")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Prevalence of Pelvic Floor Disorders in Parous Women from the Tibet Autonomous Region: A Cross-Sectional Study
Authors Lv A, Ding T, DeQiong, DaWaZhuoMa, Cai L, Zhang Y, Yin J, SeZhen, Lv Q
Received 13 October 2023
Accepted for publication 28 December 2023
Published 9 January 2024 Volume 2024:17 Pages 159—167
DOI https://doi.org/10.2147/JMDH.S444616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Aiming Lv,1,2 Tong Ding,2 DeQiong,2 DaWaZhuoMa,2 Long Cai,2 Yutong Zhang,2 Jinyu Yin,2 SeZhen,2 Qiubo Lv1
1Department of Obstetrics and Gynecology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Women and Children’s Hospital of Tibet Autonomous Region, Lhasa, Tibet Autonomous Region, People’s Republic of China
Correspondence: Qiubo Lv, Department of Obstetrics and Gynecology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, No. 1 DaHua Road, Dong Dan, Beijing, 100730, People’s Republic of China, Tel +86 13801192185, Fax +86 10 85136220, Email [email protected]
Purpose: Pelvic floor disorder (PFD) seriously affects the everyday life of women. This cross-sectional study aimed to evaluate the prevalence and risk factors for postpartum PFD in women living in the Tibet Autonomous Region (TAR).
Methods: Parous women who attended the outpatient gynaecology clinic at our hospital between June 2022 and August 2022 were screened in this study. The demographic and clinical data of these women were collected. Their pelvic floor functions were evaluated via a pelvic organ prolapse (POP) quantification examination, the Pelvic Floor Distress Inventory Questionnaire-20 (PFDI-20) and the Overactive Bladder Symptom Score (OABSS).
Results: A total of 201 women were included in this study, of whom 81.09% (163/201) were Tibetan. Twenty-seven women (13.43%) were diagnosed with POP stage ≥ 2 and 27 women (13.43%) with an OABSS score ≥ 3. The median PFDI-20 total score was 4.17 (range 0– 43.75). Han women (n = 38) in the TAR had much lower PFDI-20 total scores, compared with Tibetan women (n = 163) (p < 0.05). The results of the multiple linear regression models showed that the PFDI-20 scores obtained from women living in the TAR were closely related to parity, history of heavy weight lifting, age, history of instrumental deliveries, ethnicity and number of caesarean sections.
Conclusion: Pelvic floor disorder is common among parous women living in the TAR. Ethnicity, parity, history of heavy weight lifting, age, history of instrumental deliveries and number of caesarean sections are the factors closely related to the PFDI-20 scores.
Keywords: pelvic floor disorder, Tibet Autonomous Region, pelvic organ prolapse, urinary incontinence, overactive bladder symptoms
Introduction
Pelvic floor disorder (PFD) is a series of symptoms of dysfunction caused by injuries on pelvic floor muscle (PFM) and pelvic fascia, and it is a highly prevalent condition in women.1,2 It can seriously affect women’s everyday lives, causing symptoms such as urinary incontinence (UI), faecal incontinence, pelvic organ prolapse (POP), chronic pelvic pain and sexual dysfunction.3 Most of the previous epidemiologic studies on POP and UI are based on patient reporting, which relies on women’s subjective perception and willingness to report.4 Many studies consist of case series or hospital experiences because population-based studies are difficult and expensive to implement. Pelvic floor disorder affects almost 25% of women in the United States.5 In China, the prevalence of UI is as high as 30.9%, and the incidence of self-reported symptomatic POP is up to 9.6%.3 Pelvic floor disorder not only affects the physical aspects of women but also impacts them socially and psychologically, making them prone to anxiety and depression.6 Childbirth is a well-known risk factor for PFD. Both vaginal delivery and caesarean section reduce the strength and endurance of PFM.7 However, the risk of PFD is reported to be higher among women with vaginal delivery, as PFM would be subjected to a high degree of deformation for a long period during vaginal delivery.8 Furthermore, hormonal changes during pregnancy also modify the tissues of the pelvic floor, negatively affecting its function.7 Physical activity and weight lifting are other important factors that affect pelvic floor function. Several studies suggest that intensive exercise can increase intra-abdominal pressure and worsen pelvic floor function, amplifying the risk of PFD.8 The incidence of UI is higher in professional women athletes compared with non-exercising women.9 Other factors affecting pelvic floor function include age, obesity, chronic constipation, gynaecological disorders and respiratory system diseases.8
Until now, few studies investigating the conditions of pelvic floor functions in Chinese women have included women from the Tibet Autonomous Region (TAR). The TAR, with an average altitude of >4000 m, has historically been home to a large number of ethnic minority residents, including Tibetan populations.10 The unique hypobaric hypoxia environment and other related factors have caused a suboptimal health status among the populations in the TAR. Furthermore, women in the TAR have more pregnancies, less access to obstetric care and more physical strain in daily life compared with women living in urban areas. Fan et al even found that Tibetan women had smaller pelvises compared with Chinese Han women.11 Due to these factors, PFD may be more common and may affect daily life more severely in women living in the TAR. To validate this hypothesis, we conducted this cross-sectional study to evaluate the prevalence and risk factors for postpartum PFD in women living in the TAR.
Materials and Methods
Patients
This cross-sectional study was approved by the ethics committee of the Women and Children’s Hospital of Tibet Autonomous Region in accordance with the Declaration of Helsinki (No. qfeyy-2022002). Parous women who attended the outpatient gynaecology clinic at the hospital for routine examinations between June 2022 and August 2022 were screened in this study. Before being recruited, all participants were informed in detail about the purpose of the study, the process and the written information related to the study.
The inclusion criteria were as follows: (1) non-pregnant women aged >18 years; (2) permanent residents in the TAR; (3) parous women; and (4) women who were postpartum for >1 year. The exclusion criteria were as follows: (1) pregnant women; (2) women with a history of previous gastrointestinal, anorectal or gynaecological surgery; and (3) women who were unable to complete the questionnaire or follow instructions due to cognitive or language deficits.
All participants who met the inclusion and exclusion criteria were recruited by gynaecological clinicians. The recruiters provided a written commitment to keep all participants’ personal information anonymous during the experiment and did not participate in the interviews, data analysis or manuscript writing.
Data Collection
Women who agreed to participate in the study were asked to answer a structured questionnaire, which was explained in detail by trained staff and administered in a face-to-face interview. Information on demographic and clinical data, including age, ethnicity, educational level, gravidity, parity, number of spontaneous vaginal deliveries, number of caesarean sections, history of previous gynaecological surgery, moderate- and high-intensity activity (metabolic equivalent of task >3), history of instrumental deliveries and history of lifting more than half their own body weight after delivery (>1 time per week) was obtained through this questionnaire. The questionnaire also contained items to identify UI, anal incontinence, constipation, defecation disorders, history of urinary tract infection, the presence of urgent urination, the presence of frequent micturition, the habit of holding urine and the use of Kegel exercises. A preliminary study was conducted before the present one to ensure the comprehensibility of the questionnaire items. At the end of each interview, the questionnaires were checked for consistency and completeness. The interviews were conducted by a chief physician, a medical doctor and a PhD student who was not involved in the data analysis. The interviews were audio recorded. No explicit time constraints were applied, but each interview typically lasted 30–40 mins.
A POP quantification (POP-Q) examination was performed on the maximal Valsalva manoeuvre by an expert urogynaecologist with >10 years of experience, with the participants in the lithotomy position, backs elevated to 45° and during maximal strain. All participants were asked to complete items from the Pelvic Floor Distress Inventory Questionnaire-20 (PFDI-20) and Overactive Bladder Symptom Score (OABSS) after the interview and physical examination. All the above data were collected only once throughout the study period.
Study Tools
The PFDI-20 questionnaire is designed to comprehensively evaluate the distress caused by the presence of PFD. It consists of three scales: the POP distress inventory (POPDI-6; 6 questions), the Urogenital Distress Inventory (UDI-6; 6 questions) and the Colorectal-Anal Distress Inventory (CRADI-8; 8 questions). Each item is scored as 0–4. The score for each subscale is calculated by averaging the sum of the items and the number of items in the subscale and multiplying the result by 25. The PFDI-20 total score is represented by the sum of the scores of the three subscales. The higher the score is, the more effective the PFD.12
The OABSS is a well-known questionnaire for assessing the severity of overactive bladder (OAB) using four questions, including storage symptoms during daytime voiding, storage symptoms during night-time voiding, urgency and urge incontinence.13 The overall OABSS score is the sum of the scores of the four questions. A higher score indicates a higher symptom burden. Here, a diagnosis of OAB was made if the total OABSS score was 3 points.14
The POP-Q system, which is approved by the International Continence Society, is a standardised measurement of POP that includes measurements of the genital hiatus, perineal body, point Ba (the lowest point of the anterior vaginal wall), point Bp (the lowest point of the posterior vaginal wall), C (cervix or cuff descent) and total vaginal length (TVL).15 The prolapse is staged according to the most distal point, which is classified as stage 0 (no prolapse), stage 1 (the most distal portion of the prolapse is more than 1 cm above the level of the hymen), stage 2 (the most distal portion of the prolapse is situated between 1 cm above the hymen and 1 cm below the hymen), stage 3 (the most distal portion of the prolapse is more than 1 cm beyond the plane of the hymen, but not completely everted) and stage 4 (complete procidentia or vault eversion; the most distal prolapse is >[TVL−2] cm).16 Patients with POP-Q stage ≥2 are considered to have symptomatic prolapse.
Statistical Analysis
Data analysis was performed using the SPSS 22.0 software package. The measurement data that fulfilled normal distribution were presented as mean ± SD and compared using the t‐test. The measurement data that had not fulfilled normal distribution were presented as median and range and compared using the Wilcoxon rank-sum test. The categorical data were presented as percentages (%), and the comparison was conducted via the chi-squared test or Fisher’s exact test. Multiple linear regression analysis with a stepwise method was used to examine the effect of different demographic and clinical characteristics on PFDI-20 total scores. A value of p < 0.05 was considered as statistically significant.
Results
A total of 214 parous women met our inclusion criteria, and 13 were excluded due to being unable to complete the questionnaire or assessment. Finally, 201 women were included, with a mean age of 34.90 ± 8.65 years. Among the enrolled participants, 81.09% (163/201) were Tibetan. Most of the participants had attained high school or above education. The mean gravidity was 3.12 ± 1.62 (range 1–8) and the mean parity was 2.20 ± 0.87 (range 1–5). A total of 37.31% (75/201) of the participants reported UI, 19.40% (39/201) reported urgent urination and 15.92% (32/201) reported frequent micturition. The demographic and clinical characteristics are shown in Table 1.
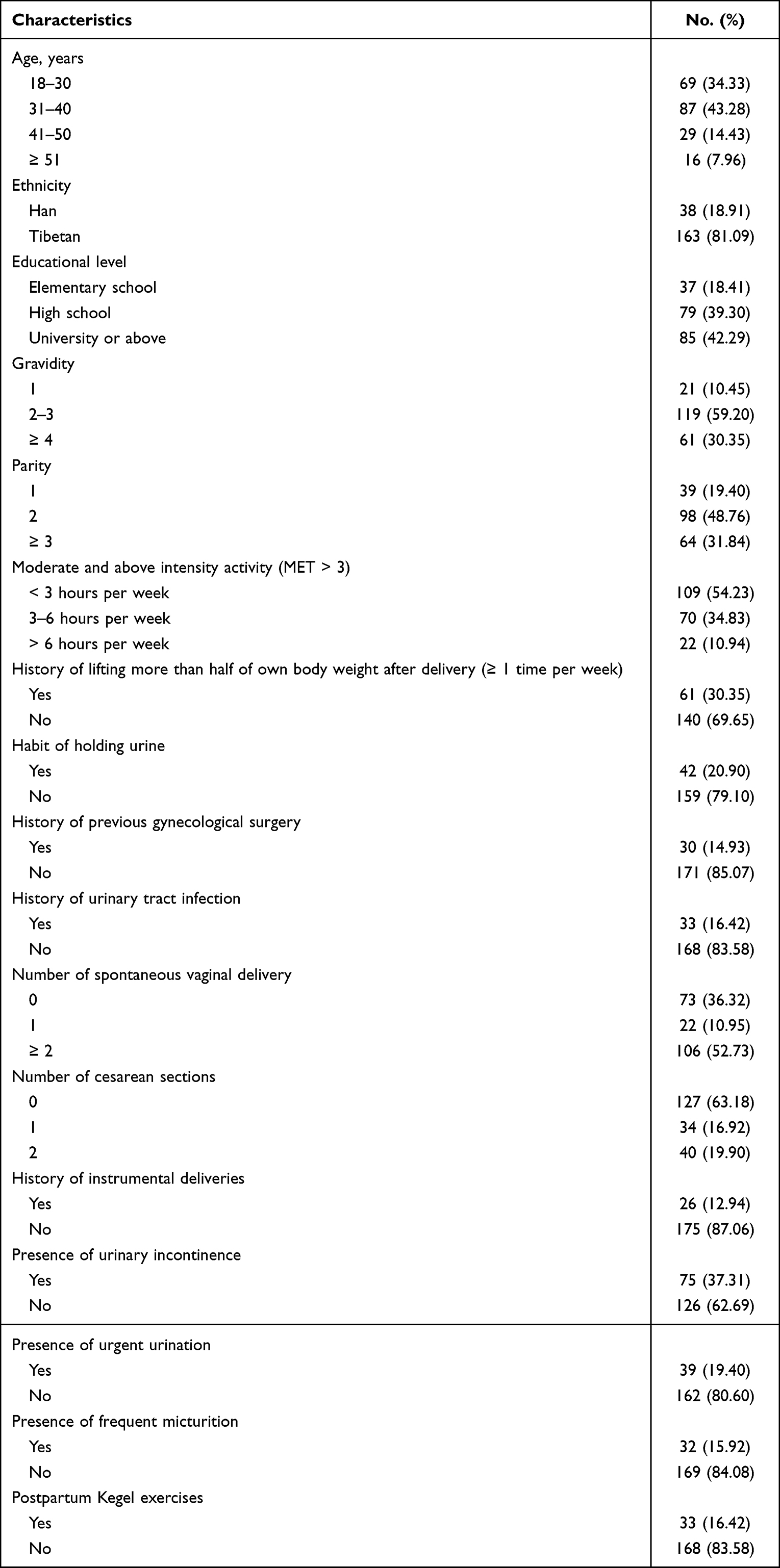 |
Table 1 The Demographic and Clinical Characteristics of the Enrolled Participants |
According to the POP-Q system, there were 97 (48.26%) women with POP-Q stage 1. A total of 27 participants (13.43%) reached the diagnostic criteria for POP (stage ≥2). Among them, 26 (12.94%) were stage 2, and 1 (0.50%) was stage 3. No woman with POP-Q stage 4 was found (Figure 1). The range of OABSS scores of all participants was 0–9. There were 27 (13.43%) women with an OABSS score ≥3 points. The median POPDI-6 score, CRADI-8 score, UDI-6 score and PFDI-20 total score were 0 (range 0–12.50), 0 (range 0–12.50), 4.17 (range 0–37.50) and 4.17 (range 0–43.75), respectively. The UDI-6 inventory contributed the most points in the PFDI-20 scores. There were 116 (57.71%) participants with a PFDI-20 score ≥1 point.
 |
Figure 1 The results of pelvic organ prolapse quantification (POP-Q) examination. |
Subsequently, the participants were divided into two groups based on ethnicity: a Tibetan group (n = 163) and a Han (n = 38) group. As shown in Table 2, the Han women had much lower UDI-6 scores and PFDI-20 total scores compared with the Tibetan women (p = 0.001 and 0.003, respectively). Furthermore, the Han women also had much lower OABSS scores than the Tibetan women (p = 0.012, Table 2). The above results indicated that Tibetan women living in the TAR have a higher risk of PFD (particularly regarding the aspect of urogenital distress) than Han women living in the same area.
 |
Table 2 The Comparisons of PFDI-20 Scores and OBASS Scores Between Tibetan and Han Women in Tibetan Plateau |
Multiple linear regression models showed that the PFDI-20 scores obtained from women living in the TAR were closely related to parity (β = 4.641; 95% CI = 2.973–6.310; p < 0.001), history of lifting more than half their own body weight after delivery (>1 times per week) (β = 3.836; 95% CI = 1.489–6.184; p = 0.001); age (β = 3.390; 95% CI = 2.150–4.630; p < 0.001), history of instrumental deliveries (β = 5.200; 95% CI = 2.362–8.038; p < 0.001), ethnicity (β = −3.104; 95% CI = −5.653–[−8.038]; p = 0.017) and number of caesarean sections (β = −1.505; 95% CI = −2.763–[−0.248]; p = 0.019) (Table 3).
 |
Table 3 Multivariate Linear Regression Analysis for Factor Associated with PFDI-20 Scores |
Discussion
Our results suggest that the prevalence of POP in Tibetan parous women is high, but that severe POP is rare. A total of 27 (13.43%) women were diagnosed as OAB based on the OABSS scores, and 116 (57.71%) participants had been troubled by at least one aspect of PFD symptoms. The PFDI-20 scores were closely related to ethnicity. Other factors that were associated with PFDI-20 scores were parity, history of heavy weight lifting, age, history of instrumental deliveries and number of caesarean sections. We also found that UDI-6 contributed the most points in the PFDI-20 scores, suggesting that most of the participants in our study were affected by urogenital distress.
According to the Chinese epidemiological census data, the prevalence of symptomatic POP (stage ≥2) in Chinese women is 9.6%;17 however, the data are more significant in plateau women. Similar results have been found in other populations living at high altitudes. Nepal and the TAR are both located in the TAR plateau. Thus, the Nepali population has certain similar characteristics as those in the TAR. Caagbay et al18 evaluated the pelvic floor functions of 123 Nepali women and found that 29 (24%) of the enrolled participants had POP-Q stage ≥1, eight (7%) had POP-Q stage 3 and three (2%) POP-Q stage 4.
Pelvic floor disorder is one of the most common health problems for women, particularly for parous women. A previous meta-analysis, which included 49 studies, reported that the overall pooled prevalence of PFDs in low- and middle-income countries was 25%.16 The studies, conducted by Chinese groups, found that the prevalence of UI in adult Chinese women was 31.1%,19 and POP was reported to affect 9.67% of urban Chinese women.19
A meta-analysis of 18 studies on PFD/UI showed that Caucasian women accounted for 70–89% of the PFD literature, whereas Asian women accounted for only 0.5%–6%,20 which may be due to ethnocultural and racial differences. It also suggests that PFD studies would benefit from targeted minority sampling. Recent studies have reported that the prevalence of PFD differs between ethnic groups. Thus, ethnicity is likely to be a significant risk factor for PFD.21,22 The Tibetan nationality is one of the Chinese minorities who have lived on the Tibetan plateau for centuries. The population features in this nationality showed relative stability, such as similar lifestyle, same religion, more physical strain in daily life and >2 children during these centuries,23 which is different from the Han population. Furthermore, Tibetan women may be more easily affected by PFD. As expected, in the present study, we found that Tibetan women had much higher UDI-6, PFDI-20 and OABSS scores than Han women. These results suggest that Tibetan women may have more severe PFD symptoms than Han women who live in the TAR permanently, particularly regarding the aspect of urogenital distress. The multiple linear regression analysis further confirmed that the PFDI-20 scores were closely related to ethnicity. However, the number of Han women enrolled in this study was relatively small. Further studies are needed to confirm our conclusion.
The OABSS has been developed to express all of the OAB symptoms in a single result, which is usually used in the objective diagnosis of OAB.24 According to statistics from different countries, the prevalence of OAB among women ranges from 6.0% to 17.4%.25 The prevalence of OAB in our studied population falls within this range. The PFDI-20 questionnaire was developed to assess the impact of PFD on health-related quality of life in women. Arruda et al12 suggested that PFD symptoms can be classified as mild (1–15 points), moderate (16–34 points) and severe (>35 points) based on PFDI-20 total scores; however, this classification has not been validated by other groups.
Other factors that were associated with PFDI-20 scores analysed by our multiple linear regression analysis were parity, history of heavy weight lifting, age, history of instrumental deliveries and number of caesarean sections. Consistent with previous studies,26 our data suggest that parity is significantly associated with PFD. Intensive exercise can increase intra-abdominal pressure and worsen the pelvic floor function. Similar to other studies,27 a history of heavy weight lifting was found to be a risk of PFD in this study. The activity of PFM has been reported to decrease with increasing age.28,29 MacLennan et al30 found that PFDs were strongly associated with instrumental delivery. Our study obtained a similar result. Although both vaginal delivery and caesarean section could influence the strength and endurance of PFM, the risk of PFD has been reported to be higher among women with vaginal deliveries.7 Our results supported this opinion. Compared with women with vaginal delivery (number of caesarean sections = 0), those with >1 caesarean sections had lower PFDI-20 scores.
The present study has several limitations. First, the sample size was extremely small, and only a small number of the Han population were enrolled. In addition, women from other ethnic groups, such as those of Moinba nationality, were not included in the study, meaning our study population did not fully represent the women in the TAR. Second, we did not perform an a priori sample size calculation because there were no available data. Furthermore, the cross-sectional nature of this study meant the causality between the dependent and independent variables could not be fully established. Finally, due to medical constraints, we used only three scale instruments to evaluate PFD in our study population. Other tools, such as electromyography, transperineal ultrasound and magnetic resonance imaging, are needed to comprehensively evaluate PFM strength and the prevalence of PFD in women living in the TAR.
Conclusions
Our results provide objective data on the pelvic floor health status of parous women in Tibet; that is, postpartum PFD is common among parous women in the TAR. Ethnicity, parity, history of heavy weight lifting, age, history of instrumental deliveries and number of caesarean sections are the factors closely related to the PFDI-20 scores.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of our hospital, and written informed consent was obtained from all participants.
Funding
1.National High Level Hospital Clinical Research Funding, BJ-2019-138. 2.The Natural Science Foundation of the Tibet Autonomous Region organized a group aid project for Tibetan medicine, XZ2022ZR-ZY16(Z).
Disclosure
The authors report no conflicts of interest in this work.
References
1. González-Gutiérrez MD, López-Garrido Á, Cortés-Pérez I, Obrero-Gaitán E, León-Morillas F, Ibáñez-Vera AJ. Effects of non-invasive radiofrequency diathermy in pelvic floor disorders: a systematic review. Medicina. 2022;58(3):437. doi:10.3390/medicina58030437
2. Verbeek M, Hayward L. Pelvic floor dysfunction and its effect on quality of sexual life. Sex Med Rev. 2019;7(4):559–564. doi:10.1016/j.sxmr.2019.05.007
3. Zhu H, Zhang D, Gao L, et al. Effect of pelvic floor workout on pelvic floor muscle function recovery of postpartum women: protocol for a randomized controlled trial. Int J Environ Res Public Health. 2022;19(17). doi:10.3390/ijerph191711073
4. Larsudd-Kåverud J, Gyhagen J, Åkervall S, et al. The influence of pregnancy, parity, and mode of delivery on urinary incontinence and prolapse surgery-A national register study. Am J Obstet Gynecol. 2023;228(1):
5. Wheat JE, Khan M, Banaag A, et al. Prevalence of pelvic floor disorders in United States active-duty service women seeking medical care. Female Pelvic Med Reconstr Surg. 2022;28(6):e195–e200. doi:10.1097/spv.0000000000001183
6. Rashidi F, Mirghafourvand M. Pelvic floor disorder and relevant factors in Iranian women of reproductive age: a cross-sectional study. BMC Women's Health. 2023;23(1):71. doi:10.1186/s12905-023-02226-1
7. Dietz HP, Scoti F, Subramaniam N, Friedman T, Shek KL. Impact of subsequent pregnancies on pelvic floor functional anatomy. Int Urogynecol J. 2018;29(10):1517–1522. doi:10.1007/s00192-018-3567-9
8. Tim S, Mazur-Bialy AI. The most common functional disorders and factors affecting female pelvic floor. Life. 2021;11(12):1397. doi:10.3390/life11121397
9. Shaw JM, Nygaard IE. Role of chronic exercise on pelvic floor support and function. Curr Opin Urol. 2017;27(3):257–261. doi:10.1097/mou.0000000000000390
10. Gipson JD, Moucheraud C, Gyaltsen K, Tsering L, Nobari TZ, Gyal L. Nomadic Tibetan women’s reproductive health: findings from cross-sectional surveys with a Hard-to-Reach Population. Reprod Health. 2021;18(1):63. doi:10.1186/s12978-020-01052-0
11. Fan X, Zhou Z, Stewart M, et al. Comparing the Pelvis of Tibetan and Chinese Han Women in Rural Areas of China: two population-based studies using coarsened exact matching. J Obstet Gynaecol. 2022;42(3):403–409. doi:10.1080/01443615.2021.1908241
12. de Arruda GT, de Andrade DF, Virtuoso JF. Internal structure and classification of pelvic floor dysfunction distress by Pfdi-20 Total Score. J Patient Rep Outcomes. 2022;6(1):51. doi:10.1186/s41687-022-00459-6
13. Homma Y, Yoshida M, Seki N, et al. Symptom assessment tool for overactive Bladder Syndrome--Overactive Bladder Symptom Score. Urology. 2006;68(2):318–323. doi:10.1016/j.urology.2006.02.042
14. Hikita KS, Honda M, Hirano S, et al. Comparison of the overactive bladder symptom score and the overactive bladder symptom score derived from the bladder diaries. Neurourol Urodyn. 2016;35(3):349–353. doi:10.1002/nau.22719
15. Nam G, Lee SR, Kim SH, Chae HD. Importance of translabial ultrasound for the diagnosis of pelvic organ prolapse and its correlation with the Pop-Q examination: analysis of 363 cases. J Clin Med. 2021;10(18):4267. doi:10.3390/jcm10184267
16. Samantray SR, Mohapatra I. Study of the relationship between Pelvic Organ Prolapse Quantification (Pop-Q) staging and decubitus ulcer in pelvic organ prolapse. Cureus. 2021;13(1):e12443. doi:10.7759/cureus.12443
17. Pang H, Zhang L, Han S, et al. A nationwide population-based survey on the prevalence and risk factors of symptomatic pelvic organ prolapse in adult women in China - A pelvic organ prolapse quantification system-based study. BJOG. 2021;128(8):1313–1323. PMID: 33619817; PMCID: PMC8252658. doi:10.1111/1471-0528.16675
18. Caagbay D, Fatakia FT, Dietz HP, Raynes-Greenow C, Martinho N, Black KI. Is pelvic floor muscle strength and thickness associated with pelvic organ prolapse in Nepali Women? A cross-sectional study. Braz J Phys Ther. 2021;25(2):214–220. doi:10.1016/j.bjpt.2020.05.011
19. Islam RM, Oldroyd J, Rana J, Romero L, Karim MN. Prevalence of symptomatic pelvic floor disorders in community-dwelling women in low and middle-income countries: a systematic review and meta-analysis. Int Urogynecol J. 2019;30(12):2001–2011. doi:10.1007/s00192-019-03992-z
20. Mckay ER, Davila JL, Lee JA, Rolston R, Agalliu I, Abraham NE. Representation of minority groups in key pelvic floor disorder trials. Female Pelvic Med Reconstr Surg. 2021;27(10):602–608. PMID: 34554142. doi:10.1097/SPV.0000000000001002
21. Cheung RY, Shek KL, Chan SS, Chung TK, Dietz HP. Pelvic floor muscle biometry and pelvic organ mobility in East Asian and Caucasian Nulliparae. Ultrasound Obstet Gynecol. 2015;45(5):599–604. doi:10.1002/uog.14656
22. Abdool Z, Dietz HP, Lindeque BG. Ethnic differences in the levator hiatus and pelvic organ descent: a prospective observational study. Ultrasound Obstet Gynecol. 2017;50(2):242–246. doi:10.1002/uog.17297
23. Zhao Y, Luo H, Zhang X, et al. Clinicopathological characteristics and health care for Tibetan women with breast cancer: a cross-sectional survey. BMC Cancer. 2019;19(1):380. doi:10.1186/s12885-019-5580-x
24. Lai YT, Lin AW, Zheng ZH, et al. Perceptions of pelvic floor dysfunction and rehabilitation care amongst women in Southeast China after radical hysterectomy: a qualitative study. BMC Women's Health. 2022;22(1):108. doi:10.1186/s12905-022-01687-0
25. Wróbel A, Skorupska K, Rechberger E, et al. Reliability of the Polish version of the Overactive Bladder Symptom Score (Oabss) questionnaire: correlation of the Oabss with Urodynamic Study and the Udi-6 and Iiq-7 questionnaires. Int Urogynecol J. 2019;30(12):2135–2139. doi:10.1007/s00192-019-04060-2
26. Chang YW, Lo TS, Chang HN, Shiao YH, Yeh YC. Laser acupuncture alleviates symptoms and improves quality of life in women with overactive bladder: a double-blind, pilot randomized controlled trial. Evid Based Complement Alternat Med. 2020;2020:1705964. doi:10.1155/2020/1705964
27. Al-Badr A, Saleem Z, Kaddour O, et al. Prevalence of pelvic floor dysfunction: a Saudi National Survey. BMC Women's Health. 2022;22(1):27. doi:10.1186/s12905-022-01609-0
28. Malaekah H, Al Medbel HS, Al Mowallad S, Al Asiri Z, Albadrani A, Abdullah H. Prevalence of pelvic floor dysfunction in women in Riyadh, Kingdom of Saudi Arabia: a cross-sectional study. Women's Health. 2022;18:17455065211072252. doi:10.1177/17455065211072252
29. Chen GD. Pelvic floor dysfunction in aging women. Taiwan J Obstet Gynecol. 2007;46(4):374–378. doi:10.1016/s1028-4559(08)60006-6
30. MacLennan AH, Taylor AW, Wilson DH, Wilson D. The prevalence of pelvic floor disorders and their relationship to gender, age, parity and mode of delivery. Bjog. 2000;107(12):1460–1470. doi:10.1111/j.1471-0528.2000.tb11669.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.