")
Back to Journals » International Medical Case Reports Journal » Volume 17
Primary Cardiac Sarcoma, Diagnostic and Therapeutic Challenges in Resource Limited Setting: Case Report
Authors Mulisa MD , Bekele SK , Woldemichael SB, Gaito SG, Abrar FN, Hailu BG
Received 22 August 2023
Accepted for publication 16 January 2024
Published 25 January 2024 Volume 2024:17 Pages 57—61
DOI https://doi.org/10.2147/IMCRJ.S436528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Merga Daba Mulisa,1 Shalom Kassahun Bekele,1 Sisay Bekele Woldemichael,2 Sitota Ganjula Gaito,3 Fadil Nuredin Abrar,4 Betelhem Gebreamlak Hailu4
1Department of Internal Medicine, School of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Cardiothoracic Unit, Cardiac Center of Ethiopia, Addis Ababa, Ethiopia; 3Cardiology Unit, Cardiac Center of Ethiopia, Addis Ababa, Ethiopia; 4Department of Pathology, School of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Merga Daba Mulisa, Department of Internal Medicine, School of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia, Tel +251912684411, Email [email protected]
Abstract: Left atrial masses are commonly caused by atrial myxomas and metastatic tumors. Primary cardiac sarcomas are rare. Patients present with symptoms related to the tumor location. There are only a few case reports on this rare disease. We report the case of a 17 years old male patient presented with shortness of breath for 2-month duration. Echocardiography revealed a left atrial mass that was later surgically excised and histopathology confirmed a primary cardiac sarcoma. We discuss the diagnostic and therapeutic challenges encountered in the management of this rare disease. To the best of our knowledge, this is the first case reported in East Africa.
Keywords: primary cardiac sarcoma, atrial mass, atrial myxoma
Introduction
Primary cardiac tumors are rare, with an incidence of approximately 0.02%. Most of the primary cardiac tumors are benign, whereas the rest are malignant. By comparison metastatic cardiac tumors are more common than primary cardiac tumors. The most common tumors that metastasis to the heart include melanoma, lung cancer, lymphoma, breast cancer, leukemia, stomach cancer, liver and colon cancers.1,2
Malignant tumors constitute about 15% of the primary cardiac tumors. From this sarcoma are the most common type. The most commonly reported sarcomas include rhabdomyosarcomas, angiosarcomas, myxosarcomas, fibrosarcoma, and leiomyosarcoma.3 Cardiac sarcomas are most frequently diagnosed as angiosarcoma. Most angiosarcomas occur in the right atrium, resulting in obstruction of the inflow or outflow of blood.4
The symptoms and signs of cardiac tumors generally depend on the location. They produce symptoms through different mechanisms, including: obstruction of the circulation through the heart or heart valve, symptoms of heart failure, local invasion leading to arrhythmia or pericardial effusion, embolization that could be systemic or pulmonary, and tumors that can also cause systemic or constitutional symptoms. However, some tumors are incidental finding.5
Cardiac sarcomas are extremely rare, and only isolated case reports have been published. To the best of our knowledge, there are no case reports of this rare disease entity in East Africa, and this is the first case to be reported in this region. Here, we present the case of 17 years old Ethiopian male patient who presented with shortness of breath of 2 months.
Case Presentation
A 17yrs old male with no prior medical history presented with shortness of breath for 2-month duration, with associated fatigue and palpitations. In addition, the patient experienced left-sided chest discomfort and intermittent dry cough for the same duration.
On presentation, the patient was afebrile, and had sinus tachycardia (110 b.p.m) with borderline blood pressure of 90/60 mmHg. He had an elevated respiratory rate of 24 breaths/minute with an oxygen saturation of 92% on room air. Upon further examination, the patient had pale conjunctiva and cardiac auscultation revealed a grade 3 diastolic murmur over the apex. In addition, he had no peripheral edema, and the chest was resonant with comparable breath sounds heard in both lung fields.
Laboratory investigations revealed moderate anemia (hemoglobin 9.2 g/dL) and elevated levels of acute phase reactants (ESR of 120mm/hr and CRP protein, 2 mg/dL). ECG revealed sinus tachycardia and chest radiography revealed a left atrial border bulge and increased vascular markings.
Transthoracic Echocardiography (Figure 1A and B) showed a 4cm × 5cm big mass in the left atrium occupying the entire left atrium with an obstructive effect on the mitral valve, resulting in severe mitral stenosis, mild-to-moderate mitral regurgitation, and severe tricuspid regurgitation with severe pulmonary hypertension.
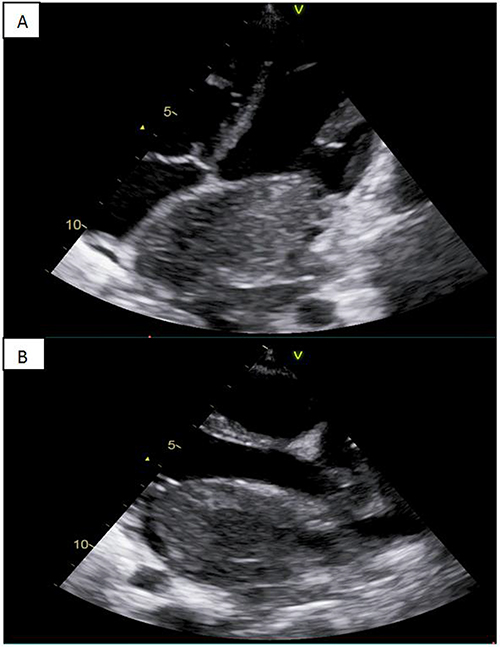 |
Figure 1 Trans thoracic echocardiographic image, (A) apical view, (B), parasternal long axis view. |
Owing to the obstructive effect of the mass, an open-heart surgery was performed to resect the mass. Intraoperative findings revealed a 7cm × 8cm friable mass growing from the posterior wall of the left atrium and filling the lumen. The mass had a broad base and transmural growth, with invasion of the posterior pericardium. The mass was excised together with the posterior wall of the left atrium with a 0.5cm margin, and the posterior wall of left atrium was reconstructed using the pericardium.
Subsequently, the histological results revealed a high-grade sarcoma with a possible differential diagnosis of rhabdomyosarcoma and leiomyosarcoma (Figure 2A–D), and immunohistochemistry was recommended.
 |
Figure 2 Histology results. Photomicrography of pleomorphic spindle cells arranged in storiform pattern, Low power magnification x10 (A), Medium power magnification x20 (B), (C) High power photomicrography of pleomorphic spindle cells (Magnification x40) and (D) Areas of extensive necrosis (Magnification x40); Microscopy showed highly pleomorphic polygonal to spindle cells with vesicular nuclei, prominent nucleoli and abundant eosinophilic cytoplasm arranged in short intersecting fascicles and storiform pattern. Frequent mitotic figures and extensive areas of necrosis were also noted. |
During his first and only oncology outpatient department visit, immunohistochemistry was recommended; however, the patient was lost to follow- up.
Three-months post-operatively, the patient presented with severe headache and non-contrast brain CT showed intracranial bleeding. Repeat transthoracic echocardiography performed during this visit revealed a mass involving the right atrium and right ventricle, with extension to the left ventricle. The patient died 3 months after the initial diagnosis.
Discussion
Primary cardiac sarcomas (PCS) are the most common malignancy that affects the heart.3 PCS are believed to arise denovo; they do not arise from benign tumors.5 Most of the patients are diagnosed in the age between 40 and 59 years.6 As already discussed, the clinical manifestations of PCS are mainly dependent on the location of the tumor.5
Diagnostic methods include cardiac imaging modalities such as echocardiography, cardiac magnetic resonance imaging, computed tomography, positron emission tomography, and histologic evaluation. Transthoracic echocardiography is often the first and most commonly used diagnostic tool for patients suspected of having cardiac mass because of its availability and low cost.7 However, computed tomography and cardiac magnetic resonance imaging are usually required to rule out tumors.7,8 Several cases of malignant cardiac sarcomas misdiagnosed as cardiac myxomas have been reported.9,10
Due to limited data on primary cardiac tumors, there is currently no guideline-directed management of primary cardiac tumors.8
Our patient was presented with shortness of breath for 2 months, and echocardiography showed a 4cm × 5cm mass in the left atrium occupying the entire left atrium with an obstructive effect on the mitral valve, resulting in severe mitral stenosis and severe pulmonary hypertension. With a pre-operative diagnosis of atrial myxoma, surgery was performed, and the mass was excised. Histopathological examination revealed a high -grade sarcoma. As it was mentioned, like our patient, there are reports of cases of malignant primary cardiac tumor misdiagnosed as an atrial myxoma.
Although surgical management is the treatment of choice for primary cardiac sarcoma, the long - term prognosis is poor.11 The median survival time of these patients was between 6 and 12 months. Advanced age and advanced disease with metastasis are independent risk factors for poor prognosis. Surgery, adjuvant chemotherapy, and radiation do not affect the mortality.6
Our patient had a smooth early postoperative period, and was discharged with improvement. He was followed-up for 3 months until he developed intra-cranial bleeding, and repeated echocardiography showed a mass that involved the right atrium and right ventricle with extension to the left ventricle. This is most likely due to the metastasis of cardiac sarcoma to other parts of the heart that are not involved during surgery.
Conclusion
Primary cardiac sarcomas are rare. Patients often present with symptoms related to tumor location. The patients may have been misdiagnosed with atrial myxoma, as observed in our study. Despite surgical resection, the prognosis for these patients is poor.
Data Sharing Statement
Laboratory investigations, patient physical findings, imaging results and histopathology results used to support the findings of this study are included in the article.
Ethical Approval
The authors’ institution does not require ethical approval for publication of single case report.
Consent for Publication
The patient’s family provided oral informed consent for the publication of details including, history, physical findings, laboratory reports, imaging, and histopathology results. The verbal consent was witnessed and is held on file within our institution.
Acknowledgments
The authors thank Dr. Adane Petros for his support in preparing this case report.
Funding
No funding was used in this case report.
Disclosure
We authors have no conflict of interest.
References
1. Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996;77(1):107. PMID: 8540447. doi:10.1016/s0002-9149(97)89149-7
2. Abraham KP, Reddy V, Gattuso P. Neoplasms metastatic to the heart: review of 3314 consecutive autopsies. Am J Cardiovasc Pathol. 1990;3(3):195–198. PMID: 2095826.
3. Molina JE, Edwards JE, Ward HB. Primary cardiac tumors: experience at the University of Minnesota. Thorac Cardiovasc Surg. 1990;38(Suppl 2):183–191. PMID: 2237900. doi:10.1055/s-2007-1014064
4. Siontis BL, Zhao L, Leja M, et al. Primary cardiac sarcoma: a rare, aggressive malignancy with a high propensity for brain metastases. Sarcoma. 2019;2019:1960593. PMID: 30962762; PMCID: PMC6431449. doi:10.1155/2019/1960593
5. Vander Salm TJ. Unusual primary tumors of the heart. Semin Thorac Cardiovasc Surg. 2000;12(2):89–100. PMID: 10807431. doi:10.1053/ct.2000.5080
6. Bangolo A, Fwelo P, Iyer KM, et al. Primary cardiac sarcoma: clinical characteristics and prognostic factors over the past 2 decades. Diseases. 2023;11(2):74. doi:10.3390/diseases11020074
7. Pino PG, Moreo A, Lestuzzi C. Differential diagnosis of cardiac tumors: general consideration and echocardiographic approach. J Clin Ultrasound. 2022;50(8):1177–1193. PMID: 36218203; PMCID: PMC9828386. doi:10.1002/jcu.23309
8. Gupta R, Meghrajani V, Desai R, Gupta N. Primary malignant cardiac tumors: a rare disease with an adventurous journey. J Am Heart Assoc. 2020;9(10):e016032. PMID: 32389052; PMCID: PMC7660851. doi:10.1161/JAHA.120.016032
9. Hasegawa T, Nakagawa S, Chino M, Kunihiro T, Ui S, Kimura M. Primary cardiac sarcoma mimicking benign myxoma: a case report. J Cardiol. 2002;39(6):321–325.
10. Kim JT, Baek WK, Kim KH, Yoon YH, Kim DH, Lim HK. A primary cardiac sarcoma preoperatively presented as a benign left atrial myxoma. Yonsei Med J. 2003;44(3):530–533. doi:10.3349/ymj.2003.44.3.530
11. Matteucci M, Ferrarese S, Mantovani V, et al. Surgical treatment of primary cardiac tumors in the contemporary era: a single-centre analysis. J Card Surg. 2021;36(10):3540–3546. PMID: 34254361; PMCID: PMC8518736. doi:10.1111/jocs.15813
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.