")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Randomized Double-Blinded Comparison of Intermittent Boluses Phenylephrine and Norepinephrine for the Treatment of Postspinal Hypotension in Patients with Severe Pre-Eclampsia During Cesarean Section
Authors Pan ZB, Sheng ZM , Zhu M , Mei Z , Shen YP, Liu JP, Qian XW
Received 26 October 2023
Accepted for publication 8 February 2024
Published 29 February 2024 Volume 2024:18 Pages 639—650
DOI https://doi.org/10.2147/DDDT.S446657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Zheng-Bin Pan,1,2 Zhi-Min Sheng,1 Miao Zhu,1 Zhong Mei,1 Yan-Ping Shen,1 Jin-Ping Liu,1 Xiao-Wei Qian1
1Department of Anesthesiology, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Anesthesiology, Shaoxing Maternity and Child Health Care Hospital, Shaoxing, People’s Republic of China
Correspondence: Xiao-Wei Qian, Department of Anesthesiology, Women’s Hospital, Zhejiang University School of Medicine, Xueshi Road 1, Hangzhou, 310006, People’s Republic of China, Email [email protected]
Background: Norepinephrine has fewer negative effects on heart rate (HR) and cardiac output (CO) for treating postspinal hypotension (PSH) compared with phenylephrine during cesarean section. However, it remains unclear whether fetuses from patients with severe pre-eclampsia could benefit from the superiority of CO. The objective of this study was to compare the safety and efficacy of intermittent intravenous boluses of phenylephrine and norepinephrine used in equipotent doses for treating postspinal hypotension in patients with severe pre-eclampsia during cesarean section.
Methods: A total of 80 patients with severe pre-eclampsia who developed PSH predelivery during cesarean section were included. Eligible patients were randomized at a 1:1 ratio to receive either phenylephrine or norepinephrine for treating PSH. The primary outcome was umbilical arterial pH. Secondary outcomes included other umbilical cord blood gas values, Apgar scores at 1 and 5 min, changes in hemodynamic parameters including CO, mean arterial pressure (MAP), HR, stroke volume (SV), and systemic vascular resistance (SVR), the number of vasopressor boluses required, and the incidence of bradycardia, hypertension, nausea, vomiting, and dizziness.
Results: No significant difference was observed in umbilical arterial pH between the phenylephrine and norepinephrine groups (7.303± 0.38 vs 7.303± 0.44, respectively; P=0.978). Compared with the phenylephrine group, the overall CO (P=0.009) and HR (P=0.015) were greater in the norepinephrine group. The median [IQR] total number of vasopressor boluses required was comparable between the two groups (2 [1 to 3] and 2 [1 to 3], respectively; P=0.942). No significant difference was found in Apgar scores or the incidence of maternal complications between groups.
Conclusion: A 60 μg bolus of phenylephrine and a 4.5 μg bolus of norepinephrine showed similar neonatal outcomes assessed by umbilical arterial pH and were equally effective when treating PSH during cesarean section in patients with severe pre-eclampsia. Norepinephrine provided a higher maternal CO and a lower incidence of bradycardia.
Keywords: phenylephrine, norepinephrine, hypotension, umbilical arterial pH
Introduction
Severe pre-eclampsia is a critical disorder of pregnancy associated with placental hypoperfusion.1,2 Currently, spinal anesthesia is the preferred anesthetic method in pre-eclamptic women without contraindications to neuraxial anesthesia.1 Although postspinal hypotension (PSH) is less frequent, less severe, and easier to treat in patients with severe pre-eclampsia compared with healthy parturients, effective treatment of hypotension is essential in women with severe pre-eclampsia given the potential adverse effects to the fetus for pre-existing fetoplacental hypoperfusion.1
Phenylephrine is widely used in obstetric anesthesia. However, it may cause reflex decreases in maternal heart rate (HR) and cardiac output (CO) while increasing blood pressure (BP).3–5 Although these changes seem to be tolerated well by healthy parturients and fetuses, a potentially compromised fetus born to a mother with severe pre-eclampsia may not be able to compensate for further reduction in uteroplacental blood.6 Therefore, investigators have explored an alternative vasopressor with less reflexive negative chronotropic effects.
Norepinephrine is an α-adrenergic receptor agonist with weak β-adrenergic receptor agonist activity. Growing evidence supports that norepinephrine is as effective as phenylephrine in maintaining BP and has better maintenance of HR and CO than phenylephrine.7–14 In addition, norepinephrine has advantages in neonatal outcomes. In a meta-analysis that included 52 RCTs with a total of 4126 patients, norepinephrine was considered to have a low probability of adversely affecting the fetal acid-base status as assessed by their effect on umbilical arterial base excess (probability rank order: norepinephrine > mephentermine > metaraminol > phenylephrine > ephedrine).15 Nevertheless, most studies comparing the two drugs were performed in low-risk parturients despite using different dosing regimens and schedules. The evidence on the optimum vasopressor choice for treating PSH in patients with severe pre-eclampsia is inadequate. Further studies are warranted to investigate whether norepinephrine has any clinically significant advantage on neonatal outcomes in this type of patient.
Therefore, we aimed to compare the safety and efficacy of phenylephrine and norepinephrine administered as intermittent boluses at equipotent doses for treating PSH in patients with severe pre-eclampsia during cesarean section.
Materials and Methods
This randomized, controlled, double-blinded study was conducted between June 21, 2021, and March 15, 2022, after approval of the Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine (Hangzhou, China) (Approval No. IRB-20211038-R). The study was registered prior to patient enrollment at the Chinese Clinical Trials Registry (www.chictr.org.cn, Registration No. ChiCTR2100047529, principal investigator: Xiao-Wei Qian). Written informed consent was obtained from all participants.
We recruited patients with severe pre-eclampsia for cesarean section under spinal anesthesia. Exclusion criteria included: American Society of Anesthesiologists physical status (ASA)>4, multiple pregnancies, height<140 cm or>180 cm, weight<50 kg or>100 kg, age<18 years or>40 years, thrombocytopenia, coagulopathy, any contraindication to spinal anesthesia, active labor, umbilical cord prolapse, placenta previa or other placental abnormalities, cardiovascular or cerebrovascular disease, known fetal abnormalities, less than 28 weeks gestation, and inability or refusal to give informed consent.
A computer-generated randomization list (Microsoft Excel, Microsoft Corporation, Redmond, WA, USA) with 1:1 allocation was created by an independent statistician. Random codes were placed in sealed opaque envelopes and sequentially handed to a research nurse responsible for preparing the study drugs in identical syringes labeled “study drug”. In cases of spinal anesthesia failure or if the patient did not develop hypotension predelivery, this patient was excluded from the study, and the random code was automatically allocated to the next patient. All patients, surgeons, and other investigators were blinded to the group allocation.
Upon arrival into the operating room, the patient was placed in the left uterine displacement (LUD) position. The antecubital vein was cannulated with an 18-gauge indwelling needle to establish vascular access. Standard monitoring was applied, including electrocardiography, non-invasive BP, and pulse oximetry. Cardiovascular monitoring was performed with a TL-400 non-invasive hemodynamic monitor (T-Line-400, TensysMedical Inc., San Diego, CA, USA). After a bracelet equipped with a sensor was placed on the wrist, the pulse wave was obtained. CO, stroke volume(SV), and systemic vascular resistance (SVR) could be detected. After a brief calm period, the baseline mean arterial pressure (MAP) and other hemodynamic parameters were determined by averaging three consecutive measurements taken 1 minute apart with a difference of less than 10%.
Patients were placed in the left lateral position for regional anesthesia. The epidural puncture was performed with an 18-gauge Tuohy needle at the estimated L1-2 vertebral interspace conformed by the loss-of-resistance to saline technique. The epidural catheter was inserted 3–4 cm cephalad into the epidural space. No anesthetics were given through the epidural catheter at this time. Spinal anesthesia was then performed in the midline at the estimated L3-4 vertebral interspace using a 25-gauge spinal needle. After confirming free outflow of cerebrospinal fluid, 3 mL (15 mg) of hyperbaric ropivacaine (1.5 mL ropivacaine 1% + 1.5 mL dextrose 10%) was injected intrathecally over 30 seconds. Co-hydration with 10 mL kg-1 Lactated Ringer’s solution was rapidly administered, initiated after cerebrospinal fluid appeared in the hub of the spinal needle. Thereafter, no further fluids were administered. The patient was then returned to the LUD position. Loss of cold sensation up to the T6 dermatome or above was considered adequate for surgery. All patients continued to receive 40% oxygen by face mask during their surgery.
MAP and HR were recorded every minute immediately after completion of intrathecal injection. CO, SV, and SVR were measured continuously and recorded at 1-minute intervals. Patients were randomly allocated to receive an intravenous bolus of 4.5 µg norepinephrine (the norepinephrine group) or 60 µg phenylephrine (the phenylephrine group) to rescue maternal hypotension, which was defined as MAP<80% of baseline. If hypotension was not corrected within 1 min, an additional bolus of assigned vasopressor was administered until hypotension was corrected. If hypotension was not corrected by cumulative use of 300 µg phenylephrine or 22.5 µg norepinephrine, an intravenous bolus of 10 mg ephedrine was given for rescue. Atropine 0.5 mg was administered intravenously for bradycardia (HR<60 bpm) comorbid with hypotension or HR<50 bpm, irrespective of BP. Urapidil 10 mg was administered intravenously when the MAP was ≥ 120% of the baseline. These steps were repeated if necessary.
The study endpoint was set at delivery. Umbilical artery and vein blood samples were collected from a double-clamped cord, and blood gas was immediately analyzed. Neonatal outcomes were evaluated by a pediatrician unaware of the group assignment. The treatment after the study period was at the discretion of the attending anesthesiologist.
The primary outcome was umbilical arterial pH. Secondary outcomes included other umbilical cord blood gas values, changes in hemodynamic parameters (CO, MAP, HR, SV, and SVR) during the study time, Apgar scores at 1 and 5 min, the number of vasopressor boluses required, and the incidence of bradycardia, hypertension, nausea, vomiting and dizziness.
Sample Size Calculation
We estimated that 40 participants per study group would be needed to detect a difference of 0.03 units in umbilical arterial pH with 80% power and a two-tailed P-value of 0.05. This was based on a previous study that compared phenylephrine and norepinephrine while treating postspinal hypotension and found a standard deviation of 0.049 for the umbilical arterial pH in patients receiving norepinephrine.16 Therefore, we calculated the number of patients required for the study to be 33 per group. To compensate for a potential dropout rate of 10%, we planned to enroll 40 patients in each group.
Statistical Analysis
We performed all statistical analyses using IBM SPSS Statistics version 25.0 (IBM SPSS Inc., Chicago, IL, USA) and GraphPad Prism version 8.0 (GraphPad Inc., San Diego, CA). Continuous data were assessed for normality by ShapiroeWilk’s test and analyzed using Student’s t-test or Mann–Whitney U-test as appropriate. Categorical data were analyzed using the Chi-square test or Fisher’s exact test. Since the number of data points recorded varied among patients because of varying surgical times, serial hemodynamic data (MAP, HR, CO, SV, and SVR) were analyzed by a two-step summary measures technique.17 First, the area under the curve (AUC) for values plotted against time was calculated using the trapezium rule; standardized values were derived by dividing the values for AUC by the number of data points recorded for each patient. Then, standardized values were compared using the t-test or Mann–Whitney test. P<0.05 was regarded as statistically significant.
Results
A total of 128 patients were screened for eligibility. Of these, 12 met one or more exclusion criteria, and 36 were excluded because they did not experience hypotension predelivery. Eighty patients underwent randomization and were evenly allocated to the phenylephrine and the norepinephrine group (Figure 1). Umbilical arterial blood gas was not performed in one patient due to difficulty in umbilical cord blood sample collection in the phenylephrine group. In the norepinephrine group, one patient was excluded because the difference in pH between the umbilical arterial and venous blood samples was less than 0.02 units, indicating that both samples came from the same vessel. Thus, umbilical arterial and venous blood gas values were available for final analysis in 39 patients in each group. The demographic data, baseline characteristics, sensory block level, surgical time, and intravenous fluid volume given were comparable between groups (Table 1).
 |
Table 1 The Demographic Data, Baseline Characteristics, Intraoperative Details and Maternal Side Effect |
 |
Figure 1 Flow diagram of study. |
Neonatal outcomes are summarized in Table 2. Umbilical arterial pH (primary outcome) was comparable between groups. No neonate had fetal acidosis, defined as umbilical arterial pH<7.20. We also detected no difference in other umbilical cord blood gas values. Neonatal weights and Apgar scores at 1 minute and 5 minutes were comparable between groups. The number of neonates in the phenylephrine group with Apgar score<7 at 1 minute was 1 versus 1 in the norepinephrine group. One neonate had Apgar scores<9 at 5 min in the phenylephrine and norepinephrine groups, respectively.
 |
Table 2 Neonatal Outcomes |
Due to the failure to obtain hemodynamic data, 27 patients in the phenylephrine group and 26 patients in the norepinephrine group were finally included in the analysis of CO, SV, and SVR. The baseline hemodynamic values were comparable between groups (Table 3). Since the time from spinal anesthesia to delivery varied among patients, a variable number of measurements of hemodynamics were recorded for each patient. Individual changes in CO over time for each patient are shown in Figures 2. Figure 3 showed that the overall CO was greater in the norepinephrine group compared with that in the phenylephrine group (standardized CO 6.31 ± 1.08 L min-1 vs 5.45 ± 1.21 L min-1, P = 0.009). HR and SV were greater in the norepinephrine group than in the phenylephrine group (standardized HR 80.4 ± 7.3 vs 85.3 ± 9.9,P = 0.015; standardized SV 78.1 ± 16.2 vs 67.4 ± 18.5 mL, P = 0.029). There were no significant differences in the standardized MAP (standardized MAP 100.5 ± 10.8 vs 96.6 ± 10.7, P = 0.718) and SVR (1181 (855, 2466.54) dyn s cm-5 vs 1177 (645.31, 2175.88) dyn s cm-5, P = 0.656) between groups. There were no statistically significant differences in the incidence of hypertension and the number of vasopressor boluses. Serial changes in MAP, HR, and CO in the first 12 min (a time point with data available for most patients) after subarachnoid block are shown in Figures 4–6.
 |
Table 3 Baseline Hemodynamics Obtained by the TL-400. Hemodynamic Data Were Not Available for 25 Patients |
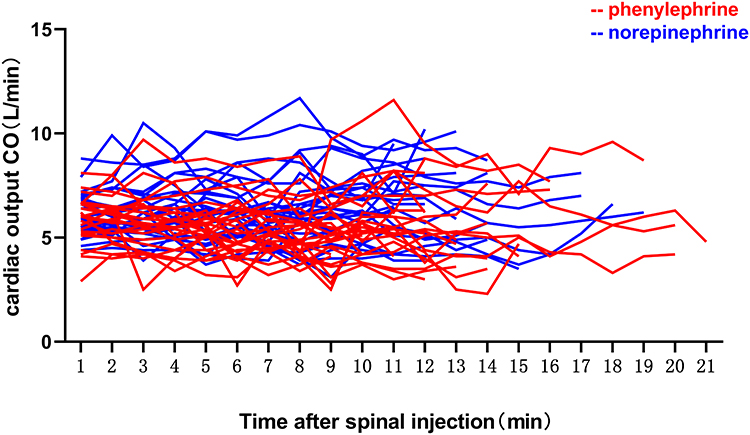 |
Figure 2 Changes in cardiac output (CO) for all patients plotted against time. Values on the x-axis corresponded to the number of each consecutive CO measurement made with the TL-400 monitor set to record at 1-min. |
 |
Figure 3 Bars show the area under the curve (AUC) for the two groups standardized for each patient by dividing by the number of data points recorded. Comparison of the calculated values for standardized AUC showed that CO was greater over time in the norepinephrine group versus the phenylephrine group (P = 0.009). |
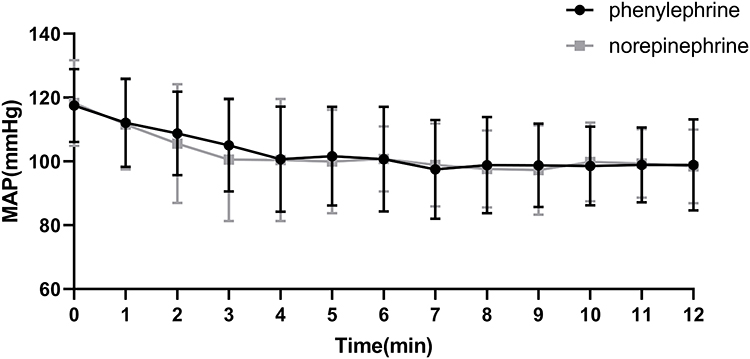 |
Figure 4 Serial changes in mean arterial pressure (MAP) for the first 12 minutes after subarachnoid block, data are presented as mean and standard deviation(SD). The value at time 0 corresponds to the baseline value. |
 |
Figure 5 Serial changes in heart rate (HR) for the first 12 minutes after subarachnoid block, data are presented as mean and SD. The value at time 0 corresponds to the baseline value. |
 |
Figure 6 Serial changes in CO for the first 12 minutes after subarachnoid block, data are presented as mean and SD. The value at time 0 corresponds to the baseline value. |
The incidence of bradycardia was higher in the phenylephrine group compared with that in the norepinephrine group (20.5% vs 5.1%, P = 0.042). No patients developed reflex hypertension or dizziness in either group. Two patients developed nausea in each group, which resolved with the treatment of hypotension and did not require any other specific treatment.
Discussion
The main finding of our study was that when norepinephrine was used as an intermittent bolus regimen to treat PSH in patients with severe pre-eclampsia under cesarean section, there was no between-group difference in umbilical arterial pH when compared to equipotent boluses of phenylephrine. The two vasopressors had similar efficacy for maintaining MAP, whereas the overall maternal CO and HR were greater in the norepinephrine group.
Hypotension after spinal anesthesia is primarily due to a decrease in arteriolar dilation and SVR caused by sympathetic nerve blockade.3 A pure α-1 agonist such as phenylephrine is appropriate and recommended, for it directly counteracts this mechanism. Physiological studies have proved that HR and SV increase modestly after the induction of spinal anesthesia as a compensatory mechanism.6 However, patients with pre-eclampsia are in a state of low cardiac output. The use of phenylephrine may further decrease CO.3–5 Transient decreases in CO are accommodated without detrimental effects in healthy women but harming the fetus born to a mother with severe pre-eclampsia.18 Glycopyrrolate pre-treatment before phenylephrine infusion had been studied as a means of increasing HR and CO.19 However, this increases the incidence of dry mouth and hypertension after surgery. The latter is particularly inappropriate in patients with severe pre-eclampsia. Norepinephrine may be a better choice because it provides better CO when maintaining BP. Previous studies comparing norepinephrine and phenylephrine to treat PSH during cesarean section were mainly performed in low-risk, elective cases.8,12–14,20,21 Recently, some studies have focused on pre-eclampsia patients with uteroplacental insufficiency to investigate whether norepinephrine was superior to phenylephrine in terms of umbilical arterial pH, as umbilical arterial pH is a well-established measure of the neonatal condition immediately before delivery and is valuable for assessing uteroplacental perfusion and the impact of vasopressor therapy on the fetus.16,22 Guo et al used prophylactic norepinephrine or phenylephrine infusion for PSH during cesarean section in patients with pre-eclampsia.23 Similarly, a study by Wang et al was published comparing phenylephrine, norepinephrine, and ephedrine to treat PSH in pre-eclamptic patients.24 No difference in umbilical arterial blood gas values was reported between the patients receiving phenylephrine or norepinephrine. The findings of these studies were consistent with ours. Nevertheless, they recruited patients with pre-eclampsia regardless of the severity. As uteroplacental insufficiency is more significant in severely pre-eclamptic patients than those without severe disease,25–27 this group of patients is at particularly high risk. Mohta et al randomized severely pre-eclamptic patients undergoing cesarean section with spinal anesthesia to receive either phenylephrine or norepinephrine boluses and found no differences in umbilical arterial pH.28 However, patients with severe pre-eclampsia in that study were analyzed as a subgroup. There is therefore, insufficient power to detect a difference based on this number of cases. Our study, specifically designed to assess neonates born to mothers with severe pre-eclampsia, did not find a difference in umbilical arterial pH directly compared as a primary outcome between groups. In addition, there were no differences in other umbilical cord blood gas values and Apgar scores. Norepinephrine did not show an advantage in fetuses over phenylephrine in patients with severe pre-eclampsia.
In our study, we found that norepinephrine provided greater HR, CO, and SV than phenylephrine. Activation ofα-adrenergic agonists increases SVR by arteriolar vasoconstriction. At the same time, norepinephrine acts on β1 receptors in the myocardium and exerts positive inotropic and chronotropic effects. The greater SV and HR might be attributed to the inotropic effect and positive chronotropic effect, respectively. The HR in the norepinephrine group was also greater than the baseline value, which might be a direct positive chronotropic effect over a reflex chronotropic effect. The superiority of CO in the norepinephrine group might be obtained from the synergy of HR and SV. However, Ngan Kee et al, while comparing the efficacy of norepinephrine or phenylephrine in maintaining maternal SBP close to baseline, observed that norepinephrine provided greater CO than phenylephrine, mainly derived from greater HR rather than SV.14 One reason most likely contributing to this discrepancy is the different detection methods for hemodynamic parameters. Ngan Kee et al used suprasternal Doppler to track the CO and SV trends, and it is an intermittent measurement. In contrast, the TL-400 monitor applied in our study automatically updated sequential quantitative CO and SV values. Another possible reason is that Ngan Kee et al compared norepinephrine with phenylephrine based on an estimated potency ratio of 20:1, whereas we used a ratio of 13:1. The differences observed may be more of a dose than a drug effect. In another study, Wang et al detected a larger SV in the norepinephrine group, which was attributed to increased myocardial contractility by β-adrenergic action and increased return blood volume by β-adrenergic action on the vessel.29 They also detected that the SVR in the norepinephrine group was smaller. Contrarily, we did not detect a difference in SVR. One probable reason is that women with severe pre-eclampsia react differently to maternal vasopressor administration than other women due to different β2-adrenoceptor density and function.30 Despite the differences, these studies and ours consistently demonstrated that norepinephrine was superior to phenylephrine in maternal CO.
Prophylactic infusion is a recommended paradigm for the management of PSH to minimize hemodynamic fluctuation and maternal complications.5 However, patients with pre-eclampsia have a lower incidence of PSH and increased sensitivity to vasopressors.31 Administration of vasopressor as prophylactic infusion may result in reactive hypertension. Therefore, vasopressors were administered as boluses in our study. Equivalent dosing is essential to ensure that dosing bias does not influence the comparison of clinical efficacy. We adopted a bolus dose of phenylephrine (60 µg) and an estimated equipotent bolus dose of norepinephrine (4.5 µg) to be administered in the present study. The dose of norepinephrine and phenylephrine were chosen based on two studies. Our previous sequential allocation study determined the 90% effective dose (ED90) of phenylephrine to be 62 µg, used as intermittent boluses for treating PSH in patients with severe eclampsia undergoing cesarean section.32 For clinical practice, phenylephrine 60 µg was recommended for both effectiveness and safety. In a dose-response study, Ngan Kee et al determined the relative potency of norepinephrine and phenylephrine when used to rescue PSH during cesarean section in normotensive women is estimated to be nearly 13: 1.8 This potency ratio was obtained in normotensive patients, and we assumed the same ratio for the two drugs in patients with severe pre-eclampsia.
Invasive measurements of CO in parturients using dye or thermal dilution methods have been used over the years. Nevertheless, because of the risks of complications from these invasive methods, there has been much recent interest in non-invasive monitors of the circulation, such as transthoracic echocardiography, suprasternal Doppler, and transthoracic electrical bioimpedance. In the present study, we introduced the non-invasive TL-400 system to assess the hemodynamic parameters (CO, SV, and SVR). TL−400 is based on applanation tonometry.33,34 The arterial pulse wave is obtained by flattening the artery to make the transmural pressure zero, then using a transducer strapped to the artery to measure CO, SV, and SVR continuously.
Hypotension after the induction of spinal anesthesia may cause brainstem hypoxemia and thus trigger the vomiting center to induce emesis. The incidence of nausea and vomiting was comparable between groups in our study. However, the overall incidence was lower than that of healthy parturients undergoing elective cesarean section reported in previous studies. This may be because we enrolled patients with higher basic BP values in our study. The vomiting center would not be triggered even if BP reached the defined hypotension value.35 Another factor that may contribute to reducing the incidence of nausea and vomiting is the absence of intrathecal opioids.36
Patients with pre-eclampsia are at increased risk of pulmonary edema due to increased capillary, decreased colloid oncotic pressure, increased hydrostatic pressure, and, in some cases, left ventricular dysfunction.1 Pulmonary edema is more common in pre-eclampsia and is associated with increased fluid administration and disease severity.37 Accordingly, we adopted a restrictive approach to fluid management.38 None of the patients in our study developed pulmonary edema.
The incidence of hypotension in the present study was approximately 70%. The incident appears high, given that women with pre-eclampsia are known to have less hypotension than healthy women.39 However, compared to previous studies in patients with pre-eclampsia, our definition of hypotension was conservative (20% below baseline), and we used a relatively high dose of ropivacaine (15 mg) for spinal anesthesia.40
We acknowledge several limitations. First, the TL-400 is susceptible to motion artifacts when used. However, even if the absolute values are inaccurate relative to invasive monitors, the relative difference in values between randomized groups is still valid. Second, we did not perform further evaluation of the newborn, such as cerebral functioning monitoring, cranial ultrasound, electroencephalogram, etc., as neonates with similar UA pH may have very different outcomes. Finally, although we detected a difference in overall CO between the two groups in our study, Global measurements of CO do not necessarily represent regional flow in the uterus and placenta.41 Drugs may even affect global and regional blood flow inversely. Whether a global measure of CO is the ideal parameter to base hemodynamic therapy in obstetric patients needs to be proven.
Conclusion
In summary, we conclude that a 60 µg bolus of phenylephrine and a 4.5 µg bolus of norepinephrine showed similar neonatal outcome assessed by umbilical arterial pH and were equally effective when treating PSH for cesarean section in patients with severe pre-eclampsia. Norepinephrine provided a higher maternal CO and a lower incidence of bradycardia.
Abbreviations
PSH, postspinal hypotension; BP, blood pressure; ASA, American Society of Anesthesiologists physical status; LUD, left uterine displacement; MAP, mean arterial pressure; HR, heart rate; CO, cardiac output; SV= hydroxyethyl starch; SVR= systemic vascular resistance.
Article Highlights
● In patients with severe pre-eclampsia, phenylephrine and norepinephrine showed similar umbilical arterial pH for treating of post-spinal hypotension.
● Compared with phenylephrine, norepinephrine provided greater maternal cardiac output and a lower incidence of bradycardia.
Data Sharing Statement
The data that support the findings of the study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine (Hangzhou, China) (Approval No. IRB-20211038-R), registered at the Chinese Clinical Trial Registry (www. chictr.org.cn, registration No. ChiCTR2100047529, principal investigator: Xiao-Wei Qian). Informed written consents were obtained from all subjects.We confirm our study complies with the Declaration of Helsinki.
Consent for Publication
All authors have read and approved the manuscript, and agreed to submit to your journal.
Acknowledgments
Assistance with the study: The authors thank all the colleagues in the Department of Anesthesiology, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Funding
Financial support and sponsorship: none.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Henke VG, Bateman BT, Leffert LR. Focused review: spinal anesthesia in severe preeclampsia. Anesthesia Analg. 2013;117(3):686–693. doi:10.1213/ANE.0b013e31829eeef5
2. Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010;376(9741):631–644. doi:10.1016/S0140-6736(10)60279-6
3. Dyer RA, Reed AR, van Dyk D, et al. Hemodynamic effects of ephedrine, phenylephrine, and the coadministration of phenylephrine with oxytocin during spinal anesthesia for elective cesarean delivery. Anesthesiology. 2009;111(4):753–765. doi:10.1097/ALN.0b013e3181b437e0
4. Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Columb M. The dose-dependent effects of phenylephrine for elective cesarean delivery under spinal anesthesia. Anesthesia Analg. 2010;111(5):1230–1237. doi:10.1213/ANE.0b013e3181f2eae1
5. Kinsella SM, Carvalho B, Dyer RA, et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia. 2018;73(1):71–92. doi:10.1111/anae.14080
6. Langesaeter E, Rosseland LA, Stubhaug A. Continuous invasive blood pressure and cardiac output monitoring during cesarean delivery: a randomized, double-blind comparison of low-dose versus high-dose spinal anesthesia with intravenous phenylephrine or placebo infusion. Anesthesiology. 2008;109(5):856–863. doi:10.1097/ALN.0b013e31818a401f
7. Hasanin AM, Amin SM, Agiza NA, et al. Norepinephrine Infusion for Preventing Postspinal Anesthesia Hypotension during Cesarean Delivery: A Randomized Dose-finding Trial. Anesthesiology. 2019;130(1):55–62. doi:10.1097/ALN.0000000000002483
8. Ngan Kee WD. A Random-allocation Graded Dose-Response Study of Norepinephrine and Phenylephrine for Treating Hypotension during Spinal Anesthesia for Cesarean Delivery. Anesthesiology. 2017;127(6):934–941. doi:10.1097/ALN.0000000000001880
9. Ngan Kee WD. Norepinephrine for maintaining blood pressure during spinal anaesthesia for caesarean section: a 12-month review of individual use. Internat J Obstet Anesth. 2017;30:73–74. doi:10.1016/j.ijoa.2017.01.004
10. Ngan Kee WD, Lee SWY, Ng FF, Khaw KS. Prophylactic Norepinephrine Infusion for Preventing Hypotension During Spinal Anesthesia for Cesarean Delivery. Anesthesia Analg. 2018;126(6):1989–1994.
11. Onwochei DN, Ngan Kee WD, Fung L, Downey K, Ye XY, Carvalho JCA. Norepinephrine Intermittent Intravenous Boluses to Prevent Hypotension During Spinal Anesthesia for Cesarean Delivery: A Sequential Allocation Dose-Finding Study. Anesthesia Analg. 2017;125(1):212–218. doi:10.1213/ANE.0000000000001846
12. Sharkey AM, Siddiqui N, Downey K, Ye XY, Guevara J, Carvalho JCA. Comparison of Intermittent Intravenous Boluses of Phenylephrine and Norepinephrine to Prevent and Treat Spinal-Induced Hypotension in Cesarean Deliveries: Randomized Controlled Trial. Anesthesia Analg. 2019;129(5):1312–1318. doi:10.1213/ANE.0000000000003704
13. Mohta M, Dubey M, Malhotra RK, Tyagi A. Comparison of the potency of phenylephrine and norepinephrine bolus doses used to treat post-spinal hypotension during elective caesarean section. Internat J Obstet Anesth. 2019;38:25–31. doi:10.1016/j.ijoa.2018.12.002
14. Ngan Kee WD, Lee SW, Ng FF, Tan PE, Khaw KS. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology. 2015;122(4):736–745. doi:10.1097/ALN.0000000000000601
15. Singh PM, Singh NP, Reschke M, Ngan Kee WD, Palanisamy A, Monks DT. Vasopressor drugs for the prevention and treatment of hypotension during neuraxial anaesthesia for Caesarean delivery: a Bayesian network meta-analysis of fetal and maternal outcomes. Br J Anaesth. 2020;124(3):e95–e107. doi:10.1016/j.bja.2019.09.045
16. Ngan Kee WD, Lee SWY, Ng FF, Lee A. Norepinephrine or phenylephrine during spinal anaesthesia for Caesarean delivery: a randomised double-blind pragmatic non-inferiority study of neonatal outcome. Br J Anaesth. 2020;125(4):588–595. doi:10.1016/j.bja.2020.05.057
17. Matthews JN, Altman DG, Campbell MJ, Royston P. Analysis of serial measurements in medical research. BMJ. 1990;300(6719):230–235. doi:10.1136/bmj.300.6719.230
18. Tihtonen K, Koobi T, Yli-Hankala A, Huhtala H, Uotila J. Maternal haemodynamics in pre-eclampsia compared with normal pregnancy during caesarean delivery. BJOG. 2006;113(6):657–663. doi:10.1111/j.1471-0528.2006.00931.x
19. Ngan Kee WD, Lee SW, Khaw KS, Ng FF. Haemodynamic effects of glycopyrrolate pre-treatment before phenylephrine infusion during spinal anaesthesia for caesarean delivery. Internat J Obstet Anesth. 2013;22(3):179–187. doi:10.1016/j.ijoa.2013.03.008
20. Vallejo MC, Attaallah AF, Elzamzamy OM, et al. An open-label randomized controlled clinical trial for comparison of continuous phenylephrine versus norepinephrine infusion in prevention of spinal hypotension during cesarean delivery. Internat J Obstet Anesth. 2017;29:18–25. doi:10.1016/j.ijoa.2016.08.005
21. Hasanin A, Amin S, Refaat S, et al. Norepinephrine versus phenylephrine infusion for prophylaxis against post-spinal anaesthesia hypotension during elective caesarean delivery: A randomised controlled trial. Anaesth Crit Care Pain Med. 2019;38(6):601–607. doi:10.1016/j.accpm.2019.03.005
22. Johnson JW, Richards DS, Wagaman RA. The case for routine umbilical blood acid-base studies at delivery. Am J Clin Exp Obstet Gynecol. 1990;162(3):621–625. doi:10.1016/0002-9378(90)90970-I
23. Guo L, Qin R, Ren X, et al. Prophylactic norepinephrine or phenylephrine infusion for bradycardia and post-spinal anaesthesia hypotension in patients with preeclampsia during Caesarean delivery: a randomised controlled trial. Br J Anaesth. 2022;128(5):e305–e307. doi:10.1016/j.bja.2022.01.027
24. Wang X, Mao M, Liu S, Xu S, Yang J. A Comparative Study of Bolus Norepinephrine, Phenylephrine, and Ephedrine for the Treatment of Maternal Hypotension in Parturients with Preeclampsia During Cesarean Delivery Under Spinal Anesthesia. Med Sci Monit. 2019;25:1093–1101. doi:10.12659/MSM.914143
25. Maynard SE, Karumanchi SA. Angiogenic factors and preeclampsia. Semin Nephrol. 2011;31(1):33–46. doi:10.1016/j.semnephrol.2010.10.004
26. Phipps EA, Thadhani R, Benzing T, Karumanchi SA. Pre-eclampsia: pathogenesis, novel diagnostics and therapies. Nat Rev Nephrol. 2019;15(5):275–289. doi:10.1038/s41581-019-0119-6
27. Lunell NO, Nylund LE, Lewander R, Sarby B. Uteroplacental blood flow in pre-eclampsia measurements with indium-113m and a computer-linked gamma camera. Clin Exp Hypertens B. 1982;1(1):105–117. doi:10.3109/10641958209037184
28. Mohta M, L R, Chilkoti GT, Agarwal R, Malhotra RK. A randomised double-blind comparison of phenylephrine and norepinephrine for the management of postspinal hypotension in pre-eclamptic patients undergoing caesarean section. Eur J Anaesthesiol. 2021;38(10):1077–1084. doi:10.1097/EJA.0000000000001461
29. Wang X, Mao M, Zhang SS, Wang ZH, Xu SQ, Shen XF. Bolus norepinephrine and phenylephrine for maternal hypotension during elective cesarean section with spinal anesthesia: a randomized, double-blinded study. Chin Med J. 2020;133(5):509–516. doi:10.1097/CM9.0000000000000621
30. Landau R, Dishy V, Wood AJ, Stein CM, Smiley RM. Disproportionate decrease in alpha- compared with beta-adrenergic sensitivity in the dorsal hand vein in pregnancy favors vasodilation. Circulation. 2002;106(9):1116–1120. doi:10.1161/01.CIR.0000028334.32833.B0
31. Aya AGM, Vialles N, Tanoubi I, et al. Spinal anesthesia-induced hypotension: a risk comparison between patients with severe preeclampsia and healthy women undergoing preterm cesarean delivery. Anesthesia Analg. 2005;101(3):869–875. doi:10.1213/01.ANE.0000175229.98493.2B
32. Liu JP, Pan ZB, Zhu M, et al. Determination of the 90% Effective Dose of Phenylephrine Boluses to Treat Spinal Anesthesia-Induced Hypotension in Patients with Severe Preeclampsia during Cesarean Delivery: A Pilot Study. Drug Des Devel Ther. 2021;15:3765–3772. doi:10.2147/DDDT.S323715
33. Saugel B, Meidert AS, Langwieser N, et al. An autocalibrating algorithm for non-invasive cardiac output determination based on the analysis of an arterial pressure waveform recorded with radial artery applanation tonometry: a proof of concept pilot analysis. J Clinl Monit Comput. 2013;28(4):357–362. doi:10.1007/s10877-013-9540-8
34. Li M, Ding J, Peng M. A Prospective Comparison of TL-400 and NICOM for Goal-Directed Fluid Therapy in Gastrointestinal Tumors Surgery; 2021.
35. Fujii Y, Saitoh Y, Tanaka H, Toyooka H. Granisetron/dexamethasone combination for reducing nausea and vomiting during and after spinal anesthesia for cesarean section. Anesthesia Analg. 1999;88(6):1346–1350. doi:10.1097/00000539-199906000-00028
36. Dahl JB, Jeppesen IS, Jørgensen H, et al. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing Cesarean section with spinal anesthesia. J Am Soc Anesthesiologists. 1999;91(6):1919.
37. Dennis AT, Solnordal CB. Acute pulmonary oedema in pregnant women. Anaesthesia. 2012;67(6):646–659. doi:10.1111/j.1365-2044.2012.07055.x
38. Pretorius T, van Rensburg G, Dyer RA, Biccard BM. The influence of fluid management on outcomes in preeclampsia: a systematic review and meta-analysis. Internat J Obstet Anesth. 2018;34:85–95. doi:10.1016/j.ijoa.2017.12.004
39. Aya AGM, Mangin R, Vialles N, et al. Patients with severe preeclampsia experience less hypotension during spinal anesthesia for elective cesarean delivery than healthy parturients: a prospective cohort comparison. Anesthesia Analg. 2003;97(3):867–872. doi:10.1213/01.ANE.0000073610.23885.F2
40. Mei Z, Ngan Kee WD, Sheng Z-M, et al. Comparative dose-response study of hyperbaric ropivacaine for spinal anesthesia for cesarean delivery in singleton versus twin pregnancies. J Clin Anesth. 2020;2020:67.
41. Thiele RH, Nemergut EC, Lynch C. The Physiologic Implications of Isolated Alpha1 Adrenergic Stimulation. Anesthesia Analg. 2011;113(2):284–296. doi:10.1213/ANE.0b013e3182124c0e
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.