")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 16
Peritoneal Dialysis Patient Training Program to Enhance independence and Prevent Complications: A Scoping Review
Authors Jaelani TR , Ibrahim K , Jonny J, Pratiwi SH, Haroen H, Nursiswati N, Ramadhani BP
Received 27 March 2023
Accepted for publication 4 August 2023
Published 11 September 2023 Volume 2023:16 Pages 207—222
DOI https://doi.org/10.2147/IJNRD.S414447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Toni Rahmat Jaelani,1 Kusman Ibrahim,1 Jonny Jonny,2 Sri Hartati Pratiwi,1 Hartiah Haroen,1 Nursiswati Nursiswati,1 Bunga Pinandhita Ramadhani2
1Faculty of Nursing, Padjadjaran University, Bandung, West Java, Indonesia; 2Nephrology Division, Department of Internal Medicine, Gatot Soebroto Indonesia Army Central Hospital, Jakarta, Indonesia
Correspondence: Toni Rahmat Jaelani, Faculty of Nursing, Padjadjaran University, Jalan Ir. Soekarno Km. 21 Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62-813-2211-0115, Fax +62-022-7795596, Email [email protected]
Background: Peritoneal dialysis (PD) training is essential to ensure patient independence and prevent life-threatening complications, such as peritonitis. The International Society for Peritoneal Dialysis (ISPD) recommends that every PD unit worldwide implement local PD training programs with the goal of improving self-care capabilities. This scoping review aims to give an overview of recent literature and recommendations on PD training programs aiming to improve the quality of care and outcomes for PD patients.
Methods: The literature search was conducted using the PC (Population, Concept) approach. The population of interest in this study is PD patients, and the study concept is the PD training program. Several databases were used to conduct the literature search, including PubMed, Science Direct, and CINAHL. The search process began from July 2022 until January 2023. The inclusion criteria for the search included research articles and recommendations.
Results: The search yielded 22 articles recommending training programs lasting from 5– 8 days, with 1– 3-hour sessions and a nurse-to-patient ratio of 1:1. A cumulative training time of 15 hours or more is recommended to enhance patient independence and reduce peritonitis rates. Home-based or in-unit PD training, conducted by experienced nurses using adult learning strategies, has shown significant value in improving self-care and preventing peritonitis. Evaluating training outcomes should encompass knowledge, skills, and attitudes, and the impact on peritonitis rates. Training programs should be flexible and consider physiological and psychosocial barriers to achieving the best results.
Conclusion: There are a variety of strategies for dialysis training concerning duration, session length, patient-to-trainer ratio, timing, methods, location, compliance, and the need for retraining. More evidence is needed to assess the impact of PD patient training programs on self-care capabilities and peritonitis incidence. Future studies should investigate the effects of training programs on compliance, self-efficacy, and patient and nurse perspectives.
Keywords: training program, peritoneal dialysis, chronic kidney disease, patient education, nursing
Introduction
The United States Renal Data System (USRDS) has reported that hemodialysis (HD) is the dominant form of Renal Replacement Therapy (RRT), with the number of HD users ranging from 111,000 to 113,000 over the course of four consecutive years up to 2018. Meanwhile, despite a yearly upward trend, the utilization of PD as a form of RRT only reached 18,631 cases. Evidence suggests that RRT is underutilized worldwide, particularly in low-to-middle-income countries, where RRT is often unavailable and inaccessible.1 This data aligns with the findings of the Indonesian Renal Registry (IRR) 2018 report, which shows that HD is the most commonly used form of RRT in the country, and only 2% of patients use PD in the form of Continuous Ambulatory Peritoneal Dialysis (CAPD). A significant difference was found between PD and HD patients in Indonesia, despite the increasing end-stage-kidney-disease (ESKD) population. The percentage of patients using HD increased to 40% within five years, contributing to 98–99% of all dialysis patients.2
PD is a well-established RRT option that is associated with several advantages, including the ability to preserve residual renal function, offer greater empowerment to patients and families, efficiently remove solutes and solvents, decrease the burden on neutering, improve survival rates and overall quality of life, which are comparable or even superior to those observed in HD.3 However, PD is also associated with a number of risks of complications, including infectious and non-infectious complications that can lead to PD failure. Among infectious, peritonitis and catheter-related infections, such as exit-site or tunnel infection, are the most common causes of PD failure in patients undergoing CAPD. Non-infectious complications, such as catheter malfunctions caused by changes in catheter position, can also contribute to PD failure. The incidence of infection, including peritonitis, exhibits variability across developed and developing countries. However, the International Society for Peritoneal Dialysis (ISPD) recommends a peritonitis incidence rate of no more than 0.4–0.5 episodes per year for patients with risk factors, with the condition that no more than 80% of patients experience peritonitis within a given year.4,5 Peritonitis is a significant predictor of PD technique failure, mortality, and method switching to HD.6–9
Patients undergoing PD, including CAPD, require robust self-care support to mitigate the risks of complications. ISPD has recommended guidelines for preventing peritonitis through optimal training programs. However, there is still uncertainty about the best methods, location, timing, and trainers recommended for effective PD training.4,5 Given the importance of patient training in reducing the incidence of peritonitis and the discontinuation of PD, ensuring the adequacy of self-care support and training programs is paramount.10,11 While several studies have identified risk factors for peritonitis, little attention has been paid to the role of PD training in reducing this complication. Several studies have recommended observing a suitable training program that improves patient outcomes, particularly in reducing complications such as peritonitis.12–31
The use of PD in Indonesia is hindered by various obstacles. These include the high cost of PD, lack of medical facilities and trained personnel, particularly in remote areas, and insufficient awareness and knowledge about PD among the community and healthcare professionals.2 Additionally, there is no national standard for PD training, which leads to PD units conducting training programs based on their own practices and procedures. The training programs often lack specified durations or standardized nurse-to-patient ratio, and the training evaluation is either non-existent or performed with non-standardized formats. Moreover, the absence of structured home visits or telenursing programs hinders the assessment of patient compliance with PD procedures. These issues emphasize the need to develop and implement standardized PD training programs to ensure patient independence and prevent life-threatening complications such as peritonitis, in Indonesia. Thus, there is a need for current evidence-based guidelines and recommendations to optimize PD training programs. This scoping review identifies and summarizes recent literature studies and recommendations regarding PD training programs worldwide. The findings of this review can inform the development of a standardized and effective PD training program to improve the quality of care and outcomes for PD patients.
Method
The search and selection criteria used in this scoping review study are based on the recommendations of The Joanna Briggs Institute (JBI) in 2014 with the PC (Population & Concept) approach. The study population includes PD patients, and the concept is the training program. The question in the study refers to the PC component: “How is the self-care training program in Peritoneal Dialysis (PD) patients based on the existing literature?”.
The literature sources were obtained from multiple databases, including PubMed, Science Direct, and CINAHL, with Medical Subject Headings (MeSH), used as an alternative search for articles (Table 1). The search process was conducted from the beginning of July 2022 until January 2023.
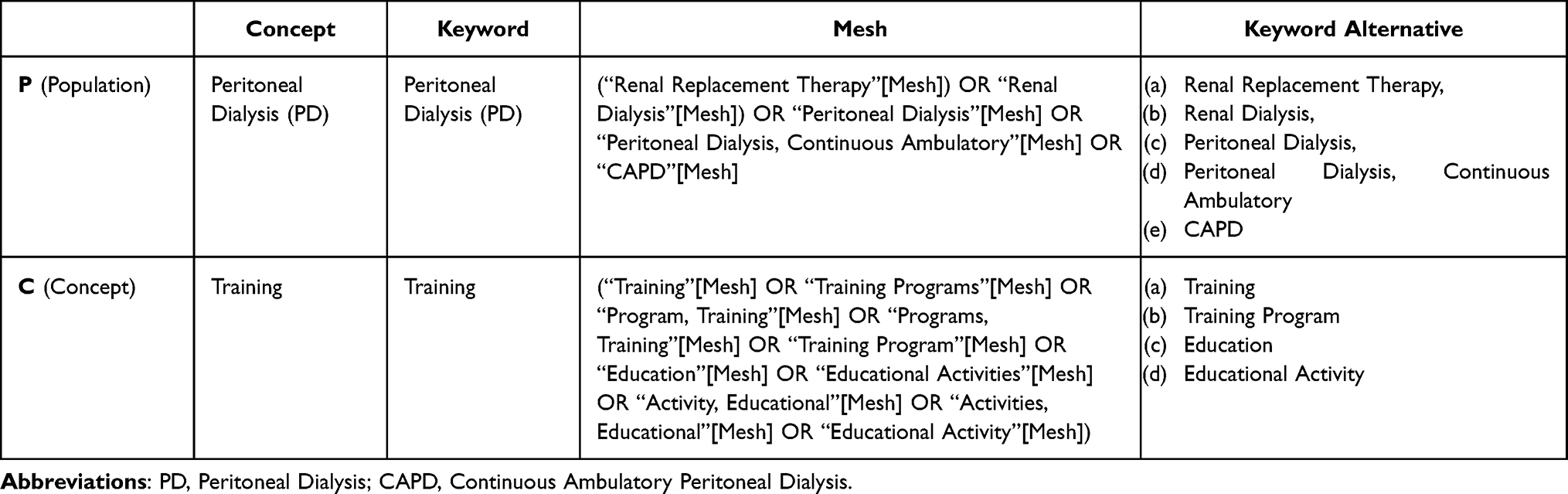 |
Table 1 Data Search |
During the initial search for this study, the database was searched using the keywords “Population” and “Concept” for a limited period between 2002–2023, with full-text English articles only. The search results were imported into Mendeley, and duplicate results were removed using a reference tool. The screening process involved manually sorting the title and abstract to identify articles relevant to the research objectives. The articles that fulfilled the inclusion criteria, namely research articles and recommendations specific to the research questions, were included, while non-research letters, editorials, invited commentary, reviews, abstract-only articles, and other nonspecific articles about the PD training program were excluded. Disagreements were resolved through discussion with other authors. The next step involved a detailed analysis of the full text, resulting in 22 studies for inclusion. The review process is presented in a PRISMA diagram, as shown in Figure 1.
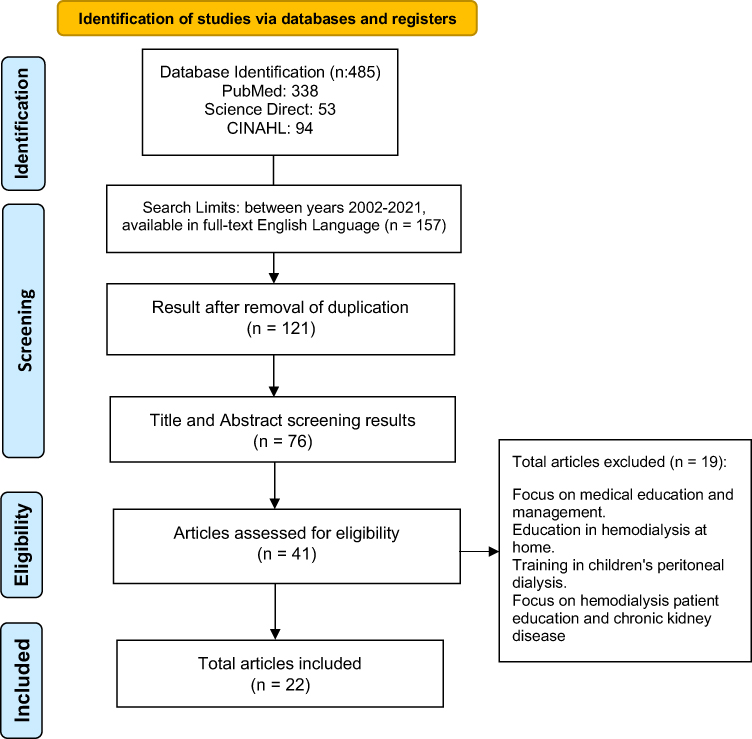 |
Figure 1 PRISMA literature search flowchart. |
Data Extraction
Standardized forms were used, which contained information such as the author, year, title, location, sample, and results. The results were then categorized based on the length or duration of the training program, trainer-to-patient ratio, timing, location, compliance, retraining, and home visits, as well as the qualifications of the trainer staff.
Result
Study Selection
The literature search for this study was conducted from July 2022 until January 2023. The initial search pooled 487 articles, after which 157 articles remained. After removing duplicates, 121 articles were eligible for screening based on their titles and abstracts. Subsequently, 76 articles were selected, and 41 underwent a feasibility assessment. Finally, 22 articles were deemed eligible and included in the study.
Characteristics of Study
The study includes 22 articles with the following designs: five prospective observational research articles, five retrospective observational articles, three articles on experimental studies, one article containing mixed-method, two articles on a randomized control trial, one qualitative article, one comparative article, one article on prospective cohort study, one article on the retrospective case-control study, one article on an international survey, and one article on training recommendations. The studies were conducted in various settings, including Europe (seven articles), America (one article), Latin America (two articles), Asia (six articles), the Middle East (one article), and a multi-centred study (4 articles). The characteristics of the included studies are summarized in Table 2.
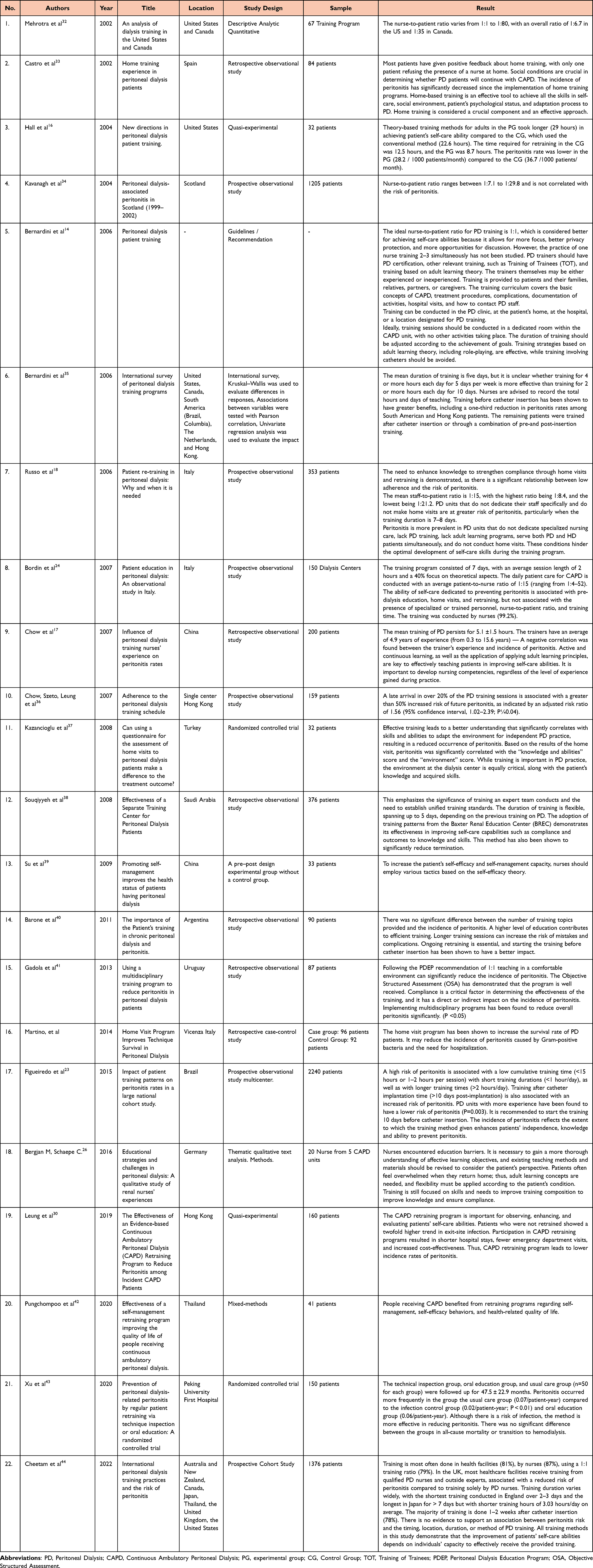 |
Table 2 Characteristics of the Included Studies |
Time and Duration of Peritoneal Dialysis Training
There are ten articles discussing training time. Four articles recommend a training duration of five days with a range of 1–3 hours/session,11,14,45 and one article recommends seven days with a duration of 2 hours/session.24 The cumulative recommended training hours are at least 15 hours.13 One study mentions a duration of 5.1 ±1.5 hours per day or per session,17 and one article reports 29 hours of training on adult learning concepts and 22.6 hours with conventional learning.16
Other studies conducted training for 7–8 days without specifying the number of sessions.18 One article emphasizes that longer training leads to errors and a greater risk of complications.40 Another study shows that the shortest training time is 2–3 days and the longest is > 7 days, but with short training hours, averaging 3.03 hours/day, and both durations show no risk of peritonitis.44
The Ratio of Nurse-to-Patient During Peritoneal Dialysis Training
Six articles discuss the nurse-to-patient ratio during PD training. Two of them suggest that the ratio of nurses has an insignificant impact on the incidence of peritonitis. Three articles recommend a 1:1 nurse-to-patient ratio, while the remaining articles suggest a larger ratio.14,18,24,32,34,44
Time of Training
Training time recommended before catheter insertion was reported in three studies.14,23,40 One study found that more training was conducted 1–2 weeks after catheter insertion (78%), while the rest was carried out after catheter insertion or a combination of before and after catheter insertion, particularly in Japan.44 Another article found greater benefits in combining training before and after catheter insertion.40 Generally, training conducted before catheter insertion is recommended, but following local policy, it may be appropriate to consider training before and after catheter insertion. This aligns with the principle that PD training should not be done in patients with catheters to avoid the risk of infections during the training.
Training Strategy
Four studies recommend training with adult learning methods to achieve patient independence.14,16,17,26 Such training should be adjusted based on the patient’s ability and assessment of learning needs. In one article, conventional learning was compared with adult learning methods in terms of their effectiveness, cumulative duration, and incidence of peritonitis.
Training Location
Four articles discuss the PD training locations, in which one explains that larger and more experienced dialysis locations provide more significant benefits in reducing peritonitis.14,23,33,44 Another recommendation offers more comprehensive options for training locations, though it does not specify which is better. In contrast, one study observed more benefits when training was conducted in the patient’s home,33 while another study found that more training was conducted in healthcare facilities, with no evidence to support peritonitis.
Compliance, Retraining, and Home Visits
Six articles found that home visits and retraining can reduce peritonitis related to compliance, knowledge, and skills from training outcomes.18,24,33,37,43,46 One other article found that training is associated with compliance and the incidence of peritonitis.41 One study examined that non-compliance with training schedules, such as late arrival, can increase the risk of peritonitis.17 Two articles found that retraining is linked to decreased peritonitis, hospitalizations, and low ER visits.16,30 Two other articles resulted in training with reasonable strategies to improve self-efficacy, which leads to adherence during home care.39,42 One RCT found that retraining through monitoring the engineering inspection group, the oral education group, and the ordinary treatment group showed that the peritonitis clearance time for the groups with infection and oral education had a lower risk than regular treatment and those who were transferred to hemodialysis. All causes of death did not differ significantly between groups.43
Trainer Staff Qualifications
Six articles specifically mention the qualifications of trainer staff.14,17,18,24,44 The trainer must have PD certification and supporting training certification for the healthcare worker. All articles discuss the correlation between a trainer’s certification and experience in improving a patient’s self-care abilities and reducing the incidence of peritonitis.
Discussion
Time and Duration of Peritoneal Dialysis Training
The included study provides an overview of the initial training time for PD patients with varying durations of independence. The use of adult learning methods for initial training may take longer, but it is considered effective and can result in shorter retraining times in achieving patient independence and reducing peritonitis.16 The duration of training per session will determine how long the training is conducted. The recommended duration ranges from 1–3 hours per session, with a total training duration of more than 15 hours spread over 5–8 days, according to ISPD and numerous studies. This has been shown to improve independence outcomes and reduce peritonitis rates.13,17,24,35,47 However, longer sessions and durations (>13 sessions) are statistically significant risk factors for higher peritonitis risk but are not associated with shorter permanence in PD.48
The important role of patients is found in training programs that are conducted within a duration of fewer than 5 days, with flexible session durations and topics in accordance with ISPD recommendations, in order to achieve independence. The importance of repeated training and adherence to ISPD standards was found in studies with a total training duration of 25–40 hours per week.49 Other studies showed that there was no significant training duration associated with a reduction in the risk of peritonitis.24,44 Similarly, the timing of training initiation, training duration, location, or use of competency assessment did not predict the risk of peritonitis.24 However, they were associated with pre-dialysis education, home visits, and retraining.
The duration of training can affect the effectiveness of a program in achieving self-care abilities, as it is related to changes in patient’s physiological conditions, boredom, and decreased patient concentration, which can increase the risk of errors in the learned procedures.23 A study showed that the shortest training duration was 2–3 days, while the longest was over 7 days, but with shorter training hours, averaging 3.03 hours per day. Neither duration showed a risk of peritonitis while yielding similar improvements in self-care abilities.44 A flexible 5-day training program with variable training durations based on the patient’s condition and prior independent PD knowledge was found to be effective.38 Nearly all studies regarding training duration provided insights into outcomes such as peritonitis and self-care abilities. Longer training periods with manipulation of patient catheters increased the risk of peritonitis.38 All training durations should be adapted based on the assessment of training needs and the achievement of goals in attaining patient independence.4,45
The duration, timing and session length of the training will be adjusted according to each individual patient and the unit’s experience in providing training. Assessment of patient needs during training recommended ISPD using the VARK instrument (Visual, Aural, Read/Write & Kinesthetic).50,51 Training time may also differ for the elderly population, people with comorbidities, and those with a low educational status who may require longer training to acquire self-care skills due to the higher risk of peritonitis.11 Many studies have shown that elderly age (>65th) is a risk factor for peritonitis.44 Other studies have found that training for parents, patients with comorbidities, and those with low educational status requires longer training to achieve self-care abilities and is more likely to develop peritonitis.11 It is also necessary to consider specific issues related to the aging process, such as weakness, dementia, loneliness, vision and hearing impairments, cognitive dysfunction, and mobility issues.45
ISPD has provided recommendations to increase studies related to training programs, especially regarding the number of training hours per day, total hours, and teaching days. Studies are also recommended to accommodate the local uniqueness of each unit to be developed and report on its results, primarily related to the incidence of peritonitis and exit site infection. Nevertheless, ISPD emphasizes that not only the time, pattern, and criteria of training alone are important but also the achievement of the educational objectives of the planned program to achieve patient independence and prevent peritonitis.4,5
The Nurse-to-Patient Ratio During Peritoneal Dialysis Training
Training has become an essential responsibility of nurses, with 99.2% of training being performed by them.24 Training should be conducted in a comfortable and private setting, ensuring nurses are not disturbed during training.41 A 1:1 ratio of nurse-to-patient has shown better outcomes in achieving self-care abilities, which is associated with increased focus, privacy and more opportunities for discussion.32,35,45 Additionally, the dedication of nurses solely serving PD patients, without concurrent HD services, has shown superior outcomes in improving self-care abilities and reducing peritonitis.45,52 However, other studies have found no relationship between the nurse-to-patient ratio and the dedicated self-care abilities for preventing peritonitis.24,34
Time of Training
The optimal timing for PD training is 10 days before catheter placement, as the incidence of peritonitis increases with training conducted 10 days or more after catheter insertion.23 It is not recommended to provide training for patient independence directly on an already placed catheter when the patient has not been confirmed to be capable of performing self-care. Training that begins with simulation on a manikin is recommended in the ISPD syllabus, and direct self-care of the catheter is performed once the patient has been deemed capable during the simulation phase.4 Consideration should be given to the risk of infection when manipulating the catheter for learning purposes, and the patient’s readiness to cope with the new condition of self-care should be prepared in advance. While early training for CAPD is recommended, adherence to proper procedures is important in preventing the risk of infection.
Training Strategy
The adult learning method is more effective for training patients in PD. This method focuses on patients’ abilities, needs, and responses, providing them with a comfortable and easily understood learning experience. The ultimate goal is to improve the patient’s adherence to the procedure and reduce infection-related complications, particularly peritonitis. In adult learning, it is crucial to prioritize relevant and updated information that can be applied relatively quickly and facilitate changes in patients’ knowledge and behaviors to support their health.23
Training initiation with adult learning principles yields good self-care abilities and lower rates of peritonitis.17 Trainers should be willing to develop appropriate training skills based on adult learning principles.16,17,26,35 PD training can be provided to the patient themselves, family members, relatives, partners or third-party caregivers, depending on the capabilities of the patient and their family. Other studies have shown that training programs conducted by a third party connected with PD nurses yield better results in improving self-care.38 Patients should be facilitated to determine their own learning pace. When training individual patients, nurses should consider the response to uremic impacts and other medical conditions that may hinder training.4,22,45 A study of 280 PD patients found that 33.9% required assistance, particularly due to physical (62.1%) or operational (66.3%) disabilities, and showed better outcomes. Patients who had barriers to PD self-care but still performed PD without assistance and were older exhibited a higher prevalence of diabetic nephropathy and PD-related infections, lower educational levels, and lower serum albumin (p < 0.05).53
The focus of patient self-care training is to increase knowledge and the ability to perform fluid exchange procedures, exit site care, and ensure an attitude conducive to preventing complications.4 Therefore, a safe, effective, and well-planned training program should be prepared by the PD unit to train patients.13,35 Patient self-care abilities can be obtained through structured training patterns or criteria to enhance knowledge, skills, and attitudes.54,55 Poorly performed self-care procedures such as skipping the use of masks and other standard procedures are independent risk factors for peritonitis.9,21
A training program utilizing computerized guidelines (Cycler Training Curriculum) can achieve the goal of increasing patient independence, even in the presence of barriers such as physical disabilities, differences in education, and technical experience in computer or technology usage.56 Guidance from the PD team is an essential part of achieving the goal of improving self-care abilities. All of these conditions indicate that the acceptance of training program patterns or criteria is highly influenced by the capabilities and involvement of individual participants, companions, or family members, as well as the competencies of the trainers themselves.35,44,54,57
Various media such as video playback, booklets, and manikins greatly facilitate the accelerated improvement of patient self-care abilities, particularly during training intervals or when training is conducted. Several concept-or-theory-based learning approaches, such as the Health Belief Model (HBM)58 and Orem’s nursing theory,59,60 have been proven to enhance knowledge, skills, attitudes and create a supportive environment for PD patients’ self-care at home.
Study Location
The study can be conducted at various locations, such as PD clinics, hospitals, patients’ homes, or appropriate areas facilitated with PD training, ideally in a specialized room in the CAPD unit.15 A larger HD unit contributes to a lower risk of peritonitis as experienced units have implemented good standards and have trainers with capable skills who handle more frequent and complex cases and procedures. In the absence of a home visit, training in patients’ homes is crucial to ensure a safe environment, including a safe place for a procedure, sanitation, lighting, and air circulation. Home visit-based training has shown better results in evaluating compliance and self-care by enhancing knowledge and skills.11,33,37
Compliance, Retraining, and Home Visits
The training program is believed to improve compliance, self-efficacy, and quality of life in PD patients.39,41,42 Studies have shown that adherence and compliance can be improved through initial training programs, and the need for retraining can indicate areas where patients require further education. Compliance can be assessed through home visits or hospital visits. Retraining will be shorter in duration for patients who have received comprehensive initial training using adult learning methods.16 Retraining programs can help improve self-care abilities, especially in patients with specific barriers.49 Retraining program is believed to play a major role in reducing the risk of peritonitis and enhancing self-care abilities.61 These findings are consistent with other studies that have found a relationship between home visits and retraining with dedicated self-care abilities to prevent peritonitis.24
Long-term therapy can cause fatigue and procedural errors leading to complications, making the maintenance of retraining programs crucial for patient safety.40 The ISPD recommends retraining for patients undergoing extended hospitalization, post-peritonitis, altered mental status, changes in the products used, completion of the CAPD program after HD, and catheter infection. The recommendations are in line with the guideline from the United Kingdom, which recommends patients must undergo retraining every year or more frequently if there is associated with infection.14,23,62 Home visits are essential for observing practical procedures, assessing compliance, and creating a supportive environment. An article by Bordin et al (2007) stated home visit correlates with a lower peritonitis rate. Schaepe et al (2015) found improved training outcomes through home visits. Home visits determine the need for retraining in reducing various complications, including peritonitis, and became part of observing observational procedures of action, environment, and psychosocial support.16,18–21,23,30,42 Another study that the importance of home visits to ascertain the weakest point in patients in carrying out PD procedures.63 Video training is also an effective alternative that can significantly reduce the number of home visits.64 Once training is complete and the patient begins PD, home visits by PD nurses are critical for detecting compliance with all procedures taught in training and reducing the risk of peritonitis.5,24 In conclusion, home visits are an important tool for observing technique procedures, assessing compliance, and improving training outcomes, ultimately reducing the risk of peritonitis.
Trainers Staff Qualifications
All of the selected studies emphasize the importance of trainers having basic PD training and specialized training for teaching PD patients using the adult learning method to lower the risk of peritonitis and enhance patient independence. While trainer experience is essential, active training of nurses is necessary to maintain their competence in teaching PD patients, as this competence cannot be solely acquired through experience alone.17 Some studies measure experience in terms of years worked, but the selected studies define experience as the duration of work in a specialized PD unit.
The qualifications of the nurses should also be seen by who is training them. As described in some studies in China and Hong Kong, there is a different impact with junior and senior trainers, where senior nurses will serve patients with more complicated conditions, and vice versa. The involvement of third-party nurse trainers was implemented in the United Kingdom, which showed a decrease in the peritonitis rate. However, the training is mainly conducted by nurses working in PD units (87%).44 Nonetheless, some recommendations and studies acknowledge the limitations of PD nurses who may lack competence and training in adult education.40 It is essential to qualify competent staff in conducting training evaluations to identify training programs, obstacles, and ways to overcome them by the medical and nurse care team.65
However, other studies have found a negative relationship between trainer experience and self-care abilities as well as the incidence of peritonitis, emphasizing the importance of training for nursing staff.17 Therefore, training and retraining are needed for the CAPD team to improve their experience and skills so that CAPD can become a more acceptable modality of RRT with better outcomes.7
Conclusion
Our review included a total of 22 training programs for PD patients to achieve self-reliance. Despite current training recommendations, the study showed variations in PD patient training program strategies, and various outcomes regarding the incidence of peritonitis were observed across studies. Several studies and ISPD recommendations acknowledge the lack of evidence regarding training criteria or patterns. Therefore, existing recommendations can serve as a starting point for PD centers to develop relevant training patterns that suit their local unit conditions. These patterns should aim to achieve the same training objectives and include evaluations of their impact on self-care abilities and various complications, including peritonitis. Home visits are considered the best method for assessing knowledge and compliance with procedural practices and identifying the need for retraining. Additionally, the peritonitis rate is an important indicator to evaluate training effectiveness in the long term. The findings of this review highlight the importance of developing an evidence-based PD training program that can be implemented in countries that have not yet established standardized PD training programs, such as Indonesia. By implementing a well-structured training program, patients can achieve independence and minimize life-threatening complications such as peritonitis, leading to better patient outcomes.
Recommendation
More studies need to be conducted to look for various patterns of PD patients’ self-reliance training and their impact on complications, compliance assessments, and self-efficacy. The effectiveness of local training programs and combinations with ISPD recommendations need to be evaluated for evidence in the future. The perspectives of patients and trainers will help provide an overview of the direct and indirect effects of PD training programs on various risks of PD complications.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Okpechi IG, Jha V, Cho Y, et al. The case for increased peritoneal dialysis utilization in low-and-lower-middle-income countries. Nephrology. 2022. doi:10.1111/nep.14024
2. Jonny VL, Kusumaningrum VF. Peritoneal dialysis in Indonesia: current status, challenges and prospects. Peritoneal Dialysis Int. 2022;42(4):428–433. doi:10.1177/08968608211034985
3. François K, Bargman JM. Evaluating the benefits of home-based peritoneal dialysis. Int J Nephrol Renovasc Dis. 2014;7:447–455. doi:10.2147/IJNRD.S50527
4. Li PK, Szeto CC, Piraino B, et al. ISPD peritonitis recommendations: 2016 update on prevention and treatment. Peritoneal Dialysis Int. 2016;36(5):481–508. doi:10.3747/pdi.2016.00078
5. PKT L, Chow KM, Cho Y, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Peritoneal Dialysis Int. 2022;42(2):110–153. doi:10.1177/08968608221080586
6. Hsieh YP, Chang CC, Wen YK, Chiu PF, Yang Y. Predictors of peritonitis and the impact of peritonitis on clinical outcomes of continuous ambulatory peritoneal dialysis patients in Taiwan—10 years’ experience in a single center. Peritoneal Dialysis Int. 2014;34(1):85–94. doi:10.3747/pdi.2012.00075
7. Wearne N, Kilonzo K, Effa E, et al. Continuous ambulatory peritoneal dialysis: perspectives on patient selection in low- to middle-income countries. Int J Nephrol Renovasc Dis. 2017;10:1–9. doi:10.2147/IJNRD.S104208
8. Ma X, Shi Y, Tao M, et al. Analysis of risk factors and outcome in peritoneal dialysis patients with early-onset peritonitis: a multicentre, retrospective cohort study. BMJ Open. 2020;10(2):e029949. doi:10.1136/bmjopen-2019-029949
9. Tian Y, Xie X, Xiang S, et al. Risk factors and outcomes of high peritonitis rate in continuous ambulatory peritoneal dialysis patients: a retrospective study. Medicine. 2016;95(49):e5569. doi:10.1097/MD.0000000000005569
10. Piraino B, Bernardini J, Brown E, et al. ISPD position statement on reducing the risks of peritoneal dialysis-related infections. Peritoneal Dialysis Int. 2011;31(6):614–630. doi:10.3747/pdi.2011.00057
11. Schaepe C, Bergjan M. Educational interventions in peritoneal dialysis: a narrative review of the literature. Int J Nurs Stud. 2015;52(4):882–898. doi:10.1016/j.ijnurstu.2014.12.009
12. Kong ILL, Irene LP, Mok GWS, et al. Setting Up A Continuous Ambulatory Peritoneal Dialysis Training Program. Peritoneal Dialysis International: Journal of the International Society for Peritoneal Dialysis. 2003;23(2_suppl):178–182. doi:10.1177/089686080302302s37
13. Figueiredo AE, Bernardini J, Bowes E, et al. A Syllabus for Teaching Peritoneal Dialysis to Patients and Caregivers. Perit Dial Int. 2016;36(6):592–605. doi:10.3747/pdi.2015.00277
14. Judith Bernardini VP. Peritoneal Dialysis Patient Training, 2006. Int Soc Peritoneal Dialysis. 2006;15(4):243–247.
15. Bender FH, Bernardini J, Piraino B. Prevention of infectious complications in peritoneal dialysis: best demonstrated practices. Kidney Int. 2006;70(SUPPL. 103):S44–S54. doi:10.1038/sj.ki.5001915
16. Hall G, Bogan A, Dreis S. New directions in peritoneal dialysis patient training. Nephrol Nursing J. 2004;31:49.
17. Chow KM, Szeto CC, Law MC, Fun Fung JS, Li PKT. Influence of peritoneal dialysis training nurses’ experience on peritonitis rates. Clin J Am Soc Nephrol. 2007;2(4):647–652. doi:10.2215/CJN.03981206
18. Russo R, Manili L, Tiraboschi G, et al. Patient re-training in peritoneal dialysis: why and when it is needed. Kidney Int. 2006;70(SUPPL. 103):127–132. doi:10.1038/sj.ki.5001929
19. Ballerini L, Paris V. Nosogogy: when the learner is a patient with chronic renal failure. Kidney Int. 2006;70(SUPPL. 103):122–126. doi:10.1038/sj.ki.5001928
20. Bieber SD, Mehrotra R. Patient and Technique Survival of Older Adults with ESRD Treated with PeritonealDialysis. Perit Dial Int. 2015;35(6):612–617. doi:10.3747/pdi.2015.00050
21. Dong J, Chen Y. Impact of the bag exchange procedure on risk of peritonitis. Peritoneal Dialysis Int. 2010;30(4):440–447. doi:10.3747/pdi.2009.00117
22. Zhang L, Hawley CM, Johnson DW. Focus on peritoneal dialysis training: working to decrease peritonitis rates. Nephrol Dialysis Transplant. 2016;31(2):214–222. doi:10.1093/ndt/gfu403
23. Figueiredo AE, Moraes TP, Bernardini J, et al. Impact of patient training patterns on peritonitis rates in a large national cohort study. Nephrol Dial Transplant. 2015;30(1):137–142. doi:10.1093/ndt/gfu286
24. Bordin G, Casati M, Sicolo N, Zuccherato N, Eduati V. Patient education in peritoneal dialysis: an observational study in Italy. J Ren Care. 2007;33(4):165–171. doi:10.1111/j.1755-6686.2007.tb00067.x
25. Gadola L, Poggi C, Dominguez P, Poggio MV, Lungo E, Cardozo C. Risk factors and prevention of peritoneal Dialysis-Related peritonitis. Peritoneal Dialysis Int. 2019;39(2):119–125. doi:10.3747/pdi.2017.00287
26. Bergjan M, Schaepe C. Educational strategies and challenges in peritoneal dialysis: a qualitative study of renal nurses’ experiences. J Clin Nurs. 2016;25(11–12):1729–1739. doi:10.1111/jocn.13191
27. Cho Y, Johnson DW. Peritoneal dialysis-related peritonitis: towards improving evidence, practices, and outcomes. Am J Kidney Dis. 2014;64(2):278–289. doi:10.1053/j.ajkd.2014.02.025
28. Shubayra A Brief Communication Continuous Ambulatory Peritoneal Dialysis: nurses’ Experiences of Teaching Patients; 2015. Available from: http://www.sjkdt.org.
29. Hurst H. A new peritoneal dialysis training guideline from the ISPD nursing committee. Peritoneal Dialysis Int. 2016;36(6):585–586. doi:10.3747/pdi.2016.00191
30. Leung WY. The Effectiveness of an Evidence-based Continuous Ambulatory Peritoneal Dialysis (CAPD) Retraining Program to Reduce Peritonitis among Incident CAPD Patients. PQDT - Global. 2019;184.
31. Yang Z, Xu R, Zhuo M, Dong J. Advanced nursing experience is beneficial for lowering the peritonitis rate in patients on peritoneal dialysis. Peritoneal Dialysis Int. 2012;32(1):60–66. doi:10.3747/pdi.2010.00208
32. Mehrotra R, Blake P, Berman N, Nolph KD. An analysis of dialysis training in the United States and Canada. Am J Kidney Dis. 2002;40(1):152–160. doi:10.1053/ajkd.2002.33924
33. Castro MJ, Celadilla O, Muñoz I, et al. Home training experience in peritoneal dialysis patients. EDTNA-ERCA J. 2002;28(1):36–39. doi:10.1111/j.1755-6686.2002.tb00196.x
34. Kavanagh D, Prescott GJ, Mactier RA. Peritoneal dialysis-associated peritonitis in Scotland (1999-2002). Nephrol Dialysis Transplant. 2004;19(10):2584–2591. doi:10.1093/ndt/gfh386
35. Bernardini J, Price V, Figueiredo A, Riemann A. International survey of peritoneal dialysis training programs. Ind Innov. 2006. doi:10.1080/1366271032000141643
36. Chow KM, Szeto CC, Leung CB, Law MC, Kwan BCH, Li PKT. Adherence to peritoneal dialysis training schedule. Nephrol Dialysis Transplant. 2007;22(2):545–551. doi:10.1093/ndt/gfl563
37. Kazancioglu R, Ozturk S, Ekiz S, Yucel L, Dogan S. Can using a questionnaire for assessment of home visits to peritoneal dialysis patients make a difference to the treatment outcome? J Ren Care. 2008;34(2):59–63. doi:10.1111/j.1755-6686.2008.00023.x
38. Souqiyyeh MZ, Al-Wakeel J, Al-Harbi A, et al. Effectiveness of a separate training center for peritoneal dialysis patients. Saudi J Kidney Dis Transpl. 2008;19(4):574–582.
39. Su CY, Lu XH, Chen W, Wang T. Promoting self-management improves the health status of patients having peritoneal dialysis. J Adv Nurs. 2009;65(7):1381–1389. doi:10.1111/j.1365-2648.2009.04993.x
40. Barone RJ, Campora MI, Gimenez NS, Ramirez L, Santopietro M, Panese SA. The importance of the Patient’s training in chronic peritoneal dialysis and peritonitis. Adv Perit Dial. 2011;27(December 2015):97–100.
41. Gadola L, Pogg C, Poggio M, et al. Using a multidisciplinary training program to reduce peritonitis in peritoneal dialysis patients. Peritoneal Dialysis Int. 2013;33(1):38–45. doi:10.3747/pdi.2011.00109
42. Pungchompoo W, Parinyajittha S, Pungchompoo S, Kumtan P. Effectiveness of a self-management retraining program improving the quality of life of people receiving continuous ambulatory peritoneal dialysis. Nurs Health Sci. 2020;22(2):406–415. doi:10.1111/nhs.12672
43. Xu Y, Zhang Y, Yang B, et al. Prevention of peritoneal dialysis-related peritonitis by regular patient retraining via technique inspection or oral education: a randomized controlled trial. Nephrol Dialysis Transplant. 2020;35(4):676–686. doi:10.1093/ndt/gfz238
44. Cheetham MS, Zhao J, McCullough K, et al. International peritoneal dialysis training practices and the risk of peritonitis. Nephrol Dial Transplant. 2022;37(5):937–949. doi:10.1093/ndt/gfab298
45. Hurst H, Figueiredo AE. The needs of older patients for peritoneal dialysis: training and support at home. Peritoneal Dialysis Int. 2015;35(6):625–629. doi:10.3747/pdi.2014.00337
46. Martino F, Adibelli Z, Mason G, et al. Home visit program improves technique survival in peritoneal dialysis. Blood Purif. 2014;37(4):286–290. doi:10.1159/000365168
47. Bernardini J, Price V, Figueiredo A. ISPD GUIDELINES / RECOMMENDATIONS Peritoneal Dialysis Training. Peritoneal Dialysis Int. 2006;26(May):625–632. doi:10.1177/089686080602600602
48. Sosa Barrios RH, Burguera Vion V, Campillo Trapero C, et al. Peritoneal dialysis (PD) technique training: what features influence learning time? Clin Exp Nephrol. 2021;25(3):289–296. doi:10.1007/s10157-020-01990-w
49. Chen TW, Li SY, Chen JY, Yang WC. Training of peritoneal dialysis patients - Taiwan’s experiences. Peritoneal Dialysis Int. 2008;28:72–75. doi:10.1177/089686080802803s15
50. Thepsatitporn S, Pichitpornchai C. Visual event-related potential studies supporting the validity of VARK learning styles’ visual and read/write learners. Adv Physiol Educ. 2016;40(2):206–212. doi:10.1152/advan.00081.2015
51. Auguste BL, Girsberger M, Kennedy C, et al. Are adverse events in newly trained home dialysis patients related to learning styles? A single-centre retrospective study from Toronto, Canada. BMJ Open. 2020;10(1):e033315. doi:10.1136/bmjopen-2019-033315
52. Bernardini J, Valerie P, Figueiredon A. PERITONEAL DIALYSIS PATIENT TRAINING, 2006. Int Soc Peritoneal Dialysis. 2006;15(4):243–247.
53. Huang J, Gu A, Li N, et al. Self-care or assisted PD: development of a new approach to evaluate manual peritoneal dialysis practice ability. Ren Fail. 2022;44(1):1319–1325. doi:10.1080/0886022X.2022.2108448
54. Darmayanti D, Simatupang TM, Rudito P. Patient engagement activities with health care professionals in continuous ambulatory peritoneal dialysis therapy: an exploratory pilot study. Int J Nephrol Renovasc Dis. 2019;12:103–112. doi:10.2147/IJNRD.S185691
55. Schellartz I, Ohnhaeuser T, Mettang T, Scholten N. The role of personal attitudes of control and responsibility for the uptake of peritoneal dialysis- a national survey among dialysis patients. BMC Nephrol. 2021;22(1). doi:10.1186/s12882-021-02303-3
56. Bernardini J, Davis DJ. Evaluation of a computer-guided curriculum using animation, visual images, and voice cues to train patients for peritoneal dialysis. Peritoneal Dialysis Int. 2014;34(1):79–84. doi:10.3747/pdi.2012.00304
57. Perl J, Fuller DS, Bieber BA, et al. Peritoneal Dialysis-Related Infection Rates and Outcomes: results From the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS). Am J Kidney Dis. 2020;76(1):42–53. doi:10.1053/j.ajkd.2019.09.016
58. Peikani F, Shahgholian N, Kazemi A. The effect of health-belief-model-based training on behaviors preventing peritonitis in patients on peritoneal dialysis. Int J Prev Med. 2018;9(1). doi:10.4103/ijpvm.IJPVM_566_17
59. Horsburgh ME Self-Care of Well Adult Canadians and Adult Canadians with End Stage Renal Disease. Available from: www.elsevier.com/locate/ijurstu.
60. O’Shaughnessy M. Application of Dorothea Orem’s Theory of Self-Care to the Elderly Patient on Peritoneal Dialysis. Nephrol Nurs J. 2014;41(5):495–497.
61. Tamayo Isla RA, Mapiye D, Swanepoel CR, Rozumyk N, Hubahib JE, Okpechi IG. Continuous ambulatory peritoneal dialysis in Limpopo province, South Africa: predictors of patient and technique survival. Peritoneal Dialysis Int. 2014;34(5):518–525. doi:10.3747/pdi.2013.00334
62. Campbell D. Peritoneal dialysis-related infections in patients on peritoneal dialysis and measures designed to prevent them. 2016.
63. Ozturk S, Yucel L, Guvenc S, Ekiz S, Kazancioglu R. Assessing and training patients on peritoneal dialysis in their own homes can influence better practice. J Ren Care. 2009;35(3):141–146. doi:10.1111/j.1755-6686.2009.00089.x
64. Viglino G, Neri L, Barbieri S, Tortone C. Peritoneal dialysis training performed remotely: results and comparison with Home Training. Clin Exp Nephrol. 2022;27(1):72–78. doi:10.1007/s10157-022-02276-z
65. Mehrotra R. Peritoneal dialysis education: challenges and innovation. Semin Dial. 2018;31(2):107–110. doi:10.1111/sdi.12666
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.