")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 16
Prevalence of Hypertension and Its Associated Factors Among Adults Living with HIV on Antiretroviral Treatment in Selected Public Hospitals in Addis Ababa, Ethiopia
Authors Haile M , Degelo T, Adilo TM, Adem FM, Gidisa B
Received 14 December 2023
Accepted for publication 8 March 2024
Published 21 March 2024 Volume 2024:16 Pages 109—122
DOI https://doi.org/10.2147/HIV.S447396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Meskelu Haile,1,* Tamiru Degelo,1,* Takele Menna Adilo,2 Fatimetu Mohammed Adem,2 Bedasa Gidisa3
1Providers Affairs and Quality Assurance Directorate, Ethiopian Health Insurance Service, Addis Ababa, Ethiopia; 2School of Public Health, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Public Health Department, Ethiopian Public Health Institute, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Meskelu Haile; Tamiru Degelo, Providers Affairs and Quality Assurance Directorate, Ethiopian Health Insurance Service, Addis Ababa, Ethiopia, Tel +251-966-817-727 ; +251-947-419-065, Email [email protected]; [email protected]
Introduction: Hypertension significantly increases the risk of heart, brain, and renal diseases and is one of the leading causes of death and disease worldwide. It is a major comorbidity among HIV-positive people. There have been limited attempts to detect hypertension and its related variables in patients receiving antiretroviral treatment, notably in Addis Ababa, Ethiopia. The current study intended to examine the incidence of hypertension and related variables among adults aged 18 and over living with HIV on ART at selected public referral hospitals in Addis Ababa, Ethiopia.
Methods: A hospital-based cross-sectional study was conducted on 411 HIV-positive individuals aged 18 on ART at Alert and St. Peter’s Specialized Hospitals. The research was conducted between December 15, 2021, and January 20, 2022, using an interviewer administered standardized questionnaire. Epi-Info version 7.0 was used to enter and code the collected data, which was subsequently exported to SPSS version 23.0. Bivariate and multivariate logistic regression models were used to identify associated variables.
Results: The prevalence of hypertension among people with HIV on ART was 37.5% (95% CI: 32.8– 42.5). Age groups 35– 50 years (AOR: 2.18; 95% CI: 1.13– 4.21), alcohol consumption (AOR: 5.58; 95% CI: 2.92– 10.65), no physical exercise (AOR: 2.35; 95% CI: 1.06– 5.21), family history of hypertension (AOR: 4.39, 95% CI: 2.48– 7.76), duration of ART (AOR: 3.13; 95% CI: 1.20– 8.12), low CD4 count (AOR: 1.87; 95% CI: 1.04– 3.37), and body mass index greater than or equal to 25 kg/m2 (AOR: 2.38; 95% CI: 1.33– 4.25) were factors associated with hypertension among HIV patients on ART.
Conclusion and Recommendation: According to this study, hypertension is prevalent in HIV-positive people. Factors related with hypertension in PLHIV include alcohol intake, lack of physical activity, age 35– 50 years, family history of hypertension, ART duration, low CD4 count, and BMI ≥ 25kg/m2. As a result, health education on the significance of keeping a healthy lifestyle can be effective in preventing and treating hypertension in HIV patients.
Keywords: Hypertension, PLHIV, ART, associated factors, Addis Ababa
Introduction
Hypertension is defined as an intermittent or prolonged increase in systolic or diastolic blood pressure over normal.1 It greatly raises the risk of heart, brain, and renal illness and is one of the top causes of mortality and disease globally.2 According to a WHO research, hypertension affects estimated 1.28 billion individuals aged 30–79 years globally, with the majority (two-thirds) residing in low- and middle-income countries (LMIC).2 Noncommunicable diseases (NCDs) cause 41 million deaths globally each year, with LMICs, including sub-Saharan Africa, accounting for nearly 75% of these deaths. Hypertension is leading to CVD responsible for over 17 million deaths each year.3
In sub-Saharan Africa (SSA), the dual burden of cardiovascular disease (CVD) and human immunodeficiency virus (HIV) infection is a public health problem. In 2020,4 around 37.7 million individuals worldwide were living with HIV/AIDS. With 25.6 million persons living with HIV, sub-Saharan Africa is the most afflicted area, accounting for two-thirds (2/3rd) of global total new HIV infections.4 Currently, there is an increasing burden of NCDs in the SSA’s general population, posing global HIV-related mortality has decreased substantially in the recent decade due to the increased use of ART, particularly SSA.5 Adults with HIV are increasingly living longer lives with a combined disease burden: HIV infection and chronic NCDs such as CVD.6 CVD is the leading cause of mortality worldwide,7 and it happens earlier and more frequently among persons living with HIV (PLHIV). In comparison to individuals who do not have HIV, PLHIV have a 50% greater risk of myocardial infarction and stroke, as well as a fourfold increased risk of sudden cardiac death. HIV-infected adults with hypertension have a higher risk of CVD and all-cause mortality (twofold higher risk) than HIV-uninfected adults with hypertension or HIV-infected adults with normal blood pressure.6,8,9
Hypertension is the leading cause of cardiovascular disease worldwide including among PLHIV. Hypertension in PLHIV is on the rise, and it is linked to ART use and age. Adults living with HIV on ART had a greater incidence of hypertension than HIV-uninfected persons. A recent meta-analysis of data from throughout the globe indicated that 35% of all HIV-infected individuals on ART had hypertension, in comparison to an estimated 30% of HIV-uninfected persons.6 Among ART-experienced persons over 50 years, more than half have hypertension.6,9,10
Hypertension affects 4.7–54.4% of PLHIV in high-income countries and 8.7–45.9% in low- and middle-income countries.11 According to studies done in Ethiopia, the prevalence of hypertension in PLHIV varied from 11.0% to 41.3%.12–14 Other studies have found that various risk variables, such as older age, male sex, a family history of hypertension, a longer duration of HIV infection, a low CD4 count, a high viral load, and a higher body mass index, contribute to the increased incidence of hypertension in HIV-infected people.15 Furthermore, the use of some drugs included in combination ART regimens has been linked to an increased risk of hypertension in people living with HIV, and drugs like Lopinavir/r well known for their metabolic issues.16 According to a meta-analysis of almost 44,000 HIV-infected individuals, the risk of hypertension was twice as high in ART-exposed patients as in treatment-naive patients.17
Several observational studies have revealed that PLHIV are more likely than HIV-negative persons to develop hypertension, with some studies indicating an increased incidence and others reporting a decreased prevalence. Inflammation, microbial translocation, renal disease, long-term ART exposure, and behavioral risks contribute to increased hypertension in PLHIV. In some circumstances, PLHIV may have a reduced incidence of hypertension due to advanced HIV illness, better blood pressure control due to more healthcare assistance, and lower levels of behavioral risk factors.17
Hypertension is prevalent among PLHIV in Ethiopia; however, studies on its causes and prevention are limited.11 Until now, the emphasis on risk reduction among ART patients has not been extended to the diagnosis, prevention, or management of hypertension. Furthermore, additional important factors such as recent ART adherence, prevention of opportunistic infections, recent WHO stage, salt consumption, family history of hypertension, history of diabetes mellitus, and comorbidities were not included in the current studies.11–13 Therefore, this study aimed to evaluate the prevalence of hypertension and its contributing factors among adults living with HIV receiving ART at Alert and St. Peter’s Specialized Hospitals in Addis Ababa, Ethiopia. This finding might help determine the prevalence of hypertension and the variables that contribute to it.
Materials and Methods
Study Design and Setting
A hospital-based cross-sectional research was done at Alert and St. Peter’s Specialized Hospitals from December 15, 2021, to January 20, 2022, among patients visiting the two referral-specialized hospitals’ ART clinics. These public hospitals are located in the Kolfe Keranio and Gulele sub-cities of Addis Ababa, the capital city of Ethiopia. Two of the seven government-owned tertiary hospitals in Addis Ababa receive referrals from around the country. They have been serving about 9777 PLHIV; of these, Alert Hospital serves 7484, and SPSH serves 2293.
Population of the Study
The source population included all HIV-positive people who had follow-up appointments at hospital ART clinics. Adult HIV-infected patients receiving HIV care in hospitals during the research period who met the inclusion criteria comprised the study population. The study included all persons living with HIV over the age of 18 years who had been taking ART for at least 6 months prior to the study period. The trial excluded pregnant women and individuals who were very unwell or unable to respond to therapy.
Sample Size Determination
The sample size to calculate the prevalence of hypertension in this study was determined using a study on the prevalence of hypertension among adults living with HIV who received ART at Debre Markos Hospital, which was 41.3%13 at 95% confidence interval and 5% margin of error. Given the non-response rate, the total sample size was 411 people. The sample size to describe risk factors associated with HTN was calculated using Epi Info version 7.0 statistical software with 95% CI, 5% margin of error, and 80% statistical power, taking age, physical activity, and antiretroviral therapy regimens as the major statistically significant variables13 into account. The highest sample size (n = 174) was reached by examining the proportion of hypertension in unexposed people (ie, no physical activity), with an AOR of 2.72.13 Finally, the projected sample size for the second aim was lower than that for the first. As a result, the largest sample size (411) was determined to be the minimum required sample size for this investigation.
Sampling Procedures
The study was carried out at two tertiary institutions, which included 28.6% of all referral hospitals in Addis Ababa, using a basic random sample procedure with a lottery system.
A survey of the two hospitals showed that the total number of patients attending ART clinics in the last 6 months (July–November 2021) was 9777; of these, 7484 and 2293 patients were attending Alert and SPSH ART clinics, respectively. However, the monthly average patient flow to the ART clinic during the last 6 months was 3259 which was because patients were attending the clinic every other month to receive ART services for Covid-19 protocols. Among these, 411 participants were selected for this study. The sample size was allocated to the two selected hospitals using a probability proportional to the size. Participants were chosen via systematic random selection. By dividing the total number of HIV-positive people getting ART at the selected hospitals by the final sample size, the sampling interval (kth) was calculated ( ). The initial sample was drawn at random from the attending patients, and every eighth sample was drawn for data collection until the requisite sample was received from the research participant for daily follow-ups.
). The initial sample was drawn at random from the attending patients, and every eighth sample was drawn for data collection until the requisite sample was received from the research participant for daily follow-ups.
Data Collection Tools and Procedure
The data was gathered via a standardized questionnaire delivered by an interviewer. The questionnaires were adopted and modified from prior local investigations.12,13,18–21 To measure blood pressure, the patient’s arm was bare and supported, a cuff size appropriate for the patient arm was used (the length of the bladder should be 80%, and the width of the bladder should be at least 40% of the circumference of the upper arm), the lower edge of the cuff was 3 cm above the elbow crease, no talking or moving before or during the measurement, legs uncrossed, feet flat on the floor, and the patient was given an adequate rest for 5 min. An average of at least two blood pressure readings obtained 5 min apart were utilized in the study.22
All anthropometric measures were taken twice, with the average being recorded. The respondents’ weights were measured with a conventional beam balance, and the scale was verified and calibrated to zero before each measurement. After removing heavy clothing, the respondents’ weights were measured and recorded to the closest 0.1KG. A standard scale was used to assess the respondents’ height. The participants took off their shoes and stood in the horizontal plane. The occiput, shoulder, buttocks, and heels all made contact with the measuring board, and height was measured to closest 0.1 cm.
While the patient was breathing and standing, the waist circumference was measured at midway between the lowest margin of the last perceptible rib and the top iliac crust and classified according to WHO guidelines. Hip circumference was measured using tape in a horizontal plane, contacting but without squeezing the skin, at the place producing the largest circumference across the buttocks. The waist-to-hip ratio was computed by dividing the mean waist circumference by the mean hip circumference.
Data Quality Control
To assure data quality, the tool was created in English first, then translated into Amharic, and finally back to English. The data collectors were trained for 2 days on how to use the data gathering instrument and methodologies. At Zewditu Memorial Hospital, the data collecting instrument was pretested on 5% of the total sample size. Data were acquired throughout ART care follow-up by interviewing patients who attended Alert and St. Peter’s Specialized Hospitals’ ART clinics. Clinical data was also gathered via analyzing patient charts. As data collectors, four bachelor’s degree nurses from Alert and St. Peter’s Specialized Hospitals participated. The primary investigators were in charge of daily supervision. Furthermore, study team members reviewed the acquired data for completeness and consistency during data administration, storage, and analysis.
Study Variables
Dependent Variable
Hypertension in adults living with HIV on antiretroviral therapy.
Independent Variables
The sociodemographic factors included age, sex, residence, religion, occupation, monthly income, educational status, and marital status.
Physical activity, cigarette smoking, alcohol drinking, khat chewing, and food intake (fruit and vegetables and salt consumption) were all behavioral variables.
Body mass index, waist circumference, and waist-to-hip ratio are anthropometric parameters.
Clinically related factors included family history of hypertension, CD4 count, viral load, ART adherence (duration and regimens), history of diabetes mellitus, WHO stage, opportunistic infection OI and prophylaxis, and comorbidity diseases.
Operational Definitions
Hypertension: It is defined as either a systolic blood pressure (SBP) of 140 mmHg or a diastolic blood pressure (DBP) of 90 mmHg or both. It is separated into two stages: Stage I (SBP 140–159 mmHg or DBP 90–99 mmHg) and Stage II (SBP >160 mmHg or DBP >100 mmHg).1
Body mass index (BMI): It is a statistical indicator that estimates body fat in boys and females of any age using a person’s weight and height. It is computed (weight/height squared) and classed as underweight (18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), or obese (>30 kg/m2).12,23
Waist circumference (WC): The WHO classifies WC as low risk (94 cm) for males and 0.80 cm for females, high risk (94–102 cm) for males and (80–88 cm) for females, and extremely high risk (>102 cm) for males and (>88 cm) for females.
Waist-to-hip ratio (WHR): A normal WHR is 0.90 or less for males and 0.85 or less for females, according to WHO categorization. Abnormal waist–hip ratio (WHR) was defined as WHR > 0.9 in men and WHR > 0.85 in women.
Family History of Hypertension was characterized as a history of hypertension in the respondent’s father, mother, or full brother or sister.
Physical activity: A person engaged in any physical exercise, including walking, for more than 30 min each day. Low = 30 min daily total physical activity (TPA), moderate = 30–59 min daily TPA, and high = >60 minutes daily TPA.18
Cigarette Smoker: A research subject is deemed a cigarette smoker if he or she is presently smoking or has previously smoked cigarettes on a daily or less frequent basis.11
Khat chewer: A khat chewer is a research participant who consumes khat once in the 30 days before the data collecting period in this study.11
Alcohol consumption: According to the WHO categorization, it was classed as low (1 alcoholic beverage per week), moderate (1–21 alcoholic beverages per week), or high to excessive (>21 alcoholic beverages per week).23
Sufficient fruit and vegetable: The intake of a day's history was utilized and 4–7 days of fruit and vegetable consumption per day was deemed enough.20
Viral load is the number of HIV copies per mL in the plasma.24
Comorbid disease: a chronic disease with a confirmed diagnosis of the disease other than HIV infection24 like hypertension, Cardiovascular disease, mental health disorders, TB, etc.
Opportunistic infections (OIs) occur more frequently and with greater severity in those with weaker immune systems, including HIV patients.25
Adherence to ART: An adult’s recent adherence to ART is classified as poor when he or she takes less than 85% of the dose, fair when he or she takes 85–94% of the dose, and excellent when he or she takes 95% or more of the dose.24
Data Processing and Analysis
The acquired data was reviewed for correctness and cleaned many times before being input into a computer with the Epi-Info version 7:0 software and exported to SPSS version 23.0 for statistical analysis. Cross-tabulation findings were used to manage missing values. The model’s fitness was evaluated using the Hosmer-Lemeshow test. To investigate the relationship between dependent and independent variables, binary logistic regression analysis was performed. To reduce potential confounders, all variables (p-value 0.25) were included in the multivariable model. The variance inflation factor (VIF) test was used to measure the correlation between independent variables in a multicollinearity test. Using multivariable logistic regression, odds ratios (OR) and 95% confidence intervals (CI) were calculated to assess the strength of the link and identify components related with hypertension. With p-values of 0.05, all factors were declared significant predictors of hypertension using multivariable logistic regression. Finally, the study’s findings are presented in text, graphs, and tables.
Ethical Consideration
The study was carried out after receiving ethical approval from Saint Paul’s Hospital Millennium Medical College’s (SPHMMC) Institutional Review Board (IRB) that the research was done in accordance with relevant guidelines and regulations (ethics approval reference number PM23/475), and all the processes were performed in accordance with the Declaration of Helsinki.
Permission and support letters were then written to Alert and St. Peter’s Specialized Hospitals from SPHMMC. After discussing the research’s aims, each study participant provided informed consent to indicate their desire to participate. Respondents unwilling to participate in the study were excluded. Respondents were informed that all collected data would be kept confidential and used only for intended purposes. Coding was used instead of a personal identifier to ensure data security and confidentiality.
Results
Socio Demographic Characteristics of the Participants
The research had 405 participants out of a total of 411 study participants sampled, with a response rate of 98.5%. Of these, 158 (39.0%) were male and 258 (61.0%) were female. The mean age of the respondents was 44.27 (±10.70) years, with a minimum of 18 years and a maximum of 81 years. Regarding age distribution, 64 (15.8%) were in the age range of 18–34 years, 236 (58.3%) of them were at the age interval of 35–50 years and 105 (25.8%) of them were above 50 years old. Approximately 145 (35.1%) had primary level of education and only 63 (15.6%) diploma and above level. Respondents were predominantly from urban 392 (96.8%). The respondents reported that their estimated monthly income of less than 2000 Ethiopian Birr was about 207 (51.1%) and greater than 5000 were only 72 (17.8%) (Table 1).
 |
Table 1 Socio-Demographic Characteristics of the Study Participants Among HIV Positive Adults on ART at Alert and SPSH, AA Ethiopia, December 15/2021-January 2022 (n = 405) |
Behavioural Characteristics of Respondents
Fifty-one (12.6%) of participants were cigarette smokers. One hundred and thirteen (27.9%) of participants were alcohol consumers, and 35 (8.6%) were khat chewers. Only sixty-two (15.3%) of respondents had a practice of doing regular physical exercise. Approximately 139 (34.3%) and 80 (19.8%) participants reported that they did not consume fruits and vegetables per week, respectively (Table 2).
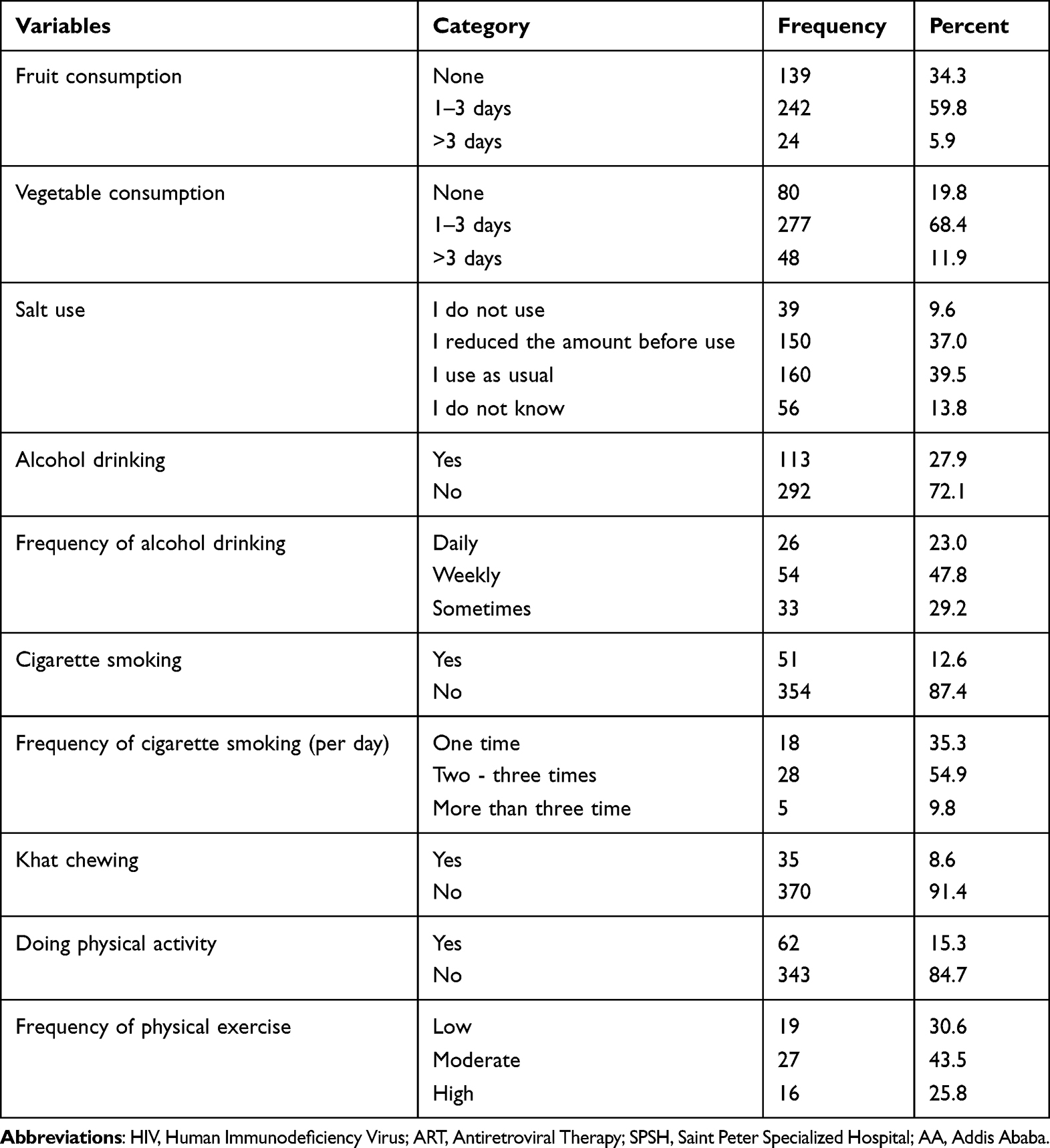 |
Table 2 Behavioral Characteristics of Respondents Among HIV Positive Adults on ART at Alert and SPSH, AA Ethiopia, December 15/2021-January 2022 (n = 405) |
Clinical Related Characteristics of Respondents
Approximately 62 (15.3%) of individuals had a history of hypertension. Almost one-third of the 131 respondents (32.3%) reported a family history of hypertension. The majority 332 (82%) of participants were in WHO stage I. More than one-fourth (28.1%) had fewer than 350 cells/mm3 CD4 counts, the majority 352 (86.9%) had undergone ART for 5 years or more, and around three-quarters (76.3%) had received OI prophylaxis. Diabetes mellitus affected 44 (10.9%) of the patients. The majority of subjects (92.1%) and less than one-tenth (7.9%) reported good and fair/poor ART adherence, respectively. The majority of patients (83.0%) did not acquire comorbidities. Participants in the research had a body mass index of less than 25, and document evaluation revealed that 214 (52.8%) of responders had at least one form of opportunistic illness, with TB accounting for 104 (47.3%). Two-fifths (39.5%) of trial participants were on the HAART regimen of TDF+3TC+EFV, one-fourth (26.4%) were on AZT/3TC/NVP, one-fifth (20.5%) were on TDF/3TC/NVP, and 13.6% were on AZT/3TC/EFV (Table 3).
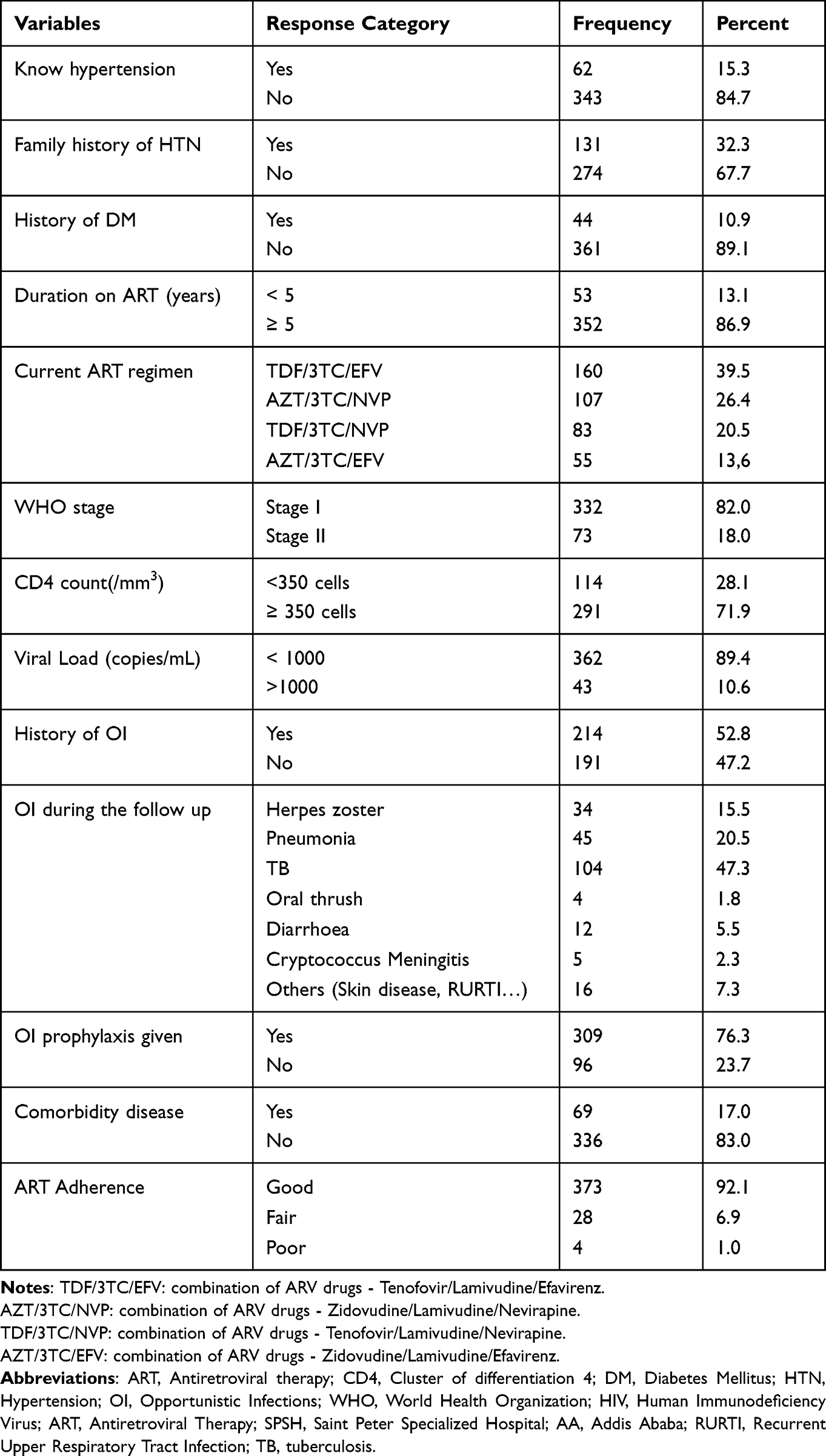 |
Table 3 Clinical Related Characteristics of HIV Positive Adults on ART at Alert and SPSH, AA Ethiopia, and December 15/2021-January 2022 (n = 405) |
Anthropometric Related Characteristics of Respondents
In terms of anthropometric parameters, the participants’ mean (±SD) weight was 62.7 (±13.007) kg. The mean (±SD) height was 1.62 (±0.087) meter. The respondents’ mean (±SD) body mass index (BMI) was 23.61 (±4.53) kg/m2. One hundred and one (24.9%) and fifty (12.3%) of those polled were overweight or obese. Approximately 152 (37.5%) of respondents had a large waist circumference, whereas 227 (56.0%) had a large waist-to-hip ratio (Table 4).
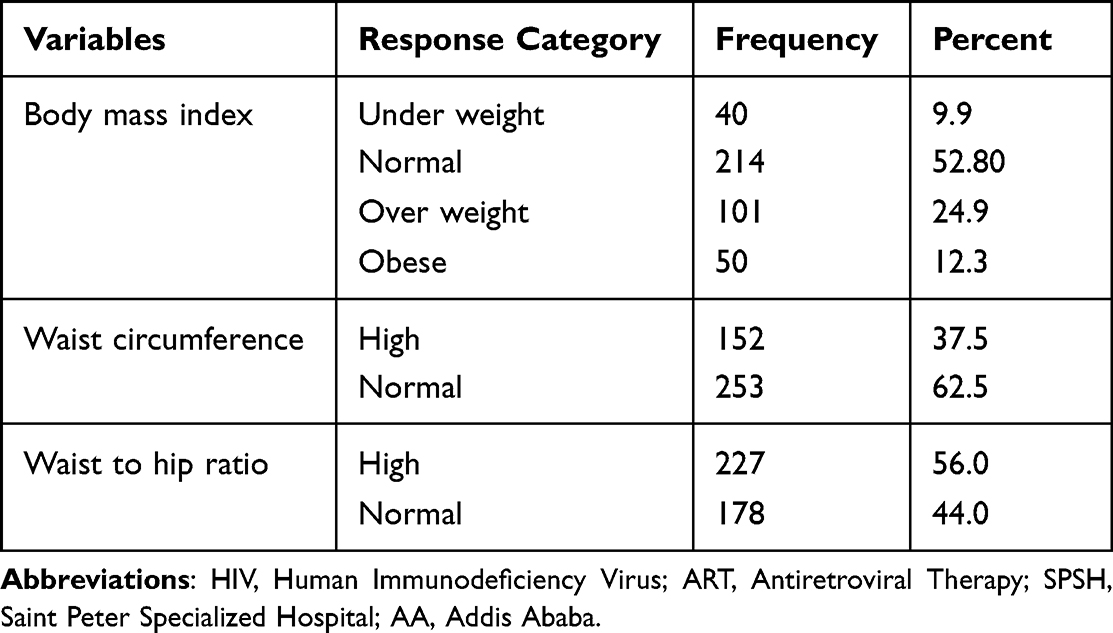 |
Table 4 Anthropometric-Related Characteristics of HIV Positive Adults on ART at Alert and SPSH, AA Ethiopia, and December 15/2021-January 2022 (n = 405) |
Prevalence of Hypertension Among Adults Living with HIV on ART
The prevalence of hypertension among study participants was determined to be 152 (37.5%), with a 95% confidence interval (CI) of 32.8–42.5. SBP and DBP mean values were 125.64 mm hg ±21.30 SD and 78.38 mm hg ±12.59 SD, respectively. Ninety (22.2%) of the hypertensive people detected did not aware they had hypertension (new cases). During the data collection period, about 62 (15.3%) of hypertensive patients reported using antihypertensive medications (Figure 1).
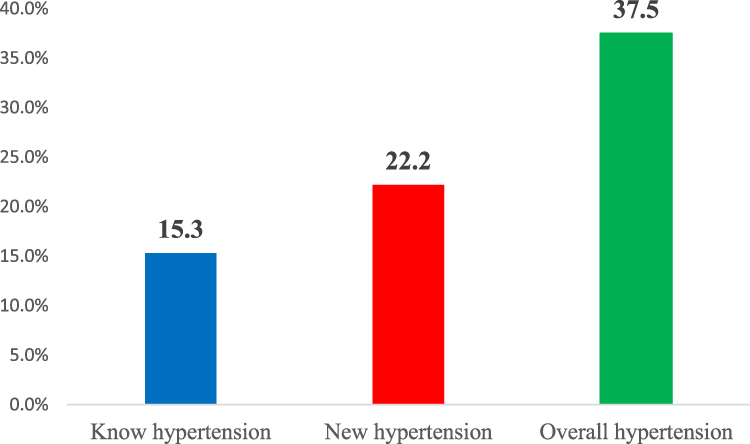 |
Figure 1 Prevalence of hypertension among Adults living with HIV on ART at Alert and SPSH in AA, Ethiopia, 2022(N = 405). |
Associated Factors of Hypertension Among Adults Living with HIV
Variables such as family history of hypertension and age; alcohol consumption and absence of physical exercise; duration of ART, low CD4 count, and BMI were significantly associated with hypertension in the multivariable analysis.
As expected family history of hypertension was found to be 4.39 (AOR=4.39, 95% CI (2.48–7.76)) times more likely to develop hypertension than non-family history of hypertension. Respondents in age group (35–50) years were 2.18 (AOR=2.18; 95% CI: 1.13–4.21) times more likely to develop hypertension compared to those in the age group (18–34) years.
Alcohol users were 5.58 (AOR=5.58, 95% CI 2.92 −10.65) times more likely to develop hypertension than non-drinkers, according to this study. Participants who did not engage in regular physical activity had a 2.35-fold increased risk of hypertension compared to those who did (AOR=2.35, 95% CI: 1.06–5.21).
In addition, ART duration was significantly associated with hypertension. Participants who had been receiving ART for ≥5 years were 3.13 times more likely to develop hypertension than their counterparts (AOR: 3.13, 95% CI: 1.20–8.12).
Furthermore, participants with a low CD4 count (350 cells/mm3) were 1.87 times (87%) more likely to develop hypertension than those with a high CD4 count (350 cells/mm3). Finally, individuals with a BMI greater than or equal to 25 (25 kg/m2) had a 2.38 (AOR=2.38, 95% CI: 1.33–4.25) higher risk of hypertension than those with a BMI of less than 25.
However, in the bivariate analysis, marital status, cigarette smoking, current ART regimen, history of opportunistic infections, comorbidity disease, WC, and WHR were significantly associated with hypertension, but not in the multivariate logistic regression analysis (p>0.05) (Table 5).
 |
Table 5 Bi-Variable and Multivariable Analysis of Factors Associated with Hypertension Among HIV Positive Adults on ART at Alert and SPSH in AA, Ethiopia, 2022 (N = 405) |
Discussion
The purpose of this study was to look at the prevalence of hypertension and its risk factors in adults living with HIV using ART. In this study, the prevalence of hypertension among PLHIV was 37.5% (95% CI: 32.8–42.5).
The prevalence of this study is in line with the findings of Debre Markos Hospital Northeast Ethiopia (41.3%),13 Brazilian Society of Tropical Medicine (35.9%)%,26 and United States—Medical Monitoring Project Brief Report (42.4%).27 This prevalence is higher than that reported in previous studies conducted in South Ethiopia (11%), North West Ethiopia (14.0%), Bahir Dar (14.1%), North East Ethiopia (29.7%), South Africa (11.8% in 2005,9.5% in 2008, and 14.3% in 2017), Tanzania (12.5%), Uganda (29%), and Senegal (11% to 22%),11,12,18,19,28–31 respectively. This might be due to differences in the sample size and lifestyle factors, such as smoking. The observed difference might potentially be explained by differences in the length of HIV infection, the kinds and duration of ART exposure, or differences in the age distribution of individuals in prior and current research.
However, this incidence among PLHIV was lower than the 71%32 found in a survey of the rural black population of Mthatha Town, South Africa. This disparity might be attributed to differences in the socioeconomic position of respondents between the two research populations, behavioural characteristics of study participants, and the blood pressure cutoff point.
The current study found that alcohol consumption, family history of hypertension, body mass index (BMI) of 25 kg/m2, long duration of ART, age, lack of physical activity, and low CD4 count were all significantly associated with hypertension in Adults living with HIV on ART.
Respondents with a family history of hypertension were 4.39 (AOR: 4.39, 95% CI: 2.20–7.08) times more likely than their counterparts to acquire hypertension. This is supported by studies conducted in the northeast19 and South Ethiopia.23 One probable explanation is that the family has the same genes that predispose a person to high blood pressure and stroke. Furthermore, this might be because family shared similar interests such as feeding habits, exercise, and alcohol use, all of which can be harmful to one’s health.
This study found that age was a factor in hypertension. Participants aged 35–50 years were 2.18 (AOR=2.18, 95% CI: 1.13–4.21) times more likely to develop hypertension than those aged 18–34. This discovery is consistent with research findings from Debre Markos Referral Hospital, Bahir Dar City, and North East Ethiopia16,18,19 and outside the country in Kenya, South Africa, Cameron, GA South Metropolis, and Brazil.31–36 This is explained by the fact that aging causes a loss of vessel function due to stiffening of the arterial vasculature, and vascular changes include advanced reductions in viscoelastic properties of vessels, progressive atherosclerotic arterial disease, and hypertrophy/sclerosis of muscular arteries and arterioles, which narrow the vessel wall and increase resistance to blood pressure.13
Alcohol use was another factor of hypertension in this research. When compared to individuals who did not use alcohol, the risks of getting hypertension were 5.58 (AOR: 5.58, 95% CI 2.92–10.65) times higher. This result was supported by studies conducted in South Ethiopia,9 Kenya,33 and South Africa.31 This might be due to residence (urban) and exposure to risk factors, such as the harmful use of alcohol and the timely increase in alcohol consumption. This may also be due to cultural differences, differences in sample size, and educational status.
Another predictor of hypertension was regular physical activity. Participants in the study who did not engage in regular physical activity were 2.35 times more likely to acquire hypertension than their counterparts (AOR: 2.35, 95% CI: 1.06–5.21). A research completed at the Debre Markos Referral Hospital in North East Ethiopia aided the current investigation.13 This might be attributed to the significant buildup of fat in tissues and organs, which affects hemodynamic pathways and leads to hypertension in people who do not engage in regular exercise.
Furthermore, among adults living with HIV, the duration of ART was substantially related with hypertension. Participants who had been undergoing ART for 5 years or more were 3.13 times more likely than their peers to develop hypertension (AOR: 3.13, 95% CI: 1.20–8.12). This finding is consistent with those of other studies conducted in South, Northwest, and East Ethiopia.9,11,13,18 This link between ART length and hypertension may be mediated directly by changes in endothelial function, or it may be attributed to longevity as well as age-related comorbidities such as ART-related changes in body composition and weight gain.6,8,19,37
A low CD4+ T cell count was shown to be substantially linked with hypertension in HIV-positive individuals in the current investigation. Participants with a CD4+ T-cell count of 350 cells/mm3 were 87% more likely than those with a CD4+ T-cell count of 350 cells/mm3 to develop hypertension (AOR: 1.87, 95% CI: 1.04–3.37). This finding is consistent with studies conducted in North East Ethiopia19 and Tanzania.29 Low CD4 cell count is related with chronic immunological activation and persistent microbial translocation, which might explain this connection.14
Finally, higher BMI was linked to a higher incidence of hypertension in HIV-positive individuals. Participants with a BMI of 25 kg/m2 were 2.38 times more likely than their counterparts to develop hypertension (AOR=2.38, 95% CI: 1.33–4.25). This finding is comparable to that of a study conducted at Debre Markos Referral Hospital, Northeast Ethiopia, South Ethiopia, GA South Metropolis, Rural Black Population of Mthatha Town, South Africa, and Brazil.13,19,23,32,35 Obesity in HIV/AIDS patients may be related with significant weight gain during HAART and should be avoided. This might be due to changes in dietary habits, a lack of activity, or other factors.
This study has its own strengths; it used the standard tool to follow the WHO STEP-wise approach for chronic noncommunicable disease risk factor surveillance among the study population, and the study’s validity and reliability improved, providing strong evidence on the level and significant determinants of the concerned bodies.
There are certain limitations to this study, which are mostly connected to the nature of the cross-sectional study design, which did not demonstrate the cause-and-effect connection of factors. The performance of the research participants’ behavioral practices was not observed since their behavioral practices were gathered via an interviewer-administered structured questionnaire. As a result, recollection bias and social desirability bias might have occurred. Information on lipid profile, renal function, and other laboratory data were not gathered due to resource constraints. An average of at least two blood pressure readings obtained 5 min apart was utilized to measure hypertension, so this may overestimate the prevalence in the study.
Conclusion
More than one-third of the research participants developed hypertension, according to the current study. Alcohol use, lack of physical activity, age 35–50 years, family history of hypertension, length of ART, low CD4 count, and body mass index 25kg/m2 were found to be risk factors for hypertension among HIV/AIDS patients. The emphasis should be on teaching individuals about the use of lifestyle modifications, alcohol consumption reduction, suitable regular physical activity, and weight loss promotion. To investigate the effects of ART on hypertension, prospective or long-term trials are necessary.
Abbreviations
AIDS, Acquired Immune Deficiency syndrome; AOR, Adjusted odds ratio; ART, Anti-retroviral therapy; ARV, Antiretroviral; ATV, Atazanavir; AZT, Zidovudine; BMI, Body mass index; CVDs, Cardiovascular diseases; CD4, Cluster of differentiation 4; CI, Confidence Interval; COR, Crude odds ratio; DM, Diabetes Mellitus; DBP, Diastolic blood pressure; D4T, Stavudine; EFV, Efavirenz; FMOH, Federal Ministry of Health; HAART, Highly Active Anti-viral Therapy; HIV, Human Immunodeficiency Virus; NCDs; Non-communicable diseases; OR, Odds ratio; OI, Opportunistic infection; PLHIV, People living with Human Immunodeficiency Virus; PH, Public Health; SPHMMC, St. Paul’s Hospital Millennium Medical College; SPSH, Saint Peter’s Specialized Hospital; SSA, Sub-Saharan Africa; SBP, Systolic blood pressure; SPSS, Statistical Package for Social Sciences; TPA, Total physical activity; WC, Waist Circumference; WHO, World Health Organization; WHR, Waist-to-hip ratio.
Data Sharing Statement
The datasets used in this work are accessible upon reasonable request from the corresponding author.
Acknowledgments
We would like to thank St. Paul’s Hospital Millennium Medical College (SPHMMC) for funding this study and giving the ethical clearance. We would also like to thank all the data collectors and study participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Dagnaw WW, Yadeta D, Feleke Y, Kebede T. Ethiopian national guideline on major NCDs 2016 guidelines on clinical and programmatic management of major non communicable diseases; 2016.
2. Risk NCD, Collaboration F. Articles worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants; 2021;398.
3. World Health Organization. Non-communicable diseases; 2021. Available from: https://who.int/news-room/factsheet/detail/noncommunicable-diseases.
4. Sheet F. FACT SHEET 2021 Global HIV statistics; 2021; 1–6.
5. Frank TD, Carter A, Jahagirdar D, et al. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980 – 2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the global burden of diseases, injuries, and risk factors study 2017. The Lancet HIV. 2019;6:831–859.
6. Feinstein MJ, Hsue PY, Bloomfield GS, et al. HHS Public Access; 2021.
7. Roth GA, Abate KH, Abay SM Global Health Metrics Global, regional, and national age-sex-specific mortality and life expectancy, 1950 – 2017: a systematic analysis for the Global Burden of Disease Study 2017. 2018:1980–2017.
8. Shah ASV, Stelzle D, Lee KK, et al. Europe PMC funders group global burden of atherosclerotic cardiovascular disease in people living with the human immunodeficiency virus: a systematic review and meta-analysis. Circulation. 2019;138(11):1100–1112.
9. Fahme SA, Bloomfield GS, Peck R Hypertension in HIV-Infected Adults: novel Pathophysiologic Mechanisms; 2018:44–55.
10. Peck RN, Shedafa R, Kalluvya S, et al. Hypertension, kidney disease, HIV and antiretroviral therapy among Tanzanian adults: a cross-sectional study. BMC Med. 2014;12(125):1–11. doi:10.1186/s12916-014-0125-2
11. Nguyen KA, Peer N, Mills EJ, et al. Burden, determinants, and pharmacological management of hypertension in HIVpositive patients and populations: a systematic narrative review. AIDS Rev. 2015;17(2):83–95. PMID: 26035166.
12. Lukas K, Markos E, Belayneh F, Habte A, Torpey K. The magnitude of hypertension and associated factors among clients on highly active antiretroviral treatment in Southern Ethiopia, 2020:A hospital-based cross-sectional study. PLoS One. 2021;16(10):e0258576. doi:10.1371/journal.pone.0258576
13. Id AG. Hypertension among people living with human immunodeficiency virus receiving care at referral hospitals of Northwest Ethiopia. PLoS One. 2020:1–13. doi:10.1371/journal.pone.0238114
14. Sewale Y, Afenigus AD, Haile D, Shiferaw WS. Magnitude of hypertension and associated factors among human immunodeficiency virus positive adults receiving anti-retroviral therapy at debre markos referral hospital, Northwest, Ethiopia. HIV AIDS. 2020;12:629–637. PMID: 33116925; PMCID: PMC7588266. doi:10.2147/HIV.S280630
15. Fiseha T, Belete AG, Dereje H, Dires A Hypertension in HIV-infected patients receiving antiretroviral therapy in Northeast Ethiopia; 2019.
16. Jamieson L, Njc I, Fox MP, et al. And control of hypertension among HIV- positive adults on antiretroviral treatment in public sector treatment programs in South Africa; 2018:1–19.
17. Nduka CU, Stranges S, Sarki AM, Kimani PK, Uthman OA. Evidence of increased blood pressure and hypertension risk among people living with HIV on antiretroviral therapy: a systematic review with meta-analysis. Journal of Human Hypertension. 2016;30(6):355–362. doi:10.1038/jhh.2015.97
18. Davis K, Perez-Guzman P, Hoyer A, et al. Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies. BMC Med. 2021;19(105):1–6. doi:10.1186/s12916-021-01978-7
19. Getahun Z, Azage M, Abuhay T. Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city. Ethiopia. 2020;10:1–12.
20. Kebede B, Ayele G, Haftu D, Gebremichael G The prevalence and associated factors of hypertension among adults in Southern Ethiopia; 2020.
21. Stepwise TWHO. The WHO STEPwise approach to chronic disease risk factor surveillance (STEPS); 2015.
22. Ababa A Guidelines on clinical and programmatic management of major non communicable diseases; 2016.
23. Debiso AT. Incidence and predictors of systemic hypertension among cohort of HIV / aids infected patients in health facilities of South Ethiopia; 2020:47–63. Available from: 10.4236/aid.2020.102005.
24. Federal Ministry of Health. National comprehensive HIV prevention, care and treatment training for health care providers. Participant manual; 2018:1–123.
25. Division of HIV/AIDS prevention, national center for HIV/AIDS, viral hepatitis, STD, and TB prevention, centers for disease control and prevention. Available from: https://www.cdc.gov/hiv/basics/livingwithhiv/opportunisticinfections.html.
26. Costa AN, Val F, Macedo ÁE, Cubas-vega N, Vinicius M, Lacerda G. Major article increased prevalence of hypertension among people living with HIV: where to begin ?; 2020:1–6.
27. Olaiya O, Weiser J, Zhou W, Patel P, Bradley H. Hypertension among persons living with HIV in medical care in the United States — medical monitoring; 2014:1–5.
28. Lubega G, Mayanja B, Lutaakome J, et al. Prevalence and factors associated with hypertension among people living with HIV / AIDS on antiretroviral therapy in Uganda; 2021.
29. Njelekela M, Muhihi A, Aveika A, et al. Prevalence of hypertension and its associated risk factors among 34, 111 HAART Na \ ve HIV-infected adults in dar es Salaam, Tanzania; 2016.
30. Africa W, Seydi M, Doye IN, et al. Increasing prevalence of hypertension among HIV-positive and negative adults in Senegal; 2018;1–14.
31. Chiwandire N, Zungu N, Mabaso M, Chasela C. Trends, prevalence and factors associated with hypertension and diabetes among South African adults living with HIV, 2005 – 2017; 2021;1–14.
32. Sharma JR, Mabhida SE, Myers B, et al. Prevalence of hypertension and its associated risk factors in a rural black population of Mthatha town, South Africa; 2021.
33. Mbuthia GW, Magutah K, Mcgarvey ST. HIV Patients. Int J Hyperten. 2021;2021:8. doi:10.1155/2021/5544916
34. Ephraim RKD, Sakyi SA, Fondjo LA, Afrifa J, Agyeman P, Darko P. Determinants of isolated systolic hypertension among HIV / AIDS on highly active antiretroviral therapy: a cross sectional study in the GA South metropolis; 2018:360–364.
35. Arruda Junior ER, Lacerda HR, Moura LC, et al. Risk factors related to hypertension among patients in a cohort living with HIV/AIDS. Braz J Infect Dis. 2010;14(3):281–287. PMID: 20835513. doi:10.1590/s1413-86702010000300014
36. Dzudie A, Hoover D, Kim H, et al. Hypertension among people living with HIV / AIDS in Cameroon: a cross-sectional analysis from central Africa international epidemiology databases to evaluate AIDS. PLOS ONE. 2021:1–17. doi:10.1371/journal.pone.0253742
37. van Zoest RA. Ageing with HIV: from pathogenesis to policy; 2019.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.