")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 7
Prevalence and cost of imaging in inpatient falls: the rising cost of falling
Authors Fields J, Alturkistani T, Kumar N, Kanuri A, Salem D, Munn S, Blazey-Martin D
Received 31 December 2014
Accepted for publication 12 March 2015
Published 3 June 2015 Volume 2015:7 Pages 281—286
DOI https://doi.org/10.2147/CEOR.S80104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio L Colombo
Jessica Fields,1 Tahani Alturkistani,2 Neal Kumar,3 Arjun Kanuri,3 Deeb N Salem,1 Samson Munn,2 Deborah Blazey-Martin1
1Department of Medicine, Tufts Medical Center, Boston, MA, USA; 2Department of Radiology, Tufts Medical Center, Boston, MA, USA; 3Tufts University School of Medicine, Boston, MA, USA
Objective: To quantify the type, prevalence, and cost of imaging following inpatient falls, identify factors associated with post-fall imaging, and determine correlates of positive versus negative imaging.
Design: Single-center retrospective cohort study of inpatient falls. Data were collected from the hospital's adverse event reporting system, DrQuality. Age, sex, date, time, and location of fall, clinical service, Morse Fall Scale/fall protocol, admitting diagnosis, and fall-related imaging studies were reviewed. Cost included professional and facilities fees for each study.
Setting: Four hundred and fifteen bed urban academic hospital over 3 years (2008–2010).
Patients: All adult inpatient falls during the study period were included. Falls experienced by patients aged <18 years, outpatient and emergency patients, visitors to the hospital, and staff were excluded.
Measurements and main results: Five hundred and thirty inpatient falls occurred during the study period, average patient age 60.7 years (range 20–98). More than half of falls were men (55%) and patients considered at risk of falls (56%). Falls were evenly distributed across morning (33%), evening (34%), and night (33%) shifts. Of 530 falls, 178 (34%) patients were imaged with 262 studies. Twenty percent of patients imaged had at least one positive imaging study attributed to the fall and 82% of studies were negative. Total cost of imaging was $160,897, 63% ($100,700) from head computed tomography (CT).
Conclusion: Inpatient falls affect patients of both sexes, all ages, occur at any time of day and lead to expensive imaging, mainly from head CTs. Further study should be targeted toward clarifying the indications for head CT after inpatient falls and validating risk models for positive and negative imaging, in order to decrease unnecessary imaging and thereby limit unnecessary cost and radiation exposure.
Keywords: inpatients, falls, diagnostic imaging, health care costs, incident reporting
Introduction
Inpatient falls have been a quality of care issue for decades and add to the significant financial burden of health care costs. The Centers for Medicare and Medicaid Services has stopped paying for inpatient care related to iatrogenic events,1 encouraging widespread quality initiatives designed to reduce nosocomial complications including falls from patient beds. Inpatient falls alone are quite common, ranging from 2.3 to 17.1 falls per 1,000 patient-days.2,3 Approximately 30% of these falls result in morbidity and up to 6% of these injuries are serious, including fractures, subdural hematomas, significant bleeding, and even death.2,4,5 Patients who sustain fall-related injuries are reported to have higher overall hospital charges than similar matched patients who did not fall during their hospitalization. Falls that occur in hospital and result in injury are costly to both patients and health care institutions;6 in 1995 these charges, including surgical interventions, imaging, and additional hospital days, were more than $4,200 higher for patients experiencing an injurious inpatient fall than for those who did not.7
Bohl et al considered imaging among the components of cost after “medical fall” (any fall, regardless of setting, that results in medical attention),8 Wong et al analyzed all costs related to serious inpatient fall-related injuries,9 and Haines et al considered cost of overall imaging studies when analyzing potential cost savings from a patient education program to prevent inpatient falls,10 but to our knowledge, there are no studies designed specifically to evaluate the type, prevalence, and cost of imaging studies related to all falls that occur in patients already hospitalized. To address this gap, this study’s objectives were to 1) quantify the type, prevalence, and financial cost of imaging hospitalized patients following a fall; 2) identify risk factors associated with imaging patients after a fall; and 3) identify correlates for patients both with positive and negative imaging studies.
Methods
This study was conducted at Tufts Medical Center, a 415-bed urban academic teaching hospital affiliated with Tufts University School of Medicine in Boston, MA, USA. The study design was a retrospective cohort study, which included all adult inpatients who experienced a fall between January 1, 2008 and December 31, 2010. All 530 inpatient falls reported on medical, surgical, neurological, psychological, and gynecological services were included. Medical services included all general medicine, medical subspecialty, and medical intensive care patients. Surgical services included all general surgical, surgical subspecialty, and surgical intensive care patients. Neurological services included neurology and neurosurgery. Pediatric inpatients (age <18 years), emergency department patients, outpatients, visitors to the hospital, and staff members were excluded as the aim was to study imaging related to falls that occurred in hospitalized adults. The study was approved by the Institutional Review Board of Tufts Medical Center/Tufts University School of Medicine.
Patient falls were identified using the hospital’s online adverse event reporting system, DrQuality (Quantros, Inc., Milpitas, CA, USA). DrQuality, an online reporting system implemented at Tufts Medical Center in 2002, is available to all employees of Tufts Medical Center, including physicians, nurses, pharmacists, technicians, and other ancillary staff, to document medical errors and near misses. All falls occurring in the hospital are documented exclusively in the DrQuality reporting system, most often by nurses. A fall is defined within the adverse event reporting system as an involuntary descent to the floor. At Tufts Medical Center in 2008, the rate of reported falls was 2.2 falls per 1,000 patient-days and in 2009 and 2010 the rate was 2.3 falls per 1,000 patient-days.
DrQuality error reports categorized as “falls” occurring between January 1, 2008 and December 31, 2010 were collected and reviewed. Age, sex, medical record number, date of fall, time of fall, location of the fall, clinical service, admitting diagnosis, Morse Fall Scale assessment, fall protocol use, and whether the fall was witnessed were extracted from these DrQuality reports. We controlled for variability by having a single radiology resident perform subsequent chart reviews using only medical record number and date of fall to identify fall-related imaging studies. The criteria used to define “fall-related” were 1) the study was performed immediately following the fall through the time of discharge and 2) it was ordered to evaluate a fall-related condition according to the order given to the radiology department and/or the patient’s medical record. Imaging studies included all radiographic studies, including X-ray, computed tomography (CT), and magnetic resonance imaging (MRI) related to the fall during the inpatient stay (initial images and those ordered to reassess fall-related pathology). A positive finding on an imaging study was defined as any new finding that could potentially be explained by the trauma of the fall based on medical record review. For example, a head CT that shows a new bleed after fall would be considered positive, as would a new fracture consistent with the mechanism of the fall, while a head CT with a new malignant lesion would not.
Cost was calculated based on total charges billed by Tufts Medical Center at the time of the study, both professional and facilities fees, for each radiographic study ordered per fall. Patients who fell more than once during the study period were included repeatedly with each distinct fall episode for cost calculations, but were excluded when performing statistical analysis of characteristics of falling patients.
Characteristics of patients who were imaged were compared to those who were not imaged using the chi-square test and Student’s t-test as appropriate. Patients with positive imaging were compared to those with negative imaging in the same manner.
Results
Characteristics of inpatients who fell
During the study period from 2008 to 2010, 530 inpatient falls were reported at Tufts Medical Center. There were 46,192 admissions to the hospital with 229,601 total patient-days during this time. Therefore, the fall incidence rate was 2.3 falls per 1,000 patient-days. The characteristics of inpatients who fell are listed in Table 1. There were 530 falls with 507 unique patients who fell once. The mean age of patients who fell was 60.7 years (range 20–98), while the average age of an adult inpatient during the study period was 54 years. The Tufts Medical Center adult inpatient population was 47% male; however men fell more frequently than woman (55% versus [vs] 45%), although this difference was not statistically significant (P=0.96).
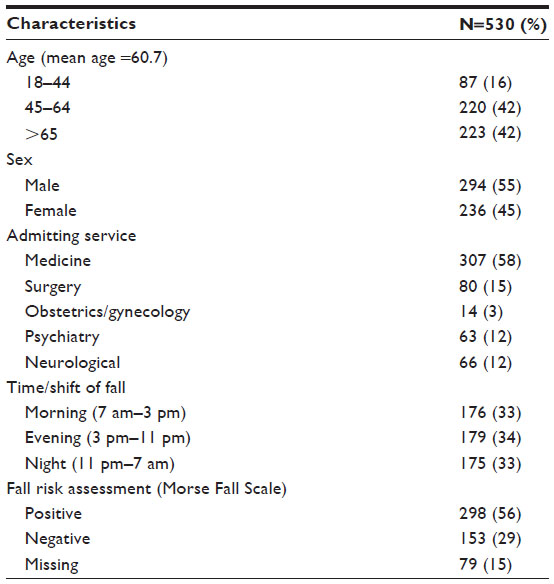 | Table 1 Characteristics of 530 inpatients who fell from 2008 to 2010 during stay at Tufts Medical Center |
Falls occurred on all adult inpatient services without association with identified fall risk. The medical services at Tufts Medical Center are the largest group of services, and most of the inpatient falls did occur on the medical services (58%). Falls were evenly divided throughout the day among shifts, morning (33%), evening (34%), and night (33%). Morse Fall Scale assessment was documented in 85% of the DrQuality reports; 56% of those who fell were deemed to be at risk of falls, whereas 29% were not.
Characteristics of inpatients imaged after fall
Of the 530 falls during the study period, 178 (34%) patients were imaged after the fall and their characteristics are listed in Table 2. Imaged patients were approximately 3 years older on average than non-imaged (62.6 years vs 59.7 years, P=0.07). More patients were imaged after falling on the medicine service than on the other services (medicine 39%, surgery 19%, obstetrics/gynecology 28%, psychiatry 30%, neurology 32%; P=0.02). Sex, Morse Fall Scale, and shift during which the fall occurred were not significantly associated with obtaining post-fall imaging (Table 2).
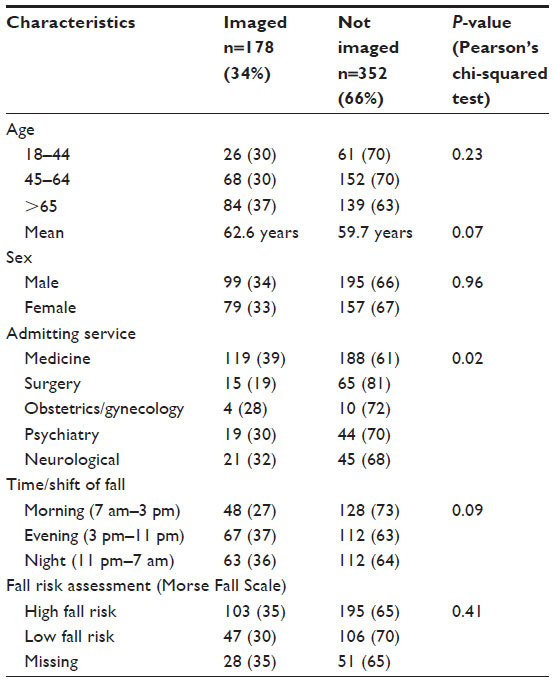 | Table 2 Characteristics of 178 patients who were imaged and 352 patients not imaged after a fall from 2008 to 2010 during hospital stay |
Characteristics of inpatients with positive and negative imaging studies
Of the 178 inpatients who were imaged following their fall, 35 (20%) patients had a positive study (Table 3). However, positive imaging after fall was not statistically associated with age, sex, time of day, admitting service, or Morse Fall Scale risk.
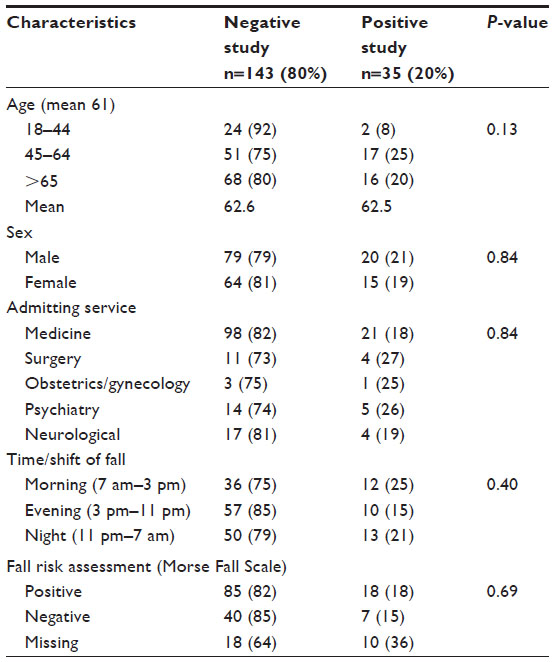 | Table 3 Characteristics of 178 patients imaged after an inpatient fall from 2008 to 2010 comparing those with positive (35) to those with negative studies (143) |
Relative frequency and cost of imaging
Of the 530 inpatient falls, 178 patients (34%) were imaged with a total of 262 fall-related studies ordered. There was an average of 1.5 studies ordered per patient (range 1–5 studies). Of all the studies ordered following a fall (Table 4), the preponderance were head CTs (152 studies, 58%). Of the head CTs, 85% were negative, whereas 70% of the other CTs were negative, 83% of X-rays and 63% of MRIs. The total cost of head CTs was $100,700 (63%), other CTs $37,482 (23%), X-rays $12,603 (8%), and MRIs $10,112 (6%); the overall cost of imaging during the 3-year study period was $160,897.
 | Table 4 Cost of imaging by type, cost per positive imaging study |
Discussion
The intent of this study was to look specifically at imaging performed due to inpatient falls and assess their type, prevalence, and contribution to health care costs. As the US Centers for Medicare and Medicaid Services withdraws payment for iatrogenic conditions, cost of imaging for inpatient falls may come under increased scrutiny, and this study provides a starting point for understanding these costs.
In order to understand imaging patterns and costs, we first needed to analyze the characteristics of the inpatient falls that occurred during the study period (Table 1). Fallers were slightly older than the average adult inpatient during the study period (60.7 vs 54 years). Forty-two percent of the patients in our study who fell were >65 years, the age one qualifies for Medicare. Sex was not statistically associated with inpatient falls, and while patients fell on all inpatient services included in our study and equally at all times of day, the largest share of falls took place on our largest service, adult medicine. Unfortunately we did not have access to the hospital level data needed to determine whether this rate was disproportionately high relative to the other services.
We theorized that assessed fall risk could be related to likelihood of falls and imaging, however while the Morse Fall Scale assessment was performed by protocol on all new admissions, 15% of the time it was not documented in the adverse event reporting system (DrQuality). Fifty-six percent of those who fell had a positive assessment documented, and therefore had fall precautions in place (non-skid socks, yellow wrist band, and yellow precaution signs as well as escort for toileting), yet they fell anyway. Nearly 30% of those who fell were assessed as not at risk for fall, and therefore had received no precautions prior to the fall. It is possible that patients with precautions in place may have suffered less injury due to these precautions, but this study was designed to look at imaging, and could not quantify subsequent injury.
With respect to whether or not imaging was performed after a fall, our study suggested that patients may be less likely to be imaged if they are younger (less than 65 years of age), if they fell on the morning shift, or if they fell on a surgical service (Table 2). Explanations for these findings include clinical comorbidities not collected in DrQuality reports and other patient factors such as ability to give a good history for unwitnessed falls, level of staffing on different shifts, and differences in the training of the physicians caring for these patients (surgeons, medical doctors, and psychiatrists).
In terms of the imaging studies themselves, our study found that the majority of the imaging studies ordered following an in hospital fall are head CTs, and that these are relatively expensive ($662 per head CT vs $194 per X-ray). Head CTs made up 63% of the total cost ($100,700 of the $160,897 spent on post-fall imaging over 3 years), and a large portion of the head CTs were negative (85%). This rate is greater than that of the other types of imaging studies with the exception of X-rays, which were negative 83% of the time but accounted for only 8% of the total cost of post-fall imaging.
The clinical rationale behind the substantial use of head CTs after inpatient falls is likely multifactorial. A common and significant risk a physician faces when assessing a patient after a fall is missing an acute intracranial hemorrhage (ie, subdural hematoma);11 these can be difficult to diagnose on physical exam, especially early on, and devastating to the patient and physician if missed. For unwitnessed falls in which the patient cannot provide a clear history, the definitive method to rule out intracranial hemorrhage at present is head CT. Non-contrast head CTs are quick and pose little risk to the patient other than radiation exposure and expense, making it relatively easy to justify ordering one if even a small risk of hemorrhage exists. At present, physicians have only their clinical assessment to guide them in their decision to order a head CT, and as there is no evidence-based algorithm to help them estimate the risk of intracranial hemorrhage after inpatient fall for any given patient, many will err on the side of caution. Regardless of the clinical rationale, the fact that such a high percentage of these head CTs are negative raises the question of whether they are all medically necessary.
Using the hospital incident reporting system to collect our data had the advantage of ensuring that all falls were included in the study, but it also created limitations, as the system was designed for quality and safety reporting purposes, not for research. Each report had standardized fields with and without dropdown boxes to record pertinent information about the fall, however, not all of these fields were mandatory, and consequently, there was missing data. The reporting template did provide space for free text, but did not specify or suggest what information should be included, thus free text inputs were subjective, variable, and often not present, making it very difficult to include them in the analysis. There was also very little clinical data in the reports (ie, mental status, anticoagulation, or sedating medications), which also limited our ability to analyze the factors contributing to imaging for falls and the clinical outcomes associated with these falls. Other limitations of this study were that it was a single center retrospective study with no available control group. In addition, while our study is not sufficiently powered to help us identify the patients who can safely avoid imaging after an in hospital fall, it does give us a better understanding of current imaging practices and the costs associated with them.
As the cost of health care in the US continues to skyrocket, understanding the role and subsequent financial implications of imaging in inpatient falls is an important piece of the bigger picture.12 The concern about costs associated with inpatient falls is not limited to the US;13 Nadkarni et al looked specifically at orthopedic injuries caused by inpatient falls in the UK and found that the additional hospital costs incurred by such injuries contributed a significant expenditure to the national health system5 and the cost of falls worldwide has also been studied.14–16 Our study found that the bulk of costs related to post-fall imaging stem from head CTs, the lion’s share of which are negative. The difficulty for clinicians is that no evidence-based algorithm exists to help predict which patients should be imaged following their inpatient fall and which can safely be watched.
Further studies are needed in order to better identify the clinical indications for imaging after inpatient falls, and would allow for modeling to help support decision making in determining when it is safe to monitor the patient clinically rather than order a head CT. Of course, elimination of imaging from inpatient falls and optimal patient safety comes ultimately with the prevention of falls themselves, and remains both the best practice and the ultimate goal.
Acknowledgments
Special thanks to Heather Baer, Harvard School of Public Health, for her help with the initial statistical analysis and planning, and to Dr Mary Lee, Tufts University, for her guidance on completion of the final manuscript.
Disclosure
The authors have no conflicts of interest to disclose.
References
Rosenthal MB. Nonpayment for performance? Medicare’s new reimbursement rule. N Engl J Med. 2007;357(16):1573–1575. | |
Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med. 2004;19(7):732–739. | |
Galbraith JG, Butler JS, Memon AR, Dolan MA, Harty JA. Cost analysis of a falls-prevention program in an orthopaedic setting. Clin Orthop Relat Res. 2011;469(12):3462–3468. | |
Bradley SM. Falls in older adults. Mt Sinai J Med. 2011;78(4):590–595. | |
Nadkarni JB, Iyengar KP, Dussa C, Watwe S, Vishwanath K. Orthopaedic injuries following falls by hospital in-patients. Gerontology. 2005;51(5):329–333. | |
Fischer ID, Krauss MJ, Dunagan WC, et al. Patterns and predictors of inpatient falls and fall-related injuries in a large academic hospital. Infect Control Hosp Epidemiol. 2005;26(10):822–827. | |
Bates DW, Pruess K, Souney P, Platt R. Serious falls in hospitalized patients: correlates and resource utilization. Am J Med. 1995;99(2):137–143. | |
Bohl AA, Phelan EA, Fishman PA, Harris JR. How are the costs of care for medical falls distributed? The costs of medical falls by component of cost, timing, and injury severity. Gerontologist. 2012;52(5):664–675. | |
Wong CA, Recktenwald AJ, Jones ML, Waterman BM, Bollini ML, Dunagan WC. The cost of serious fall-related injuries at three Midwestern hospitals. Jt Comm J Qual Patient Saf. 2011;37(2):81–87. | |
Haines TP, Hill AM, Hill K, et al. Cost effectiveness of patient education for the prevention of falls in hospital: economic evaluation from a randomize controlled trial. BMC Med. 2013;11:135. | |
Nurmi I, Luthje P. Incidence and costs of falls and fall injuries among elderly in institutional care. Scand J Prim Health Care. 2002;20(2):118–122. | |
Titler M, Dochterman J, Picone D, et al. Cost of hospital care for elderly at risk of falling. Nurs Econ. 2005;23(6):290–306. | |
Haines TP, Nitz J, Grieve JB, et al. Cost per fall: a potentially misleading indicator of burden of disease in health and residential care settings. J Eval Clin Pract. 2011;19(1):153–161. | |
Heinrich S, Rapp K, Rissmann U, Becker C, Konig HH. Cost of falls in old age: a systematic review. Osteoporos Int. 2010;21(6):891–902. | |
NSW Health [homepage on the Internet]. Watson W, Clapperton A, Mitchell R. Sydney, NSW: The incidence and cost of falls injury in older people in New South Wales 2006/07; 2010. Available from: http://www0.health.nsw.gov.au/pubs/2010/costoffall.html. Accessed March 28, 2015. | |
Tiedemann AC, Murray SM, Munroe B, Lord SR. Hospital and non-hospital costs for fall-related injury in community dwelling older people. N S W Public Health Bull. 2008;19(9–10):161–165. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.