world outcomes. Even though the main difference between clinical trials and real-world studies is the under-treatment due to the high burden/noncompliance related to anti-VEGF or short-term corticosteroids therapies and not the reason above.13,14
The objective of this study was to investigate the real-world effectiveness and safety profile of the FAc implant over three years of treatment in eyes with DME through an audit of three large treatment centres in the UK with the largest ethnic diversity outside of the southeast of the UK.15
Materials and Methods
Study Design
This study involved retrospective collection of data from a cohort of diabetic patients with DME treated with the FAc intravitreal implant in 2014 and 2015 and with three-year follow-up expected. The study was conducted across three sites in the West Midlands region of the UK: Birmingham Midland Eye Centre (BMEC), New Cross Hospital, Wolverhampton, and Queen Elizabeth Hospital, Birmingham. Ethics approval was not required as this was a service evaluation.
Patients treated with FAc intravitreal implant for management of DME were identified by the authors. All patients were included according to the inclusion/exclusion criteria detailed below. Ethical approval was not required as this was a retrospective collection of data.
This real-world cohort included 109 eyes from patients with DME treated between 2014 and 2015 at three sites in the West Midlands region of the UK and with three years of follow-up since treatment commenced. Thirteen eyes were excluded due to missing baseline data (n=1) or missing three-year follow-up data (n=12) due to death or moving out of area, so the analysis population included 96 eyes: 37 from BMEC, 34 from New Cross Hospital, Wolverhampton, and 25 from Queen Elizabeth Hospital, Birmingham.
Study Endpoints
Baseline patient demographic data were recorded, including age; sex; duration of DME; type of diabetes; prior treatments (including macular, focal and grid laser, pan-retinal photocoagulation and intravitreal therapy); and current intraocular pressure (IOP)-lowering drugs.
The following measurements were also collected at baseline and at one, two and three years’ post-implant: best recorded visual acuity (BRVA), measured with an Early Treatment Diabetic Retinopathy Study (ETDRS) letter chart; central retinal thickness (CRT); IOP; and use of supplementary treatments in combination with the FAc implant.
Rates of functional and anatomical response at three years were assessed based on the criteria defined by the Diabetic Retinopathy Clinical Research Network (DRCR.net): anatomical response was classed as a reduction of ≥20%16 and functional response as an increase of ≥5 EDTRS letters, with a good functional response defined as ≥15 EDTRS letters. Outcomes were also analyzed according to baseline BRVA (<60 EDTRS letters or ≥60 EDTRS letters).
Data and Statistical Analyses
Data are presented per eye and were included in the analyses only if patients had been treated with the FAc intravitreal implant for three years, baseline readings for both BRVA and CRT were recorded in the patient notes, and three-year outcome readings were available for at least one of VA or CRT. Data were reported as mean ± standard deviation (SD) unless otherwise stated. Statistical testing was performed using paired t-tests, and significance was taken as p<0.05. Values at reported time points were compared against baseline levels. A subgroup analyses compared the results for patients with BRVA <60 letters and ≥60 letters at baseline to assess differences in outcomes for patients with poor and moderate starting visual acuity.
Results
Patient Demographics
The baseline demographics and ocular characteristics of the eyes are summarized in Table 1. In terms of prior treatment, 90 (93.8%) eyes had prior intravitreal treatment (mean 1.8±0.8 different intravitreal therapies prior to FAc implant) and 33 (34.4%) of eyes were tried on both bevacizumab and ranibizumab therapy prior to FAc treatment.
 |
Table 1 Baseline Demographics and Ocular Characteristics |
Effectiveness
BRVA
Figure 1A shows change in BRVA from baseline up to three years’ follow-up, with data recorded at years one, two and three. The effects of the FAc implant on BRVA peaked at one year and were maintained up to three years after implantation. Mean BRVA was 49.0 letters at baseline, increasing to 54.5 letters at one year after FAc implantation, 53.3 letters at two years and 53.0 letters at three years (p<0.05, paired t-test; all time points versus baseline), representing overall changes from baseline of 5.5 letters, 4.3 letters and 4.0 letters at years one, two and three, respectively. Eleven (11.6%) patients lost 10 letters or more by year three; four of these patients lost ≥35 letters: two lost 35 letters and one each lost 40 and 50 letters.
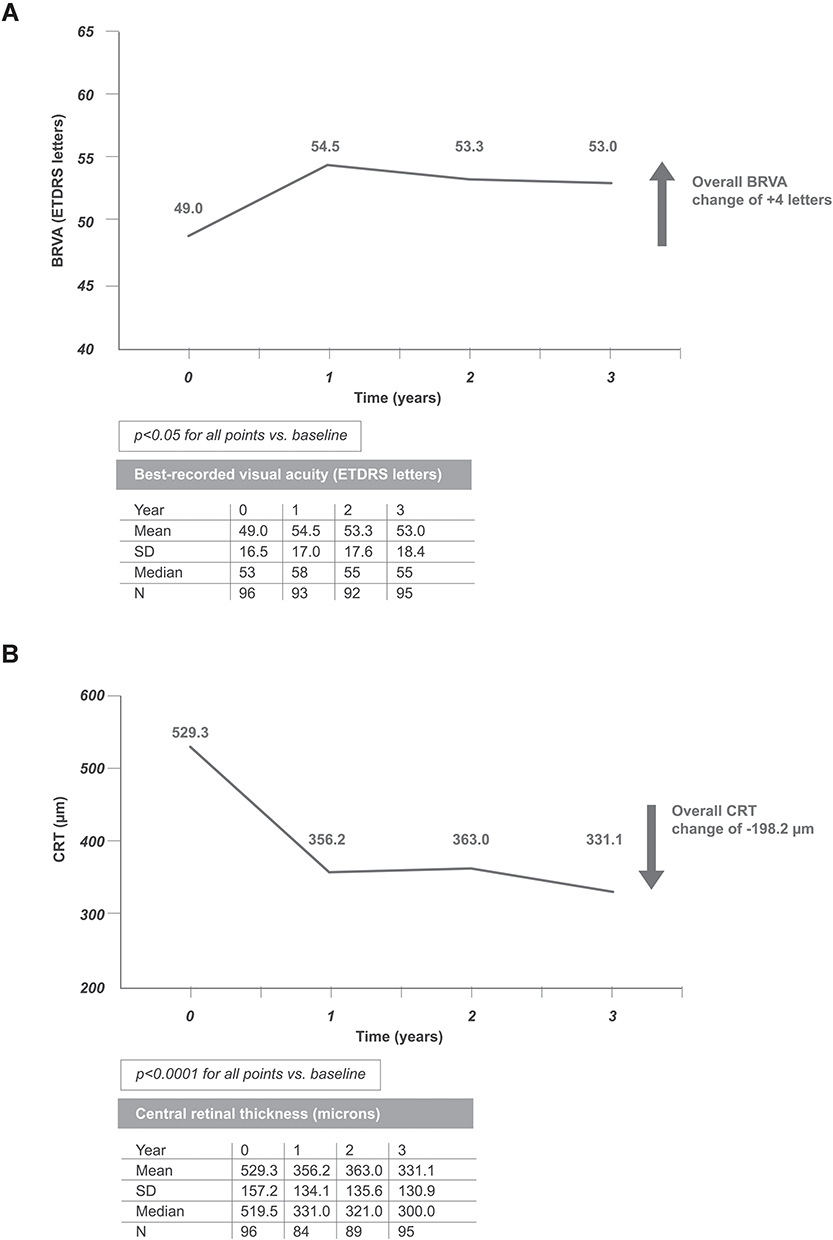 |
Figure 1 Mean BRVA (A) and CRT (B) at baseline, one, two and three years’ follow-up in 96 eyes after FAc implantation. |
CRT
Figure 1B shows change in CRT from baseline to three years’ follow-up. The effects of the FAc implant on CRT were sustained for up to three years after FAc implantation. Mean CRT was 529.3 µm at baseline, decreasing to 356.2 µm at one year after FAc implantation, 363.0 µm and 331.1 µm at years two and three, respectively (p<0.0001, paired t-test; all time points versus baseline). From the baseline of 529.3 µm, CRT decreased by 173.1 µm at year one after FAc implantation, and 166.3 µm and 198.1 µm at years two and three, respectively.
Functional and Anatomical Responses
Overall, 78.1% of eyes had a gain or maintained BRVA over a three-year follow-up period, while 52.6% of eyes gained ≥5 letters, thus responding functionally according to the definition of DRCR.net. Compared with good functional responders (≥15 letters gained, n=18), poor functional responders (≥5 letters lost, n=20) had:
- longer mean duration of DME (4.2 years vs 3.8, respectively)
- more mean previous intravitreal treatments (7.5 [n=19] vs 6.2 [n=17])
- received a similar number of supplementary intravitreal treatments (7.2 [n=11] vs 7.2 [n=10]).
According to the definition of DRCR.net, 72 (75%) eyes responded anatomically, defined as a decrease in CRT of ≥20% (Figure 2). Interestingly, only 39 (54.2%) of these eyes showed a corresponding VA gain of ≥5 letters, which complements previous findings that VA responses do not correlate with anatomical responses.
 |
Figure 2 Mean BRVA and CRT at baseline, one, two and three years’ follow-up after FAc implantation in eyes that responded anatomically (increase of ≥20% EDTRS letters). |
Supplementary Intravitreal Treatment
Overall, 53 (55.2%) eyes required no supplementary therapy during the three years of follow-up. The 43 (44.8%) eyes that received supplementary intravitreal injections had a mean of 6.8 intravitreal injections over the three years, with a mean time to first treatment of 2.0±0.7 years. Overall, 7.1 anti-VEGFs were given to 40 patients vs 1.3 corticosteroid treatments given to eight patients. Laser treatment was required in seven (7.3%) of 96 eyes after FAc implant, with a mean time to laser of 2.3±0.5 years.
Subgroup Analyses
BRVA (<60 Letters vs ≥60 Letters)
Compared with eyes with BRVA ≥60 letters at baseline (n=30), those with BRVA <60 letters at baseline (n=66) had:
- slightly longer mean duration of disease (3.8 years vs 3.7 years)
- lower mean BRVA (41.0 letters vs 66.7 letters)
- higher CRT (560.1 µm vs 461.5 µm)
- higher rate of proliferative retinopathy (29.2% vs 13.5%).
Subgroup analysis identified greater gains in EDTRS letters in patients with baseline BRVA <60 letters than in those with ≥60 letters at baseline; mean increase of 6.4 letters from a baseline of 41.0±13.2 letters to 47.4±18.6 letters (p<0.005 vs baseline) versus mean loss of 1.7 letters from a baseline of 66.7±5.6 letters to 65.0±10.6 letters (p>0.05 vs baseline), respectively. However, of patients who lost letters, the greatest loss was also observed in the <60 group, with three eyes losing ≥35 letters in the ≥60 letters group. Overall, eyes with ≥60 letters at baseline maintained BRVA over the three years of treatment (Figures 3 and 4).
 |
Figure 3 Mean BRVA (EDTRS letters) at baseline, one, two and three years’ follow-up after FAc implantation in eyes with BRVA <60 letters and ≥60 letters at baseline. |
 |
Figure 4 Box and whisker plot comparing mean change in BRVA (EDTRS letters) at three years’ follow-up for eyes with BRVA <60 letters and ≥60 letters at baseline. Values shown include the median (centre box line), the 25th and 75th interquartile ranges (box) and maximum and minimum values (whisker bars). |
CRT
Subgroup analysis also identified a numerical trend towards a greater reduction in CRT in patients with baseline BRVA <60 letters than in those with ≥60 letters at baseline, with mean decreases of 225.0 µm from baseline of 560.1±162.3 µm to 335.1±139.7 µm vs mean reduction of 139.4 µm from 461.5±122.6 µm to 322.2±110.0 µm, respectively.
Supplementary Intravitreal Treatments
Subgroup analysis identified that similar proportions of patients with baseline BRVA <60 letters and ≥60 letters at baseline required supplementary intravitreal treatments during follow-up after FAc implant, but the mean number of treatments given was lower for those with BRVA <60 letters: 6.4±4.4 (n=29) vs 7.6±5.6 (n=14).
Safety
IOP-Related Events
Increases in IOP to ≥30 mmHg were seen in 12 (12.5%) eyes and to ≥25 mmHg in 23 (24.0%) eyes.
At baseline 10 (10.4%) eyes were receiving IOP-lowering drops. A further 4 (4.2%) had a history of IOP therapy requiring treatment. By year 3, 29 (30.2%) eyes were being managed with IOP-lowering drops (mean of 1.6 treatments). Seventeen (17.7%) eyes required changes to or started IOP-lowering therapy. Of the 10 (10.4%) eyes receiving IOP-lowering treatment at baseline, five (5.2%) required an increase in or additional IOP-lowering treatment.
Two eyes received selective laser trabeculectomy (SLT), one received cyclodiode laser treatment, and one required trabeculectomy due to neovascular glaucoma.
Discussion
This is the first time that data on VA, CRT, IOP and use of supplementary treatments in combination with the FAc implant in the UK have been collected from three centres based in the Midlands area of the United Kingdom. The study confirms the effectiveness and tolerability of the FAc implant up to 36 months in a real-world setting and the benefits to patients in terms of improving or maintaining vision.
Use of the FAc implant led to clinically meaningful outcomes over a 36-month period, with VA improved or maintained in 78.1% of eyes. The FAc implant was able to maintain moderate vision, as shown by the stabilization of VA when starting VA was ≥60 letters, which remained above this value throughout the 36 months. Although marked improvements in VA were observed in the group with a worse starting VA (<60 letters), final VA was significantly lower than in those with starting VA ≥60 letters (47.4 letters vs 65.0 letters), which highlights the value of treating earlier to sustain better functional vision for patients.
As Figure 4 shows, on average, more eyes in the ≥60 letter group (n=10/30; 33.3%) experienced letter loss than in the <60 letter group (n=13/66; 19.7%); However, the greatest mean loss occurred in eyes in the <60 letter group, with an average of 18.6 letters lost at month 36 versus 12.7 letters in the ≥60 letter group. This is important, as the greater loss in BRVA combined with the poorer starting VA, means that the risk of a poorer overall outcome is greater should an eye experience a loss of letters. Indeed, three eyes in the <60 letter group had losses of ≥35 letters and the BRVA letter score was zero in all three cases at month 36. These patients had diabetes for many decades (two had type 1 and one died in his 50s) and proliferative diabetic retinopathies (ie, known retinal ischemia). There was clearly retinal ischemia in these patients with longstanding diabetes and one also had known structural damage from ERM/scarring. A fourth patient with the largest letter loss (50 letters) was from the ≥60 letter group, with a BRVA letter score of 76 at baseline and 26 at three years. This patient had type 2 diabetes, DME for 6.6 years, ERM and IOP of 22 mmHg at baseline. He had significant prior laser therapy and was receiving IOP therapy. His left eye has been very successfully treated with FAc implant and then retreated after 3 years.
The other notable impact is the effect of letter losses on the overall mean. Indeed, when those eyes with a letter loss (ie, a loss ≥–1 at month 36) were excluded, to analyze only those eyes that remained unchanged or improved, changes in VA were 12.6±11.0 ETDRS letters (n=52) in the <60 letter group versus 3.9±3.3 ETDRS letters (n=20) in the ≥60 letter group. Irrespective of these changes, the final VA in the <60 letter group was still notably lower at month 36 than was observed in the ≥60 letter group (ie, 52.9 vs 69.3 letters, respectively). This again emphasizes the importance of treating VA sooner to achieve the best functional outcomes for the patient.
Baseline CRT was slightly higher in this study (529.3 µm) compared with other real-world FAc studies (451–494 µm),17–20 which may reflect higher DME disease activity in our study population due to delays before being moved on to effective therapy for a variety of reasons. This also seems to be reflected in the observation that BRVA was below 60 ETDRS letters in around two-thirds of the patients studied and that prior treatments (7.3 intravitreal treatments including both anti-VEGFs and corticosteroids) had been extensively used prior to commencing therapy with the fluocinolone acetonide implant. In all analyses, CRT was consistently improved. This contrasts with findings from studies with the dexamethasone implant: for example, in the Macular Edema: Assessment of Implantable Dexamethasone in Diabetes (MEAD) trial, peak CRT was variable4 although this effect may be explained by the fixed 6-monthly treatment regimen in MEAD trial when it is known that levels of dexamethasone peak around 2 months after injection.21
Baseline characteristics showed that patients had advanced disease (mean duration 3.7 years) and had already received multiple treatments prior to the FAc implantation; however, a single FAc treatment resulted in sustained, stable and predictable mean improvements in both BRVA and CRT that lasted up to 36 months. Overall improvements in VA and CRT in the Retro-IDEAL study, which reported mean outcomes from real-life clinical practices in Germany, were consistent with the those in the study reported here, although it is important to acknowledge that the follow-up period in Retro-IDEAL was on average 30.8 months and so outcomes are not directly comparable.21
The subgroup analysis of anatomical responders confirms previous findings that VA responses do not correlate linearly with anatomical response.
Fifty-three (55.2%) eyes required no supplementary therapy during the three years of follow-up. This is lower than the figure recorded in the Retro-IDEAL study over the same duration of follow-up (69.1%).22 As 42.7% of eyes in our study had proliferative diabetic retinopathy at baseline, some use of anti-VEGF may have been associated with treatment of this comorbidity. The current data also shed light on differences between the intravitreal therapies used. Consistent with the Retro-IDEAL study,22 anti-VEGFs were used more commonly than corticosteroids (7.1 anti-VEGFs were given to 40 patients vs 1.3 corticosteroid treatments given to eight patients). The most frequently administered anti-VEGF was ranibizumab (n=27 eyes, with a mean number of injections of 5.7) followed by aflibercept (n=20 eyes, with a mean number of injections of 6.0). In 10 patients, multiple classes of anti-VEGF were used as supplemental treatments.
The FAc implant was well tolerated, with 30.2% of eyes requiring an IOP-lowering drop after FAc implantation,18,22,23 which is in line with other real-world data. This was lower than the overall number reported in the Retro-IDEAL study (49.4%),22 although the Retro-IDEAL study had a significantly larger proportion of patients being treated with IOP-lowering drops at baseline (22.2%) than the current study (10.4%).22 In terms of pressure changes, both studies reported a similar number of patients with an IOP ≥30 mmHg (12.5% vs 12.3% in the Retro-IDEAL study22). In the Retro-IDEAL study,22 IOP-lowering surgery was required in 3.7% of eyes vs 1.0% in the current study, both of which are lower than the 4.8% reported in the FAME trial.3 The findings of our study confirm the safety profile of the FAc implant previously identified in other real-world studies in the UK, Germany, Portugal and the United States.18,22–24
Visual acuity outcome in our study may have been underestimated, because we used BRVA rather than best corrected VA (BCVA).
Conclusion
This study further supports the effectiveness and tolerability of the 0.2 µg/day FAc implant over a 36-month period in patients with DME, with results demonstrating that clinically meaningful changes in anatomy and function were observed and maintained throughout the duration of the study.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Ethical approval was not required as this was a retrospective collection of data.
Acknowledgments
Editorial support in the development of this manuscript was provided by Gemma Lough and Prescript Communications and funded by Alimera Sciences in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Alimera Sciences.
Disclosure
Miss Bushra Mushtaq reports grants and personal fees from Novartis and consultant advisory board and travel grants from Bayer and Alimera Sciences, outside the submitted work. Miss Helen Palmer reports non-financial support from Alimera Sciences during the conduct of the study. The authors reported no other potential conflicts of interest for this work.
References
1. Sivaprasad S, Gupta B, Gulliford MC, et al. Ethnic variations in the prevalence of diabetic retinopathy in people with diabetes attending screening in the United Kingdom (drive uk). PLoS One. 2012;7(3):e32182–e82. doi:10.1371/journal.pone.0032182
2. Wells JA, Glassman AR, Ayala AR, et al.; Diabetic Retinopathy Clinical Research N. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203. doi:10.1056/NEJMoa1414264
3. Campochiaro PA, Brown DM, Pearson A, et al. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology. 2012;119(10):2125–2132. doi:10.1016/j.ophtha.2012.04.030
4. Boyer DS, Yoon YH, Belfort R
5. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European society of retina specialists (euretina). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
6. Kodjikian L, Bellocq D, Bandello F, et al. First-line treatment algorithm and guidelines in center-involving diabetic macular edema. Eur J Ophthalmol. 2019;29(6):573–584.
7. Gonzalez VH, Campbell J, Holekamp NM, et al. Early and long-term responses to anti–vascular endothelial growth factor therapy in diabetic macular edema: analysis of protocol i data. Am J Ophthalmol. 2016;172:72–79. doi:10.1016/j.ajo.2016.09.012
8. Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet. 2010;376(9735):124–136. doi:10.1016/S0140-6736(09)62124-3
9. Alimera Sciences. Iluvien 190 Micrograms Intravitreal Implant in Applicator. Aldershot: Alimera Sciences Limited; 2019.
10. Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626–35.e2. doi:10.1016/j.ophtha.2010.12.028
11. Loewenstein A, Chakravarthy U. 0.19 mg fluocinolone acetonide intravitreal implant: place in the management of diabetic macular edema. Minerva Oftalmol. 2018;60(2):71–82.
12. Fusi-Rubiano W, Blow RR, Lane M, Morjaria R, Denniston AK. Iluvien (fluocinolone acetonide 0.19 mg intravitreal implant) in the treatment of diabetic macular edema: a review. Ophthalmol Ther. 2018;7(2):293–305. doi:10.1007/s40123-018-0145-7
13. Pochopien M, Beiderbeck A, McEwan P, Zur R, Toumi M, Aballéa S. Cost-effectiveness of fluocinolone acetonide implant (iluvien®) in uk patients with chronic diabetic macular oedema considered insufficiently responsive to available therapies. BMC Health Serv Res. 2019;19(1):22. doi:10.1186/s12913-018-3804-4
14. Quhill F, Beiderbeck A. Cost advantage of fluocinolone acetonide implant (iluvien®) versus ranibizumab in the treatment of chronic diabetic macular oedema. Glob Reg Health Technol Assess. 2017;4(1):
15. Wykoff CC, Chakravarthy U, Campochiaro PA, Bailey C, Green K, Cunha-Vaz J. Long-term effects of intravitreal 0.19 mg fluocinolone acetonide implant on progression and regression of diabetic retinopathy. Ophthalmology. 2017;124(4):440–449. doi:10.1016/j.ophtha.2016.11.034
16. Dugel PU, Campbell JH, Kiss S, et al. Association between early anatomic response to anti-vascular endothelial growth factor therapy and long-term outcome in diabetic macular edema: an independent analysis of protocol i study data. Retina. 2019;39(1):88–97. doi:10.1097/IAE.0000000000002110
17. Alfaqawi F, Lip PL, Elsherbiny S, Chavan R, Mitra A, Mushtaq B. Report of 12-months efficacy and safety of intravitreal fluocinolone acetonide implant for the treatment of chronic diabetic macular oedema: a real-world result in the United kingdom. Eye (Lond). 2017;31(4):650–656. doi:10.1038/eye.2016.301
18. Bailey C, Chakravarthy U, Lotery A, Menon G, Talks J. Real-world experience with 0.2 mug/day fluocinolone acetonide intravitreal implant (iluvien) in the United kingdom. Eye (Lond). 2017;31(12):1707–1715. doi:10.1038/eye.2017.125
19. Fusi-Rubiano W, Mukherjee C, Lane M, et al. Treating diabetic macular oedema (dmo): real world uk clinical outcomes for the 0.19mg fluocinolone acetonide intravitreal implant (iluvien) at 2 years. BMC Ophthalmol. 2018;18(1):62. doi:10.1186/s12886-018-0726-1
20. Currie CJ, Holden SE, Berni E, Owens DR. Evaluation of the clinical effectiveness of fluocinolone acetonide 190 micrograms intravitreal implant in diabetic macular edema: a comparison between study and fellow eyes. Curr Med Res Opin. 2017;33(sup2):19–31. doi:10.1080/03007995.2017.1366659
21. Chang-Lin JE, Attar M, Acheampong AA, et al. Pharmacokinetics and pharmacodynamics of a sustained-release dexamethasone intravitreal implant. Invest Ophthalmol Vis Sci. 2011;52:80–86. doi:10.1167/iovs.10-5285
22. Augustin AJ, Bopp S, Fechner M, et al. Three-year results from the retro-ideal study: real-world data from diabetic macular edema (DME) patients treated with iluvien® (0.19 mg fluocinolone acetonide implant). Eur J Ophthalmol. 2019;1120672119834474.
23. Chakravarthy U, Taylor SR, Koch FHJ, Castro de Sousa JP, Bailey C. Changes in intraocular pressure after intravitreal fluocinolone acetonide (iluvien): real-world experience in three European countries. Br J Ophthalmol. 2019;103(8):1072–1077. doi:10.1136/bjophthalmol-2018-312284
24. Eaton A, Koh SS, Jimenez J, Riemann CD. The user study: a chart review of patients receiving a 0.2 microg/day fluocinolone acetonide implant for diabetic macular edema. Ophthalmol Ther. 2019;8(1):51–62. doi:10.1007/s40123-018-0155-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.