")
Back to Journals » Clinical Audit » Volume 14
Quality Improvements in Timeliness to Antibiotics in Solid Organ Malignancy Patients Admitted with Febrile Neutropenia and Neutropenic Sepsis Through the Establishment of an Acute Medical Unit
Authors Ong YJ, Sikotra N, Prunster J, Bailey N, Hadfield J, Smith R, Skiba R, Arellano A, Gabbay E, Clay TD
Received 28 July 2021
Accepted for publication 17 November 2021
Published 11 January 2022 Volume 2022:14 Pages 1—8
DOI https://doi.org/10.2147/CA.S330869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zoka Milan
Yang Jian Ong,1– 3 Nisha Sikotra,1,4 Janelle Prunster,1,2 Nicola Bailey,2 Jane Hadfield,2 Rosemary Smith,2 Rohen Skiba,2 Astrid Arellano,5 Eli Gabbay,1– 3,6 Timothy D Clay1,7,8
1Bendat Respiratory Research and Development Group, St John of God Healthcare, Subiaco, Western Australia, Australia; 2Department of Medical Teaching, St John of God Healthcare, Subiaco, Western Australia, Australia; 3The University of Notre Dame, Fremantle, Western Australia, Australia; 4Research Department, St John of God Healthcare, Subiaco, Western Australia, Australia; 5Department of Infectious Diseases, St John of God Healthcare, Subiaco, Western Australia, Australia; 6Department of Respiratory Medicine, St John of God Healthcare, Subiaco, Western Australia, Australia; 7Department of Medical Oncology, St John of God Healthcare, Subiaco, Western Australia, Australia; 8School of Medical and Health Sciences, Edith Cowan University Joondalup, Joondalup, Western Australia, Australia
Correspondence: Nisha Sikotra Tel +61 08 9382 9172
Email [email protected]
Background: Febrile neutropenia (FN) is a medical emergency that requires prompt empirical antibiotic treatment. Logistical factors can hamper the timely delivery of antibiotics for patients with suspected FN.
Aim: To determine our institution’s adherence to timeliness of antibiotic administration after the implementation of strategies following a previous audit.
Methods: Two retrospective audits were performed. Patients were identified through hospital coding and data were extracted from medical records. Interventions following the first audit included targeted staff education; development of a “Febrile Neutropenia Box” and the establishment of an acute medical unit (AMU). Adherence to guidelines and the effect of interventions were compared.
Results: Audit one: 72 admissions (January 2017–December 2017); audit two: 55 admissions (October 2018–October 2019). Median time to antibiotics and adherence to 60-minute administration target: audit one: 135 minutes (range 15– 5160; 11% adherence); audit two: 80 minutes (range 0– 2130; 45% adherence, P=< 0.001). In audit two, the admission ward was the major factor that reduced time to treatment – AMU: 43 minutes (range 0– 440; 70% adherence); oncology ward: 98 minutes (range 0– 2130; 40% adherence); other wards: 190 minutes (range 0– 750; 27% adherence) (p=0.028 for adherence).
Conclusion: A gap in our routine care of FN was identified. We assessed the effects of several interventions. The most important intervention was the introduction of the AMU which allowed sufficient resources to address time critical tasks. Health institutions without an emergency department should consider similar pathways to ensure timely care for patients with FN. Auditing current practice and evaluating interventions are important.
Keywords: febrile neutropenia, quality improvement, complications of cancer, clinical practice guidelines, FN
Introduction
Febrile neutropenia (FN) is a known cytotoxic chemotherapy-related complication occurring in 10–50% of patients with solid organ malignancies.1,2 FN results in unplanned hospital admissions and deviations from cancer treatment protocols, which may have effects on the efficacy of therapy, particularly in the curative treatment setting. Further, FN is associated with significant morbidity and in-hospital mortality rate of 9.5%.3,4 Thus, early clinical recognition is crucial to ensure implementation of immediate management. As per guidelines, all patients with fever following chemotherapy should be managed as a FN patient and receive empirical antibiotics in a timely manner (within 60 minutes of initial presentation or 30 minutes in the setting of haemodynamic instability) without awaiting laboratory confirmation of the neutrophil count.5,6
However, the timeliness in delivering treatment for suspected FN patients remains a major issue in many institutions that care for patients with malignancy. Previous studies, including our own, showed a range from 9–26% of patients receiving empiric antibiotics within 60 minutes of initial presentation.7–9 Our initial clinical audit of 72 admissions showed a prolonged median time to antibiotics administration to febrile neutropenic patients at 135 minutes, which is beyond the recommended time. We identified potential barriers to timely treatment which included: delayed assessment by nursing and junior medical staff, lack of awareness about the importance of FN and failure to have appropriate antibiotic therapy readily available in a timely manner.7,8 At the time of our first study, our hospital did not include a dedicated Acute Medical Unit (AMU) nor an emergency department. Patients were admitted directly to an inpatient ward after liaison with their treating oncologist. Following the initial audit, specific strategies have been implemented which included: establishment of an AMU to streamline FN admissions, a FN pathway, a “febrile neutropenia box” containing a flow chart of immediate patient management and a stock of appropriate antibiotics available on AMU and the oncology ward, simplification of FN alert card and redesign of patient education.
The aim of this study was to determine our institution’s adherence to timeliness of antibiotic administration after the implementation of these strategies by comparing results from the previous audit to results of this current audit.
Methods
This study was approved by the St John of God Human Research Ethics committee; approval number #1570. Privacy and data protection guidelines were adhered to. The initial retrospective clinical audit (pre-intervention audit) consisted of patients admitted between January 2017 and December 2017. Eligible patients were identified by searching the hospitals coding systems for the International Classification of Disease–Clinical Modification (ICD-CM) code D70.1 (Agranulocytosis secondary to cancer chemotherapy) and screened for eligibility. Inclusion criteria were: patients with a diagnosis of solid organ malignancy treated by chemotherapy that was causative of or contributed to neutropenia (granulocyte count <0.5×10^9 cells/L or is expected to decrease to <0.5×10^9 cells/L over the next 48 hours), temperature greater than 38C (documented by the patient or medical/nursing staff), and age greater than or equal to 18 years.8 Cases were excluded if admission was primarily related to reasons other than neutropenic fever or if patient management during admission may have been impacted by an alternative diagnosis. Data were extracted from the hospital medical records and included; patient demographics (Table 1), time to antibiotic, name of antibiotic used, duration of antibiotics, clinical parameters and in-hospital mortality. Time to antibiotic was calculated from documented time of nursing admission of patient. Quantitative data such as positive culture results were also collected.
 |
Table 1 Pre- and Post-Intervention Patient Characteristics and Admission Data |
Following the pre-intervention audit, potential reasons for a prolonged time-to-antibiotic administration were identified with implementation of the following strategies:
- Establishment of an AMU to streamline the FN pathway,
- Placement of a “Febrile neutropenia box” containing a FN protocol, and a stock of appropriate antibiotics in the AMU and oncology ward,
- Simplification of FN alert card and redesign of patient education.
Another retrospective clinical audit was conducted between October 2018 and October 2019 after the aforementioned strategies had been implemented. To allow comparisons between both clinical audits, the post-intervention clinical audit was conducted with identical inclusion and exclusion criteria to the pre-intervention clinical audit. All patients who were admitted directly to the study hospital for FN during the post-intervention audit period were included (Figure 1).
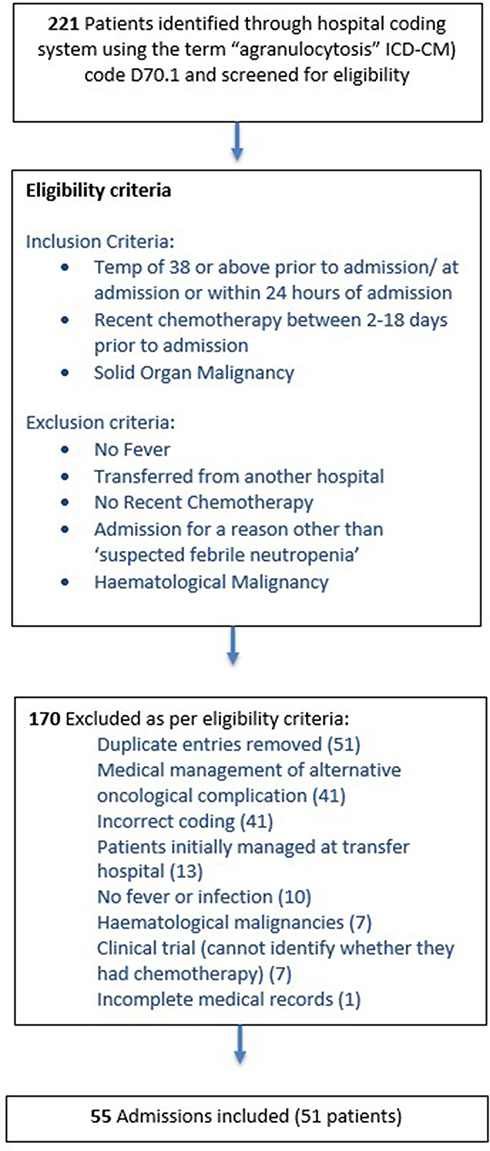 |
Figure 1 Sample selection. |
Descriptive statistics were used for both pre- and post-intervention clinical audit to analyse the data using Microsoft Excel 2016 and data analysis software “R” (R Core Team, 2014). Mean, median and ranges were calculated, and results for both clinical audit periods were compared. Results are reported with standard deviation or range as outlined in the relevant table. Independent t-tests were used to compare statistical significance between groups or Χ2 tests where there were three groups analysed. Minutes to antibiotics and length of stay have been analysed using a linear regression models. Antibiotics delivered within 1 hour has been analysed using a logistic regression model.
Results
Sixty-seven patients with 72 admissions were included in the pre-intervention cohort. The median age of patients in the pre-intervention audit was 66 years (32–83 years) and 69% of the majority of patients were female. Breast and colorectal cancers were the most cancer diagnosis of admitted patients. This current post-intervention audit consisted of patients admitted between October 2018 and October 2019. 221 admissions were identified through the hospital coding system coded as “Agranulocytosis”, 166 were excluded and 55 admissions were eligible as per the inclusion and exclusion criteria (Figure 1). Fifty-one patients were admitted during the study period across 55 admissions. Seventy-five per cent of patients had metastatic disease. Pancreatic (27%) and Gynaecological (27%) cancer were the most common cancer type (Table 1).
In the post-intervention audit, the median body temperature of patients at admission was 38.3°C. Patients had received chemotherapy at a median of 8 days prior to their admission. During admission, the median nadir neutrophil count was 0.4×10^9 /L (<0.1–0.8×10^9 /L). Forty-nine per cent received rescue Granulocyte-Colony Stimulating Factor (G-CSF). A septic screen including blood cultures and urine samples were completed on 73% of admissions. Positive cultures were identified in 15% of patients (Table 1). Table 2 shows the antibiotic administration times for both audits. In the post-intervention audit, the median time to administration of parenteral antibiotics was 80 minutes (range 0 to 2130 minutes), compared to pre-intervention audit which was 135 minutes (range 15 to 5160 minutes). Forty-five per cent of patients received their antibiotics within 1 hour of admission in post-intervention compared to pre-intervention which was 11% (Table 2). In post-intervention audit, empirical antibiotic therapy was administered in 97% of patients and continued for an average of five days (Table 2). The median length of stay was 5 days (2–50 days). Patients who received their antibiotics within 60 mins were discharged at a significantly earlier time at an average of 4 days (2–16 days) compared to patients who received their antibiotics greater than 60 minutes post admission at 5.5 days (1–50 days; p=0.028).
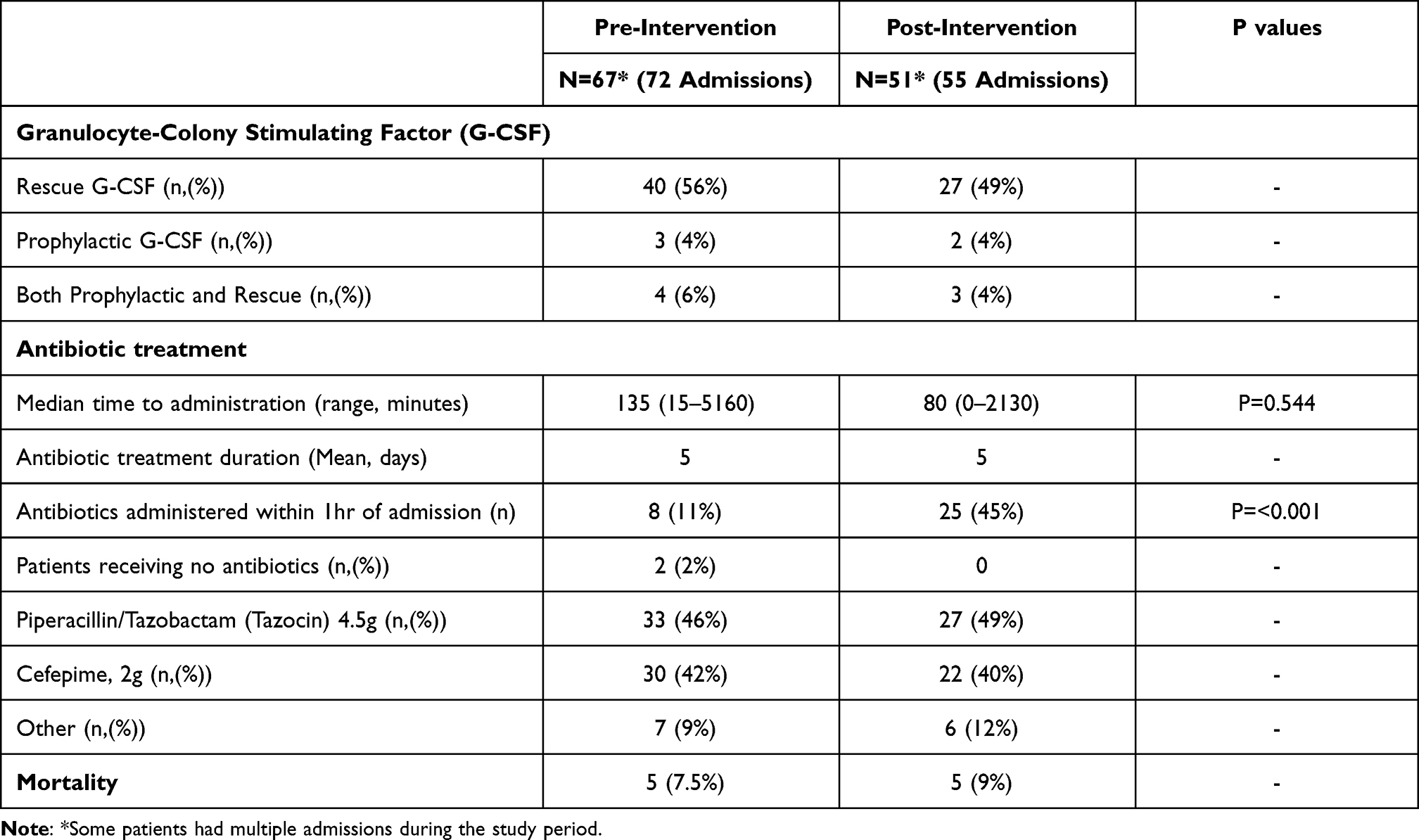 |
Table 2 Pre and Post Intervention Treatment and Outcomes |
The timeliness of antibiotic therapy in this cohort had improved compared to the first study prior period, but still fell well short of an acceptable level. We noted an apparent difference between the location of admission and the timeliness of antibiotic therapy and hypothesised that this difference may be significant (Table 3). As such a post-hoc analysis was performed on this basis. Patients admitted via the AMU received antibiotics sooner (median 43 minutes [0–440 mins]) compared to patients admitted to the specialist oncological ward (median 98 minutes [0–2130 mins]) and patients admitted to any other ward (median 190 minutes [0–750 mins]) (Table 3). All patients admitted via AMU received piperacillin/tazobactam or cefepime as per guidelines. On the other wards, one patient received cefazolin and two patients received metronidazole (one was due to a sulphur allergy). Median length of stay for patients in AMU was 4 days (2–38 days) compared to the oncological ward which was 6.5 days (2–50 days) and other wards, where length of stay was 5 days (2–34 days) (Table 2).
 |
Table 3 Comparison of Clinical Data by Admission Ward (N=Admission) |
Five patients died during their admission for FN (in hospital mortality 9.1%). The cause of death for these patients were disease progression: recurrent bowel obstruction and AKI (2 patients), multi-organ failure (2 patients) and neutropenic sepsis (1 patient).
Discussion
FN is a life-threatening complication of cancer treatment. Its management requires early recognition of the potential for this diagnosis, urgent patient assessment and treatment including administration of antibiotics within thirty minutes of presentation for unstable patients and one hour of presentation for all others.10 Although simple in principle, achieving high levels of compliance with early antibiotic administration can be challenging. In a prior audit at our centre, we identified poor adherence to time-to-treatment targets as described in FN guidelines.8
We have reaudited outcomes following several interventions where we found an improvement in timeliness of antibiotic delivery. Nonetheless, the rate of patients receiving antibiotics within 60 minutes was still low at 45%. Sub-analysis of post-intervention individual admission wards showed that 70% of patients admitted to the AMU received antibiotics within 60 minutes of presentation, with median time of 43 minutes. For patients admitted directly to the Oncology Ward the rate was 40% and with direct admission to any other ward this rate fell to 7%. It is possible that these improved rates seen on AMU and the oncological ward are due to the availability of the “febrile neutropenia box.” The box contains; two vials of Piperacillin 4g/Tazobactam 500mg, two vials of Cefepime 2g, Pathology Request Form bloods: FBP, UEC, LFT, CRP, Blood Cultures (centrally and peripherally), Pathology Request Form: Urine- Mc & S, copies of the “Nursing Policy - Management of Known or Suspected Neutropenic Fever or Sepsis” and “Pharmacy guideline-Neutropenic Fever and Sepsis Empiric Antibiotic Therapy Guideline” and a Febrile Neutropenia Admission Pathway. This was placed in AMU and the Oncology Ward following the first audit.
A further potential reason for improved timeliness to antibiotics in AMU is the availability of dedicated nursing staff and increased resources for the management of FN. Our results mirror those seen in a study of patients presenting to an emergency department where a dedicated management pathway significantly improved time to antibiotic therapy.11 Having a streamlined FN management and protocol helped to mitigate historical factors contributing to delay in antibiotics. This study also found that patients who bypassed Emergency Department (directly admitted patients) had a significant delay to antibiotic therapy, possibly due to multiple concomitant admissions with overall low nurse to patient ratio in wards as well as the non-availability of resources required for urgent management.11 In another study the use of an acute oncology service with well-trained staff and lower workload to staff ratios compared to Emergency Department this resulted in timelier management of FN patients.12
The rate of in-hospital mortality was 7.5% for the pre-intervention cohort and 9% for the post-intervention cohort respectively. These rates were consistent with other studies.3,13 Kuderer et al published results from a longitudinal database study of more than 40,000 adult cancer patients who were hospitalised in the United States with neutropenic fever identifying an in-hospital mortality of 9.5%.3 In 2008, an epidemiological study by Lingaratnam et al identified a mortality of 7.6% in Australian patients with solid organ malignancy with FN.13 Our study population was small and thus lacked the available sample size to demonstrate an impact on mortality outcomes. The importance of timely antibiotic administration on survival outcomes has been demonstrated in a larger study performed by Rosa et al, where patients with time-to-antibiotics of ≤ 30 minutes had lower mortality rates than patients with a time-to-antibiotics of between 31–60 minutes (6.4% vs. 27.2%; log-rank P= 0.020).4
We noted that patient length of stay in the post-intervention group was significantly decreased for patients who received antibiotics within 60 minutes. In particular, patients admitted to AMU had lower length of stay compared to other wards which we believe may have been positively impacted by the higher rate of time-to-antibiotics adherence. Similar correlations between length of stay and time-to-antibiotics have been shown by by Keng et al. They observed reduced length of stay (3.3 vs. 5.6 days, p ≤ 0.001) in a cohort of patients who were admitted through an Emergency Department with median time to antibiotics of 82 minutes (32% adherence to 60 minutes), compared to the direct admission patient cohort with median time to antibiotics of 169 minutes (13% adherence to 60 minutes).11 This paper and ours suggest that timeliness to antibiotics may have important implications with respect to healthcare resource utilisation.
The use of rescue G-CSF has been shown to reduce the time of neutrophil recovery and shorten the duration of hospitalisation but it does not improve mortality outcomes.14 The rates of both rescue and prophylactic G-CSF administration in managing and preventing neutropenia has not statistically changed in both pre- and post-intervention cohorts. The use of rescue G-CSF was at the discretion of clinicians.
Our retrospective study has several limitations. Firstly, the study was reliant on clinical annotation of admission times and antibiotic administration as per the medical records, rather than prospective collection. Secondly, to capture a representative group we have audited patients with subsequently confirmed FN. The total patient group presenting with febrile illnesses is larger and will include patients who required initial management on suspicion of FN given that this diagnosis is only confirmed after initial management is complete.
Despite these limitations, we believe that there are three key messages from this study. The first is the importance of having a dedicated area and adequate resources such as staffing levels and readily available antibiotics for completion of time critical tasks. In the case of our institution, the opening of an AMU allowed for improved management of FN. The second is the importance of auditing routine clinical care as a means of quality assurance and identifying areas of care that require improvement. Finally, it is important to re-audit implemented changes in clinical practice to ensure that significant improvements in pre-determined outcome measures have occurred as a result of the changes.
Conclusion
After identifying a gap in our routine care, we were able to improve timeliness of antibiotics given to patients presenting with FN through re-auditing after the initial audit. The introduction of an AMU was the most important intervention at our centre. The AMU allowed sufficient resources to address time critical tasks. Health institutions, particularly those without an emergency department, should consider similar pathways to ensure timely care for patients with FN. This study also reiterated the importance of auditing routine clinical care and implementing changes to improve practice. Finally, this study demonstrated the importance of re auditing to evaluate the effectiveness of interventions implemented to determine if improvements have occurred as a result of the changes.
Acknowledgments
We would like to acknowledge Mr Jack Bendat for his support through the Bendat Respiratory Research and Development Fund. We would like to thank Dr Sophia Connor for her assistance with data analysis. We would also like to thank Dino Cercarelli (research manager) and Karen Burn and her team (Patient Health Information Services), Nurse Managers and staff of ward 35, 72, AMU and Dr Eva Denholm (Director of Medical Services) for their support with the study.
Disclosure
All authors declare they have no conflicts of interest to report.
References
1. Klastersky J. Management of fever in neutropenic patients with different risks of complications. Clin Infect Dis. 2004;39(Suppl 1):S32–S37. doi:10.1086/383050
2. Fry WA, Phillips JL, Menck HR. Ten‐year survey of lung cancer treatment and survival in hospitals in the United States: a national cancer data base report. Cancer. 1999;86:1867–1876. doi:10.1002/(SICI)1097-0142(19991101)86:9<1867::AID-CNCR31>3.0.CO;2-9
3. Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH. Mortality, morbidity, and cost associated with neutropenic fever in adult cancer patients. Cancer. 2006;106:2258–2266. doi:10.1002/cncr.21847
4. Rosa RG, Goldani LZ. Cohort study of the impact of time to antibiotic administration on mortality in patients with febrile neutropenia. Antimicrob Agents Chemother. 2014;58(7):3799–3803. doi:10.1128/AAC.02561-14
5. Tam CS, O’reilly M, Andresen D, et al. Use of empiric antimicrobial therapy in neutropenic fever. Intern Med J. 2011;41:90–101. doi:10.1111/j.1445-5994.2010.02340.x
6. Cancer Institute NSW. Immediate management of neutropenic fever. eviQ Cancer TreatmentsOnline; [cited February 21, 2019].Available from: https://www.eviq.org.au/clinical-resources/oncological-emergencies/123-immediatemanagement-of-neutropenic-fever#.
7. Perron T, Emara M, Ahmed S. Time to antibiotics and outcomes in cancer patients with neutropenic fever. BMC Health Serv Res. 2014;14:162. doi:10.1186/1472-6963-14-162
8. Skiba R, Sikotra N, Ball T. Management of neutropenic fever in a private hospital oncology unit. Intern Med J. 2020;50:959–964. doi:10.1111/imj.14464
9. Clarke R, Warnick J, Stretton K, Littlewood T. Improving the immediate management of neutropenic sepsis in the UK: lessons from a national audit. BJHaem. 2011;153:773–779. doi:10.1111/j.1365-2141.2011.08693.x
10. Zimmer A, Freifeld A. Optimal management of neutropenic fever in patients with cancer. J Oncol Pract. 2019;1:19–24. doi:10.1200/JOP.18.00269
11. Keng MK, Thallner EA, Elson P, et al. Reducing time to antibiotic administration for febrile neutropenia in the emergency department. J Oncol Pract. 2015;11(6):450–455. doi:10.1200/JOP.2014.002733
12. Sammut SJ, Mazhar D. Management of febrile neutropenia in an acute oncology service. QJM Int J Med. 2012;105(4):327–336. doi:10.1093/qjmed/hcr217
13. Lingaratnam S, Thursky KA, Slavin MA, Kirsa SW, Bennett CA, Worth LJ. The disease and economic burden of neutropenic fever in adult patients in Australian cancer treatment centres 2008: analysis of the Victorian admitted episodes dataset. Intern Med J. 2011;41:121–129. doi:10.1111/j.1445-5994.2010.02343.x
14. Mhaskar R, Clark OA, Lyman G, Botrel TE, Paladini LM, Djulbegovic B. Colony‐stimulating factors for chemotherapy‐induced neutropenic fever. Cochrane Database Syst Rev. 2014:CD003039. doi:10.1002/14651858.CD003039.pub2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.