")
Back to Journals » International Medical Case Reports Journal » Volume 17
Primary Intra-Orbital Hydatid Cyst: A Case Report of a Rare Cause of Exophthalmos
Authors Debela AS, Abore KW , Worke AB, Wendimagegn ST
Received 12 December 2023
Accepted for publication 1 February 2024
Published 5 February 2024 Volume 2024:17 Pages 89—92
DOI https://doi.org/10.2147/IMCRJ.S454518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Asrat Sime Debela,1 Kibruyisfaw Weldeab Abore,1 Alemayehu Bedane Worke,2 Selamawit Tadesse Wendimagegn3
1Department of Ophthalmology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Radiology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Department of Pathology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Kibruyisfaw Weldeab Abore, Department of Ophthalmology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, Email [email protected]
Background: Hydatid disease is a tapeworm parasitic infection caused by Echinococcus granulosus that commonly affects the liver and lungs during its life cycle in the human body. Orbital involvement is a very rare occurrence and isolated orbital Echinococcosis is extremely rare.
Case Presentation: A 60-year-old female Eritrean woman presented with 3-month history of painless protrusion of the left eye. Physical examination showed significantly decreased visual acuity of the left eye, left eye proptosis, and papilledema. Laboratory investigations were normal and orbital CT scan examination was suggestive of orbital hydatid cyst. After giving two weeks course of oral Albendazole, anterior orbitotomy and cyst excision was done. Post-op biopsy was conclusive of orbital hydatid cyst. She had mild lid swelling and adduction deficit on her post-operative follow-up. Subsequent longer duration of follow-up of the patient was not possible since the patient relocated back to Eritrea.
Conclusion: Orbital hydatid cyst is an extremely rare presentation of human Echinococcus granulosus infection. However, it should be considered one of the differential diagnoses among patients living in an endemic area and presenting with proptosis of the eye. A preoperative course of anthelmintic followed by surgical excision of the cyst is the definitive management.
Keywords: hydatid cyst, hydatid disease, orbit, Echinococcosis, Ethiopia
Background
Hydatid cyst is a zoonotic infection caused by the tapeworm Echinococcus granulosus.1 It is endemic to Africa, Asia, Australia, and Mediterranean countries.2 Dogs are the definitive hosts for the parasite while sheep and cattle serve as intermediate hosts.3 Humans are accidental intermediate hosts affected by the tapeworm after ingesting viable eggs. During its life cycle in the human body, the tapeworm commonly affects the liver and lungs.4 Rarely, echinococcosis may involve the orbit and patients may present with proptosis, decreased vision, and ocular pain.2,4–6 Here, we present a case of a 60-year-old woman who presented with left eye proptosis secondary to a primary orbital hydatid cyst. To the best of the author’s knowledge, this is the first reported case of orbital hydatid disease from Ethiopia.
Case Presentation
A 60-year-old female sheep herder from Eritrea presented to St. Paul’s Hospital Millennium Medical College ophthalmology department with a 3-month history of painless left eye protrusion associated with progressive decreased vision of the left eye. Otherwise, she had an unremarkable history. Visual acuity in the right eye was 6/18 and counting finger in front of the eye on the left eye. Physical examination revealed a 4 mm discrepancy on exophthalmometry between the two eyes with a proptosis of 21 mm on the left eye. On fundus examination, there was a tortuous temporal arcade and grade 4 papilledema in the left eye. Otherwise, there was an unremarkable finding. Laboratory investigation revealed a normal complete blood count. Computerized tomography (CT) of the brain and orbit showed a well-defined thin-walled non-enhancing fluid density cystic mass in the left orbital cavity measuring 2.6 cm by 2.0 cm by 1.9 cm with compression and lateral displacement of the globe as well as compression and stretching of the optic nerve (Figure 1A–C). The left medial rectus muscle was not clearly and separately visualized from the lesion. There were no osseous lytic or sclerotic changes of the bony orbit. The CT scan was suggestive of a hydatid cyst of the orbit. Abdominal ultrasound and chest X-ray findings were unremarkable.
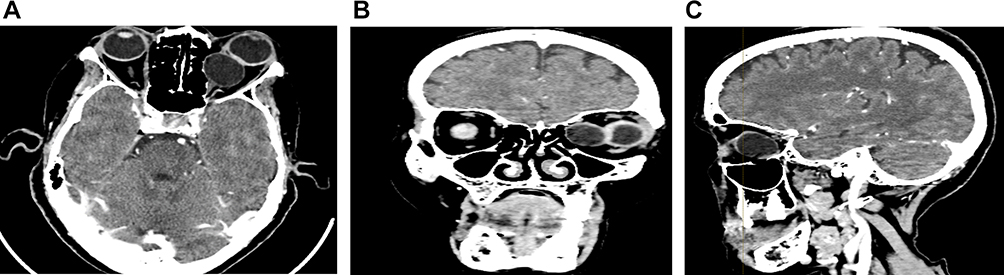 |
Figure 1 Computerized tomography (CT) of the brain and orbit with (A) Axial view, (B) Coronal view, and (C) Sagittal view respectively. |
The patient was given albendazole 400mg orally twice per day for 2 weeks and re-evaluated. Subsequently, she was taken to the operating room with an impression of a left medial mass secondary to Hydatid cyst. The cyst was approached through a medial anterior orbitotomy. Intraoperatively, a cystic mass attached to the inferior aspect of the medial rectus (MR) was identified. The cyst ruptured during manipulation and a clear fluid came out. A paper white cyst lining was removed in piecemeal and the external capsule was excised with care not to severely damage the MR muscle. Then, the surgical field was irrigated with 3% hydrogen peroxide solution followed by copious normal saline solution, and the tissue was sent for histopathological examination. Biopsy result revealed an acellular laminated membrane with germinal epithelium and a daughter cyst with protoscolices (Figure 2A and B) and surrounding soft tissue consisting of chronic inflammatory cells confirming the diagnosis of hydatid cyst. Cytology from cyst fluid showed a hemorrhagic background with no cells.
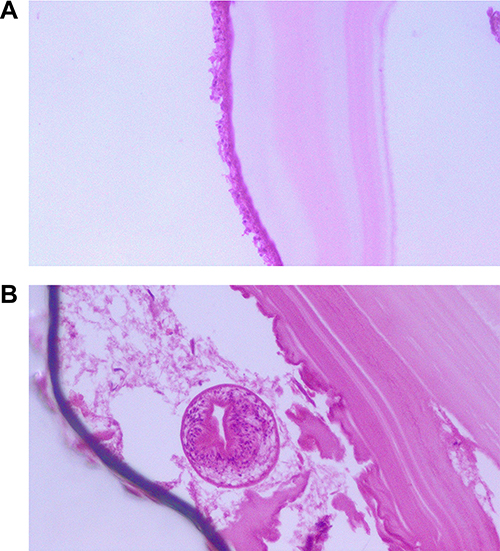 |
Figure 2 A slide showing acellular laminated membrane with germinal epithelium (A) and a daughter cyst with protoscolices (B). |
On her first postoperative day, she had lid edema with limited adduction of the left eye and mild ocular pain. Oral albendazole 400mg twice daily was continued postoperatively. Follow-up on her 7th post-operative day showed that there was mild improvement in the adduction deficit and lid swelling had resolved. Subsequent follow-up on her 21st postoperative day showed left eye visual acuity of counting fingers at two meters and the adduction deficit improved to −2. Furthermore, the optic disc edema also resolved to grade 1. However, the patient moved back to Eritrea, and we were not able to follow the subsequent progress of the patient beyond the first 3 weeks.
Discussion
Orbital hydatid disease is a very rare parasitic infection caused by the tapeworm Echinococcus granulosus.7 Similar to other zoonotic disease affecting humans, accidental ingestion of ova passed by the definitive hosts, canines, is the route of entry to the human body.8,9 Hydatid disease mainly affects the liver and the lung but it can rarely affect other organs including the orbit and the central nervous system.7,10 Previous studies have shown that orbital hydatid disease accounts for only 1% of the hydatid disease burden.11 Close contact with animals such as dogs, sheep, and cattle is a risk factor for acquiring the infection which was also identified in our patient.12
The clinical manifestation of hydatid disease is primarily related to the mass effect exerted by the cyst on adjacent structures.7 The mass effect is more pronounced in structures with limited space like the orbit.1 Patients with orbital hydatid cyst commonly present with a longstanding unilateral proptosis of the eye similar to our patient.11 Other manifestations include decreased vision due to longstanding compression of the optic nerve, ocular pain, limitation of ocular motility, and chemosis.1,12
Patients with suspected hydatid disease of the orbit should be thoroughly investigated. Complete blood count, serum antibody test, and imaging studies are crucial to exclude other potential differential diagnoses. Mass lesions such as dermoid cyst, epidermoid cyst, hemangiomas, post-traumatic hematomas, and mucocele can be considered differentials based on the presenting symptom.13 CT scan and MRI are the preferred choices of imaging and can help the clinician narrow the differential prior to surgery.1,6 However, histopathology remains the definitive diagnostic modality.1
Management of orbital hydatid disease includes a 2 to 4 week course of anthelmintic drugs, preferably albendazole, followed by surgical excision of the cyst.6,13 Preoperative anthelmintic treatment is vital to prevent parasite seeding and anaphylactic reactions in case the cyst ruptures during manipulation while performing surgery.8,13 If intraoperative rupture of cyst occurs, irrigation with hypertonic saline and hydrogen peroxide would kill daughter cysts and prevent further spread.14 The operating surgeon should aim for complete excision of the cyst with minimal ocular tissue damage.11
Conclusion
Echinococcosis, although extremely rare, has the potential to affect the eye. It should be kept in the list of differential diagnoses for patients with pertinent history and risk factors. Early recognition and treatment of orbital echinococcosis is crucial to prevent vision-related complications.
Data Sharing Statement
The data set and images supporting the conclusions of this case report are included within the article.
Ethical Approval
Ethical clearance was obtained from St. Paul’s Hospital Millennium Medical College review board (IRB reference number PM23/383).
Consent for Publication
Informed consent was obtained from the patient for the publication of this case report. Potential identifiers of the patient were excluded from the report.
Acknowledgment
We are grateful to the patient for providing consent for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding for the study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Fasina O, Ogun OG. Hydatid cyst of the orbit in a young Nigerian female: a case report. Ghana Med J. 2017;51(4):204–206. doi:10.4314/gmj.v51i4.11
2. Al-Muala HD, Sami SM, Shukri MA, Hasson HK, Alaboudy AT. Orbital hydatid cyst. Ann Maxillofac Surg. 2012;2(2):197. doi:10.4103/2231-0746.101365
3. Taghipour M, Derakhshan N, Saffarian A, Dehghanian A. Orbital hydatid cyst causing papilledema and proptosis in an adult. World Neurosurg. 2017;101:
4. Somay H, Emon ST, Orakdogen M, Berkman MZ. A primary orbital hydatid cyst. J Clin Neurosci. 2012;19(6):898–900. doi:10.1016/j.jocn.2011.09.018
5. Berradi S, Hafidi Z, Lezrek O, Lezrek M, Daoudi R. Orbital hydatid cyst. QJM. 2015;108(4):343–344. doi:10.1093/qjmed/hcu203
6. Kumar A, Parihar V, Yadav YR, Shrivastava V, Patel NK. A rare case of giant primary orbital hydatid cyst. World Neurosurg. 2019;124:197–200. doi:10.1016/j.wneu.2018.12.208
7. Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003;23(2):475–494. doi:10.1148/rg.232025704
8. M-s M, Su F, Hei Y, Feng M-Y, Yang X-J. Disseminated hydatid disease in the orbit and central nervous system. Int J Ophthalmol. 2021;14(9):1457. doi:10.18240/ijo.2021.09.25
9. Kufel J. Pathological structural changes in the brain in the course of neurocysticercosis–pathogenesis, serological diagnostics and imaging: a literature review. Ann Parasitol. 2020;66(4):441–446. doi:10.17420/ap6604.284
10. Malik A, Chandra R, Prasad R, Khanna G, Thukral BB. Imaging appearances of atypical hydatid cysts. Indian J Radiol Imaging. 2016;26(1):33. doi:10.4103/0971-3026.178284
11. Turgut AT, Turgut M, Koşar U. Hydatidosis of the orbit in Turkey: results from review of the literature 1963–2001. Intl Ophthalmol. 2004;25(4):193–200. doi:10.1007/s10792-004-6739-1
12. Santosh T, Patro MK, Bal AK, Behera B. Hydatid cyst at unusual locations: report of two cases. Human Pathol. 2017;8:59–61.
13. Chtira K, Benantar L, Aitlhaj H, Abdourafiq H, Elallouchi Y, Aniba K. The surgery of intra-orbital hydatid cyst: a case report and literature review. Pan Afr Med J. 2019;33(1). doi:10.11604/pamj.2019.33.167.18277
14. Aloua R, Slimani F. Calcified hydatid cyst of the orbit. J Pediatr Surg Case Rep. 2021;64:101708. doi:10.1016/j.epsc.2020.101708
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.