")
Back to Journals » International Medical Case Reports Journal » Volume 17
Pollicization of index Fingers For Bilateral Hypoplastic Thumbs of Twin Babies: Case Series At Cure Children’s Hospital of Ethiopia
Authors Mohammed T, Jimma TM, Zerfu TT, Kassaahun ME
Received 24 December 2023
Accepted for publication 4 April 2024
Published 11 April 2024 Volume 2024:17 Pages 327—333
DOI https://doi.org/10.2147/IMCRJ.S454360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Tuji Mohammed,1 Tesfaye Mulat Jimma,2 Tewodros Tilahun Zerfu,3 Mesfin Etsub Kassaahun3
1Department of Orthopaedic and Traumatology Surgery at St. Paul Millennium Medical College, AaBET Hospital, Addis Abeba, Ethiopia; 2Department of Plastic and Reconstructive Surgery, College of Surgeons of East Central and South Africa, Cure Hospital, Addis Abeba, Ethiopia; 3Department of Pediatric Orthopaedic Surgery, College of Surgeons of East Central and South Africa, Cure Hospital, Addis Abeba, Ethiopia
Correspondence: Tuji Mohammed, Orthopaedic and Traumatology Surgeon, Department of Orthopaedic and Traumatology Surgery at St. Paul Millennium Medical College, AaBET Hospital, Addis Abeba, Ethiopia, Tel +251937525119, Email [email protected]
Introduction: Thumb hypoplasia is a congenital birth defect in which a child is born with an underdeveloped or missing thumb. It is a rare condition affecting approximately 1 in 100,000 live births and occurs equally in both males and females. Pollicization is a surgical procedure used to treat severe thumb hypoplasia by transferring another finger to the thumb position.
Case Presentation: Twin girls aged two years and eight months, born to a 42-year-old para III mother, presented with bilateral thumb hypoplasia. There was no family history of similar complaints, and no consanguinity was identified between their parents. After excluding other associated anomalies, index finger pollicization was performed for all four hands of the children according to modified Buck-Gramcko techniques, with modifications from Ezaki et al.
Conclusion: Generally, index pollicization executed with careful preoperative, intraoperative, and postoperative planning will lead to aesthetically and functionally attractive thumbs for children with congenitally severe hypoplasia or absent thumbs.
Keywords: pollicization, thumb hypoplasia, congenital, twin baby
Introduction
The human hand has a sophisticated anatomy that allows it to perform a wide range of actions. The thumb is the most autonomous digit, accounting for approximately 40 to 50% of hand functions. Thumb hypoplasia is a congenital birth defect where a child is born with an underdeveloped or missing thumb (Online Mendelian Inheritance in Man #274205). It is a rare condition affecting approximately 1 in 100,000 live births and occurs equally in both males and females. Although involvement of the right hand is more common than that of the left, both thumbs are affected in approximately 60% of patients with thumb hypoplasia.1
Pollicization is a surgical intervention used to treat thumb hypoplasia. The most common presentation is severe thumb hypoplasia with an unstable carpometacarpal joint or congenitally absent thumb. However, other conditions affecting thumb function, such as tumors, trauma, and macrodactyly and mirror hands, are also indications for pollicization. Surgery involves creating a functional thumb by transferring another finger (usually the index finger) to the thumb position.2 Studies have also revealed transfer of the middle finger after traumatic amputation of the thumb and index finger or tumor ablation surgery.3,4 In addition to improving the physical appearance of the hand, reconstructing the thumb to improve the mobility and stability of pinching and gripping is the main objective of pollicization.
To our knowledge, this is the first report of bilateral index finger pollicization of bilateral hypoplastic thumbs in twin babies.
Case Presentation
Twin children aged 2 years and 8 months, born to a gravida 3, para 2 mother, presented to the Orthopedic department at CURE Children’s Hospital, Ethiopia. The presenting complaint was a bilateral decrease in size and poor thumb function in both children. The children were born at a local health center. The antenatal history was unremarkable, and the mother did not recall the birth weight. Apart from the decreased thumb size, they were born without any anomalies, and their parents had no consanguinity. There was no family history of twin pregnancies on either parent’s side.
On physical examination, both children had bilaterally decreased size of their thumbs with other normal-appearing digits, the wrist in a neutral position, and no limb length discrepancy. They had well-formed skin creases and thenar folds (Figure 1). The children were observed to use their index and long fingers of both hands for pinching. During a passive range of motion, the first web space was tight with excessive adduction at the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints of the thumb. The wrist, elbow, and shoulder ranges of motion were normal. On auscultation, heart sounds were well heard with clear bilateral air entry, no swelling, and no mass over the abdomen. No visible abnormalities were observed in their back or lower limbs.
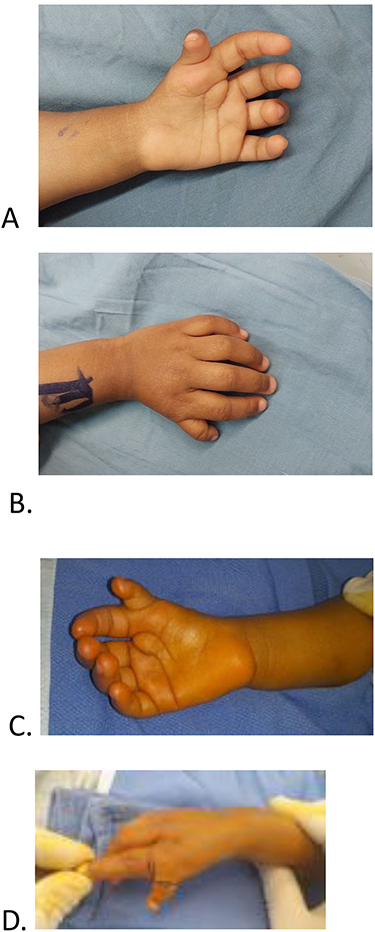 |
Figure 1 Physical appearances of the hands: (A and B) Twin A left hand; (C and D) Twin B right hand. |
X-ray images were taken and showed a significantly decreased thumb size with abnormally developed basal metacarpal bone and deficient first CMC joint, and no radial deviation of the wrist joint (Figure 2). To rule out other associated anomalies, abdominal ultrasonography and echocardiography were performed in both patients, and the results were unremarkable. On complete blood cell count, twin A had hemoglobin of 12.5 g/dl and the platelet count was 356, whereas twin B’s hemoglobin and platelet count were 13.0 g/dl and 429, respectively. Based on the above findings, a diagnosis of type IIIB bilateral thumb hypoplasia was made for both twin children according to the modified Blauth classification,5 and pollicization was performed using the Buck-Gramcko technique, as described by Ezaki et al6,7
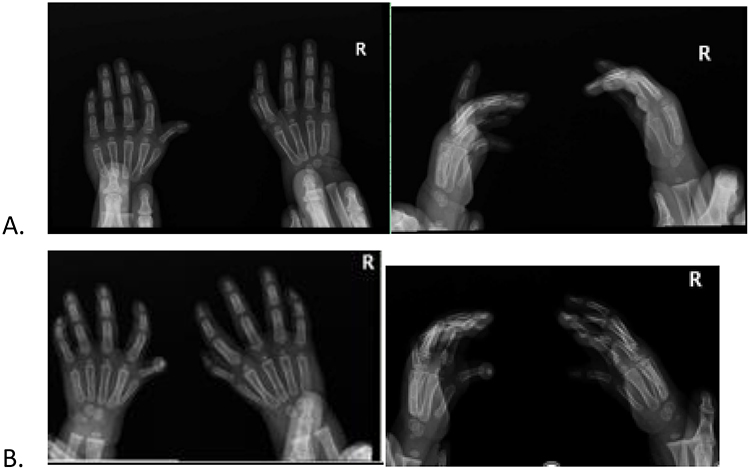 |
Figure 2 Ap and lateral X-ray of bilateral hands of the children: (A) Twin A; (B) Twin B. |
Surgical Procedure
After obtaining informed consent from the family, the infants were taken to the operating theater. General anesthesia was administered with endotracheal intubation and the skin prepared with povidone-iodine and draped. The limb was exsanguinated and an Esmarch’s tourniquet was applied.8 Similar skin incisions were utilized for all four hands, which were designed with a fish mouth appearance over the radial aspect of the index finger, and the palmar incision was more distal than dorsal so that the glabrous skin would be placed over the palmar aspect of the index finger, which in turn would improve the appearance of the index finger in the thumb position (Figure 3).9
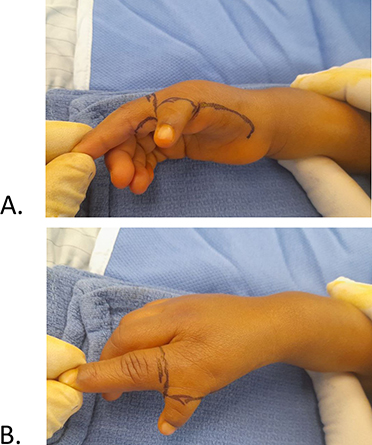 |
Figure 3 Skin design: (A) Palmar skin design; (B) Dorsal skin design. |
The volar skin incision started from the radial aspect of the index finger and continued to the thumb, looking for a vessel within the hypoplastic digit to trace the radial neurovascular bundle of the index finger. After localizing the radial neurovascular bundle of the index finger, dissection proceeded further to the ulna to identify the proper digital artery on the ulnar side of the index finger and common digital arteries in the second web space (Figure 4). To allow tension-free index finger pollicization, the radial proper digital artery of the middle finger was ligated and labeled with a stay suture. The common digital nerve to the second web space was divided along the proper digital nerve to the ulnar side of the index finger and the radial side of the middle finger. No variation was observed during dissection.
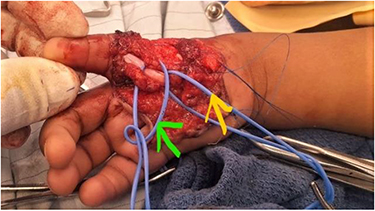 |
Figure 4 Vascular supply of the index finger; radial and ulnar proper digital arteries of the index (green arrow) and deep flexor of the index/FDP (yellow arrow). |
The intervolar plate ligament and fascia between the index and middle fingers were divided. The A1 and A2 pulleys of the index finger were opened to avoid flexor tendon buckling when the digit was shortened. The palmar digital arteries were protected with vessel loops, and dissection proceeded gently over the dorsal side. The dorsal flap was carefully raised to preserve the dorsal vein of the index finger. The extensor digitorum communis (EDC) and the extensor index proprius (EIP) were identified. The tendon of the EDC was severed at the level of the metacarpophalangeal joint for subsequent suturing to the base of the proximal phalanx. The suture was placed over the tendons of the palmar and dorsal interphalangeal muscles before dividing them for later transfer to the proximal interphalangeal joint extensor hood.
About 2 cm of the index finger metacarpal was removed with a distal cut through the physis, where physeodesis was performed to prevent growth of the pollicized index finger. Hence, a 1.0 mm K-wire was inserted retrogradely from the metacarpal head to the proximal phalanx hyperextending into the MCP joint. Using the K-wire as a joystick, the digit was positioned at 35° palmar, 20° radial abduction, and 80° pronation and was secured with the same K-wire (1.0 m). The EDC tendon was sutured to the base of the new thumb to act as the new abductor pollicis longus. The tendons of the first dorsal and palmar interosseous muscles were transferred to the radial and ulnar aspects, respectively, to act as the abductor pollicis brevis and adductor pollicis, respectively. The extensor index proprius acts as the extensor pollicis longus. The tourniquet time was 2 hrs and the vascularity of the new thumb was checked. Any redundant skin was trimmed and the wound was closed in an interrupted fashion.
After releasing the tourniquet, arterial circulation returned within a few seconds in three of the four pollicizations. However, in one case the arterial circulation was delayed beyond the expected time despite the application of warm saline-soaked gauze and release of some suture knots. Subsequently, we removed the K-wire from the proximal segment, after which the circulation returned immediately, which may be explained by inadvertent kinking of the arteries. The digit was then repositioned and fixed with the same K-wire and perfused well postoperatively (Figure 5). The skin was then closed with a 5.0 plain gut and covered with xeroform, fluffs of gauze and cotton, and a long-arm cast was applied.
 |
Figure 5 Postoperative skin perfusion: (A) palmar and (B) dorsal aspect. |
Follow-Up and Outcomes
We removed the cast and K-wires after 6 weeks of immobilization and the pollicized index fingers were well-maintained in the thumbs position. The incisions healed adequately and no wound complications were observed. Hand physiotherapy was started to increase ranges-of-motion exercises, such as playing with different toys and encouraging them to hold a pencil (Figure 6). They were able to pinch at 12 weeks and grabbing at 6 months.
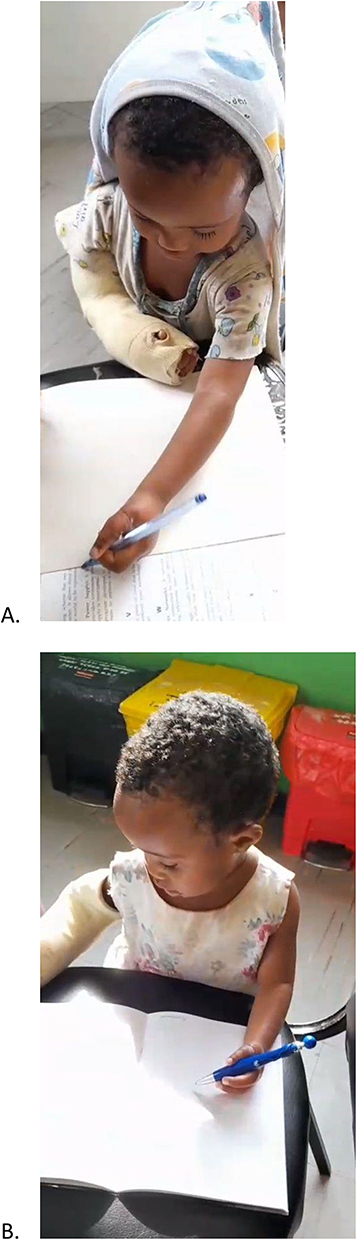 |
Figure 6 Postoperative functional outcome. (A) Twin A, (B) Twin B. |
Discussion
The thumb plays an important role in the daily activities of the human hand. Thumb hypoplasia is a spectrum of congenital abnormalities that can range from minor defects to complete absence of the thumb. An absent thumb is noticed by the parents immediately, but a hypoplastic thumb may not be noticed by the parents and diagnosed by a health-care professional after physical examination.
Embryologically, the appearance of the upper limb bud on day 28 of intrauterine development leads to hand formation. Limb bud development and differentiation are guided by various signaling centers, including the apical ectodermal ridge (AER) for proximodistal longitudinal growth, the zone of polarizing activity (ZPA) for radioulnar limb formation, and the Wnt pathway responsible for dorsoventral differentiation. Furthermore, thumb formation and differentiation are caused by prolonged and concerted interplay between transcription factors such as HOXA13, GLI3, and TBX5.10
In our patients, the exact molecular signal defects were unknown. However, based on the scientific literature, that the hand plate is well-formed (HOXA13) and that there is no extra digit (polydactyly, GLI3 mutation OMIM #174700), TBX5 (OMIM #607323) is incriminated in restraining the thumb length.11,12
Once the diagnosis of thumb hypoplasia is made, it is mandatory to obtain multiple workups, such as complete blood count, cardiac echo, abdominal ultrasound, and chromosome testing, as more than 80% of the cases are associated with other anomalies such as Fanconi’s Anemia, Thrombocytopenia-Absent Radius (TAR) syndrome, Holt Oram syndrome, and VACTERL. Although chromosome testing was not available in our setup, the results of other ancillary diagnostic workups were unremarkable for associated anomalies.13
Therefore, according to the modified Blauth classification, pollicization is a good option for types IIIB, IV, and V.5 Most medical journals have reported pollicization of different digits, such as the index finger, middle finger, and ring finger.2,3 Different authors consider index finger pollicization to be the most suitable technique to restore thumb function in the hand impaired by thumb hypoplasia and an unstable CMC joint.2,5
Following index pollicization, the hand region of the brain adapts itself and exhibits changes in the sensorimotor cortex homunculus. Studies using functional MRI have shown that motor reorganization changes over time and can be influenced by long-term training and experience over a long period of time.14
The ideal age for pollicization remains a topic of debate. It is thought that pollicization is best performed prior to the first birthday of the child, although no evidence exists to prove the best outcomes for the operation performed before 1 year of age. Ezaki et al defer pollicization before 18 months of age, claiming that the child’s hand grows rapidly in early life and that the critical arteriovenous structures can be more accurately identified and protected in older children. The fact that long-term studies did not correlate functional outcomes with the age of the patient at operation and potential cognitive sequelae from anesthesia in infancy confirms that our cases underwent surgery at an acceptable age.7,15,16
Conclusion
In conclusion, we found that it is imperative to follow the key steps of the index finger pollicization procedure to obtain an aesthetically and functionally attractive thumb. Planning incision, identification, and protection of neurovascular structures and careful transposition are all important determinants of index finger viability.
Ethics and Consent
Informed consent was obtained from the family of the children for publication of this case report with accompanying images, and the hospital approved the publication of the cases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tonkin MA. On the classification of congenital thumb hypoplasia. J Hand Surg. 2014;39(9):948–955. doi:10.1177/1753193413516246
2. Sood RF, Taghinia AH, Upton J, Labow BI. Index Finger Pollicization for Hypoplastic Thumb: surgical Technique. Plast Reconstr Surg. 2021;147(1):127–129. doi:10.1097/PRS.0000000000007442
3. Wegerif G, Barlas V, Ali B, Borah G. Pollicization of Long Finger After Traumatic Amputation of Thumb and Index Finger. Cureus. 2020. doi:10.7759/cureus.10760
4. Bahk S, Eo SR, Cho SH, Jones NF. Pollicization of the Middle Finger. J Korean Soc Microsurgery. 2015;24(2):62–67. doi:10.15596/ARMS.2015.24.2.62
5. Kawabata H, Tamura D, Goldfarb CA. Treatment of Blauth Type IIIB Thumb Hypoplasia Using a Nonvascularized Toe Phalanx. J Hand Surg Am. 2021;46(1):68.e1–68.e7. doi:10.1016/j.jhsa.2020.07.007
6. Sletten IN, Røkkum M, Winge MI. Outcome After Pollicization for Congenital Thumb Deficiency: a Cohort Study of Cases in a Single Unit, 1987 to 2016. J Hand Surg Am. 2022;47(5):479.e1–479.e9. doi:10.1016/j.jhsa.2021.05.023
7. Carter PR, Ezaki M, Oishi S. Index pollicization: an evolution of ideas and techniques from a paediatric orthopaedic institution. In: Journal of Hand Surgery: European Volume. Vol. 47. SAGE Publications Ltd; 2022:1004–1015.
8. Kasem SA, Bassiouny AAE, Rashwan DAE, Bahr MH. Minimal inflation tourniquet pressure using induced hypotension with limb occlusion pressure determination or arterial occlusion pressure estimation in upper limb surgery: a randomized double-blinded comparative study. Anesth Pain Med. 2020;10(2). doi:10.5812/aapm.102124
9. Kozin SH. Pollicization: the Concept, Technical Details, and Outcome. Clin Orthop Surg. 2012;4(1):18. doi:10.4055/cios.2012.4.1.18
10. Kozin SH. Embryology of upper extremity. J Craniofacial Surg. 2017;2:1208–1217.
11. Bastida MF, Pérez-Gómez R, Trofka A, et al. The formation of the thumb requires direct modulation of Gli3 transcription by Hoxa13. Proc Natl Acad Sci. 2020;117(2):1090–1096. doi:10.1073/pnas.1919470117
12. Oberg KC. Review of the molecular development of the thumb: digit primera. In: Clinical Orthopaedics and Related Research. New York LLC: Springer; 2014:1101–1105.
13. Thomas BP, Pallapati S. Congenital thumb differences- current concepts. J Clin Orthop Trauma. 2020;11(4):580–589. doi:10.1016/j.jcot.2020.06.018
14. Chen R, Anastakis DJ, Haywood CT, Mikulis DJ, Manktelow RT. Plasticity of the human motor system following muscle reconstruction: a magnetic stimulation and functional magnetic resonance imaging study. Clin Neurophysiol. 2003;114(12):2434–2446. doi:10.1016/S1388-2457(03)00283-9
15. Hellevuo C, V. LO, Kapanen S, Vilkki SK. Long-term outcomes after pollicization: a mean 11-year follow-up study. J Hand Surgery. 2020;45(2):173–180. doi:10.1177/1753193419876475
16. Backeljauw B, Holland SK, Altaye M, Loepke AW. Cognition and brain structure following early childhood surgery with anesthe. Pediatrics. 2015;136(1):e1–12. doi:10.1542/peds.2014-3526
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.