")
Back to Journals » Clinical Optometry » Volume 15
Potential Role of Biofeedback Visual Training in High-Speed Motorbike Drivers
Authors Vingolo EM , Chines C, Tanassi C , Charte A, Cecchinello L, Campigotto M
Received 23 May 2023
Accepted for publication 5 September 2023
Published 11 September 2023 Volume 2023:15 Pages 185—190
DOI https://doi.org/10.2147/OPTO.S418679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Enzo Maria Vingolo,1 Carmelo Chines,2 Cesare Tanassi,3 Angel Charte,4 Lucio Cecchinello,5 Mauro Campigotto3
1University Sapienza of Rome, Department of Ophthalmology Polo Pontino Ospedale A. Fiorini, Terracina, Italy; 2Ophthalmology, Oculista Italiano Journal, Catania, Italy; 3Nidek Inc, Fremont, CA, USA; 4Medicine, Universitat de Barcelona, Barcelona, Catalunya, Spain; 5LCR Honda Motor, Tokyo, Japan
Correspondence: Enzo Maria Vingolo, University “Sapienza” of Rome, Polo Pontino Italy, Department of Ophthalmology, Ospedale A. Fiorini, Terracina, 04120, Italy, Email [email protected]
Purpose: In several sports, appropriate training strategies remain a challenge for athletes and coaches, with the goal of improving performance. Extensive research has proposed several technical tools for obtaining parametric evaluations before competition in real life. This study aimed to assess whether some retinal performances might be improved using psychophysical techniques in health professionals involved in motorcycle sports (FIM MotoE).
Methods: Two MotoE drivers were screened at baseline using complete ophthalmological examinations and evaluation of retinal reaction times, followed by a biofeedback training program. After 4 months of training, the subjects underwent a control visit using the same protocol as the baseline.
Results: Central reaction time was shorter for 75% of drivers, with a consistent reduction (mean value of 20%). The peripheral reaction time showed an increasing trend after visual training. In both drivers, fixation stability improved dramatically (in 30% increments).
Conclusion: The potential role of advanced technology was applied to high-speed drivers. Our results may be due to an attentional shift from the peripheral retina to the central retina during training. In our opinion, training potentiates the most useful pathways at the expense of less involved retinal and cortical areas, thus improving driving abilities and safety.
Keywords: microperimetry, fixation, biofeedback, motorcycle, high-speed drivers
Purpose
Biofeedback and neuroenhancement strategies based on microperimetry have been well known since the early 2000 era, the main field of application of these techniques in patients with low vision. Several reports in the literature indicate that their application determines improvement in visual tasks and better quality-of-life. Furthermore, the application of these techniques in visual function recovery after main surgical interventions (retinal detachment, glaucoma surgery, and vitrectomy),1,2 in which biofeedback application determined faster visual recovery and better visual acuity after treatment.
Biofeedback in healthy subjects is generally considered pleonastic because there is usually no need to have better visual performance in real-life conditions. Considering high-speed motor drivers and their need for very fast reflexes and retina–brain connections, we thought that it would be interesting to understand the effect of biofeedback-driven neuroenhancement on these parameters.
Actual knowledge of visual psychophysical resources covers several sports,3 including handball, shooting, boxing, horse racing, etc., with the aim of speed recovery after injury or trauma involving the visual system or the eye directly. Several studies have reported that using biofeedback enables the recovery of visual acuity after retinal detachment or head injury. This study is the first to be applied to healthy subjects with the goal of improving standard performance to obtain the best competition results. We chose high-speed drivers because, in our opinion, their visual capabilities are usually used at the maximum of their power owing to the short time allowed in a race. In this view, increasing basal capabilities would make it possible to obtain better performance during a race.
Appropriate training burden monitoring is still a challenge for support staff, athletes, and coaches, with the final goal of improving performance and sports results. In recent years, extensive research has proposed several external and internal technical device indicators to obtain parametric evaluations before competition.3 The potential role of advanced technology in improving motion skills in sports and accelerating physical rehabilitation has been researched and demonstrated in several studies.4,5 We focused on more than 100 papers describing applications and systems that implement a complete real-time feedback loop, which must include the use of sensors, real-time processing, and concurrent feedback. Several studies have indicated cognitive factors to be a practical strategy. However, they have never been considered to improve sports performance during the training-monitoring process.
In our opinion, better knowledge of brain power capabilities may explore new methods for assessing cognitive demand in an applied setting to sports, in part through a very new neuro-ergonomic approach, which can be exploited and applied to our better understanding of fatigue, sports injury recovery, overtraining, and individual performance capabilities that critically improve sports results and increase athletes’ safety during races.
While the assessment of cognitive demand in sports is still in its infancy, it may represent a fruitful approach if applied with rigorous protocols and deep knowledge of the neurobehavioral and cognitive aspects of several eye diseases, as presented in many studies since the early 2000s.
In this pilot study, we assessed if the performance improvement acquired in retinal diseases via biofeedback and other psychophysical techniques may also be applied in healthy riders in professional motorsports (FIM MotoE World Cup). The total pool of drivers was 15, and study extension of the subjects in this study was limited by the copyright strategy of the team that did not want to lose any eventual performance gap over other racers or teams.
Materials and Methods
Two MotoE Championship drivers were analyzed with full ophthalmological screening at baseline, while all other pilots overcome a basic clinical examination to obtain driver license for Moto GP World Championship and were considered at the same level as healthy people on the grid. The scheduled protocol was evaluation of Best Corrected Visual Acuity (BCVA) with LACE computerized presentation system, EDTRS Chart with random letter presentation, Humphrey automated Visual field test with computerized full threshold strategy (central 30°+ peripheral 60°), aberrometry with Topcon aberrometer, OCT scans and fundus photography with Nidek “Mirante” system, Nidek MP3 microperimetry, threshold strategy, fixation evaluation, reaction time analysis for peripheral (40 stimuli) and central areas (12 stimuli) reaction time was automatically measured by a built in Microperimeter software, considering the time lapse from stimulus presentation and subject reaction done with the pressure on a button, this reaction time was measured in 40 different locations in the peripheral region (outer 20° from fixation point) and 12 different points inside the 20° region (central) all locations were standardized in each examination, reaction time value, for each point was repeated three times and the actual value was determined as the mean value of these measurements. Clinical examination also included anterior chamber slit-lamp analysis and fundus stereo biomicroscopy by 90D lens. Both subjects had logMAR values > 0 in the OU the protocol and the study comply with the Declaration of Helsinki. After the baseline, both drivers followed a customized training program based on a specially developed computerized device using biofeedback stimulation of a randomly presented patterned checkboard (10°C for the central area and 0.5°C for the peripheral area) at least three times a week for 10 min for each eye. After 4 months of training, the subjects underwent a control visit using the same protocol as the baseline.
Statistical evaluation was performed using Microsoft Excel (Microsoft, Redmond, WA, USA) with the Student’s paired t-test.
Results
- Central reaction time (Figure 1) was shorter for both drivers in three of the four eyes with a very important reduction (mean reduction was 20%), mean value for baseline central reaction time was of 448.75 ± 31.34 ms; after the training registered values were for reaction time 409.75 ± 18.48 ms with a statistically significant reduction in the central reaction time (P=0.0031).
- The peripheral reaction time (Figure 2) showed after visual training showed an increase in the elapsed time from the stimulus, and the mean value for baseline central reaction time was of 447.25 ± 53.01 ms. At the end of training, the peripheral reaction time was 469.75 ± 59.86 ms with significant power (P=0.004).
- In both drivers, fixation stability (Figure 3) was dramatically improved (with 30% and more increments), in fact the mean value for baseline fixation, evaluated as Behavior Central Ellipse Area (BCEA), was 5.34 ± 4.27 square degrees at baseline, while at the end of the training it was 3.51 ± 2.96 square degrees. This consistent reduction in fixation values means that fixation points were concentrated in a smaller area, indicating a better concentration on visual saccadic tasks (P=0.0008). This suggests that their driving ability might be more rapid, safe, and fast because their attention was pointed towards the racetrack, evaluating with more accuracy and rapidity distances, curves, and obstacles provided by the track or other riders.
 |
Figure 1 Central reaction time after the training. |
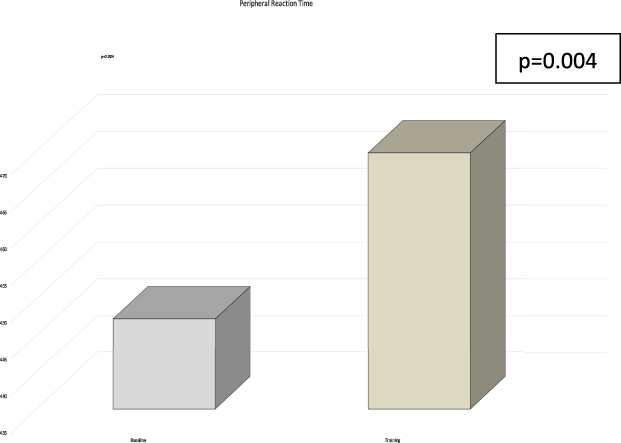 |
Figure 2 Peripheral reaction time after the training. |
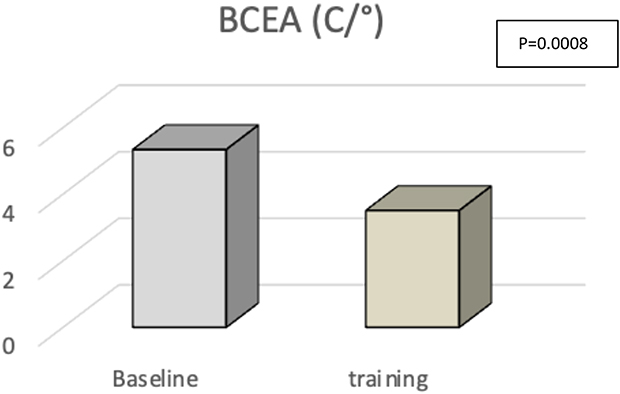 |
Figure 3 Behaviour contour ellipse area (BCEA) after the training. |
Discussion
In the studies that we have focused on, more than 100 papers have described applications and systems that implement a complete real-time feedback loop,1 which usually includes the use of sensors, real-time processing, and concurrent feedback. In our opinion, this increase in peripheral reaction time may be due to an attention shift during training from the peripheral retina (less involved in the high-speed drive) to the central retina, which is highly significant for receptive fields in the central retina and primary visual cortex. In our opinion, the training potentiates the most useful pathways at the expense of less involved retinal and cortical areas (usually driving at high speed; there is a visual field constriction directly correlated to the speed), which is due to the slower frequency response of rods and peripheral low spatial frequency receptive fields driven by the magnocellular system.
The origin and implications of fatigue in exercise have been widely investigated but are not completely understood, given the complex multifactorial mechanisms involved.6 Understanding the fatigue mechanism in motorsports is essential to help trainers and physicians prescribe adequate training loads. As in the retina, central and peripheral fatigue are two unison constructs of Integrative Governor Theory, in which homeostatic principles underpin psychological and physiological drives and requirements.7 The relative activity of each is regulated by dynamic negative feedback and acts as a fundamental general operational controller.
Fatigue is conditioned by factors such as sex, which affects men and women differently. Each intervention can improve sports performance. Also, in Motorsports, fatigue is a complex mechanism, and it is not only muscular but also visual and mental, and in this view, our results, even limited to a very small sample, seem to suggest that improving the visual capability of the athlete may have a positive influence on their performance.
Moreover, we cannot exclude the safety aspects of this increase in performance in the central area of vision because a faster answer time means faster reflexes and counteraction that at high speed may also benefit thousands of seconds, which could mean the difference between a victory and an accident.8
As our study indicated, real-time Biomechanical Feedback has great potential in many areas. In recent years, sensors have been the focus of such research. New types of processing devices, methods, algorithms, actuators, communication technologies, and protocols will be explored in greater depth in the future. We think of the possibility of using wearable devices such as virtual reality helmets for simultaneous simulation of race and pattern stimulation to improve reflexes and fixation offline from the race; thus, during real-life performances, drivers would be better trained to run. Our pilot study was limited to only two pilots of a single team, and for security reasons, until these data became public, the owner of the racing team did not allow us to include more pilots from other teams. As the study will be published, the Motor Sports Agency (DORNA) will be involved in our program with other drivers. We can confirm our data on a higher cluster of subjects, and we can schedule different approaches to stimulation trials by changing the spatial frequency of the stimuli or their position in the visual field.8
Further steps of this preliminary study, in our view, may be as follows:
- Try to improve consistency in visual training exercises (daily or at least twice-a-week sessions) during the interval between the two races.
- Evaluate reaction time and fixation stability before or during the race weekends.
- To compare visual function post-training results with driving performances either in trials or in the race, use a speed/fixation stability evaluation, lap time/fixation stability, or reaction time (either peripheral or central) during race weekends.
- Increase the number of drivers involved in the training. This will allow us to try new biofeedback strategies and parameters and to tabulate the results to obtain better performances.
In our opinion, this report opens a new field in training resources, considering the application not in patients with damaged visual systems but in healthy subjects. The results of increasing the normal capabilities to a higher level of performance and results, even in a very low number of studied drivers (only two on a platform of 15 drivers) are very promising.
This study opens the research of new tasks to obtain better performance in sports in which visual system efficiency is crucial, not with drugs or artificial tools, but only exploiting the neuroenhancement capabilities of the retina and brain of healthy subjects. The results are promising, and we need to apply them to a wider number of drivers and sports, nevertheless main brand resistances, and to different sports to compare results.
Conclusions
The potential role of advanced technology is to improve motion skills in sports for training or speed post-injury rehabilitation for several medical tasks but not for high-speed drivers. We have focused on many studies with applications or systems that implement a complete real-time feedback loop using sensors, real-time processing, and concurrent feedback. From our data, training potentiates the most useful pathways at the expense of less involved retinal and cortical areas with a positive influence on race results and with safety implications on rapidity in rescue maneuvers and to avoid crashes during the race. In our opinion, training potentiates the most useful neural pathways with its neuroenhancement activity in high spatial frequency receptive areas included in the parvocellular system (sharp vision and central areas) at the expense of less involved retinal and cortical areas, mainly driven by low spatial frequency receptive fields mainly expressed in the magnocellular system (motion detection and peripheral visual field). Visual biofeedback training is a new and still unexplored field of research because it has proven effective in the case of eye diseases. However, its potentiality in subjects with normal vision remains unknown. Our study opens a new window into how it is possible to improve visual performance in athletes from different disciplines. We chose a preliminary study on motor drivers whose visual performance greatly affects the race results and drivers’ safety. Our data may modify training programs in this discipline, and positive results may be applied to sports such as basketball, soccer, and football.
Patient Involvement
Participants were involved in the conceptualization phase, informing them of all measures that were taken and which aims were directed. Both drivers provided written informed consent to participate in this study.
Data Sharing Statement
Raw data were generated at the Nidek Technologies Center, Padua, Italy. The derived data supporting the findings of this study are available from the corresponding author, EMV, upon request.
Ethical Approval Information
University Sapienza of Rome Department of Sense Organs session of February 7, 2021, approval n° 7/21.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
C.T. and M.C. are employees of Nidek Technologies Inc., and C.C. is a consultant of the SIFI group. The authors report no other conflicts of interest in this work.
References
1. Vingolo EM, Napolitano G, Fragiotta S. Microperimetric biofeedback training: fundamentals, strategies and perspectives. Front Biosci. 2018;10(1):48–64. doi:10.2741/s500
2. Vingolo EM, Cavarretta S, Domanico D, Parisi F, Malagola R. Microperimetric biofeedback in AMD patients. Appl Psychophysiol Biofeedback. 2007;32(3–4):185–189. doi:10.1007/s10484-007-9038-6
3. Shei RJ, Holder IG, Oumsang AS, Paris BA, Paris HL. Paris: wearable activity trackers–advanced technology or advanced marketing? Eur J Appl Physiol. 2022;21:1–16. doi:10.1007/s00421-022-04951-1
4. Hribernik M, Umek A, Tomažič S, Kos A. Review of real-time biomechanical feedback systems in sport and rehabilitation. Sensors. 2022;22(8):3006. doi:10.3390/s22083006
5. Perrey S. Training monitoring in sports: it is time to embrace cognitive demand. Sports. 2022;10(4):56. doi:10.3390/sports10040056
6. Mueller S, Mueller J, Stoll J, Mayer F. Effect of six-week resistance and sensorimotor training on trunk strength and stability in elite adolescent athletes: a randomized controlled pilot trial. Front Physiol. 2022;13:802315. doi:10.3389/fphys.2022.802315
7. Tornero-Aguilera JF, Jimenez-Morcillo J, Rubio-Zarapuz A, Clemente-Suárez VJ. Central and peripheral fatigue in physical exercise explained: a narrative review. Int J Environ Res Public Health. 2022;19(7):3909. doi:10.3390/ijerph19073909
8. Verboschi F, Domanico D, Nebbioso M, Corradetti G, Scalinci SZ, Vingolo EM. New trends in visual rehabilitation with MP-1 microperimeter biofeedback: optic neural dysfunction. Funct Neurol. 2013;28(4):285.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.