")
Back to Journals » Clinical Ophthalmology » Volume 15
Population-Based Incidence of Ocular Neovascularization Following Central Retinal Artery Occlusion in Olmsted County, Minnesota
Authors Tanke LB, Chodnicki KD, Olsen TW, Bhatti MT, Chen JJ
Received 3 July 2021
Accepted for publication 12 August 2021
Published 21 August 2021 Volume 2021:15 Pages 3531—3537
DOI https://doi.org/10.2147/OPTH.S327704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Laurel B Tanke,1 Kevin D Chodnicki,1 Timothy W Olsen,1 M Tariq Bhatti,1,2 John J Chen1,2
1Department of Ophthalmology, Mayo Clinic, Rochester, MN, USA; 2Department of Neurology, Mayo Clinic, Rochester, MN, USA
Correspondence: John J Chen
Department of Ophthalmology, Mayo Clinic, Rochester, MN, USA
Email [email protected]
Purpose: To determine the population-based incidence of ocular neovascularization (NV) following central retinal artery occlusion (CRAO) and systemic risk factors associated with its development.
Methods: Diagnosis of CRAO between January 1, 1976, and September 9, 2016, was identified using the Rochester Epidemiology Project, a medical records linkage system for all medical care provided to residents of Olmsted County, Minnesota. Records were reviewed to confirm the diagnosis of CRAO, and data were collected on ocular NV and associated systemic diseases.
Results: There were 89 patients with CRAO. Subsequent ocular neovascularization developed in 14 (16%) patients. Neovascularization of the iris (NVI) was present in 9/14 (64%) of these patients, neovascularization of the angle (NVA) in 10/14 (71%), neovascularization of the disc (NVD) in 2/14 (14%), and neovascularization elsewhere (NVE) in 1/14 (7%). Of these 14 patients with NV, 9 (64%) developed neovascular glaucoma (NVG). The mean time from CRAO diagnosis to NV was 82 days (range 22 to 268 days). Excluding the patients with proliferative diabetic retinopathy or CRAO caused by CRVO, the mean time to NV diagnosis was 80 days and the shortest time to NV diagnosis was 22 days. Diabetes mellitus was present in 64% of those with NV compared to 23% of those without NV (P = 0.003).
Conclusion: The population-based incidence of ocular neovascularization following CRAO is 16% and developed within 2 months in half the cohort. Patients with diabetes mellitus are at increased risk for NV complications.
Keywords: central retinal artery occlusion, neovascular glaucoma
Central retinal artery occlusion (CRAO) is an ophthalmic emergency, analogous to a cerebrovascular accident (CVA) of the central retinal artery.1 This condition is characterized by a macular cherry red spot and surrounding inner retinal opacity, due to retinal ischemia. A CRAO is most commonly caused by an embolus originating from the internal carotid artery, often secondary to atherosclerosis.1 The annual incidence of CRAO is estimated to be about 1.9 in 100,000 people.2 A CRAO is associated with a poor visual outcome and may result in ocular neovascularization (NV) and neovascular glaucoma (NVG). Screening for NV after a CRAO is important because NV is associated with ocular complications and reduced visual acuity, and NVG is painful and often necessitates surgical intervention.3 If ocular NV is detected early and managed with treatments such as panretinal photocoagulation (PRP) or intravitreal anti-vascular endothelial growth factor (VEGF) injections, ocular morbidity is reduced.4
The reported incidence of ocular neovascularization following a CRAO is variable. Previous estimates of incidence have ranged from 3.0% to 31.6%, and previous studies have found associations between ocular NV development and various systemic conditions, including diabetes mellitus and atherosclerosis.3,5–7 Most prior studies utilize institution-based data derived from large tertiary care centers and may contain inherent bias toward more severe disease. In this study, a population-based cohort of patients diagnosed with a CRAO was evaluated using the Rochester Epidemiology Project (REP) to determine the incidence of ocular NV and associated systemic diseases with reduced bias.
Methods
Medical records of patients with a diagnosis of CRAO from January 1, 1976, to September 9, 2016, in Olmsted County, Minnesota, were identified using the REP.2 The REP is a multicenter medical records linkage system that allows for population-based studies of disease in residents of Olmsted County in Southeastern Minnesota. It indexes all diagnostic and procedure information from Mayo Clinic in Rochester, Minnesota, and other facilities that provide health care to residents in this community.8 Patient charts were identified using Hospital International Classification of Disease Adaptation, International Classification of Diseases (ICD)-9, and ICD-10 codes for central and branch retinal artery occlusions.
A retrospective chart review was performed on the electronic and paper medical records to confirm the diagnosis of CRAO. Diagnosis was confirmed based on clinical history, ophthalmic exam, and ancillary testing, including fluorescein angiography (FA) and optical coherence tomography (OCT), if it was available. In cases in which the diagnosis of CRAO was in question, a staff neuro-ophthalmologist reviewed the data to make the final determination. Patients were excluded if they were younger than 18 years when diagnosed, the original diagnosis was made outside of the study window, or the CRAO diagnosis was not correct. Data were collected on demographics, including age, sex, and race; comorbidities diagnosed before or during the workup of the CRAO, including active or former smoking status, diabetes mellitus, hypertension, hyperlipidemia, coronary artery disease, glaucoma, history of CVA, and carotid imaging, and the etiology of the CRAO. Ipsilateral carotid artery stenosis was assessed with a combination of carotid ultrasound, CTA, MRA, and cerebral angiogram.
Charts were reviewed for any ocular neovascularization, neovascularization of the disc (NVD), neovascularization of the iris (NVI), neovascularization of the angle (NVA), neovascularization elsewhere (NVE), and neovascular glaucoma (NVG). NVG was defined as NVI or NVA with intraocular pressure (IOP) >21 mmHg in patients without a prior history of glaucoma or ocular hypertension.6,7 In patients with a prior history of glaucoma or ocular hypertension, NVG was defined as NVI or NVA with a greater than 25% increase in IOP compared to the IOP measured at CRAO diagnosis. Alternative causes of elevated IOP were excluded. Other variables collected included time from CRAO to neovascularization, visual acuity at the time of NV, and treatment at the time of NV diagnosis. For patients with NVG, visual acuity at the time of NVG diagnosis, IOP at the time of CRAO, peak IOP at any point at or after the NVG diagnosis, final IOP, and NVG treatment were recorded.
This study was approved by the Institutional Review Boards of Mayo Clinic and Olmsted Medical Center in Rochester, Minnesota. It conforms to the requirements of the United States Health Insurance Portability and Accountability Act (HIPAA) and adheres to the tenets of the Declaration of Helsinki.
Results
Between 1976 and 2016, out of 965 unique patient charts reviewed using the ICD-9 and ICD-10 codes for CRAO and BRAO, 89 patients were confirmed to have a new CRAO during the study period and were residents of Olmsted County, MN. The median age was 76 (range 46 to 100 years), and 56% were male. The age- and sex-adjusted incidence of CRAO for the cohort was 2.58/100,000 (95% CI 2.04–3.11). Among the 89 patients with CRAO, 14 (16%) subsequently developed ocular NV. The general characteristics of the whole cohort are summarized in Table 1. The groups were similar between those with and without NV, except diabetes mellitus was present in 64% of those with NV compared to 23% of those without NV (P = 0.003). Among 26 patients with CRAO and diabetes, 9 (34.6%) developed NV compared to the 5 (8.0%) of those with CRAO without diabetes (p = 0.002). The etiology of the CRAO was similar between the groups, but in 3 of the patients who developed NV, central retinal vein occlusion (CRVO) was the cause of the CRAO. With the patients with coinciding CRVO excluded, 11 (13%) of the 89 total patients developed NV directly as a result of CRAO. Of the 9 patients who developed NV and had diabetes, 4 had no history of diabetic retinopathy, 3 had non-proliferative diabetic retinopathy in the ipsilateral eye, and 2 had long-standing proliferative diabetic retinopathy in the ipsilateral eye at the time of the CRAO. Only one of the patients with diabetes developed NV in the contralateral eye, but it was 3 years after the CRAO, compared to 3 months after the CRAO in the ipsilateral eye. Patients who did not develop NV had a median ophthalmology follow-up of 3.9 years (range 0 to 17.8 years), which was similar to those that developed NV (median 3.6 years; range 0.3 to 17.0 years).
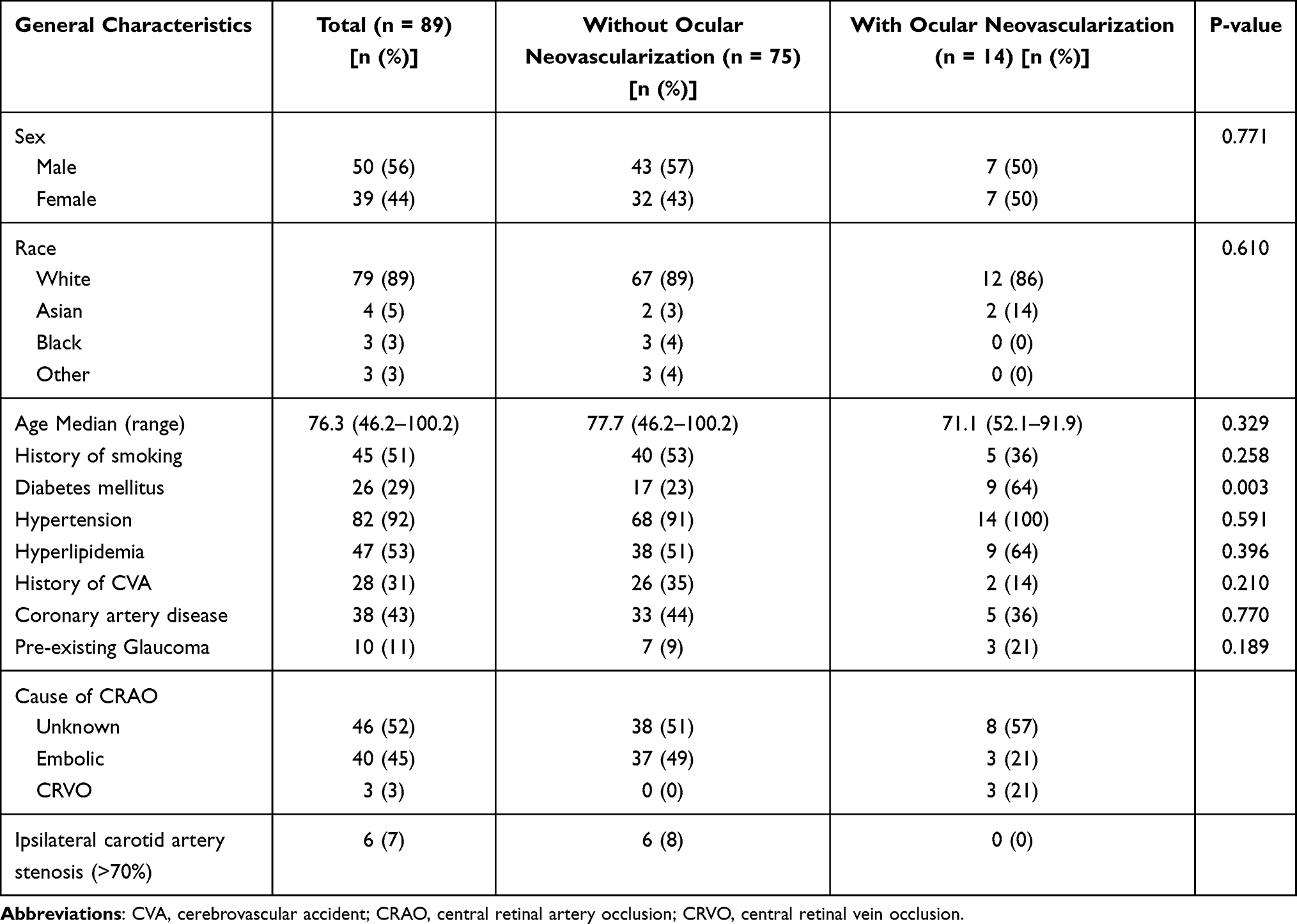 |
Table 1 General Characteristics of Patients With and Without Ocular Neovascularization After Central Retinal Artery Occlusion |
Features of the 14 patients that developed ocular NV are summarized in Table 2. NVI was present in 9 (64%) of these patients, NVA in 10 (71%), NVD in 2 (14%), and NVE in 1 (7%). The mean time from CRAO diagnosis to NV was 82 days (range 22 to 268 days). The mean time from CRAO diagnosis to NVG was 221 days (range 22 to 1380 days), and the mean time from NV to NVG was 154 days (range 0 to 1358 days). No patients with ocular NV had significant (>70%) ipsilateral carotid artery stenosis. Excluding the patients with proliferative diabetic retinopathy or CRAO caused by CRVO, the mean time to NV diagnosis was 80 days, and the earliest time to NV diagnosis was 22 days.
 |
Table 2 Features of Patients That Developed Ocular Neovascularization After Central Retinal Artery Occlusion |
Of the 14 patients with NV, 9 (64%) developed NVG. The mean change in IOP from baseline, at time of CRAO diagnosis, to the time of NVG diagnosis was 30.3 mmHg. Of the 5 patients that did not develop NVG, one patient was observed, two patients were treated with intravitreal anti-VEGF injections and PRP, one patient was treated with PRP alone, and one patient was treated with anti-VEGF injections alone. Of the patients who developed NVG, seven were diagnosed with NVI and/or NVA on the same day as their NVG diagnosis, one developed NVG one month after NV diagnosis despite treatment with PRP and Avastin at the initial NV diagnosis, and one developed NVG four years after the diagnosis of NVI despite PRP treatment at the initial NVI diagnosis. Management after diagnosis of NVG is summarized in Table 3. All of the patients received topical IOP lowering medications, three (33%) received oral acetazolamide, four (44%) had PRP, one (11%) received intravitreal anti-VEGF injections, and three (33%) received surgical treatment with anterior chamber paracentesis, cryoablation, Ahmed tube placement, or cyclophotocoagulation.
 |
Table 3 Features of Patients That Developed Neovascular Glaucoma After Central Retinal Artery Occlusion |
Discussion
Our population-based study revealed a 16% ocular NV incidence following CRAO. NVG subsequently developed in 64% of the patients with NV or 10% of the total CRAO cohort. Only two patients went on to develop NVG despite being treated with PRP at the initial diagnosis of NV. The mean time from CRAO to NV diagnosis was 82 days. The results of this study support the practice of early detection and treatment of NV following CRAO. We believe that patients should be carefully monitored monthly for at least 9 months after CRAO diagnosis for the development of NV. Some patients may not need as stringent of monitoring (for example, those that have shown reperfusion on angiography), but more research is needed.
The 16% incidence of NV following CRAO aligns with estimates from prior non-population-based studies (3.0 to 31.6%).3,5–7 The only prospective case series evaluating NV after CRAO performed by Duker et al also found a very similar incidence of 16.6%.3,5–7 Our study is the first population-based study to estimate the incidence of NV after CRAO. It is important to note that our study does not include all patients seen at the Mayo Clinic but rather only the patients residing in Olmsted County using the Rochester Epidemiology Project in order to provide the population-based frequency of NV after CRAO. If all patients seen at the Mayo Clinic with CRAO during this time period were included, the numbers would be larger but would have the caveat of potential referral bias. More severe cases could be referred, potentially with a higher degree of NV or other complications from the CRAO. Therefore, we believe that our estimate of NV after CRAO is accurate for the general population.
In three of the patients who developed NV after CRAO, their CRAO was caused by a CRVO. CRVO is a well-established driver of NV.9 Therefore, in these patients, the CRVO likely drove the development of the NV. Excluding these patients leaves 11 (13%) of the 89 patients with NV caused by CRAO alone. Prior studies on CRAO secondary to CRVO have reported that the incidence of neovascularization ranges widely, from 0 to 81%.10,11 In our study, all three (100%) of the patients with CRAO caused by CRVO developed NVA and NVG.
The 82-day mean time from CRAO to NV diagnosis is also very similar to prior studies, reporting an average interval between one and three months.3,5–7 With a shortest time from CRAO to NV of 22 days, our study also supports the notion that NV can occur very early after presentation with CRAO. Four of the 14 (28%) patients who developed NV in our study developed it after four months, although two were very close, at 122 and 124 days. Other studies have found shorter times from CRAO to NV than our shortest time of 22 days, even as early as the same day as CRAO presentation.7,9 Duker et al found the shortest time from CRAO to NV of 12 days, and Jung et al found the shortest time of 1 week.5,6 Our longest time of 268 days falls within the range of previously reported longest intervals, which have varied widely across studies. Mason et al reported the longest time of 137 days, while Duker et al reported the longest time of 15 weeks, and Jung et al reported the longest time of 15 months.5–7
We found that diabetes mellitus is a significant risk factor for NV development following CRAO. Diabetes mellitus was present in 64% of patients who developed NV, but only 23% of those who did not develop NV. The association between diabetes mellitus and the development of NV was also reported by Mason et al, who found an odds ratio of 5.2 for type 2 diabetes mellitus.7 In general, systemic hyperglycemia in diabetes is associated with microvascular changes with impaired blood vessel function and increased angiogenesis.12 Molecules, like VEGF and hypoxia-inducible factor (HIF), are also responsible for retinal neovascularization and retinal vascular leakage-associated complications of diabetes.12 Similar vascular injury may also likely contribute to the increased risk of neovascularization in diabetic patients after CRAO. Of the 9 patients that developed NV and had diabetes, only one developed NV in the eye contralateral to the CRAO, and it developed 3 years after the CRAO compared to 3 months after the CRAO in the ipsilateral eye. This suggests that diabetes and diabetic retinopathy are predisposing factors, but not causative of the NV in these patients.
There is controversy in the literature about a possible cause and effect relationship between CRAO and neovascularization. Hayreh et al assert that the primary etiology for the production of neovascularization with CRAO is anterior segment ischemia from carotid or ophthalmic artery insufficiency and that the development of CRAO and NVG is often both secondary to ocular ischemia as a result of a simultaneous fall of blood pressure within the central retinal artery combined with a rise of IOP.13 Our study does not support either of these explanations for the development of NV in the majority of CRAO. None of the patients in our study who developed NV had significant carotid artery stenosis, and NV was not present in any of the patients at the time of CRAO diagnosis. This temporal relationship suggests that the retinal ischemia following the CRAO likely induces secondary NV in the vast majority of CRAO, and this theory aligns with the findings of Rudkin et al.3
The study limitations include the retrospective nature with less consistent follow-up. Due to the lack of standardized follow-up exams, gonioscopy may not have been performed consistently on each patient, which may have affected the timing of detection of neovascularization. Also, 90% of the population included in this study is white, so the generalizability to other demographics is unclear. Two patients in our study had no follow-up after their CRAO diagnosis, and some had limited follow-up after their diagnosis. While most with NVG would have pain that would prompt a return visit, ocular NV without NVG is painless and could potentially go undiscovered. Also, not all of the patients underwent FA, and although the diagnosis of CRAO was confirmed by chart review, it is possible that a small number of patients suffered an ophthalmic artery occlusion. Also, this study period extends back to 1976, so there is the possibility that some of the CRAOs in the early portion of the study may have had an etiology that was not identified because of limitations in testing at that time. Finally, this study includes patients before the anti-VEGF era, so the proportions of how patients who developed NV were treated are likely skewed towards PRP.
In conclusion, the population-based incidence of ocular neovascularization after CRAO in Olmsted County, Minnesota, is 16%. Due to the ocular morbidity of NVG, we stress the importance of monthly follow-up examinations for these patients with undilated gonioscopy beginning after their CRAO diagnosis. Our data suggest that close monitoring up to 9 months after CRAO may be warranted. Patients with diabetes mellitus should be educated that they are at higher risk for ocular NV complications. Future studies may help determine factors that may reduce the NV risks, such as the degree of ocular reperfusion.
Funding
There is no funding to report.
Disclosure
Dr Timothy W Olsen reports personal fees from American Academy of Ophthalmology; Secretary for Quality of Care, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Varma DD, Cugati S, Lee AW, Chen CS. A review of central retinal artery occlusion: clinical presentation and management. Eye. 2013;27(6):688–697. doi:10.1038/eye.2013.25
2. Leavitt JA, Larson TA, Hodge DO, Gullerud RE. The incidence of central retinal artery occlusion in Olmsted County, Minnesota. Am J Ophthalmol. 2011;152(5):820–3.e2. doi:10.1016/j.ajo.2011.05.005
3. Rudkin AK, Lee AW, Chen CS. Ocular neovascularization following central retinal artery occlusion: prevalence and timing of onset. Eur J Ophthalmol. 2010;20(6):1042–1046. doi:10.1177/112067211002000603
4. Dorrell M, Uusitalo-Jarvinen H, Aguilar E, Friedlander M. Ocular neovascularization: basic mechanisms and therapeutic advances. Surv Ophthalmol. 2007;52(Suppl 1):S3–S19. doi:10.1016/j.survophthal.2006.10.017
5. Duker JS, Sivalingam A, Brown GC, Reber R. A prospective study of acute central retinal artery obstruction. The incidence of secondary ocular neovascularization. Arch Ophthalmol. 1991;109(3):339–342. doi:10.1001/archopht.1991.01080030041034
6. Jung YH, Ahn SJ, Hong JH, et al. Incidence and clinical features of neovascularization of the iris following acute central retinal artery occlusion. Korean J Ophthalmol. 2016;30(5):352–359. doi:10.3341/kjo.2016.30.5.352
7. Mason JO, Patel SA, Feist RM, et al. Ocular neovascularization in eyes with a central retinal artery occlusion or a branch retinal artery occlusion. Clin Ophthalmol. 2015;9:995–1000. doi:10.2147/OPTH.S82796
8. Melton LJ. History of the Rochester epidemiology project. Mayo Clin Proc. 1996;71(3):266–274. doi:10.4065/71.3.266
9. Hayreh SS, Rojas P, Podhajsky P, et al. Ocular neovascularization with retinal vascular occlusion-III. Incidence of ocular neovascularization with retinal vein occlusion. Ophthalmology. 1983;90(5):488–506. doi:10.1016/S0161-6420(83)34542-5
10. Wang H, Chang Y, Zhang F, et al. Clinical features of combined central retinal artery and vein occlusion. J Ophthalmol. 2019;2019:7202731. doi:10.1155/2019/7202731
11. Brown GC, Duker JS, Lehman R, Eagle RC. Combined central retinal artery-central vein obstruction. Int Ophthalmol. 1993;17(1):9–17. doi:10.1007/BF00918861
12. Costa PZ, Soares R. Neovascularization in diabetes and its complications. Unraveling the angiogenic paradox. Life Sci. 2013;92(22):1037–1045. doi:10.1016/j.lfs.2013.04.001
13. Hayreh SS. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog Retin Eye Res. 2005;24(4):493–519. doi:10.1016/j.preteyeres.2004.12.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.