")
Back to Journals » Patient Preference and Adherence » Volume 15
Predictors of Poor Adherence to CART and Treatment Failure at Second-Line Regimens Among Adults in Public Hospitals of Amhara Region, North-Western Ethiopia: A Retrospective Cohort Study
Authors Minwagaw MT , Akenie BB, Tewabe DS , Tegegne AS , Beyene TB
Received 12 October 2021
Accepted for publication 10 December 2021
Published 24 December 2021 Volume 2021:15 Pages 2855—2864
DOI https://doi.org/10.2147/PPA.S339108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Molalign Tarekegn Minwagaw,1 Betelihem Belete Akenie,1 Desalew Salew Tewabe,1 Awoke Seyoum Tegegne,2 Tariku Belachew Beyene3
1Department of Public Health, Amhara Public Health Institute, Bahir Dar, Ethiopia; 2Department of Statistics, Bahir Dar University, Bahir Dar, Ethiopia; 3Department of Public Health, Amhara Region Health Bureau, Bahir Dar, Ethiopia
Correspondence: Awoke Seyoum Tegegne
Department of Statistics, Bahir Dar University, Po. Box 79, Bahir Dar, Ethiopia
Tel +251 918779451
Fax + 251 2205927
Email [email protected]
Background: Globally, HIV/AIDS has challenged the lives of 36.3 million people and resulted in 17 million orphans. The disease has neither a vaccine nor a cure and the only option currently is highly active antiretroviral therapy. This research was conducted to identify the predictors of poor adherence to CART and treatment failure at second-line regimen among adults living with HIV/AIDS in public hospitals of Amhara region, north-western Ethiopia.
Methods: A retrospective cohort study design was conducted on 700 HIV-positive people who were receiving a second-line CART regimen. Participants on second-line regimens who followed their treatment between 2016 and 2019 were considered. Data were extracted from participants’ clinical charts from June 18–July 7, 2020.
Results: A multivariate regression analysis indicates that age of patients (OR = 1.025, 95% CI: 1.001– 1.321; p = 0.005), follow-up visits (OR = 0.979, 95% CI: 0.873– 0.998; p < 0.001), CD4 cell count change (OR = 0.9860; 95% CI: 0.835– 0.998; p < 0.01), marital status (OR = 0.973, 95% CI: 0.789– 0.997; p = 0.006), female HIV-infected patients (OR = 0.990; 95% CI: 0.789– 0.999; p < 0.001), rural patients (OR = 1.151; 95% CI 1.065– 1.398; p = 0.004), non-educated adult patients (OR = 1.026, 95% CI: 1.002– 1.198; p = 0.003), existence of social violence (OR = 0.012, 95% CI: 0.008– 0.134; p< 0.01), patients with opportunistic diseases (OR = 1.0345, 95% CI 1.002– 1.142; p = 0.001), CD4 cell count (OR = 0.901, 95% CI: 0.843– 0.995; p = 0.025) and malnutrition (OR = 0.883, 95% CI; 0.762– 0.954; p = 0.001) significantly affected the two response variables.
Conclusion: Several variables affected both poor adherence to HAART and treatment failure at second-line regimens in the current investigation. Due attention should be given to aged patients, rural residents, non-educated patients, and patients with other morbidities to be successful with second-line treatment regimens.
Keywords: adherence, second-line regimens, bivariate data analysis, treatment failure, HIV/AIDS
Introduction
Acquired Immune Deficiency Syndrome (AIDS) is an infectious disease of the immune system caused by the human immunodeficiency virus (HIV). It is characterized by a decrease in the number of helper T cells, which causes a severe immunodeficiency that leaves the body susceptible to a variety of potentially fatal infections.1 The virus is transmitted through infected body fluids contacted during sexual intercourse, during hypodermic syringes use, and from mother to child during pregnancy, delivery, or breastfeeding.2 HIV/AIDS became the challenge of 36.3 million people and resulted for 17 million orphans.3 Sub-Saharan Africa accounts for 71% of the HIV-infected population and 90% of the AIDS orphans.4
HIV/AIDS has neither a vaccine nor a cure.5 Treatment involves the combination of two non-nucleoside reverse transcriptase inhibitors (NRTIs) and a protease inhibitor (PI) or non-nucleoside reverse transcriptase inhibitor (NNRTI). It is recommended for all people living with HIV regardless of their CD4 cell count or clinical stage.6 Combine Antiretroviral Therapy (CART) prevents the progression of AIDS-defining illness and death by suppressing the virus’s replication or spread, allowing the immune system to recover and fight off other infections.7 It also prevents the transmission of the virus to a sexual partner and to the baby during pregnancy, birth, and breastfeeding.8,9
CART highly impacted HIV/AIDS epidemic. It has averted 1.21 million AIDS-related deaths in 2016 and 1.6 million new HIV infections among children since 1995.10 Currently, an HIV-infected person taking HAART can live for as long as an HIV naïve person.11 CART is one of the essential interventions to end the epidemic by 2030.12 Rigorous measures were taken to increase access to CART to all HIV-infected individuals across the globe and achieve 95% viral suppression by 2025.13 However, only 66% (53–79%) of them have suppressed viral load, which leads to treatment failure.14
An increasing number of patients in Sub-Saharan Africa are experiencing treatment failure to second-line CART.15 Poor adherence, disclosure status, opportunistic infection, CD4 counts < 100 cells/mm3, low BMI, and young age of 15–29 years were identified as the predictors of second-line treatment failure.16 According to the finding of a study by Molla et al., the overall rate of adherence to ART in the University of Gondar was 88.2%. Residence, age, educational status, co-morbidity, HIV disclosure status and CD4 count were associated with adherence.17,18 Social support, absence of depression, and absence of substance use were also reported as determinants of adherence to CART.19 Many studies were conducted on predictors of poor adherence separately but not associated with its effect on second-line regimens.16,17 It is known that poor adherence leads to treatment failure regardless of the treatment line regimens (first or second). The outcome of the current investigation, joint predictors of poor adherence and its consequence on second-line regimen, is important for both patients and health staff for awareness creation on health education. Multivariate data analysis indicates the different dimensions for investigation of potential predictors of the two responses. This is why the current investigation was conducted on predictors of poor adherence and treatment outcome on second-line regimen.
The current study aimed to identify predictors of poor adherence and second-line treatment failure in government hospitals of Amhara region, north-west Ethiopia. The conceptual framework for relationship between covariates is indicated in Figure 1.
 |
Figure 1 Conceptual framework between response and predictor variables in second-line regimens. |
Methods and Materials
Study Design
The study employed a retrospective cohort study design in which participants had been on second-line CART regimens and whose follow ups were between 2016 up to 2019. Data were extracted from the clinical records of participants from June 18–July 07, 2020.
Study Area
Amhara region is the second-most populous region in Ethiopia with an estimated population of 22,191,890.20 The region comprises 15 administrative zones and 180 Woredas (ANRS plan commission report, 2020). According to the 2020 Amhara National Regional State Health Bureau report, the region has one public health institute, 82 hospitals, 870 health centers, 3553 health posts, and 1200 private health facilities. In the region, about 3500 HIV-positive adults are treatment failures at the first-line regimen and are transferred to the second-line regimen.20 Hence, 3500 HIV-positive adults who are on the second-line regimen were considered as study population.
Sample Size and Sampling Procedure
Data were collected from participants in 17 government hospitals in the region. The hospitals were selected purposefully considering the high number of patients on second-line CART regimens. All patients on second-line CART regimens in the above hospitals were included in the study.
Inclusion and Exclusion Criterion
All adults who had switched to the second-line regimen in the region with follow-ups between 2016 and 2019 were included in the current investigation. Patients who attended hospitals with a small number of patients, whose follow-ups were before 2016 or were participants in the selected hospitals who were dropped, died, or transferred out before six months of stay on second-line CART regimen were excluded from this study. Hence, from a total of 3500 HIV-positive adults on the second-line regimen, 700 were selected using a stratified random sampling technique considering the selected hospitals as strata, using 95% level of confidence and 5% marginal error which indicates that the sample size was statistically valid to give a consistent result.20
Variables
Dependent Variable
The dependent variables in the current investigation were adherence level and treatment failure to second-line regimen. The first dependent variable was binary in nature (adherent or non-adherent (poor)). The second response variable was also a binary response which was categorized as treatment failure or success. A treatment is said to be failed (virological failure) if plasma viral load after 6 months on second-line ART was above 1000 copies/mL for the second time following the high viral load (>1000 copies/mL) in the first measurement.21
Independent Variable
Patients’ age (in years), sex, marital status, level of education, religion, residence, occupation, partner’s HIV status, functional status at the start of ART, opportunistic infection at the time of the switch to second-line regimen, HBV status at the time of the switch to second-line regimen, presence of chronic disease, history of drug toxicity, history of missed appointment while on second line regimen, HIV disclosure status, WHO clinical stage at the switch to second-line regimen, CD4 count at the switch to the second line regimen and viral load were independent variables.
Data Collection Procedure
Secondary data were used for this study. The data were collected from the health facilities’ ART follow-up clinic charts. It was collected by health professionals working in the ART clinics in the region.
Data Collection Tool
The data were collected through the Open Data Kit (ODK). It is a free, open-source suite of tools that allows data collection using android mobile devices and data submission to an online server, even without an internet connection or mobile carrier service at the time of data collection.22 The data collection procedure was closely supervised for assuring the quality of the data. The collected data were checked for completeness, accuracy, and clarity by taking samples.
Test of Missingness Patterns
Among the three types of missingness patterns namely, missing at random (MAR), missing completely at random (MCAR) and missing not at random (MNAR) were considered in current investigation using ANOVA and confirmed that the nature of the missingness pattern in the current investigation was Missed Completely at Random (MCAR). This indicates that missingness increased as visiting time increased.
Data Analysis
The secondary data were entered and analyzed using SAS statistical software package, version 9.2. The descriptive data analysis was conducted using frequency distribution.
Statistical Models Used in Data Analysis
In this investigation, multivariate data analysis was employed, considering binary logistic regression to be applied for the two responses with logit transformation. The result showed a binomial response conducted with a logistic regression model with the logit link function.
Before conducting the multivariate data analysis, separate models were conducted for each response using the binary logistic regression models for virological failure and adherence status.23 The covariance structure and the magnitude of residual errors were also measured in the model selection. In this regard, the model with the smallest residual error was selected.24
Formulation of Multivariate Regression Analysis
The generalized linear mixed model assumes each outcome to be binary; first the univariate models were conducted and combined through the specification of joint multivariate distribution for all random effects.
For the assessment of the relation between two responses (poor adherence and treatment failure to CART), the multivariate data analysis, particularly, joint GLMM model was fitted.25 In this model, the association between the two outcomes was quantified through the random effect given that separate random intercept for each outcome variable has been conducted.26
Results
The baseline characteristics of the current investigation are indicated in Tables 1 and 2. Tables 1 and 2 show that about 54% of the participants were female, 45% of them were married, 68.9% of the participants were literate, and the majority of the participants (84.4%) were Orthodox religious followers.
 |
Table 1 Baseline Characteristics of Participants (n = 700), Socio-Demographic Variables |
 |
Table 2 Baseline Characteristics of Participants (n = 700), Clinical Variables |
Among the participants, about 77.3% were urban residents, 32.7% them had HIV-positive partners, 81% of them had working status, 5.8% of them were TB co-infected patients, 3.9% of the HIV people at second-line regimens had experienced mental depression, 3.9% of them were pregnant mothers, 18.3% of these patients had CD4 cell count of less than 100 and about 3.4% of them did not disclose their disease status. Finally, about 60.7% of the participants were non-adherent (poor adherence) to CART and 59% of them had treatment failure at second-line regimens (Tables 1 and 2).
In the analysis, among the patients who disclosed the disease, 96.6%, reported that they got better social support from communities around them.
The covariance structure under the current investigation was tested using information criteria (AIC and BIC) as shown in Table 3.
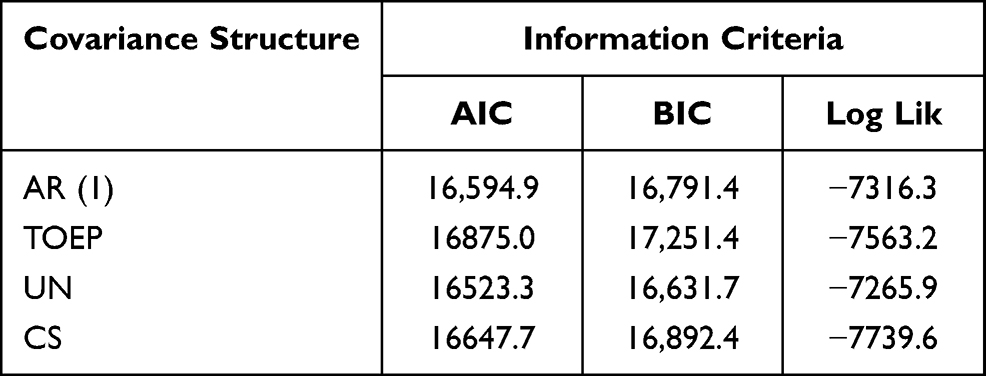 |
Table 3 Covariance Structure Under Current Investigation |
The bivariate estimate of the two responses, namely adherence to CART and treatment success at second-line regimens, is indicated in Table 4.
 |
Table 4 Multivariate Regression Analysis for Adherence to HAART and Treatment Failure Using Maximum Likelihood Estimation |
To assess the determinants of the two responses, a multivariate data analysis approach becomes more relevant. Developing models for the two response variables with uncorrelated random intercepts gives results for an initial parameter estimate. The results obtained by applying this procedure are indicated in Table 4. The multivariate data analysis was conducted using log-likelihood estimation. The SAS procedures used in generalized mixed effect models allow the bivariate data analysis to be constructed for the random effects.
This shows how to construct multivariate longitudinal data by supposing univariate random effects from a generalized mixed-effect approach for each outcome variable. Parameter estimates for the conditional independence of the random intercept model for responses namely adherence to CART and treatment outcome at second-line regimens are indicated in Table 4 .
The identical signs for the two predictors indicate that they are positively correlated with each other. Hence, patients with poor medication adherence also had treatment failure at second-line regimens. To conduct the multivariate data analysis for the two responses, the conditional assumptions of the subject-specific intercept were conducted as shown in Table 4.
Table 4 indicates that predictors such as age of patients, baseline CD4 cell count, the number of followed-up visits, marital status, CART adherence, sex, residence area and cell phone ownership, the existence of social support, social discrimination, mental stress, and level of adherence to CART had a significant effect on the variable of interest.
As age of patients increased by one year, the expected odds of having poor adherence to CART was increased by 2.5% assuming the other things were constant (OR = 1.025, 95% CI 1.001–1.321; p = 0.005). Age also affected the treatment outcome at second-line regimens. Hence, as age increased by one year, the expected odds of being a treatment failure at second-line regimens was increased by 13% (OR = 1.129, 95% CI: 1.087–1.235; p <0.01).
On the other hand, as the number of follow-up visits increased by one unit, the expected value of the odds of having poor adherence to CART was decreased by 2.1% provided the other covariates remain constant (OR = 0.979, 95% CI: 0.873–0.998; p-value < 0.001) and the expected value of being a treatment failure in second-line regimens was decreased by 3.7% (OR = 0.9675, 95% CI: 0.8925–0.9987; p = 0.012).
As CD4 cell count change increased by one cell/mm3, the expected value of odds of having poor adherence to CART was decreased by 1.4% given the other covariates were constant (OR = 0.9860; 95% CI 0.835–0.998; p < 0.01) and the expected value of treatment failure in second-line regimens was decreased by 2.2% (OR = 0.978; 95% CI: 0.857– 0.998; p < 0.001).
Comparing female HIV-infected patients with males, the expected value of odds of having poor adherence for female HIV-positive patients was decreased by 1% as compared with male patients (OR = 0.990; 95% CI: 0.789–0.999), p < 0.001). Similarly, the expected odds of being a treatment failure for female patients was decreased by 1.4% as compared with male patients (OR = 0.986; 95% CI: 0.798–0.998; p< 0.001).
However, the expected odds of having poor adherence for rural patients was increased by 15% as compared with urban patients, given the other covariates were kept constant (OR = 1.151; 95% CI: 1.065–1.398; p = 0.004).
The expected odds of having poor adherence for non-educated adult patients was increased by 2.6% compared with educated adults, other factors being constant (OR = 1.026, 95% CI: 1.002–1.198; p = 0.003). Similarly, the expected value of being a treatment failure for non-educated patients was also increased by 13.3% compared with educated patients (OR = 1.133, 95% CI: (1.034–1.234; p = 0.012), other factors being kept constant.
The existence of social violence had a statistically significant effect on the poor adherence of HIV-positive adults. Hence, the expected odds of having poor adherence for HIV-infected individuals, where there is no social violence, was decreased by 1.2% compared with those HIV-infected adults living in societies where there is social violence, other factors being kept constant (OR = 0.012, 95% CI: 0.008–0.134; p< 0.01).
The expected odds of having poor adherence for patients with opportunistic diseases was increased by 3.5% compared with non-opportunistic infectious disease patients, otherfactors being kept constant (OR = 1.0345, 95% CI: 1.002–1.142; p = 0.001).
The expected odds of being poor adherent for patients with opportunistic diseases was increased by 3.5% compared with non-opportunistic infectious disease patients, other factors being kept constant (OR = 1.0345, 95% CI: 1.002–1.142; p = 0.001).
As, CD4 cell count increased by 1 cell/mm3 of the blood, the expected value of having poor adherence for HIV-positive patients was decreased by 10%, other factors being kept constant (OR = 0.901, 95% CI: 0.843–0.995; p = 0.025).
The expected odds of having poor adherence for patients who did not get malnutrition was decreased by 12% compared with patients with malnutrition, other factors being kept constant (OR = 0.883, 95% CI: 0.762–0.954; p = 0.001).
Discussion
The current study tried to identify factors affecting the bivariate effect of poor adherence and treatment failure for HIV-positive adults under second-line CART regimens. The extent of poor adherence of the HIV-positive adults indicates that 60.7% of them had poor adherence on the second-line regimens and about 59% of the participants got treatment failure.
Age significantly affects the level of adherence and treatment outcome at second-line regimens. Hence, as age increases, having poor adherence for HIV-positive adults also increases. It is known that aged patients may forget to take medications at the prescribed time and date and this leads to patients having poor adherence. Hence, older HIV-infected individuals are more likely to have poor adherence, and this contributes to the patients being virally suppressed and failure at second-line treatment.27,28 Older HIV-positive patients, who have a high probability of having poor adherence, are thus more likely to get treatment failure at second-line treatment CART regimens.29
HIV-positive people with a low baseline CD4 cell count are more likely to have poor adherence and such patients got treatment failure at second-line CART regimens.30 This is why the two responses have a positive association between them.
As visiting time of the health institution increases the possibility of having poor adherence decreases and leads to patients being successful at second-line CART regimens. This result is similar to other previous research.31 When HIV-positive adults visit the health institution as prescribed by the health staff, such people should receive proper medication and this leads to being successful in second-line regimens.32 Hence, short visiting times harm patients, who are more likely to have poor adherence because of education and counseling should be given to patients at each visiting time.
Female HIV-positive adults are less likely to have poor adherence compared with males. The possible reason for this might be the fact that a female’s experience in taking pills for birth control plays a significant role in being medication adherent for cART and this further leads to being less likely to fail at second-line regimens.33 The experience gained from pills taken for family planning contributed for females to be CART adherent. This result is supported by previous research34 but is contradictory with another investigation.35 The reason for the contradictory result is that females hide their disease because of their fear of being stigmatized and exposed for the extra infectious disease, which leads them to have poor adherence and failed at second-line treatment regimen.35 This result also needs further investigation.
Urban HIV-positive adults are less likely to have poor adherence compared with rural HIV-positive adults. Urban patients might have a better level of education and better understanding of how poor adherence is related to treatment failure at second-line regimens compared with rural patients.36 Most of the time, rural patients come to health facilities for HIV diagnosis lately, due to cultural impact and other priorities given by rural people. This is because of the reason that societies in the rural area lack awareness on how and when a patient being virally suppressed and failed at treatment outcomes.36
Social violence has a significant effect on the likelihood of HIV-positive people having poor adherence because HIV-positive people in such situations may not disclose their disease status to their sexual partners and communities. Non-disclosure of the disease leads the patients to have poor adherence and this further leads to treatment failure on second-line CART regimens. The potential reason for this might be HIV-infected adults fear the trend that those individuals who disclose their disease experience violence from people they are living together with.37 Social violence also contributed positively for HIV-patients to have poor adherence (patients may not take pills whenever other individuals are there) which leads patients to be drug resistant and to get treatment failure at second-line regimens.
Education plays a significant role in the variation of the level of adherence and treatment outcomes at second-line regimes. Educated people are less likely to have poor adherence and to failed at second-line treatment regimens.38 The potential reason for this might be the fact that such people have more information on what HIV-positive people need to do in order to be successful in treatment outcomes. Educated HIV-positive people also have a better understanding of how the virus can be transmitted from one patient to another.39 Knowledge on how to prevent HIV transmission is important in the disclosure of HIV status and this helps for patients to be virally suppressed and to have progressive CD4 cell count change.39
Conclusion
In the current investigation, certain significant covariates on the two response variables, namely poor adherence and treatment failure, have been identified. The prevalence of poor adherence in the study area was 60.7% and that of treatment failure at second-line CART regimens was 59%. Hence, the two results indicate that more than 50% of the program needs more attention for patients to have long lives with the virus.
Common predictors were identified in the current investigation and the association between the two responses indicates that the two responses are highly correlated with each other. Hence, patients with poor adherence have a high probability of being virally suppressed and failed treatment outcomes at second-line regimes.
Due attention should be given to poor adherent HIV-positive individuals with poor adherence since it leads to treatment failure at second-line CART regimens. Hence, health-related education for HIV-positive adults is crucial to be CART adherent and to be successful at second-line CART regimens. Special support should be given for aged and rural patients, for patients whoare not aworking and for those who had low CD4 cell counts, in order for them to live longer with HIV.
Data Sharing Statement
The data used for the current investigation is within the hands of the corresponding author.
Ethical Approval and Consent for Participate
Informed consent has been waived, because the data were secondary and there was no chance of communication between investigators and respondents. To secure the confidentiality and compliance with the Declaration of Helsinki within the manuscript of patient related data, the name of patients was not given to investigators, rather id number and important variables related to current investigation were given to researchers. The waiver was done by Bahir Dar University Ethical approval committee, Ethiopia with reference number: RCS/1412/2021. Hence, the Bahir Dar University Ethical Committee approved this study.
Consent for Publication
This manuscript is not published in any journal or not under consideration by any other journals.
Author Contributions
All authors made a significant contribution in the conception, study design, execution and acquisition of data, analysis and interpretation. The authors also participated equally in drafting, revising or critically reviewing the article; gave final approval of the version to be published and have agreed on the journal to which the article has been submitted. Authors agreed to be accountable for all aspects of the work.
Disclosure
Authors declared that there are no conflicts of interest in this work.
References
1. Wittner M. Characterization of α4β7 integrin and CD32 expression of CD4+ memory T-cell subsets at different stages of HIV infection. Stats-und Universitätsbibliothek Hamburg Carl von Ossietzky; 2020.
2. Okoye AA, Picker LJ. CD 4+ T‐cell depletion in HIV infection: mechanisms of immunological failure. Immunol Rev. 2013;254(1):54–64. doi:10.1111/imr.12066
3. Ilo PI, Adeyemi A. HIV/AIDS information awareness among market women: a study of Olofimuyin Market, Sango-Ota, Ogun State, Nigeria. Libr Philos Pract. 2010;1:340.
4. Lowenthal ED, Bakeera-Kitaka S, Marukutira T, et al. Perinatally acquired HIV infection in adolescents from sub-Saharan Africa: a review of emerging challenges. Lancet Infect Dis. 2014;14(7):627–639. doi:10.1016/S1473-3099(13)70363-3
5. Rhodes SD, Malow RM, Jolly C. Community-based participatory research: a new and not-so-new approach to HIV/AIDS prevention, care, and treatment. AIDS Educ Prev. 2010;22(3):173–183. doi:10.1521/aeap.2010.22.3.173
6. de Béthune MP. Non-nucleoside reverse transcriptase inhibitors (NNRTIs), their discovery, development, and use in the treatment of HIV-1 infection: a review of the last 20 years (1989–2009). Antiviral Res. 2010;85(1):75–90. doi:10.1016/j.antiviral.2009.09.008
7. Ripamonti D, Bombana E, Rizzi M. Rilpivirine: drug profile of a second-generation non-nucleoside reverse transcriptase HIV-inhibitor. Expert Rev Anti Infect Ther. 2014;12(1):13–29. doi:10.1586/14787210.2014.863708
8. World Health Organization. WHO technical brief: preventing HIV during pregnancy and breastfeeding in the context of PrEP. World Health Organization; 2017.
9. Silasi M, Cardenas I, Kwon JY, et al. Viral infections during pregnancy. Am J Reprod Immunol. 2015;73(3):199–213. doi:10.1111/aji.12355
10. Kuleape JA. Glutathione S-transferase gene polymorphism and antioxidant enzymes activity in hiv/aids progression in ghanaian patients. University of Ghana; 2016.
11. Pangmekeh PJ, Awolu MM, Gustave S, et al. Association between highly active antiretroviral therapy (HAART) and hypertension in persons living with HIV/AIDS at the Bamenda regional hospital, Cameroon. Pan Afr Med J. 2019;33:87.
12. Gleeson HS, Oliveras Rodriguez CA, Hatane L, et al. Ending AIDS by 2030: the importance of an interlinked approach and meaningful youth leadership. J Int AIDS Soc. 2018;21:e25061. doi:10.1002/jia2.25061
13. Shah M, Perry A, Risher K, et al. Effect of the US National HIV/AIDS strategy targets for improved HIV care engagement: a modeling study. Lancet HIV. 2016;3(3):e140–e146. doi:10.1016/S2352-3018(16)00007-2
14. Kim SH, Gerver SM, Fidler S, et al. Adherence to antiretroviral therapy in adolescents living with HIV: systematic review and meta-analysis. AIDS. 2014;28(13):1945. doi:10.1097/QAD.0000000000000316
15. Barth RE, van der Loeff MFS, Schuurman R, et al. Virological follow-up of adult patients in antiretroviral treatment programs in sub-Saharan Africa: a systematic review. Lancet Infect Dis. 2010;10(3):155–166. doi:10.1016/S1473-3099(09)70328-7
16. Anude CJ, Eze E, Onyegbutulem HC, et al. Immuno-virologic outcomes and immuno-virologic discordance among adults alive and on antiretroviral therapy at 12 months in Nigeria. BMC Infect Dis. 2013;13(1):1–19. doi:10.1186/1471-2334-13-113
17. Molla AA, Gelagay AA, Mekonnen HS, et al. Adherence to antiretroviral therapy and associated factors among HIV positive adults attending care and treatment in University of Gondar Referral Hospital, Northwest Ethiopia. BMC Infect Dis. 2018;18(1):1–8. doi:10.1186/s12879-018-3176-8
18. Zenebe Haftu A, Desta AA, Bezabih NM, et al. Incidence and factors associated with treatment failure among HIV infected adolescent and adult patients on second-line antiretroviral therapy in public hospitals of Northern Ethiopia: multicenter retrospective study. PLoS One. 2020;15(9):e0239191. doi:10.1371/journal.pone.0239191
19. Kalichman SC, Cherry C, Amaral C, et al. Health and treatment implications of food insufficiency among people living with HIV/AIDS, Atlanta, Georgia. J Urban Health. 2010;87(4):631–641. doi:10.1007/s11524-010-9446-4
20. Ferede A, Kibret GD, Million Y, et al. Magnitude of turnover intention and associated factors among health professionals working in public health institutions of North Shoa Zone, Amhara Region, Ethiopia. Biomed Res Int. 2018;2018. doi:10.1155/2018/3165379
21. Mee P, Fielding KL, Charalambous S, et al. Evaluation of the WHO criteria for antiretroviral treatment failure among adults in South Africa. AIDS. 2008;22(15):1971–1977. doi:10.1097/QAD.0b013e32830e4cd8
22. Brunette W, Sundt M, Dell N, et al. Open data kit 2.0: expanding and refining information services for developing regions.
23. Midi H, Sarkar SK, Rana S. Collinearity diagnostics of the binary logistic regression model. J Interdiscip Math. 2010;13(3):253–267. doi:10.1080/09720502.2010.10700699
24. West SG, Taylor AB, Wu W. Model fit and model selection in structural equation modeling. Handb Struct Equ Modeling. 2012;1:209–231.
25. Do NT, Phiri K, Bussmann H, et al. Psychosocial factors affecting medication adherence among HIV-1 infected adults receiving combination antiretroviral therapy (cART) in Botswana. AIDS Res Hum Retroviruses. 2010;26(6):685–691. doi:10.1089/aid.2009.0222
26. Picheny V, Casadebaig P, Trépos R, et al. Using numerical plant models and phenotypic correlation space to design achievable ideotypes. Plant Cell Environ. 2017;40(9):1926–1939. doi:10.1111/pce.13001
27. Tshweneagae GT, Oss VM, Mgutshini T. Disclosure of HIV status to sexual partners by people living with HIV. Curationis. 2015;38(1):1–6. doi:10.4102/curationis.v38i1.1174
28. Lemin AS, Rahman MM, Pangarah CA. Factors affecting intention to disclose HIV status among adult population in Sarawak, Malaysia. J Environ Public Health. 2018;2018. doi:10.1155/2018/2194791
29. Lekas HM, Schrimshaw EW, Siegel K. Pathways to HIV testing among adults aged fifty and older with HIV/AIDS. AIDS Care. 2005;17(6):674–687. doi:10.1080/09540120412331336670
30. Strachan ED, Bennett WR, Russo J, et al. Disclosure of HIV status and sexual orientation independently predicts increased absolute CD4 cell counts over time for psychiatric patients. Psychosom Med. 2007;69(1):74–80. doi:10.1097/01.psy.0000249900.34885.46
31. Treves-Kagan S, Steward WT, Ntswane L, et al. Why increasing availability of ART is not enough: a rapid, community-based study on how HIV-related stigma impacts engagement to care in rural South Africa. BMC Public Health. 2015;16(1):1–13. doi:10.1186/s12889-016-2753-2
32. Alli F, Maharaj P, Vawda MY. Interpersonal relations between health care workers and young clients: barriers to accessing sexual and reproductive health care. J Community Health. 2013;38(1):150–155. doi:10.1007/s10900-012-9595-3
33. Ssali SN, Atuyambe L, Tumwine C, et al. Reasons for disclosure of HIV status by people living with HIV/AIDS and in HIV care in Uganda: an exploratory study. AIDS Patient Care STDS. 2010;24(10):675–681. doi:10.1089/apc.2010.0062
34. Reniers G, Armbruster B. HIV status awareness, partnership dissolution and HIV transmission in generalized epidemics. PLoS One. 2012;7(12):e50669. doi:10.1371/journal.pone.0050669
35. Amin A. Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. J Int AIDS Soc. 2015;18:20302.
36. Thior I, Rowley E, Mavhu W, et al. Urban-rural disparity in sociodemographic characteristics and sexual behaviors of HIV-positive adolescent girls and young women and their perspectives on their male sexual partners: a cross-sectional study in Zimbabwe. PLoS One. 2020;15(4):e0230823. doi:10.1371/journal.pone.0230823
37. Deribe K, Woldemichael K, Wondafrash M, et al. Disclosure experience and associated factors among HIV positive men and women clinical service users in southwest Ethiopia. BMC Public Health. 2008;8(1):1–10. doi:10.1186/1471-2458-8-81
38. Binagwaho A, Murekatete I, Rukundo A, et al. Factors associated with disclosure of HIV status among HIV positive children in Rwanda. Rwanda Med J. 2012;69(3):9–15.
39. Simmons JV, Carcioppolo N, Peng W, et al. 90 DAYS: an investigation of a short entertainment-education film to improve HIV status disclosure among black women living with HIV in Miami-Dade County. Soc Sci Med. 2021;270:113683. doi:10.1016/j.socscimed.2021.113683
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.