")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 15
Prevalence and Factors Associated with Dyslipidemia Among People Living with HIV/AIDS on Follow-Up Care at a Tertiary Care Hospital in Ethiopia: A Cross-Sectional Study
Authors Assefa A, Abiye AA , Tadesse TA , Woldu M
Received 4 November 2022
Accepted for publication 18 May 2023
Published 19 May 2023 Volume 2023:15 Pages 93—102
DOI https://doi.org/10.2147/DHPS.S395037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Siew Siang Chua
Alemayehu Assefa, Alfoalem Araba Abiye, Tamrat Assefa Tadesse, Minyahil Woldu
Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Alfoalem Araba Abiye, Email [email protected]
Background: Despite its importance as a major risk factor for cardiovascular disease, dyslipidemia remains poorly characterized in the African population.
Objective: To assess the prevalence and factors associated with dyslipidemia in people with HIV/AIDS in follow-up at Zewditu Memorial Hospital, Addis Ababa, Ethiopia.
Materials and Methods: A hospital-based retrospective cross-sectional study evaluated the charts of 288 people living with HIV/AIDS who had received Highly Active Antiretroviral Treatment for at least six months at Zewditu Memorial Hospital from July to September 2021. Sociodemographic and clinical data were collected from the patient’s charts. Statistical analysis was performed using the Statistical Package for Social Sciences software version 25.
Results: The overall prevalence of dyslipidemia was 55.2% in people living with HIV/AIDS. The prevalence of high-density lipoprotein cholesterol < 40 mg/dl in men and < 50 in women was 46.9%; total cholesterol ≥ 200 mg/dl was 22.6%; triglycerides ≥ 150 mg/dl was 18.8%, and low-density lipoprotein ≥ 130 mg/dl was 4.9%. Sex [Female adjusted odds ratio (AOR) = 0.595, 95% CI: 0.37– 0.956], age greater than 40 years (AOR = 1.026, 95% CI: 1.005– 1.048), body mass index > 25 kg/m2 (AOR = 1.767, 95% CI: 1.099– 2.84), viral load > 50 (AOR = 0.477, 95% CI: 0.27– 0.842), and CD4 < 500 (AOR = 1.938, 95% CI: 1.18– 3.183) were identified as determinants of dyslipidemia.
Conclusion: There was a high prevalence of dyslipidemia among study participants compared to several studies published in a similar population. Being male, older age, higher BMI, low CD4 count, and viral load of < 50 copies/mL were associated with dyslipidemia in people living with HIV/AIDS. Therefore, lipid profile measurements at baseline must be part of routine care to prevent the devastating effects of dyslipidemia.
Keywords: antiretroviral therapy, dyslipidemia, HIV/AIDS, Ethiopia
Introduction
Dyslipidemias, or disorders of lipoprotein and lipid metabolism, are metabolic abnormalities that cause a chronic rise in cholesterol and triglyceride (TG) levels in the blood. Raised total cholesterol (TC), high low-density lipoprotein cholesterol (LDL-C), low high-density lipoprotein cholesterol (HDL-C), and increased TG are all involved.1–3
Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) is a chronic disease associated with dyslipidemia and insulin resistance.4 Highly Active Antiretroviral Therapy (HAART) is the mainstay of treatment for people living with HIV/AIDS (PLWHA).5 The goal of HAART is to suppress viral replication so that the patient’s immune system can recover and protect against the development of AIDS and death.6 Treatment of HIV/AIDS with HAART is complex because of its interaction with lipid-lowering medications in PLWHA.7 In addition, PLWHA taking combination antiretroviral therapy (ART) experience an increase in the frequency of metabolic risk factors (insulin resistance, lipoatrophy, dyslipidemia, and fat distribution abnormalities).8 Features of dyslipidemia in PLWHA receiving HAART include increased levels of TC, LDL-C, TG, and decreased HDL-C.9
Although dyslipidemia is a significant risk factor for cardiovascular disease (CVD), it is still poorly understood in the African population. According to WHO estimates, 23.1% of Africans aged 25 or older had elevated total cholesterol levels in 2008.10 A recent systematic review and meta-analysis indicated that the pooled prevalence of dyslipidemia in Africa was 52.8%.11 These findings suggest that the prevalence of dyslipidemia is increasing in the general adult population in Africa and is even higher in individuals with other risk factors for CVD, necessitating action to control dyslipidemia and prevent CVD on this continent.3,12,13
The risk of coronary artery disease (CAD) is increased in HIV-infected individuals compared with the uninfected population, 1.5-fold to twofold.14 The increased coronary heart disease (CHD) risk observed in PLWHA is mainly (although not exclusively) due to traditional risk factors such as smoking, diabetes, and dyslipidemia.15 Overall, the loss of protection against atherosclerosis due to decreased HDL-C probably outweighs the potential benefit of decreased LDL-C and TC in untreated HIV infection.3 Dyslipidemia is a known complication of combination therapy ART; it occurs in up to 70–80% of HIV-infected persons receiving combination therapy ART.16
HIV infection and ART can induce lipodystrophy, insulin resistance, and dyslipidemia which are risk factors for metabolic syndrome. However, the mechanism for the development of lipid abnormality is still unclear and proposed to be multi-factorial. The individual contributions of HIV infection, specific ARV agents, host genetics, and changes in body composition all should be considered for the development of lipid abnormality among PLHIV. Treatment of HIV-associated dyslipidemia should be a component of an attempt to improve cardiovascular health.17,18
Evidence from earlier literature showed that characteristics such being on HAART, HIV duration, BMI, age, gender, hypertension, and diabetes had significant associations with aberrant lipid profiles. The pooled prevalence of dyslipidemia ranges from 47 to 82.3%.9,18–23 Zewditu Memorial Hospital is the largest center in Ethiopia where thousands of PLWHA are getting care and treatment. However, the prevalence of dyslipidemia and its associated factors in this patient population has not been yet studied in this largest tertiary care hospital. Therefore, the current study aimed to determine the prevalence and factors associated with dyslipidemia among PLWHA on follow-up at the ART clinic of Zewditu Memorial Hospital in Addis Ababa, Ethiopia.
Materials and Methods
Study Setting
Zewditu Memorial Hospital (ZMH) is a tertiary teaching hospital in Ethiopia’s capital, Addis Ababa. The hospital is a pioneer in the treatment of PLWHA, having launched the anti-retroviral therapy (ART program) in Ethiopia in July 2003 with the help of the Centers for Disease Control and Prevention (CDC)-Ethiopia. The hospital also provides palliative care, HIV counseling, and testing, sexually transmitted infection (STI) services, and post exposure prophylaxis (PEP).
Study Design and Period
A hospital-based cross-sectional study was conducted at ZMH between June and September 2021.
Study Population
The source population consisted of all PLWHA who had follow up at ZMH ART Clinic. All PLWHA who had follow-up appointments at the ZMH ART Clinic, were at least 18 years old, and met the inclusion criteria made up the study population. According to the available data, 6000 PLWHA are getting care and treatment in this hospital per month. All PLWHAs aged ≥18 years that had ART follow-ups for at least 6 months were included in the study. Participants whose records were incomplete were excluded from the study.
Sample Size Determination and Sampling Techniques
The sample size was determined using a single proportion formula. A proportional value of 0.5 (50%), a confidence interval of 95% (α=0.05), and d=0.05 were used; the final sample size was 288 after adjusting the sample size for a study population of less than 10, 000. Simple random sampling was used to select patient records. Medical records were used for data on demographic and clinical characteristics and lipid profiles. Measured serum levels of TC, HDL-C, LDL-C, and TG were recorded. In ZMH, before undergoing a full cholesterol test, commonly known as a lipid panel or lipid profile, patients were instructed to fast for nine to twelve hours and drink only water.
Operational Definitions
Dyslipidemia
TC ≥ 200 mg/dl, HDL-C < 40 mg/dl for males and < 50 mg/dl for females, LDL-C ≥ 130 mg/dl, TG ≥ 150 mg/dl.24
Data Collection Tool and Procedures
The data collection tool is designed to capture information on patients’ sociodemographic and clinical characteristics, and the lipid profile data (TC, HDL, LDL, TG levels). Data were collected by pharmacy students under the supervision of medical records and the I-Care system. Before the actual data collection, a pretest was conducted with 5% of the study participants to check the uniformity and comprehensibility of the data collection instrument, and necessary amendments were made to it.
Data Quality Assurance
The format for data collection was tested (on 5% of the sample) before actual data collection and corrected accordingly. The analysis was performed thoroughly to ensure its completeness. After data collection, the collected data were checked for accuracy, completeness, and clarity.
Statistical Analysis
Data were entered and analyzed using the Statistical Package for Social Sciences (SPSS) window version 23. Descriptive statistics and the chi-square test was used for categorical variables. Binary logistic regression was used to identify factors associated with abnormal serum lipid profiles. Those variables with p<0.25 in the bi-variable analysis were considered for computing multivariable analysis to adjust for any confounding effect and odds ratios at a 95% confidence interval were used to measure the association between independent variables and abnormal serum lipid profiles. In multivariable analysis, p<0.05 was used to declare the significance of the association.
Results
Sociodemographic and Clinical Characteristics of Study Participants
Out of 288 study participants, 162 (56.3%) were females with a mean age of 43.5 ± 11.27 years. One hundred twenty-five (43.4%) had been on ART for 11–15 years, followed by those who had been on HAART for 1–5 years 74 (25.7%) (Table 1).
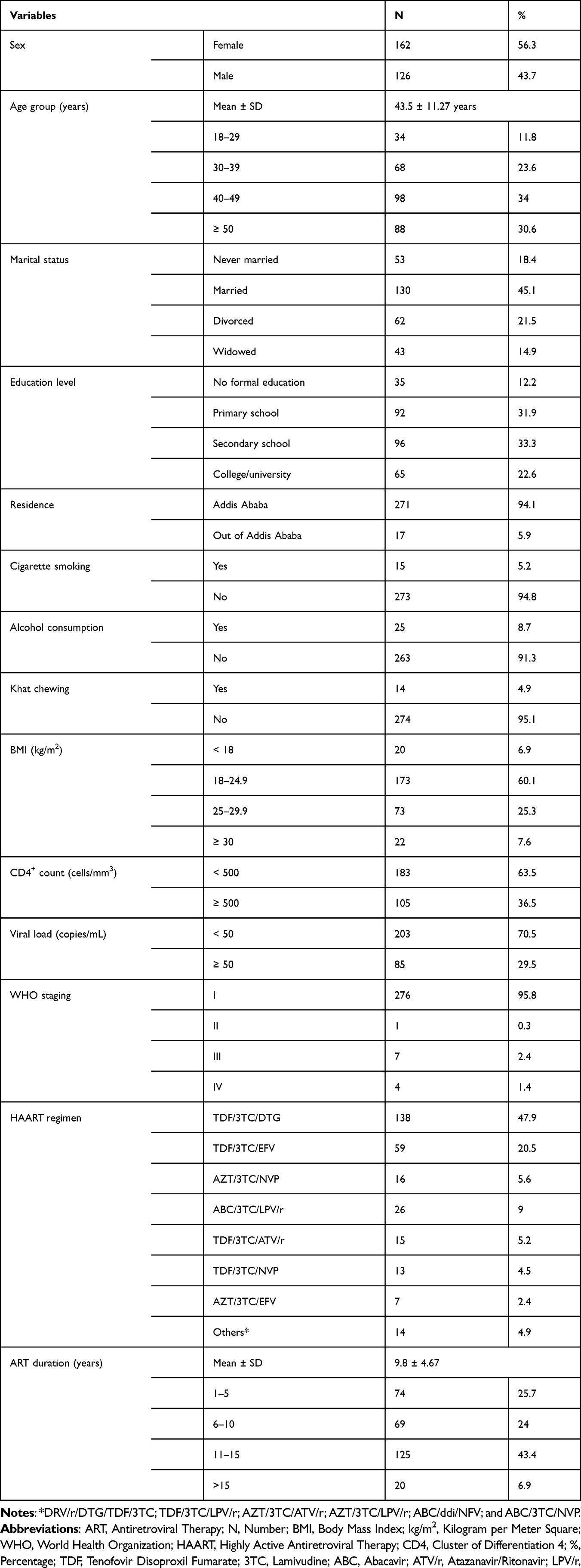 |
Table 1 Sociodemographic and Clinical Characteristics of the Study Population at Zewditu Memorial Hospital, Addis Ababa, Ethiopia (N = 288) |
Characteristics of Serum Lipid Profile Levels of the Study Participants
Out of a total, 159 (55.2%) participants had at least one lipid abnormality. Of the total number of participants, the prevalence of TC ≥ 200 mg/dl was 65 (22.6%) with a mean TC of 187.3 ± 51.6, TG ≥ 150 mg/dl was 54 (18.8%) with a mean TG of 155.5 ± 87.3 (Table 2).
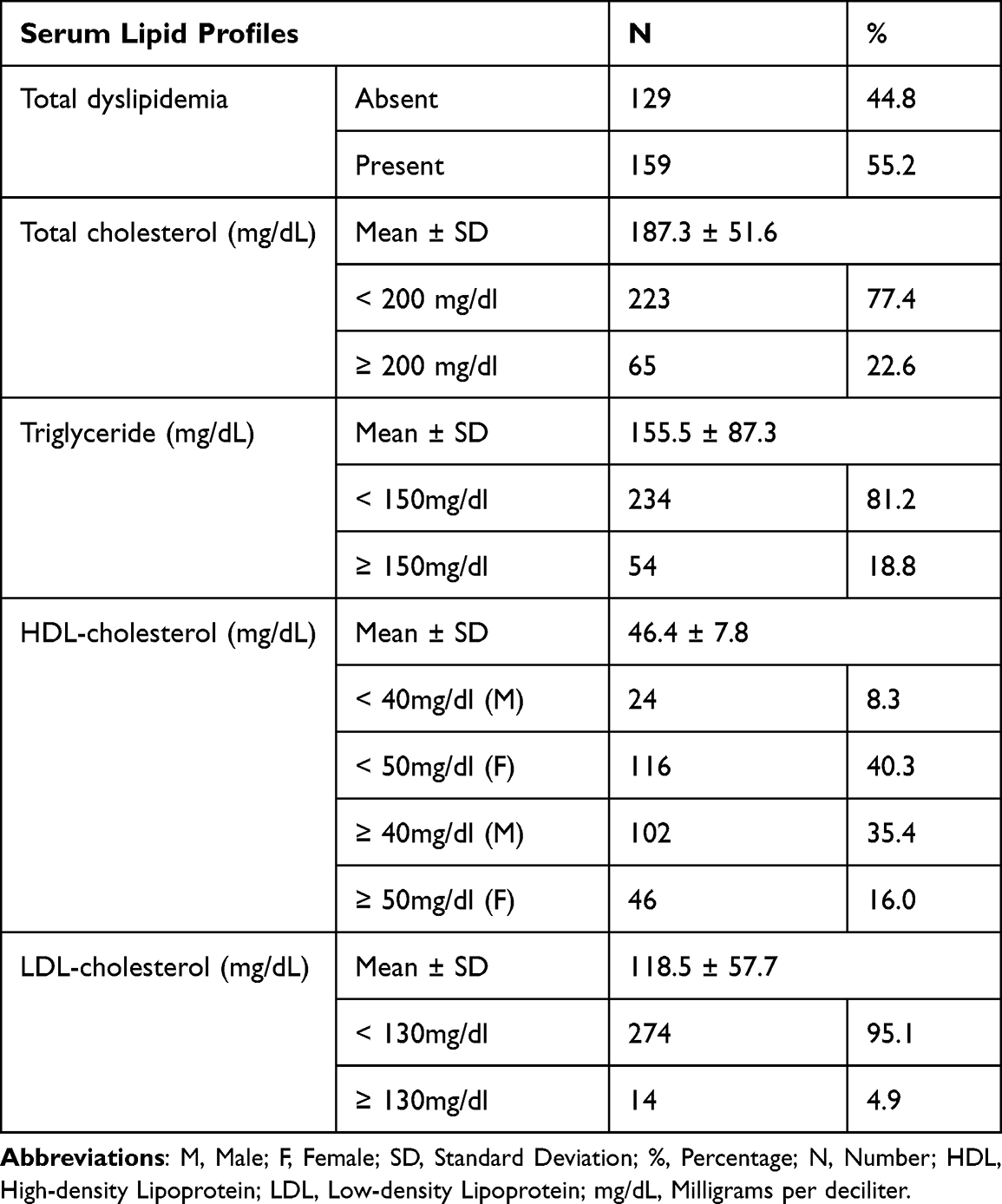 |
Table 2 Serum Lipid Profiles of Study Participants at Zewditu Memorial Hospital, Addis Ababa, Ethiopia (N=288) |
Association Between Lipid Profile Levels and Risk Factors
Factors like sex, age, BMI, CD4 cell count, and viral load had a p-value less than 0.25 in the univariate binary logistic regression analysis and were therefore included in the multivariate regression analysis. The analysis showed that sex, age, BMI, CD4 cell count, and viral load had a significant association with dyslipidemia at a p-value of < 0.05 in multivariate binary logistic regression (Table 3).
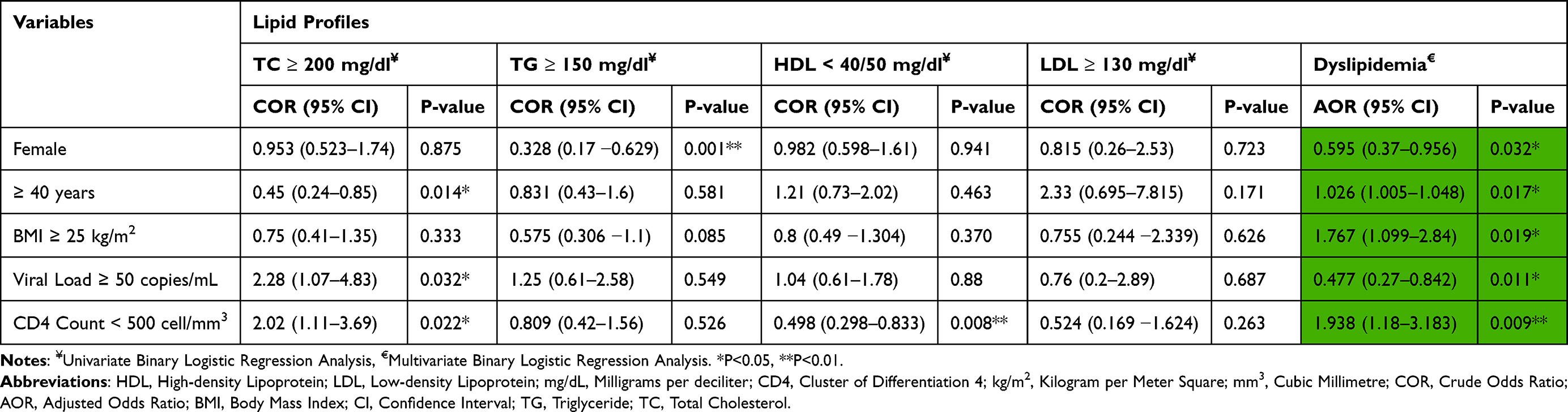 |
Table 3 Association of Lipid Profile Levels and Other Variables at Zewditu Memorial Hospital, Addis Ababa, Ethiopia (N=288) |
Discussion
This study’s overall prevalence of dyslipidemia in PLWHA was 55.2%. Similar results were reported from studies conducted on PLWHA in India (50.7%),19 Central Ethiopia (63.6%),23 and Zimbabwe (60%).25 However, a lower prevalence than the present result was documented in Eastern Ethiopia (34.8%),26 China (32.2%),27 and Iran (30.0%).28 In contrast, the prevalence is lower than in previous studies in Addis Ababa, Ethiopia (80.0%),22 Southern Ethiopia (82.3%),21 Kenya (79.6%),20 and South Africa (90.0%).29 The discrepancies could be related to differences in urbanization, socioeconomic status, dietary habits, and physical activity.
The most frequent dyslipidemia component was low HDL-C, which was followed by increased TC and elevated TG. The result may be due to the increasing consumption of simple carbohydrates and saturated fatty acids in the context of rapid urbanization and immunodeficiency resulting from HIV infection.30,31
The odds of females, AOR 0.595 (95% CI 0.37–0.956) having dyslipidemia was less, compared with male participants. This finding is inconsistent with a study from Tanzania,32 but not with studies from South Africa,33 Cameroon,9 and Latin America.34 The inconsistency is likely due to gender-specific physical activity habits and biological differences in men and women in dealing with ART adverse outcomes.35 Despite viral suppression and immune recovery promoted by modern treatment, aging, together with prolonged exposure to antiretroviral drugs, may increase the risk of dyslipidemia.4,16
Elevated body mass index was found to be positively related to dyslipidemia, ie, an increase in BMI increases the likelihood of dyslipidemia. This finding is consistent with studies from Southern Ethiopia,21 Tanzania,32 South Africa,29 and Cameroon.9 This could be because the concentration of various lipid components tends to increase with increasing BMI.36
The pathogenesis of lipodystrophy in PLWHA is multifactorial and still not fully understood. This disease is most likely the result of an interaction between antiretroviral therapy, viral infection, genetic factors, and the individual’s lifestyle.37,38 The duration of ART was not significantly related to dyslipidemia in the current study, in contrast to many others.39–41
In this study, patients with advanced age were significantly associated with an increased risk of dyslipidemia. A possible explanation for this finding could be that with advancing age, activity levels and work intensity decrease, leading to excessive fat accumulation. In addition, socioeconomic status could improve with age, leading to dietary changes.
Markers of advanced disease stage, ie, low CD4 levels, were associated with dyslipidemia. This finding is similar to studies from China,38 Cameroon,42 and Tanzania,32 which showed a strong association between CD4 count and the likelihood of abnormal lipid metabolism.
This study has shown that the prevalence of lipid abnormalities in PLWHA tends to increase with a lower viral load. This finding was consistent with the Domingo et al study.43 Intervention strategies that address dietary, lifestyle, and behavioral factors should be strengthened, especially for men, the elderly, and people with elevated BMI. The high level of dyslipidemia in this study could lead to high morbidity and mortality. Therefore, lipid profile measurements at baseline must be part of routine care to prevent the devastating effects of dyslipidemia.
Limitations of the Study
The prevalence of dyslipidemia was based on a single laboratory test, which may lead to result inconsistency. As with all cross-sectional studies, the current study was limited to examining causal associations between dyslipidemia and the identified risk factors. Moreover, data collection was done by reviewing patient charts. This may introduce recall bias because patients were not followed up to identify the effects of risk factors at the individual level. In addition, not all potential confounding factors for dyslipidemia were considered in this study.
Conclusion
In this study, the overall prevalence of dyslipidemia among PLWHA was 55.2%. Being male, older age, higher BMI, low CD4 count, and viral load of < 50 copies/mL were associated with higher risk of dyslipidemia in PLWHA.
Data Sharing Statement
All data supporting the findings are adequately included within the paper.
Ethical Considerations
Ethical approval for the study was obtained from the Ethical Review Committee of the School of Pharmacy, College of Health Sciences, Addis Ababa University with a reference number (ERB/SOP/335/13/2021), and permission was obtained from the medical director’s office and ART clinic of ZMH. The ethical standards outlined in the Declaration of Helsinki for research with human participants were followed by this study. Before data collection, the purpose and significance of the study were explained to each study participant. The participant’s name was not given at the time of data collection, all other personal information was completely obscured, and confidentiality was maintained throughout the study period.
Informed Consent
Written informed consent was obtained from all participants before the actual data collection began, and study participants had the decision-making capacity to participate in the study.
Acknowledgments
The authors would like to acknowledge the Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Science, Addis Ababa University, for facilitating the current study. We are grateful to Mr. Awgichew Kifle, a consultant biostatistician, for his approval of the current study’s statistical test findings interpretation. This study was conducted as part of the thesis work of the first author, Alemayehu Assefa.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Jeppesen J, Hein HO, Suadicani P, Gyntelberg F. Relation of high TG–low HDL cholesterol and LDL cholesterol to the incidence of ischemic heart disease. Arterioscler Thromb Vasc Biol. 1997;17(6):1114–1120. doi:10.1161/01.ATV.17.6.1114
2. Mach F. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur HEART J. 2020;41(44):4255.
3. Pirillo A, Casula M, Olmastroni E, Norata GD, Catapano AL. Global epidemiology of dyslipidaemias. Nat Rev Cardiol. 2021;18(10):689–700. doi:10.1038/s41569-021-00541-4
4. Husain NEO, Ahmed MH. Managing dyslipidemia in HIV/AIDS patients: challenges and solutions. HIVAIDS Auckl NZ. 2015;7:1.
5. Miners A, Sabin C, Trueman P, et al. Assessing the cost-effectiveness of HAART for adults with HIV in England: the cost-effectiveness of HAART. HIV Med. 2001;2(1):52–58. doi:10.1046/j.1468-1293.2001.00048.x
6. Eggleton JS, Nagalli S. Highly active antiretroviral therapy (HAART). In: StatPearls. StatPearls Publishing; 2022: Available from. http://www.ncbi.nlm.nih.gov/books/NBK554533/.
7. Calza L, Manfredi R, Chiodo F. Dyslipidaemia associated with antiretroviral therapy in HIV-infected patients. J Antimicrob Chemother. 2004;53(1):10–14. doi:10.1093/jac/dkh013
8. Pao V, Lee GA, Grunfeld C. HIV therapy, metabolic syndrome, and cardiovascular risk. Curr Atheroscler Rep. 2008;10(1):61–70. doi:10.1007/s11883-008-0010-6
9. Nsagha DS, Weledji EP, Assob NJC, et al. Highly active antiretroviral therapy and dyslipidemia in people living with HIV/AIDS in Fako Division, South West Region of Cameroon. BMC Cardiovasc Disord. 2015;15(1):95. doi:10.1186/s12872-015-0090-5
10. Kelliny C, William J, Riesen W, Paccaud F, Bovet P. Metabolic syndrome according to different definitions in a rapidly developing country of the African region. Cardiovasc Diabetol. 2008;7(1):27. doi:10.1186/1475-2840-7-27
11. Obsa MS, Ataro G, Awoke N, et al. Determinants of dyslipidemia in Africa: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;8. doi:10.3389/fcvm.2021.778891
12. Noubiap JJ, Bigna JJ, Nansseu JR, et al. Prevalence of dyslipidaemia among adults in Africa: a systematic review and meta-analysis. Lancet Glob Health. 2018;6(9):e998–e1007. doi:10.1016/S2214-109X(18)30275-4
13. World Health Organization. Noncommunicable diseases: risk factors. The Global Health Observatory; 2021. Available from: https://www.who.int/data/gho/data/themes/noncommunicable-diseases.
14. Abdulrahman A, Matthew F Coronary artery disease in HIV. American college of cardiology; 2018. Available from: https://www.acc.org/latest-in-cardiology/articles/2018/01/18/08/57/http%3a%2f%2fwww.acc.org%2flatest-in-cardiology%2farticles%2f2018%2f01%2f18%2f08%2f57%2fcoronary-artery-disease-in-hiv.
15. So-Armah K, Freiberg MS. HIV and cardiovascular disease: update on clinical events, special populations, and novel biomarkers. Curr HIV/AIDS Rep. 2018;15(3):233–244. doi:10.1007/s11904-018-0400-5
16. Feeney ER, Mallon PWG. HIV and HAART-associated dyslipidemia. Open Cardiovasc Med J. 2011;5:49–63.
17. Ojong E, Iya B, Djeufouata J, et al. Metabolic syndrome and its components among HIV/AIDS patients on antiretroviral therapy and ART-naïve patients at the University of Calabar Teaching Hospital, Calabar, Nigeria. Afr Health Sci. 2022;22(1):410–417. doi:10.4314/ahs.v22i1.50
18. Tilahun A, Chekol E, Teklemaryam AB, et al. Prevalence and predictors of dyslipidemia among HAART treated and HAART naive HIV positive clients attending Debre Tabor Hospital, Debre Tabor, Ethiopia. Heliyon. 2022;8(11):e11342. doi:10.1016/j.heliyon.2022.e11342
19. Wankhade PS, Pedhambkar RB, Pagare RS, Pedhambkar BS. Prevalence and risk factors of dyslipidemia among male industrial workers in India. Int J Community Med Public Health. 2018;5(4):1458–1465. doi:10.18203/2394-6040.ijcmph20181217
20. Tilahun H, Masyuko SJ, Mogaka JN, et al. Prevalence and correlates of dyslipidemia in HIV positive and negative adults in Western Kenya: a cross-sectional study. Medicine. 2021;100(10):e24800. doi:10.1097/MD.0000000000024800
21. Tadewos A, Addis Z, Ambachew H, Banerjee S. Prevalence of dyslipidemia among HIV-infected patients using first-line highly active antiretroviral therapy in Southern Ethiopia: a cross-sectional comparative group study. AIDS Res Ther. 2012;9(1):31. doi:10.1186/1742-6405-9-31
22. Daniel Seifu EB. Lipid profile derangements among human immunodeficiency virus infected adults receiving first line anti-retroviral therapy in Tikur Anbesa Specialized Hospital, Addis Ababa, Ethiopia: comparative Cross-Sectional Study. J AIDS Clin Res. 2014;05(08). doi:10.4172/2155-6113.1000328
23. Bayenes HW, Ahmed MK, Shenkute TY, Ayenew YA, Bimerew LG. Prevalence and predictors of dyslipidemia on HAART and HAART naive HIV positive persons in Defense Hospital, Addis Ababa, Ethiopia. Am J Health Res. 2014;2(5):303. doi:10.11648/j.ajhr.20140205.23
24. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106(25):3143–3421.
25. Zhou DT, Nehumba D, Oktedalen O, et al. Changes in lipid profiles of HIV+ adults over nine months at a Harare HIV clinic: a longitudinal study. Biochem Res Int. 2016;2016:e3204818. doi:10.1155/2016/3204818
26. Sufa B, Abebe G, Cheneke W. Dyslipidemia and associated factors among women using hormonal contraceptives in Harar town, Eastern Ethiopia. BMC Res Notes. 2019;12(1):120. doi:10.1186/s13104-019-4148-9
27. Liu X, Yu S, Mao Z, et al. Dyslipidemia prevalence, awareness, treatment, control, and risk factors in Chinese rural population: the Henan rural cohort study. Lipids Health Dis. 2018;17(1):119. doi:10.1186/s12944-018-0768-7
28. Najafipour H, Shokoohi M, Yousefzadeh G, et al. Prevalence of dyslipidemia and its association with other coronary artery disease risk factors among urban population in Southeast of Iran: results of the Kerman coronary artery disease risk factors study (KERCADRS). J Diabetes Metab Disord. 2016;15:49. doi:10.1186/s40200-016-0268-0
29. Dave JA, Levitt NS, Ross IL, Lacerda M, Maartens G, Blom D. Anti-retroviral therapy increases the prevalence of dyslipidemia in South African HIV-infected patients. PLoS One. 2016;11(3):e0151911. doi:10.1371/journal.pone.0151911
30. Feingold KR. The effect of diet on cardiovascular disease and lipid and lipoprotein levels. In: Feingold KR, Anawalt B, Blackman MR, et al. editors. Endotext. MDText.com, Inc; 2000: Available from. http://www.ncbi.nlm.nih.gov/books/NBK570127/.
31. Masson CJ, Mensink RP. Exchanging saturated fatty acids for (n-6) polyunsaturated fatty acids in a mixed meal may decrease postprandial lipemia and markers of inflammation and endothelial activity in overweight men1–3. J Nutr. 2011;141(5):816–821. doi:10.3945/jn.110.136432
32. Ombeni W, Kamuhabwa AR. Lipid profile in HIV-infected patients using first-line antiretroviral drugs. J Int Assoc Provid AIDS Care. 2016;15(2):164–171. doi:10.1177/2325957415614642
33. Bekolo CE, Nguena MB, Ewane L, Bekoule PS, Kollo B. The lipid profile of HIV-infected patients receiving antiretroviral therapy in a rural Cameroonian population. BMC Public Health. 2014;14(1):236. doi:10.1186/1471-2458-14-236
34. Cahn P, Leite O, Rosales A, et al. Metabolic profile and cardiovascular risk factors among Latin American HIV-infected patients receiving HAART. Braz J Infect Dis off Publ Braz Soc Infect Dis. 2010;14(2):158–166. doi:10.1590/s1413-86702010000200008
35. Limas TG, De, Pinto G, de A Marcato LM, Coelho DR. Analysis of the prevalence of dyslipidemia in individuals with HIV and its association with antiretroviral therapy. Rev Soc Bras Med Trop. 2014;47(5):547–551. doi:10.1590/0037-8682-0128-2014
36. Gebreegziabiher G, Belachew T, Mehari K, Tamiru D. Prevalence of dyslipidemia and associated risk factors among adult residents of Mekelle City, Northern Ethiopia. PLoS One. 2021;16(2):e0243103. doi:10.1371/journal.pone.0243103
37. Justina LBD, Luiz MC, Maurici R, Schuelter-Trevisol F. Prevalence and factors associated with lipodystrophy in AIDS patients. Rev Soc Bras Med Trop. 2014;47(1):30–37. doi:10.1590/0037-8682-0240-2013
38. Shen Y, Wang J, Wang Z, et al. Prevalence of dyslipidemia among antiretroviral-naive HIV-infected individuals in China. Medicine. 2015;94(48):e2201. doi:10.1097/MD.0000000000002201
39. Kemal A, Teshome MS, Ahmed M, et al. Dyslipidemia and associated factors among adult patients on antiretroviral therapy in armed force comprehensive and specialized Hospital, Addis Ababa, Ethiopia. HIVAIDS Auckl NZ. 2020;12:221–231. doi:10.2147/HIV.S252391
40. Fiseha T, Alemu W, Dereje H, Tamir Z, Gebreweld A. Prevalence of dyslipidaemia among HIV-infected patients receiving combination antiretroviral therapy in North Shewa, Ethiopia. PLoS One. 2021;16(4):e0250328. doi:10.1371/journal.pone.0250328
41. Abebe M, Kinde S, Belay G, et al. Antiretroviral treatment associated hyperglycemia and dyslipidemia among HIV infected patients at Burayu Health Center, Addis Ababa, Ethiopia: a cross-sectional comparative study. BMC Res Notes. 2014;7(1):380. doi:10.1186/1756-0500-7-380
42. Pefura Yone EW, Betyoumin AF, Kengne AP, Kaze Folefack FJ, Ngogang J. First-line antiretroviral therapy and dyslipidemia in people living with HIV-1 in Cameroon: a cross-sectional study. AIDS Res Ther. 2011;8:33. doi:10.1186/1742-6405-8-33
43. Domingo P, Suarez-Lozano I, Teira R, et al. Dyslipidemia and cardiovascular disease risk factor management in HIV-1-infected subjects treated with HAART in the Spanish VACH cohort. Open AIDS J. 2008;2:26–38. doi:10.2174/1874613600802010026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.