")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Potential Underestimation of Left Ventricular Mechanical Dyssynchrony in Dyssynchrony and Outcomes Assessment
Authors Zhou Z, Ma F, Zhu J, Wang J, Zhang J, Zhao D
Received 16 November 2023
Accepted for publication 5 April 2024
Published 20 April 2024 Volume 2024:17 Pages 1721—1729
DOI https://doi.org/10.2147/JMDH.S450264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zhongyin Zhou,1,* Feiyan Ma,2,* Jianxiang Zhu,1 Jialing Wang,1 Jing Zhang,3 Dongsheng Zhao4
1Department of Echocardiography, Affiliated Hospital 2 of Nantong University, First People’s Hospital of Nantong City, Nantong, 226000, People’s Republic of China; 2Department of Ultrasound, the People’s Hospital of Rugao, Nantong, 226000, People’s Republic of China; 3Department of Electroencephalogram, Affiliated Hospital 2 of Nantong University, First People’s Hospital of Nantong City, Nantong, 226000, People’s Republic of China; 4Department of Cardiology, Affiliated Hospital 2 of Nantong University, First People’s Hospital of Nantong City, Nantong, 226000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongsheng Zhao, Department of Cardiology, Affiliated Hospital 2 of Nantong University, First People’s Hospital of Nantong City, No. 666 Shengli Road, Nantong, 226006, People’s Republic of China, Tel +86 13814710785, Email [email protected]
Objective: Left ventricular (LV) mechanical dyssynchrony (LVMD) is fundamental to the progression of heart failure and ventricular remodeling. The status of LVMD in different patterns of bundle branch blocks (BBB) is unclear. In this study, we analyzed the relationship between LVMD and left ventricular systolic dysfunction using real-time three-dimensional echocardiography (RT-3DE).
Methods: RT-3DE and conventional two-dimensional echocardiography were performed on 68 patients with left bundle branch block (LBBB group), 106 patients with right bundle branch block (RBBB group), and 103 patients without BBB (Normal group). The RT-3DE data sets provided time-volume analysis for global and segmental LV volumes. The LV systolic dyssynchrony index (LVSDI) was calculated using the standard deviation (SD) and maximal difference (Dif) of time to minimum segmental volume (tmsv) for LV segments adjusted by the R-R interval. LVMD was considered if the LVSDI (Tmsv-16-SD) was greater than or equal to 5%.
Results: LVSDI is negatively and significantly correlated with left ventricular ejection fraction (LVEF), but not with BBB or QRS duration. The proportion of LVMD in the LBBB, RBBB, and Normal group was 30.88%, 28.30%, and 25.24%, respectively, and there was no significant difference.
Conclusion: In dilated cardiomyopathy, LVMD is more closely related to LVEF reduction than QRS morphology and duration.
Keywords: bundle branch block, dilated cardiomyopathy, mechanical dyssynchrony
Introduction
Patients with chronic heart failure (HF) usually have cardiac enlargement and cardiac mechanical dyssynchrony. Cardiac mechanical dyssynchrony further aggravate the symptoms of patients. Cardiac mechanical dyssynchrony is divided into three aspects: (1) atrioventricular synchrony: left atrium and left ventricle movement coordination and their diastolic relationship. (2) Interventricular synchrony: It focuses on the coordination of movement and contraction between the right and left ventricles. (3) Ventricular synchrony: It focuses on the coordination of movement and contraction of the left ventricular myocardium. Cardiac mechanical dyssynchrony, particularly left ventricular mechanical dyssynchrony (LVMD), has been identified as an important substrate and malignant prognostic factor of heart failure (HF), which can be partially corrected by cardiac resynchronization therapy (CRT) using bi-ventricular pacing.1–3 Despite the fact that CRT is currently considered a class I indication in patients with drug-refractory heart failure and a QRS duration ≥ 150 ms, nearly 30% of patients do not show improvements in clinical symptoms and 40–50% do not exhibit significant LV reverse remodeling after CRT.4 Recently, some studies have discovered that electrocardiographic dyssynchrony (QRS duration) is not always correlated with mechanical dyssynchrony and that rectifying LVMD is beneficial in increasing the rate of response to CRT.3,5,6 Few studies have been conducted to date on the relationship between the LVMD and ventricular electroexcitation mode (QRS morphology and duration) in patients with or without HF. This is an important issue for better identifying candidates who may benefit from CRT. In the past decade, real-time three-dimensional echocardiography (RT-3DE) has been established and validated as a convenient, reliable, and reproducible technique for assessing LVMD through simultaneous evaluation of multiple regional systolic changes of the LV volume and calculation of a global systolic dyssynchrony index (SDI) against angiography, radionuclide angiography, and magnetic resonance imaging (MRI).7–9 In this study, we used RT-3DE to evaluate LVMD in patients with DCM and healthy controls with different QRS morphology and duration in order to investigate their correlation and contribution to HF (dilated cardiomyopathy (DCM)).
Materials and Methods
A total of 277 patients admitted to the Second Affiliated Hospital of Nantong University between October 2010 and January 2018 were included in the single-center observational study. Among them, 76 patients with heart failure (HF) were diagnosed with dilated cardiomyopathy (HF group) and 201 patients were without heart failure (non-heart failure group). TF is a complex clinical syndrome, which includes three aspects: (1) abnormal cardiac structure and/or function leading to impaired ventricular filling (diastolic function) and/or ejection capacity (systolic function); (2) Produce the corresponding clinical symptoms and (or) signs related to heart failure; (3) It is usually accompanied by elevated levels of beneficial natriuretic peptides, and/or objective evidence of cardiogenic pulmonary or systemic congestion on imaging, or elevated ventricular filling pressure on hemodynamic examination.
Patients with non-sinus rhythm, prior pacemaker implantation, a history of myocardial infarction and severe coronary stenosis (≥70%), asymmetric hypertrophic cardiomyopathy, and valvular heart disease were excluded. All the participants underwent a standard 12-lead electrocardiography and a complete 2D/3D echocardiographic examination, including a specific LVMD evaluation. The participants were divided into three groups based on QRS morphology: 68 participants (20 in the HF group, 48 in the NHF group) with left bundle branch blocks (LBBB), 106 participants (30 in the HF group, 76 in the NHF group) with right bundle branch blocks (RBBB), and 103 participants (26 in the HF group, 77 in the NHF group) without bundle branch block (Normal). This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of Affiliated Hospital 2 of Nantong University. Written informed consent was obtained from all participants.
Standard 12-lead electrocardiograms were acquired using a scale of 10 mm/mV and a paper speed of 25 mm/s. Two independent electrophysiologists who were blinded to the clinical status of the participants conducted the measurements of QRS duration (recorded from the surface leads demonstrating the greatest values) and the assessment of QRS morphology.
Prior to RT-3DE, a conventional two-dimensional (2D) echocardiographic examination (IE 33, Philips Medical System, Andover, USA) was undertaken using a 1–5 MHz phased array transducer. The participants were examined in the left lateral decubitus position to optimize the image. Two-dimensional LV volumes and ejection fractions were assessed using the biplane Simpson method.10 RT-3DE studies were conducted using the iE33 ultrasound system with an S5-1 transducer (Philips Medical Systems, Andover, MA, USA) according to the guidelines. As previously described, three-dimensional datasets were acquired in the apical window with an ECG-gated acquisition.11 Dedicated software incorporated into the system enabled the acquisition of four small sub-volumes in real-time from alternate cardiac cycles. Subsequently, a pyramidal volume was obtained by capturing the LV in its entirety. The 3D studies were considered unsuitable for analysis if more than two segments could not be visualized or if they contained visible translation artifacts. On average, three or more cardiac cycles were analyzed by two experienced investigators who were blinded to the etiology and clinical status of the patients.
As previously described, RT-3DE datasets were analyzed using 3D-Advanced Quantification 6.0 (Philips Medical Systems) on a QLAB workstation.9 The 3D software displayed the volume-time curves for the 17 segments in which the LV volume was divided. The time to minimal systolic volume (Tmsv) in 16 segments (excluding the true apex) was identified, and the derived systolic synchrony indices were automatically calculated, including: (i) standard deviation of Tmsv in all 16 LV segments (Tmsv-16-SD); (ii) standard deviation of Tmsv in 6 basal and 6 mid segments (Tmsv-12-SD); (iii) standard deviation of Tmsv in 6 basal segments (Tmsv-6-SD); (iv) maximal difference of Tmsv among all 16 segments (Tmsv-16-Dif); (v) maximal difference of Tmsv of 6 basal and 6 mid segments (Tmsv-12- Dif); and (vi) maximal difference of Tmsv of 6 basal segments (Tmsv-6-Dif). The segments correspond to the LV 16-segment model as described by the American Society of Echocardiography. All these six parameters were finally expressed as (%R-R) Tmsv after R-R interval adjustment.8 Therefore, those participants with higher indices were more significantly identified as having LVMD. LVMD was considered if the LVSDI (Tmsv-16-SD) was >/= 5%.7,9
The data was analyzed using SPSS version 22. The median and interquartile range (IQR) represent continuous variables. Categorial variables are expressed as frequencies in numbers (n) and percentages (%) of participants. The Mann–Whitney test was used to compare LVMD status for continuous variables and the Pearson’s chi-squared test for categorical variables. Partial correlation analyses were used to analyze correlations between LV synchronicity parameters, LVEF, and QRS width. LVSDIs from DCM and NHF participants were analyzed using a receiver operating characteristics (ROC) curve analysis. The area under the curve (AUC) with a 95% coefficient index (CI) and optimal cut-off (Youden’s index) was calculated. The DeLong method was used for the comparison of two ROC curves. Multivariable and logistic binomial regressions were used to estimate the independent risk variables of BBB and DCM. A two-tailed P <0.05 was considered statistically significant.
Results
Among the 277 evaluated participants, 188 were male, with a median age of 60 and an interquartile range of 17 years. Table 1 displays the stratification of participant characteristics based on QRS morphology. There is no significant difference between the three QRS groups in the distribution of HF, hypertension, diabetes, and the majority of LVSDIs. In Table 2, multivariable logistic regression shows that the LVSDIs have no correlation with either LBBB or RBBB after adjusting for age, hypertension, diabetes, QRS width, and LVEF.
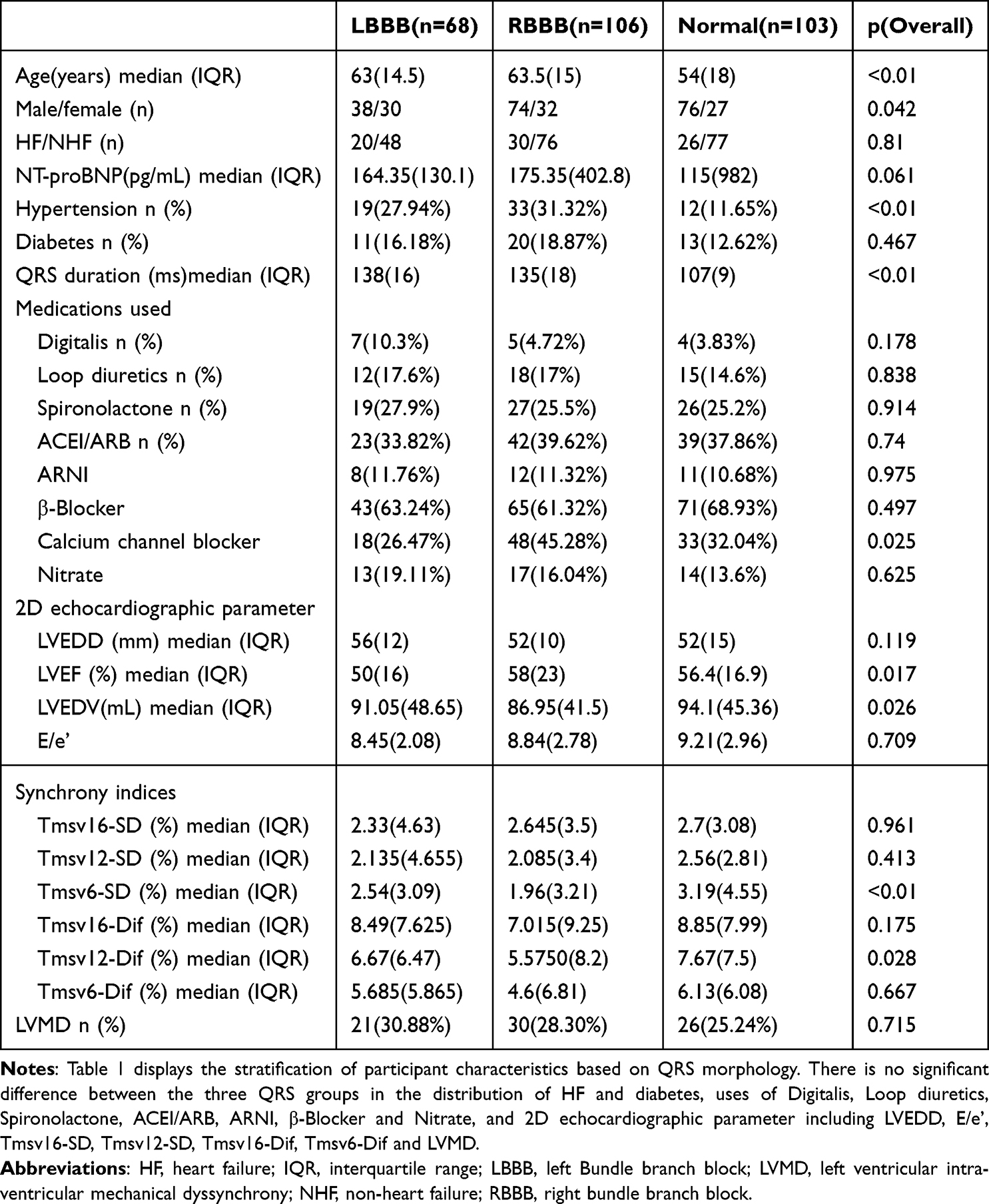 |
Table 1 The Clinical Characteristics and Ultrasonic Parameters of the Three QRS Groups. P: Level of Significance |
 |
Table 2 LVSDI in Multivariable Logistic Regression of BBB. Other Included Variables: Age, Hypertension, Diabetes, QRS Duration, LVEF. RR: Risk Ratio; P: Level of Significance |
After applying the QRS adjustment, all LVSDIs were significantly and negatively correlated with LVEF. There was no independent correlation between LVSDI and QRS width. QRS width and LVEF also play a role, as shown in Table 3. As displayed in Figure 1, all the LVSDIs are significantly higher in the DCM group. Figure 2 depicts the ROC curve. Subgroup ROC curve analysis based on QRS morphology revealed that Tmsv16-Dif had the highest DCM diagnostic efficiency in the RBBB group (AUC = 0.842, P < 0.001), which was equivalent to NT-proBNP (P = 0.43) but had no DCM diagnostic efficiency in the LBBB group, similar to NT-proBNP. (Figure 3)
 |
Table 3 Partial Correlation Analyses of LVSDIs, LVEF and QRS Duration. R: Correlation Coefficient; P: Level of Significance |
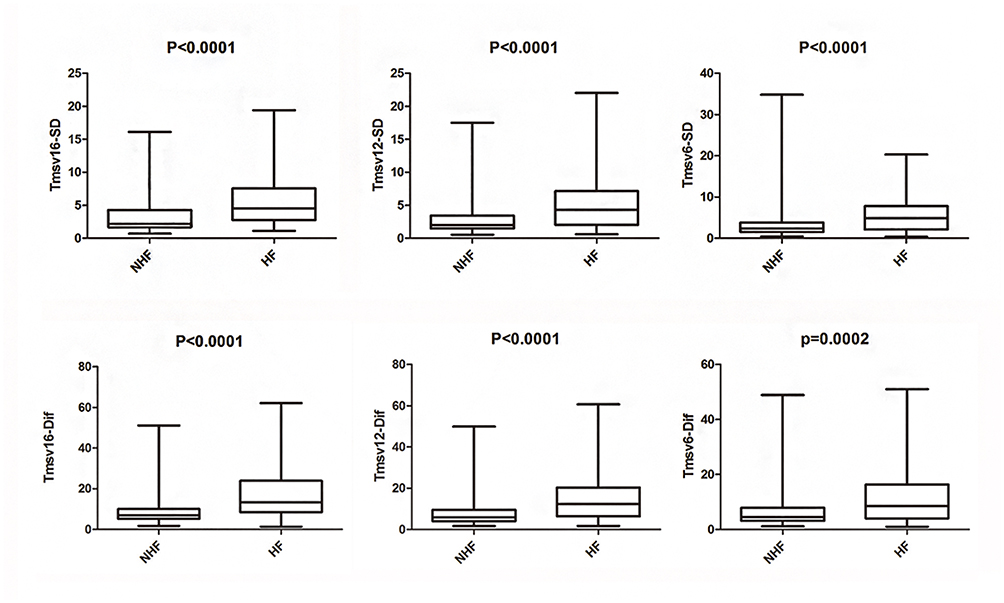 |
Figure 1 Comparison of LVSDIs between the HF and NHF groups. Nonparametric tests of two independent samples with the Mann–Whitney test are used for the difference examination. Abbreviations: LVSDI, left ventricular systolic dyssynchrony index; P, level of significance. |
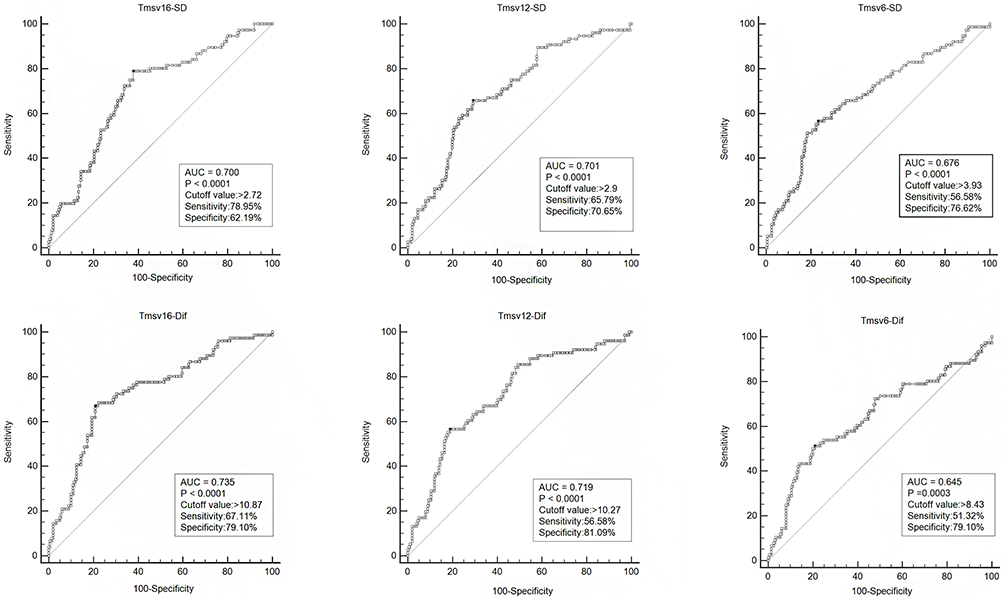 |
Figure 2 The ROC curve analysis of LVSDIs between patients with dilated cardiomyopathy (HF) and non-heart failure (NHF) participants. Abbreviations: LVSDI, left ventricular systolic dyssynchrony index; AUC, area under the curve; P, level of significance. |
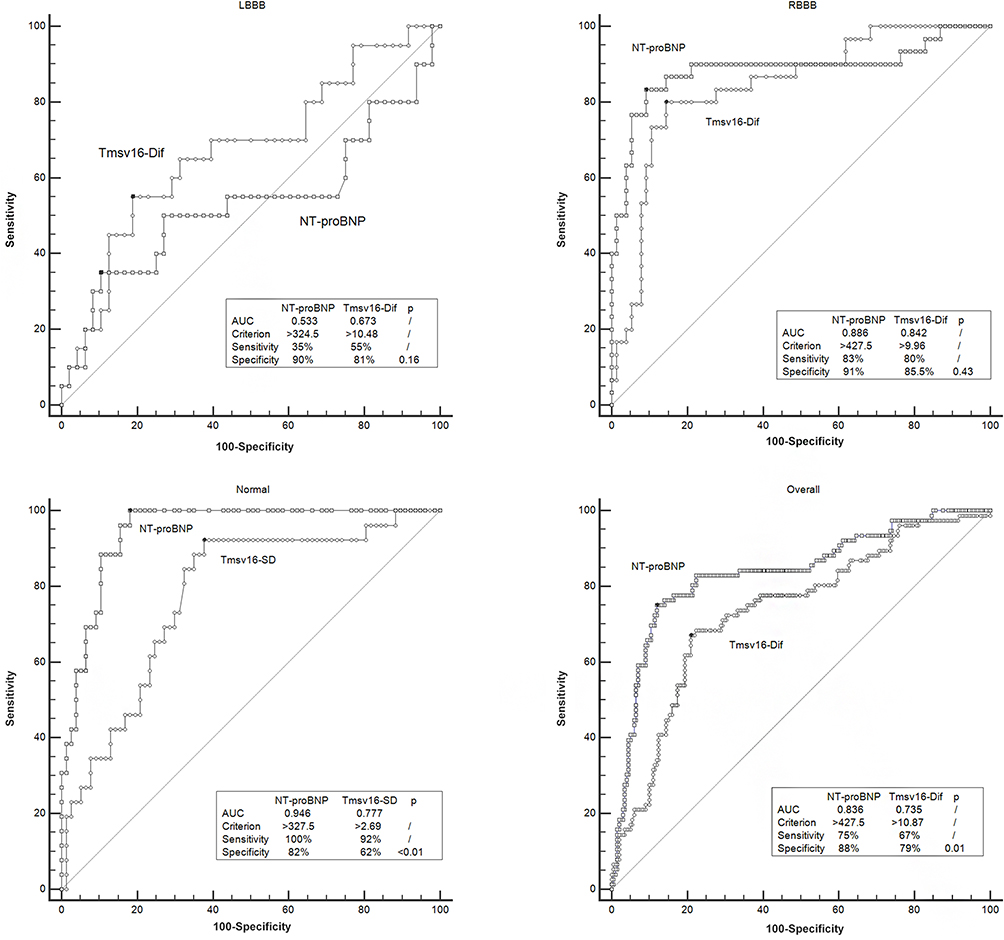 |
Figure 3 Comparison of ROC curve using the DeLong method between the LVSDI with the maximum AUC and NT-proBNP to differentiate patients with dilated cardiomyopathy (HF) in the three QRS subgroups and the overall participants. Abbreviations: LVSDI, left ventricular systolic dyssynchrony index; LBBB, left bundle branch block; RBBB, right bundle branch block; AUC, area under the curve; P, level of significance. |
The proportion of LVMD was 30.88%, 28.30%, and 25.24% in the LBBB, RBBB, and Normal groups, respectively, with no significant difference between groups. (Table 1) The prevalence of LVMD in participants with DCM was 33.33%, 57.33%, and 46.15% in the LBBB, RBBB, and Normal groups, respectively, with no statistically significant difference between groups. As displayed in Table 4, multivariable logistic binomial regression analysis shows: (1) LVMD is independently linked with HF in the overall study participants, RBBB, and Normal groups, while it is not independently linked in the LBBB group. (2) QRS duration has no correlation with HF in the overall patient population and each subgroup. (3) Diabetes is a strong risk factor for HF, regardless of QRS morphology and duration.
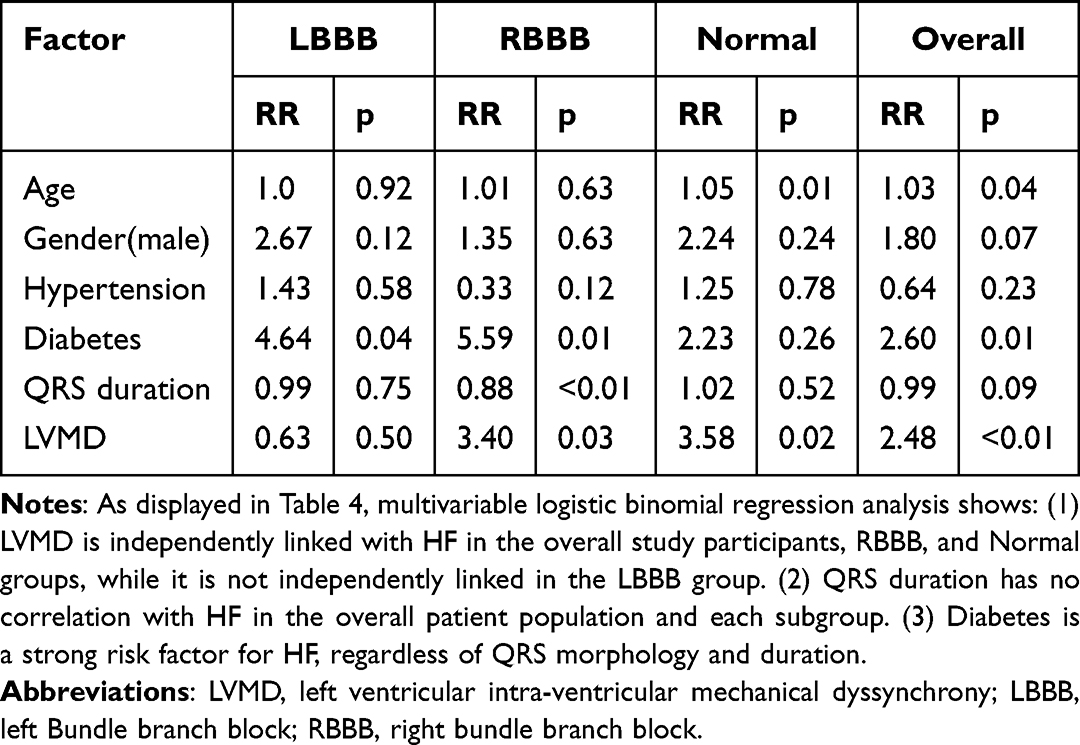 |
Table 4 Multivariable Logistic Binomial Regression of Factors Associated with Heart Failure (DCM) in Three QRS Subgroups and Overall Subjects. RR: Risk Ratio; P: Level of Significance |
Discussion
LV contraction occurs in a highly coordinated manner. Mechanical activation is triggered by the rapid propagation of electrical signals through a specialized conduction system. The systolic performance of left ventricle is affected not only by the state of myocardial contraction, but also by the synchrony of myocardium. LVMD refers to the mechanical effects of out-of-sync ventricular contraction and diastole, which may or may not be related to conduction disorders. Mechanical dyssynchrony has adverse effect on left ventricular systolic performance. Addressing LVMD with CRT has been shown to significantly reduce morbidity and mortality in patients with symptomatic systolic heart failure.
QRS widening, especially due to LBBB, indicates interventricular and intraventricular dyssynchrony in patients with heart failure and is being used as a selection criterion for CRT.12 However, even in implanted patients with a Class I recommendation, the nonresponse rate reaches up to 30–35%.13 In recent years, an increasing number of studies have found that diagnosing and treating cardiac mechanical dyssynchrony, especially LVMD, rather than the expanding QRS duration, is the key to benefiting from CRT.13–17 As a result, there is a gap between electrocardiographic dyssynchrony and mechanical dyssynchrony, and the latter appears to be more relevant in cardiac dysfunction and remodeling. LVMD can occur with normal QRS, however, patients with BBB do not always exhibit LVMD.18–20 Through RT-3DE, Bhambhani et al found that the frequency of LVMD was equivalent or even lower in patients with HF and LBBB compared to narrow QRS (47.8% vs 55.7%, P=NS),19 which is similar to our results (33.3% vs 46.5%, P = NS). The decreased frequency of LVMD in our DCM group is most likely attributable to the difference in etiology. The cases in the study by Bhambhani et al included a number of patients with ischemic cardiomyopathy (ICM) (46%),19 whose LVMD status was theoretically more severe due to scars. A recent study using SPECT to evaluate LVMD in patients with LBBB and RBBB found that the prevalence of LVMD is significantly higher in patients with LBBB (85%) than in patients with RBBB (40%) (P < 0.01),20 which is contradictory to our findings; a significant number of patients with ICM (more than 40%) were included in this study, which confirmed that LV scar was an independent factor in predicting LVMD; they concluded that LVMD was correlated with LVEF but not QRS duration, and that LVMD predicted CRT response better than QRS duration,20 which is in line with our findings.
In our study, we discovered that the correlation between LVMD and HF in the LBBB group was smaller than in the RBBB and Normal groups. We speculate that the interventricular dyssynchrony in the LBBB group was more severe, which led to heart dysfunction. LBBB was more receptive to CRT because it was frequently accompanied by a delay and diminishing of the entire LV, which contributed to low LVEF.12,21,22 LVMD is merely one of multiple independent targets of CRT,23 and conventional biventricular pacing may be harder to rectify than interventricular dyssynchrony. Although CRT has been shown repeatedly to make no difference or worsen outcomes in patients without LBBB,24–26 improved outcomes in these patients have been shown, particularly when LV lead placement is targeted intra-procedurally to areas of greatest electrical activation delay and mechanical dyssynchrony.27–29 Our result that LVMD has a larger impact on LV systolic dysfunction in the RBBB and Normal groups than in the LBBB group helps to explain this phenomenon. As seen in Figure 3, NT-proBNP has low diagnostic efficiency for LV systolic dysfunction in the LBBB participants. This may be partly due to the fact that heart failure with preserved ejection fraction (HFpEF) was not excluded in our non-HF group. NT-proBNP in our participants with normal LVEF was significantly higher in the LBBB group (median: 163.5, IQR: 113.6) than the RBBB group (median: 161.8, IQR: 76.2) and the Normal group (median: 82.0, IQR: 85.5) (P < 0.01). More research is required to determine whether LBBB or LVMD is a risk factor for HFpEF. According to a recent study, the prevalence of LVMD is similar in patients with LBBB with HFpEF (84.4%) and HFrEF (91.3%).30 Whether these patients can also benefit from CRT, is a topic worth researching further. Finally, it is unclear how differently the medication therapy impacts LVMD and LVEF. More patients in the LBBP group had been prescribed positive inotropic medications (digitalis), which may contribute to this disparity.
The spatial resolution of RT-3DE is low. In addition, relatively low volume rates (with a temporal resolution of about 40 to 50 ms) may not be sufficient to accurately assess left ventricular dyssynchrony. In addition, 3DE is limited by its inability to distinguish between active and passive movements. If it is not a single beat acquisition, it is also difficult to analyze arrhythmias. The 3DE SDI protocol has not been standardized. The SDI reference values of healthy subjects were significantly different among different software types.
There were some limitations in the present study. The sample size for this cross-sectional study is relatively modest and there was no control group and no follow up. We did not analyze the issue of interventricular dyssynchrony and its combined influence on heart failure. Atypical LBBB was neither excluded nor analyzed in the LBBB group. Subgroup analyses of those with concurrent left anterior fascicular block or left posterior branch block were not conducted in the RBBB group. Patients with intraventricular block were excluded. We will expand the sample size and set up a control group for long-term follow-up to provide insights into the progression of LVMD to evaluate its long-term impact on left ventricular cardiac function in the future.
Conclusion
LVMD, rather than QRS morphology or duration, is closely related to DCM and correlates with the degree of its LV systolic function decline, especially in patients without LBBB.
Funding
The study was supported by Nantong Municipal Science and Technology Plan (Guiding) Project (Nos. MSZ18199).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Marcassa C, Campini R, Verna E, Ceriani L, Giannuzzi P. Assessment of cardiac asynchrony by radionuclide phase analysis: correlation with ventricular function in patients with narrow or prolonged QRS interval. Eur J Heart Fail. 2007;9(5):484–490. doi:10.1016/j.ejheart.2007.01.002
2. Fauchier L, Marie O, Casset-Senon D, Babuty D, Cosnay P, Fauchier JP. Interventricular and intraventricular dyssynchrony in idiopathic dilated cardiomyopathy: a prognostic study with Fourier phase analysis of radionuclide angioscintigraphy. J Am Coll Cardiol. 2002;40(11):2022–2030. doi:10.1016/S0735-1097(02)02569-X
3. van Bommel RJ, Tanaka H, Delgado V, et al. Association of intraventricular mechanical dyssynchrony with response to cardiac resynchronization therapy in heart failure patients with a narrow QRS complex. Eur Heart J. 2010;31(24):3054–3062. doi:10.1093/eurheartj/ehq334
4. McAlister FA, Ezekowitz J, Hooton N, et al. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: a systematic review. JAMA. 2007;297(22):2502–2514. doi:10.1001/jama.297.22.2502
5. Mele D, Trevisan F, Fiorencis A, Smarrazzo V, Bertini M, Ferrari R. Current Role of Echocardiography in Cardiac Resynchronization Therapy: from Cardiac Mechanics to Flow Dynamics Analysis. Curr Heart Fail Rep. 2020;17(6):384–396. doi:10.1007/s11897-020-00484-w
6. Nitsche B, Eitel C, Bode K, et al. Left ventricular wall motion analysis to guide management of CRT non-responders. Europace. 2015;17(5):778–786. doi:10.1093/europace/euv034
7. Kapetanakis S, Kearney MT, Siva A, Gall N, Cooklin M, Monaghan MJ. Real-time three-dimensional echocardiography: a novel technique to quantify global left ventricular mechanical dyssynchrony. Circulation. 2005;112(7):992–1000. doi:10.1161/CIRCULATIONAHA.104.474445
8. Ma CY, Liu S, Zhang Q, et al. Calibration of the normal cutoff values of systolic dyssynchrony of the left ventricular synchronicity in normal subjects using real-time 3-dimensional echocardiography and the effects of age and heart rate. Cell Biochem Biophys. 2014;69(1):115–121. doi:10.1007/s12013-013-9777-3
9. Soliman OI, van Dalen BM, Nemes A, et al. Quantification of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography. J Am Soc Echocardiogr. 2009;22(3):232–239. doi:10.1016/j.echo.2008.11.009
10. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification. Eur J Echocardiogr. 2006;7(2):79–108. doi:10.1016/j.euje.2005.12.014
11. Soliman OI, Krenning BJ, Geleijnse ML, et al. A comparison between QLAB and TomTec full volume reconstruction for real time three-dimensional echocardiographic quantification of left ventricular volumes. Echocardiography. 2007;24(9):967–974. doi:10.1111/j.1540-8175.2007.00502.x
12. Stevenson WG, Hernandez AF, Carson PE, et al. Indications for cardiac resynchronization therapy: 2011 update from the Heart Failure Society of America Guideline Committee. J Card Fail. 2012;18(2):94–106. doi:10.1016/j.cardfail.2011.12.004
13. Beela AS, Unlu S, Duchenne J, et al. Assessment of mechanical dyssynchrony can improve the prognostic value of guideline-based patient selection for cardiac resynchronization therapy. Eur Heart J Cardiovasc Imaging. 2019;20(1):66–74. doi:10.1093/ehjci/jey029
14. Wang C, Shi J, Ge J, et al. Left ventricular systolic and diastolic dyssynchrony to improve cardiac resynchronization therapy response in heart failure patients with dilated cardiomyopathy. J Nucl Cardiol. 2020. doi:10.1007/s12350-020-02132-1
15. Stankovic I, Prinz C, Ciarka A, et al. Long-Term Outcome After CRT in the Presence of Mechanical Dyssynchrony Seen With Chronic RV Pacing or Intrinsic LBBB. JACC Cardiovasc Imaging. 2017;10(10 Pt A):1091. doi:10.1016/j.jcmg.2016.08.015
16. Bozyel S, Agacdiken Agir A, Sahin T, et al. Improvement in left ventricular intrinsic dyssynchrony with cardiac resynchronization therapy. Anatol J Cardiol. 2017;17(4):298–302. doi:10.14744/AnatolJCardiol.2017.7176
17. Moubarak G, Viart G, Anselme F. Acute correction of electromechanical dyssynchrony and response to cardiac resynchronization therapy. ESC Heart Fail. 2020;7(3):1302–1308. doi:10.1002/ehf2.12654
18. Ghio S, Constantin C, Klersy C, et al. Interventricular and intraventricular dyssynchrony are common in heart failure patients, regardless of QRS duration. Eur Heart J. 2004;25(7):571–578. doi:10.1016/j.ehj.2003.09.030
19. Bhambhani A, John N, Kumar B, Mathew A. Three-dimensional echocardiographic evaluation of mechanical dyssynchrony in systolic heart failure with narrow QRS complex. Indian Heart J. 2018;70(3):387–393. doi:10.1016/j.ihj.2017.10.013
20. Sillanmaki S, Gimelli A, Ahmad S, Samir S, Laitinen T, Soman P. Mechanisms of left ventricular dyssynchrony: a multinational SPECT study of patients with bundle branch block. J Nucl Cardiol. 2020. doi:10.1007/s12350-020-02054-y
21. Zhou W, Jiang Z, Chen J, Garcia EV, Li D. Development and validation of a phase analysis tool to measure interventricular mechanical dyssynchrony from gated SPECT MPI. J Nucl Cardiol. 2017;24(5):1680–1686. doi:10.1007/s12350-016-0503-6
22. Yilmaz S, Kilic H, Agac MT, et al. Left ventricular twist was decreased in isolated left bundle branch block with preserved ejection fraction. Anatol J Cardiol. 2017;17(6):475–480. doi:10.14744/AnatolJCardiol.2017.7346
23. Parsai C, Bijnens B, Sutherland GR, et al. Toward understanding response to cardiac resynchronization therapy: left ventricular dyssynchrony is only one of multiple mechanisms. Eur Heart J. 2009;30(8):940–949. doi:10.1093/eurheartj/ehn481
24. Adelstein EC, Saba S. Usefulness of baseline electrocardiographic QRS complex pattern to predict response to cardiac resynchronization. Am J Cardiol. 2009;103(2):238–242. doi:10.1016/j.amjcard.2008.08.069
25. Rickard J, Kumbhani DJ, Gorodeski EZ, et al. Cardiac resynchronization therapy in non-left bundle branch block morphologies. Pacing Clin Electrophysiol. 2010;33(5):590–595. doi:10.1111/j.1540-8159.2009.02649.x
26. Peterson PN, Greiner MA, Qualls LG, et al. QRS duration, bundle-branch block morphology, and outcomes among older patients with heart failure receiving cardiac resynchronization therapy. JAMA. 2013;310(6):617–626. doi:10.1001/jama.2013.8641
27. Baker MS, Gehi AK. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med. 2013;369(6):578.
28. Stockburger M, Moss AJ, Klein HU, et al. Sustained clinical benefit of cardiac resynchronization therapy in non-LBBB patients with prolonged PR-interval: MADIT-CRT long-term follow-up. Clin Res Cardiol. 2016;105(11):944–952. doi:10.1007/s00392-016-1003-z
29. Kandala J, Upadhyay GA, Altman RK, et al. QRS morphology, left ventricular lead location, and clinical outcome in patients receiving cardiac resynchronization therapy. Eur Heart J. 2013;34(29):2252–2262. doi:10.1093/eurheartj/eht123
30. Friedman DJ, Emerek K, Kisslo J, Sogaard P, Atwater BD. Left bundle-branch block is associated with asimilar dyssynchronous phenotype in heart failure patients with normal and reduced ejection fractions. Am Heart J. 2021;231:45–55. doi:10.1016/j.ahj.2020.10.053
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.