")
Back to Journals » Research and Reports in Urology » Volume 15
Prevalence and Management of Spermatic Cord Torsion (SCT): A Five-Year Review in Souro Sanou University Hospital of Bobo-Dioulasso (Burkina Faso)
Authors Ouattara A , Paré AK, Yé D, Traoré MZ, Simporé M, Rouamba M, Kaboré FA, Kambou T
Received 30 May 2023
Accepted for publication 8 August 2023
Published 18 August 2023 Volume 2023:15 Pages 381—385
DOI https://doi.org/10.2147/RRU.S419786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Adama Ouattara,1 Abdoul-Karim Paré,1 Delphine Yé,1 Mamadou Z Traoré,1 Mohamed Simporé,1 Mickael Rouamba,1 F Aristide Kaboré,2 Timothée Kambou1
1Division of Urology, Souro Sanou University Teaching Hospital, Bobo-Dioulasso, Burkina Faso; 2Division of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Correspondence: Adama Ouattara, Division of Urology, P.O Box 1465, Bobo-Dioulasso, Burkina-Faso, Email [email protected]
Introduction: Spermatic cord torsion (SCT) is a rare urological emergency that can jeopardize the fertility of the patient. Our study aimed to investigate the epidemiological, diagnostic and therapeutic aspects of SCT in Souro Sanou University Teaching Hospital.
Materials and Methods: This was a descriptive cross-sectional study with retrospective data collection from January 1, 2017, to December 31, 2021, in the emergency surgical and urology division of Souro Sanou University Hospital.
Results: The annual frequency of SCT was 4.4 patients/year. The mean age of the patients was 17.82 ± 6.74 years. Painful swelling of the hemi-scrotum was the main presenting symptom. The torsion involved the left spermatic cord in 50% of cases and both spermatic cords in 5% of cases. The mean time of symptoms before presentation was 78.8 hours ± 153 hours. Only 27.3% of patients presented before the 6th hour after the onset of pain. The average time from presentation to surgical intervention was 5.6 hours ± 5 hours. Orchiectomy was performed in 11 patients (47.8%). The average hospital stay was 3.1 ± 1.4 days.
Conclusion: SCT is a rare urological emergency. The prognosis depends on the duration and degree of torsion. A high orchidectomy rate can be observed with a delay in presentation.
Keywords: spermatic cord torsion, emergency, orchiectomy
Introduction
Spermatic cord torsion is the rotation of the testicle around the axis of spermatic cord.1 It is a surgical emergency involving the vessels running through the spermatic cord leading to a lack of blood supply to the testicle, hence the old name of torsion of the testicle.2 It is a rare but serious urological emergency with an approximate frequency of 1 in 4000 in subjects under 25 years of age. Any delay in diagnosis or treatment can compromise the vital and functional prognosis of the testis.3 Our study aims to contribute to improving the management of Spermatic cord torsion at Souro Sanou University Hospital of Bobo-Dioulasso.
Materials and Methods
This was a descriptive cross-sectional study with retrospective data collected over 5 years from January 1, 2017, to December 31, 2021. It consisted of all the patients admitted for torsion of the spermatic cord through urology clinic and emergency surgery departments of the Sourô Sanou University Hospital of Bobo-Dioulasso during the study period. Epidemiological, diagnostic and therapeutic variables were studied. This study complies with the Declaration of Helsinki and was performed according to local ethics committee approval under number of reference: 005/2022. Written informed consent was obtained from the father of a minor patient for publication of accompanying images (Figure 1).
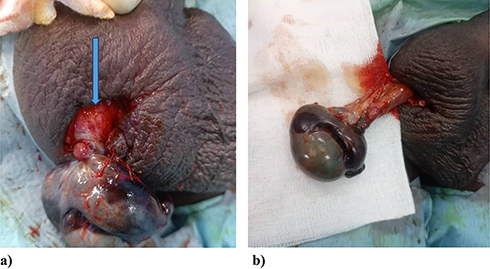 |
Figure 1 Twisted testis after scrototomy with turns, indicated by blue arrow (a). Unsatisfactory recolouring after spermatic cord detorsion (b). |
Results
The annual incidence of spermatic cord torsion is 4.4 patients/year with a minimum of 3 patients and a maximum of 7 patients. Figure 2 represents the distribution of spermatic cord torsion cases by year.
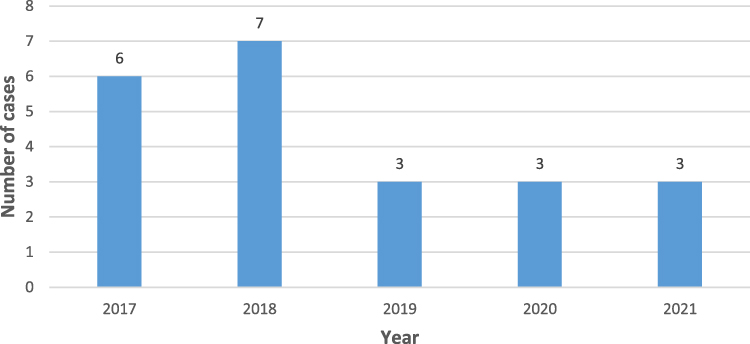 |
Figure 2 Distribution of cases of spermatic cord torsion per year. |
The mean age of the patients was 17.82 ± 6.7 years with extremes of 1 year and 33 years. Sixteen patients (72.72%) were between 13 and 25 years old and 82% were students. Seven patients (31.8%) presented directly to the university teaching hospital and fifteen patients (68.2%) were referred from other health facilities. In addition, 13.7% of patients were brought by their parents.
Testicular swelling with pain was the main reason for presentation in all the patients. The symptomatology was in the right side in 10 patients (45.0%), left in 11 patients (50.0%) and bilateral in one patient (5.0%). Contralateral cryptorchidism was found in 4 patients, and 2 patients had a history of chronic scrotal pain.
The mean duration of symptoms before presentation was 78.8 hours ± 153 hours with range of 3 hours and 720 hours. Six patients (27.3%) presented within the first 6 hours of scrotal pain and 11 patients (50.0%) presented after 18 hours of symptoms.
Scrotal swelling and testis ascension and retraction to the inguinal ring were found in 16 patients (72.7%). Two patients (9.1% of cases) presented with vomiting. Doppler Scrotal ultrasound was performed in 15 patients (68.0% of cases) which showed spiral turns of the testicular vessels in 11 patients and decrease or absent blood supply to the testis in all the 15 patients.
The average duration between presentation and surgical intervention was 5.6 hours ± 5 hours with extremes of one hour and 24 hours. Spinal anaesthesia was given in 12 patients (54.6%), general anaesthesia in 7 patients and local anaesthesia in 3 patients. The scrotal incision was used in majority of the patients (15 patients), while inguinal route was used in only one patient (4.5%).
Torsion was intravaginal in all patients. The degree or number of turns of the testis on the spermatic cord was documented in 9 patients (36.4%). A single turn was found in 2 patients, while 2 turns were found in 7 patients. Among the 23 twisted testicles, 8 were found viable; 4 (17.4%) were bluish in appearance and have satisfactory revascularization after detorsion and warming with warm-saline; but 11 (47.8%) were found necrotic and therefore underwent orchiectomy. Figure 1 presents necrotic testis images in operative view for a patient. Among the patients who underwent for orchiectomy, 9 presented 6 hours after the onset of the pain, ie, 81.8% of the 11 patients; and only 2 patients (19.2% of 11 patients) presented within 6 hours of the onset of pain. Of the 21 patients with unilateral spermatic cord torsion, contralateral orchidopexy was performed in 17 patients (76.2%) including 4 (19.1%) at the same time. The postoperative course was uneventful except for a patient has secondary gangrene of a testicle which was edematous but considered viable. The average hospital stay was 3.1 ± 1.4 days with a range of 1 and 6 days.
Discussion
Spermatic cord torsion is a common urological emergency with an estimated annual incidence 1/4000 young people under 25.4 There is a relatively low incidence of torsion of the spermatic cord in our centre (4.4 patients/year). This relatively low incidence was also noted in the series of Bah et al5 in Guinea Conakry, Gnassingbé et al6 in Togo and Niang et al7 in Senegal who reported annual incidence of 1.8 cases per year, 3.4 cases per year and 3.8 cases per year, respectively.
In our study, the average age of patients was 17.8 ± 6.4 years, reflecting a high frequency of spermatic cord torsion in adolescents. This result is close to that reported by Odzebé et al8 in Congo Brazzaville and by Bah et al in Guinea Conakry who reported mean ages of 20.2 and 19.5 years, respectively.5 Spermatic cord torsion mainly occurs at two extremes of childhood ages: in newborns and adolescents.9 It remains a problem for the young population as found in most studies.
The main symptom at presentation was painful scrotal swelling as observed in all the patients reviewed. Similar findings were reported by Gnassingbé et al6 in Togo and Bah et al in Guinea Conakry.5 For Hodonou et al2 in Benin, right or left hemi-scrotal pain was the main symptom at presentation, and it was associated with scrotal swelling in 79.0% of cases. Similarly, Dang et al10 in France also reported that sudden testicular pain was the most common symptom (81.8%).
We noted 23 twisted testicles in 22 patients, including one case of bilateral torsion on admission to the emergency room. Sahnoun et al11 in Tunisia and Kuranga et al12 in Nigeria, respectively, reported one case of bilateral spermatic cord torsion in nine patients and 6 cases in 92 patients. These results confirm the rarity of bilateral torsion of the spermatic cord.
During a torsion of the spermatic cord, the first irreversible lesions theoretically appear from the 6th hour of torsion. In our study, the average duration of symptoms before presentation was 78.8 hours. This duration seems to be long given that the outcome of the management of testicular torsion is highly time-dependent. Kaboré et al13 in Burkina Faso found an average delay of 24.6 hours; Sauvat et al14 in France an average delay of 17.0 hours and Gnassingbé et al6 in Togo an average delay of 30.0 hours. Dang et al10 in France reported an even shorter average delay of 8.0 hours. Our delay is close to that of Odzebé et al8 in Congo Brazzaville who reported an average delay of 71.4 hours. These results suggest that there is a relatively long delay before presentation in most African countries which could be explained by the relatively poor accessibility and availability of specialized health services, poor financial strength of the patient to access specialized health care and low level of knowledge of the seriousness of SCT by some health workers.
Physical examination plays an important role in the diagnosis of spermatic cord torsion. Scrotal swelling (found in all patients), scrotal elevation, horizontally lying testes and retraction of the testicle to the external inguinal ring were found in 72.7% of our patients. Kaboré et al13 in Burkina Faso, Bah et al5 in Guinea Conakry and Sauvat et al14 in France found that scrotal swelling and testicular ascension were the dominant signs. These findings suggest that any acute painful scrotal swelling in a young patient should be considered to be testicular torsion until proven otherwise; therefore, scrotal exploration must be done as an emergency even if all the physical signs are not met.
No additional examination should delay scrotal exploration whenever testicular torsion is suspected. However, scrotal Doppler ultrasound can be performed in case of diagnostic doubt.
The average time that is taken from presentation to scrotal exploration in our series was 5.6 hours, this is generally long. Dang et al10 in France reported an average treatment time of 8.0 hours, longer than that of our study. This long preoperative waiting time t could be from the logistics involved in the preoperative assessment and performance of scrotal ultrasound before the scrotal exploration. The unavailability of the operating room could also be a reason. We have only a single operating room that is dedicated to surgical emergencies in our centre.
Scrotal exploration can be done through transverse scrotal (elective), median raphe or inguinal incision. The scrotal incision is the most commonly used approach in our patients (68.2%). This result is close to that of Odzebé et al8 in Congo Brazzaville who also found that the transverse scrotal incision was the most used (65.8%). This seems to be the approach of choice of most surgeons.
All spermatic cord twists in our study were intravaginal. Odzebé et al8 in Congo Brazzaville found a similar result. On the other hand, it is different from that of Sarr et al15 in Senegal who reported five cases of extravaginal torsion and that of Sahnoun et al11 in Tunisia who noted exclusively extravaginal torsion. This could be due to the fact that intravaginal torsion is commonly seen in newborns, and there were no neonates in our study.
Of the 23 twisted testicles, 56.5% were necrotic at the time of exploration. This reflects a high frequency of testicular gangrene in our study. These results are different from those of Hodonou et al2 in Benin and Sahnoun et al11 in Tunisia who reported that the testicle was gangrenous in 27.3% and 13.8% of their patients, respectively. This high rate of testicular gangrene in our study could be due to delay in presentation with the majority of patients presenting more than 6 hours after the onset of pain, but also by the delay in surgical exploration as a result of logistic problems.
In our study 11 (44.83%) of the patients had orchiectomies. Odzebé et al8 in Congo Brazzaville and Hodonou et al2 in Benin found orchiectomy rates of 44.7% and 43.0%, respectively, which is quite close to ours. On the other hand, Grear et al16 in the United States of America, Bah et al5 in Guinea Conakry and Gnassingbé et al6 in Togo noted even lower rates of orchiectomy of 33.6%, 18 0.5% and 0.0%, respectively. This high rate of orchidectomy in our series could be due to delay presentation or delay in diagnosis and management.
In our study, the hospital stay was short. This observation is made in several other series.2,13,17 This short duration of hospitalization is explained by the rarity of complications.
Conclusion
Testicular torsion is a common and serious urological emergency because any delay in treatment may lead to serious consequences on the fertility of the patient. It is a disease that mainly affects the young. Its diagnosis is clinical and must be considered in the presence of acute painful scrotal swelling and pain. Public education on the need for an urgent presentation to a hospital in the face of any scrotal pain and swelling is necessary to shorten the time wasted before the presentation.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this study.
References
1. Gayito Adagba RA, Adabra K, Tengue K, et al. Torsion du cordon spermatique chez l’adulte. Aspects diagnostiques, thérapeutiques et pronostiques au Centre Hospitalier et Universitaire Sylvanus Olympio de Lomé [Spermatic cord torsion in adults.Diagnostic, therapeutic and prognostic aspects at Sylvanus Olympio University Teaching Hospital of Lomé]. Med Afr Noire. 2018;2018:44–48.
2. Hodonou R. La torsion du cordon spermatique (TCS) [Spermatic cord torsion (SCT)]. Med Afr Noire. 1999;46(2):70–74.
3. Kaboré FA, Kabore KK, Kabore M, et al. Predictive factors for orchiectomy in adult’s spermatic cord torsion: a case‐control study. Basic Clin Androl. 2021;31(1):2–5. doi:10.1186/s12610-021-00122-y
4. Cuckow MP, Frank JD. Torsion of testis. BJU Int. 2000;86:349–353. doi:10.1046/j.1464-410x.2000.00106.x
5. Bah OR, Roupret M, Guirassy S, Diallo AB, Diallo MB, Richard F. Aspects cliniques et thérapeutiques de la torsion du cordon spermatique: étude de 27 cas [Clinical and therapeutic aspects of spermatic cord torsion: a study of 27 cases]. Prog Urol. 2010;20(7):527–531. doi:10.1016/j.purol.2009.12.011
6. Gnassingbé K, Akakpo-Numado KG, Songne-G B, Kao M, Tékou H. Article Original Les torsions du cordon spermatique chez l’enfant [Spermatic cord torsion in children]. Afr J Urol. 2009;15(4):263–267. doi:10.1007/s12301-009-0049-9
7. Niang L, Jalloh M, Labou I, et al. Grosses bourses douloureuses: aspects cliniques et thérapeutiques [Painful bursae: clinical and therapeutic aspects]. Rev Afr Chir Spéc. 2010;4(9):33–36.
8. Odzebé AWS. Torsion du cordon spermatique et des annexes testiculaires chez le sujet adulte au CHU de Brazzaville [Torsion of the spermatic cord and testicular adnexa in adults at Brazzaville University Hospital]. Rev Afr Urol Androl. 2018;1(9):228.
9. Mongiat-Artus P. Torsion du cordon spermatique et des annexes testiculaires [Torsion of the spermatic cord and testicular adnexa]. Ann Urol. 2004;38(1):25–34. doi:10.1016/j.anuro.2003.11.001
10. Dang V, Lannes F, Bardet F, et al. Exploration chirurgicale d’une douleur testiculaire aiguë suspecte de torsion du cordon spermatique chez l’adulte: étude d’une population de 468 cas [Surgical investigation of acute testicular pain suspected of spermatic cord torsion in adults: study of a population of 468 cases]. Prog Urol. 2020;30(13):816. doi:10.1016/j.purol.2020.07.205
11. Sahnoun L, Mosbahi S, Ben Saad M, et al. Torsion testiculaire périnatale: à propos de dix cas [Perinatal testicular torsion: about ten cases]. J Pédiatrie Puériculture. 2011;24(6):276–283. doi:10.1016/j.jpp.2011.09.002
12. Kuranga SA, Rahman GA. Testicular torsion: experience in the middle belt of Nigeria. Afr J Urol. 2002;8(2):78–82.
13. Kaboré FA, Zango B, Yaméogo C, Sanou A, Kirakoya B, Traoré SS. Les torsions du cordon spermatique chez l’adulte au CHU Yalgado Ouédraogo de Ouagadougou [Spermatic cord torsion in adults at the Yalgado Ouedraogo University Hospital of Ouagadougou]. Basic Clin Androl. 2011;21(4):254–259. doi:10.1007/s12610-011-0151-2
14. Sauvat F, Hennequin S, Ait Ali Slimane M, Gauthier F. Un âge pour la torsion testiculaire ? [An age for testicular torsion?] Arch de Pédiatrie. 2002;9(12):122620111229. doi:10.1016/S0929-693X(02)00112-4
15. Sarr A, Fall B, Mouss B, et al. Aspects diagnostiques et thérapeutiques de la torsion du cordon spermatique au CHU Aristide-Le-Dantec de Dakar [Diagnostic and therapeutic aspects of spermatic cord torsion at the Aristide- Le -Dantec University teaching hospital of Dakar]. Basic Clin Androl. 2010;20(3):203–208. doi:10.1007/s12610-010-0083-2
16. Greear GM, Romano MF, Katz MH, Munarriz R, Rague JT. Testicular torsion: epidemiological risk factors for orchiectomy in pediatric and adult patients. Int J Impot Res. 2021;33(2):184–190. doi:10.1038/s41443-020-0331-8
17. Diabaté I, Ouédraogo B, Thiam M. Les grosses bourses aiguës au centre hospitalier de Louga, Sénégal: aspects épidémiologiques, étiologiques et thérapeutiques [Acute large bursae at Louga Hospital in Senegal: epidemiological, aetiological and therapeutic aspects]. Pan Afr Med J. 2016;2016:24.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.