")
Back to Journals » Open Access Surgery » Volume 17
Perioperative Blood Transfusion Strategies in Orthopaedic Surgery: A Comprehensive Review and Analysis
Authors Yaregal Melesse D , Admass BA , Admassie BM
Received 15 July 2023
Accepted for publication 4 March 2024
Published 11 March 2024 Volume 2024:17 Pages 55—62
DOI https://doi.org/10.2147/OAS.S430812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Debas Yaregal Melesse, Biruk Adie Admass, Belete Muluadam Admassie
Department of Anaesthesia, University of Gondar, Gondar, Amhara, Ethiopia
Correspondence: Debas Yaregal Melesse, Email [email protected]
Introduction: Perioperative blood transfusions are necessary during orthopaedic surgery since it is linked with significant bleeding. Remember that receiving blood transfusions containing various blood components might lead to a number of problems. In order to draw conclusions on perioperative blood transfusion methods in orthopaedic surgery, including adjuvants, this literature analysis looks at the most recent data that are currently available.
Methods: Databases and other sources were searched for pertinent literature. The following databases were searched for recent evidence: MEDLINE, EMBASE, SCOPUS, PubMed, Google Scholar, the Cochrane Library, and Science Direct. Medical heading subjects (MeSH) were merged with Boolean operators such as OR, AND, and NOT, which restrict or broaden the scope of possible supporting evidence. The weight of the evidence supporting each conclusion was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.
Results: The included literatures cover a wide range of topics, including fracture type, perioperative bleeding management techniques like adjuvant therapies used to reduce problems from blood transfusions, and hemoglobin thresholds for blood transfusion.
Conclusion and Recommendations: Patients who are at danger of bleeding during surgery or who are anemic should be handled with medication, allogenic blood transfusions (restrictive type), adjuvants, and non-pharmacological methods such tourniquets and cell savers. Instead of relying just on one transfusion technique, healthcare personnel should consider the patient’s situation in depth and use a variety of transfusion tactics.
Keywords: anemia, blood transfusion, orthopedics, perioperative, strategies
Introduction
Orthopedic operations are difficult, regularly carried out procedures that involve extensive bleeding during the operation and blood transfusions afterward.1 According to a Romanian study, 1,557,247 orthopaedic procedures were performed between 2001 and 2022.2 The balance between bleeding and thrombotic events during the perioperative phase in orthopaedic surgery is very sensitive.3 Patients with bleeding had a higher risk of in-hospital mortality or readmission than those without; also, surgical bleeding risk increased stepwise with increasing perioperative cardiovascular risks when stratified by updated cardiac risk index.4
Perioperative blood management includes adjuvant therapies and blood transfusions. Blood transfusion is the term used to describe the perioperative delivery of blood and blood products such as autologous blood, allogeneic whole blood, red blood cells, fresh frozen plasma, platelets, and cryoprecipitate. Adjuvant therapy includes drugs and treatments that limit or reduce blood loss so that allogeneic blood transfusions are not necessary.5,6 Systemic side effects from transfusions include allergic reactions, acute lung injury due to transfusions, circulatory overload, graft-versus-host disease, and infections.7–9
In regards to perioperative blood transfusions, there are basically two different schools of thought. These are transfusing at a hemoglobin threshold of 100 g/L (referred to as “liberal”) versus transfusing at a level of 70 g/L or less (referred to as “restrictive protocol”).10,11
Orthopedic operations benefit from innovations that can ensure patient safety while minimizing the need for transfusions.12 Restrictive transfusion policies may lower the need for transfusions and may prevent infections without increasing the likelihood of negative outcomes after major orthopedic surgery, according to moderately strong evidence.13,14
Blood management is one of the facets of an orthopaedic surgical patient’s management that are not directly related to the surgical method but are nevertheless crucial for a successful outcome.15 Age, the kind of fracture, and the hemoglobin (Hb) level upon admission are the key variables influencing perioperative blood transfusion.16
Tranexamic acid is a safe and efficient pharmacological blood preservation medication when treating clinically significant hemorrhage.17
Since the target organ, the bone, has a propensity to bleed profusely and can be difficult to control due to its diffuse nature, increased transfusion rates are required. In addition, most of patients receiving these treatments are often elderly women, who tend to have more cardiovascular co-morbidities, lower hemoglobin levels, and smaller blood volumes than men.18
Accurate blood loss prediction enables risk-based patient counseling, target optimization, and projection of future transfusion needs.19 Patients have been treated before they reach a certain point of decline because intraoperative blood transfusion was linked to an increase in morbidity and mortality.20 Owing to the prevalence of orthopaedic surgical procedures and the paucity of information in the literature, the review’s goal is to review current perioperative blood transfusion methods based on previously published research.
Methods
In accordance with the methodology used for the narrative review, relevant literature was looked up from databases and other sources. To locate recent evidence, the following databases were used: SCOPUS, PubMed, science direct, Google Scholar, Cochrane library, MEDLINE, and embase. By limiting or enlarging the range of potential supporting evidence, medical heading subjects (MeSH) were integrated with proximity operators and Boolean operators like OR, AND, and NOT. Perioperative AND blood AND transfusion, allogenic blood AND adjuvants, pharmacologic AND blood products AND bleeding management, autologous AND allogenic transfusion, anemia OR low hemoglobin level AND indication for blood transfusion, were terms used for searching in different databases. Endnote reference manager was used to remove duplications of extracted literatures from different sources. The review process was conducted in accordance with the preferred reporting items for systematic review and meta-analysis (PRISMA) 202021 (Figure 1). The strength of evidence supporting each conclusion was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach.22
 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed). 2021;372:n71. Creative Commons.21 |
Inclusion and Exclusion Criteria
We have incorporated randomized controlled trials, systematic reviews, meta-analyses, and observational studies on perioperative blood transfusion techniques for orthopaedic surgical patients that are published in English at any time into this narrative review. This review did not include any duplicate research, reports, commentary, full-text papers, brief communications, or letters to the editors.
Results
Identification of Studies
We have identified a total of 31, 174 studies from databases, registers, websites, organizations and citations searching. After removing duplicates, reviewing titles and abstracts, 61 studies were included in this review.
The total number of literatures identified through searching from data-bases and websites were 27,300 and 1,055 respectively. Among these evidences, duplications removed were 2045 and during screening phase with human, 25,625 literatures were excluded. Finally, this narrative review included 61 published papers (Figure 1).
Characteristics of Included Studies
The sample of studies that were part of the current review was displayed in the table below (Table 1).
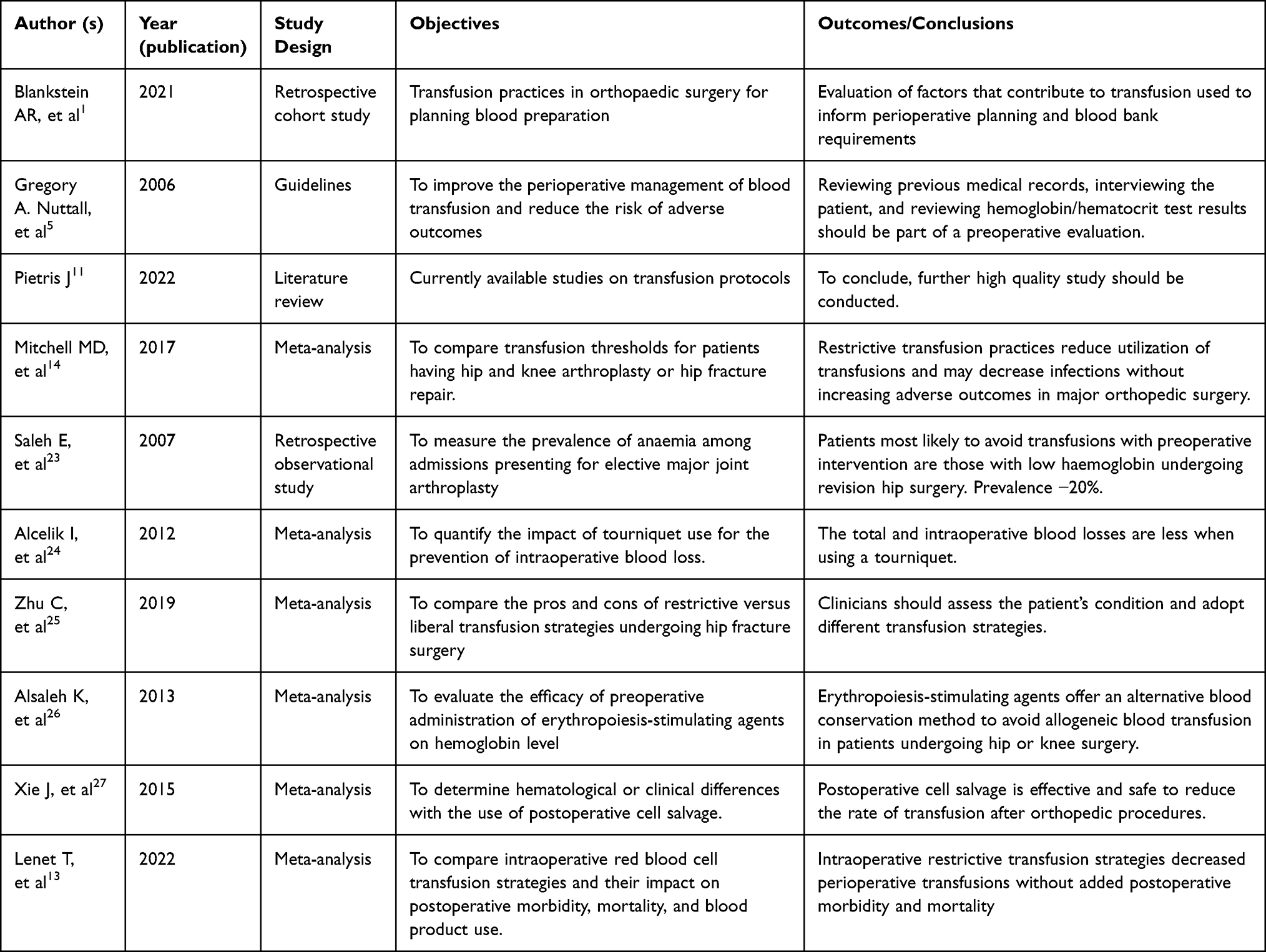 |
Table 1 Summary of Sample Literatures Used in Conclusions |
Discussion
Despite being life-saving, blood transfusions (BT) are linked to morbidity, mortality, and longer hospital stays. The goal of patient blood management (PBM) is to reduce the need for transfusions by utilizing multidisciplinary and multimodal preventive strategies, which will ultimately enhance the clinical results for patients.28
Various rates of transfusion were linked to orthopedic operations. The type of surgery has a big impact on how often red blood cells (RBCs) are transfused. Pre-emptive transfusion mitigation strategies can be facilitated by identifying procedures with the highest transfusion rates and further evaluating the factors that contribute to transfusion in groups that have previously been recognized as at-risk.1 Based on the most recent data, this review reviewed the perioperative blood transfusion strategies for various orthopedic procedures.
Perioperative Blood Transfusion Strategies for Various Orthopedic Procedures
Prior to elective surgery, anemic patients must be identified and treated using strategies that will improve clinical results.29 Age, sex, lower admission Hb level and patients with American Society of Anesthesiologists (ASA) score 3–4 were the factors.30,31 Patients with low preoperative hemoglobin, low body mass index (BMI), or low estimated glomerular filtration rate (eGFR) have significantly higher individual risks for blood transfusions and immediate postoperative problems. Therefore, it has been advised that clinicians optimize patients with a low BMI during the preoperative period, aim for a preoperative Hb 13g/dL and an eGFR 60 mL/min.32
Length of hospital stay (LOS) and post-operative infections were both considerably decreased by intravenous iron therapy (IVIT).33 Hospitals typically manage iron deficiency anemia by administering intravenous iron prior to surgery, tranexamic acid during surgery, and strict transfusion guidelines afterward.34
A restrictive red blood cell (RBC) transfusion technique is therefore preferred to a liberal transfusion strategy (hemoglobin threshold greater than 10 g/dL, typically greater than 8 g/dL), according to a number of studies35 and a meta-analysis of a range of clinical specialties showed that restrictive transfusion decreased the RBC proportion by 43% but did not impact 30-day mortality or morbidity rate.36 According to a meta-analysis, instead of just employing one transfusion technique, healthcare providers should carefully assess each patient’s condition and choose the most appropriate transfusion approach for them.25
Preoperative anemia is prevalent in approximately 20 −25% of the patients undergoing elective total hip replacement surgery.23
Hemoglobin (Hb) concentrations below 12 g /dL in females and 13 g /dL in males are considered anemic by the World Health Organization (WHO). Due to the lower total blood volume in women than in men, a 500 mL blood loss will have a bigger influence on hemoglobin levels, making this female 12 g /Dl threshold insufficient for lowering transfusion risk.37 Therefore, regardless of gender, the conference suggested using the 13 g/ dL criterion. The results of the other study showed that hemodynamic instability or excessive bleeding, not hemoglobin (Hb) level, are the reasons for BT during orthopedic surgery.28 Preoperative anemia has been linked to postoperative problems in several studies.11,12,29,31
Strategies to reduce the need for blood transfusions during surgery have mostly concentrated on decreasing transfusion thresholds. The patient target Hb before elective surgery should be within the normal range (normal female ≥ 120 g/l, normal male ≥ 130 g/l).38 Further investigation into dietary inadequacies, chronic renal failure, and/or chronic inflammatory disorders should be done in the laboratory.39 Erythropoiesis-stimulating agent (ESA) therapy should be utilized for anemic patients in whom nutritional deficiencies have been ruled out and/or repaired in addition to nutritional deficiencies being treated.40
In patients undergoing bilateral hip arthroplasty, a higher preoperative hemoglobin level, the administration of tranexamic acid (TXA), and intraoperative autologous blood transfusion using a closed suction drainage system were protective factors against the need for transfusion.41
Antifibrinolytic drug use has been linked to decreased intraoperative blood loss and postoperative transfusion rates.42
Preoperative autologous blood donation (PABD) patients are more likely to be able to donate blood before surgery while receiving erythropoietin therapy. This has the effect of reducing hemoglobin and hematocrit levels loss.43 According to a study, TXA is a transoperative technique that can help patients having primary total hip arthroplasty avoid the requirement for allogeneic blood transfusions.44
Evidence suggests that preoperative recombinant human erythropoietin (rHuEPO) and iron therapy for anemic adults before non-cardiac surgery reduces the need for RBC transfusion and, when given at higher doses, increases the haemoglobin concentration preoperatively.45
In the era of restrictive transfusion thresholds, the maximum surgical blood order schedules (MSBOS) suggest that preoperative hemoglobin levels (<11 g/dL and <9 g/dL) should be taken into account when determining the number of units to type and crossmatch, respectively, prior to surgery.46
Cell saver (CS) considerably reduces the need for allogeneic blood transfusions (ABT) during and after surgery.47 The use of a tourniquet during total knee arthroplasty (TKA) may reduce intraoperative blood loss safely, but not postoperative blood loss or actual total blood loss.48
A pneumatic tourniquet clear the surgical site from blood, minimizing blood loss and enhancing, in particular, knee replacement and cementing. However, blood stasis can cause neuromuscular dysfunction and thromboembolic consequences, with severity directly correlated with tourniquet time.24 Combined intra-articular and intravenous TXA regimen significantly reduced perioperative blood loss compared with only intravenous (IV) TXA until 7 days after TKA.49
Patients undergoing total knee arthroplasty should follow a protocol that includes regional anesthesia, the use of tourniquets and post-closure deflation, femoral canal plugging or femoral canal sparing surgical techniques, the use of TXA (topically or intravenously), and drain avoidance.50 In total joint arthroplasty (TJA), intraoperative hypothermia is linked to higher rates of blood loss and transfusion. When operating on these individuals, efforts should be taken to maintain normothermia.51
An effective combination of erythropoietin application, iron therapy, intraoperative controlled hypotension for bleeding management, and tranexamic acid administration can produce positive clinical outcomes.52
In Jehovah’s Witness (JW) patients undergoing total knee arthroplasty (TKA), a combination of hypotensive anesthesia, intravenous administration of TXA, intraoperative periarticular injection, and cell salvage appear to be sufficient in controlling the blood loss; however, further tourniquet use may not further reduce the anticipated blood loss.53 The treatment of blood loss is significantly influenced by surgical technique, awareness of the issue, and restrictions on transfusion triggers.54
Preoperative hemoglobin, anesthetic type, use of tranexamic acid, and age were found to be significant predictors of postoperative blood transfusion as per one study.55
In complete hip and knee replacements, postoperative cell salvage is effective and safe in lowering the need for allogenic blood transfusion (ABT).27
We recognise that this study has limitations; it depended on a small number of databases, may have biased the selection of articles, lacked data analysis, and used outdated references. It also did not involve systematic or meta-analysis.
Conclusion and Recommendations
Patients who are at danger of bleeding during surgery or who are anemic should be handled with medication, allogenic blood transfusions, adjuvants, and non-pharmacological methods such tourniquets and cell savers. Most essential, healthcare professionals should pay close attention to patient status during the perioperative phase and use a variety of transfusion procedures rather than relying just on one.
Acknowledgment statement
We appreciate the University of Gondar’s assistance in facilitating our access to published articles via their institutional email account.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Blankstein AR, Houston BL, Fergusson DA, et al. Transfusion in orthopaedic surgery. Bone & Joint Open. 2021;2(10):850–857. doi:10.1302/2633-1462.210.BJO-2021-0077.R1
2. Moldovan F, Moldovan L, Bataga T. A comprehensive research on the prevalence and evolution trend of orthopedic surgeries in Romania. Healthcare. 2023;11(13):1866. doi:10.3390/healthcare11131866
3. Oberweis BS, Nukala S, Rosenberg A, et al. Thrombotic and bleeding complications after orthopedic surgery. Am Heart J. 2013;165(3):427–33.e1. doi:10.1016/j.ahj.2012.11.005
4. Smilowitz NR, Ruetzler K, Berger JS. Perioperative bleeding and outcomes after noncardiac surgery. Am Heart J. 2023;260:26–33. doi:10.1016/j.ahj.2023.02.008
5. Raphael J. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American society of anesthesiologists task force on perioperative blood transfusion and adjuvant therapies. Anesthesiology. 2006;105(1):198–208. doi:10.1097/00000542-200607000-00030
6. Ferraris VA. Practice guidelines for perioperative blood management: an updated report by the American society of anesthesiologists task force on perioperative blood management*. Anesthesiology. 2015;122(2):241–275.
7. Ponnusamy KE, Kim TJ, Khanuja HS. Perioperative blood transfusions in orthopaedic surgery. The Journal of Bone and Joint Surgery American. 2014;96(21):1836–1844.
8. Ramos-Peñafiel CO, Balderas-Delgado C, Cabrera-García Á. Surgery and transfusion. Revista Médica del Hospital Gene de Méx. 2016;79(2):98–106. doi:10.1016/j.hgmx.2015.09.003
9. Taylor RW, Manganaro L, O’Brien J, Trottier SJ, Parkar N, Veremakis C. Impact of allogenic packed red blood cell transfusion on nosocomial infection rates in the critically ill patient. Crit Care Med. 2002;30(10):2249–2254. doi:10.1097/00003246-200210000-00012
10. Birlie Chekol W, Teshome M, Nigatu YA, Melesse DY. Hemoglobin threshold and clinical predictors for perioperative blood transfusion in elective surgery: systemic review. Trends Anaesth Crit Care. 2020;31:8–15. doi:10.1016/j.tacc.2019.12.003
11. Pietris J. The effect of perioperative blood transfusion thresholds on patient outcomes in orthopaedic surgery: a literature review. ANZ J Surg. 2022;92(4):661–665. doi:10.1111/ans.17560
12. Pennestrì F, Maffulli N, Sirtori P, et al. Blood management in fast-track orthopedic surgery: an evidence-based narrative review. J Orthopaedic Surg Res. 2019;14(1):263. doi:10.1186/s13018-019-1296-5
13. Lenet T, Baker L, Park L, et al. A systematic review and meta-analysis of randomized controlled trials comparing intraoperative red blood cell transfusion strategies. Annals of Surgery. 2022;275(3):456–466. doi:10.1097/SLA.0000000000004931
14. Mitchell MD, Betesh JS, Ahn J, Hume EL, Mehta S, Umscheid CA. Transfusion thresholds for major orthopedic surgery: a systematic review and meta-analysis. The Journal of Arthroplasty. 2017;32(12):3815–3821. doi:10.1016/j.arth.2017.06.054
15. L R. Strategies for blood management in orthopaedic and trauma surgery. J Bone Joint Surg Br. 2008;90:1.
16. Dai CQ, Wang LH, Zhu YQ, et al. Risk factors of perioperative blood transfusion in elderly patients with femoral intertrochanteric fracture. Medicine. 2020;99(15):e19726. doi:10.1097/MD.0000000000019726
17. Wong J, George RB, Hanley CM, Saliba C, Yee DA, Jerath A. Tranexamic acid: current use in obstetrics, major orthopedic, and trauma surgery. Canadian Journal of Anaesthesia = Journal Canadien D’anesthesie. 2021;68(6):894–917. doi:10.1007/s12630-021-01967-7
18. Müller S, Oberle D, Drechsel-Bäuerle U, Pavel J, Keller-Stanislawski B, Mortality FMB. Morbidity and related outcomes following perioperative blood transfusion in patients with major orthopaedic surgery: a systematic review. Transfus med hemo. 2018;45(5):355–367. doi:10.1159/000481994
19. Donovan RL, Lostis E, Jones I, Whitehouse MR. Estimation of blood volume and blood loss in primary total Hip and knee replacement: an analysis of formulae for perioperative calculations and their ability to predict length of stay and blood transfusion requirements. J thop. 2021;24:227–232. doi:10.1016/j.jor.2021.03.004
20. Gupta P, Kang KK, Pasternack JB, Klein E, Feierman DE. Perioperative transfusion associated with increased morbidity and mortality in geriatric patients undergoing hip fracture surgery. Geriatric Orthopc Surg amp. 2021;12:21514593211015118. doi:10.1177/21514593211015118
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
22. Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490.
23. Saleh E, McClelland DBL, Hay A, Semple D, Walsh TS. Prevalence of anaemia before major joint arthroplasty and the potential impact of preoperative investigation and correction on perioperative blood transfusions. BJA: British Journal of Anaesthesia. 2007;99(6):801–808. doi:10.1093/bja/aem299
24. Alcelik I, Pollock RD, Sukeik M, Bettany-Saltikov J, Armstrong PM, Fismer P. A comparison of outcomes with and without a tourniquet in total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. J Arthroplasty. 2012;27(3):331–340. doi:10.1016/j.arth.2011.04.046
25. Zhu C, Yin J, Wang B, et al. Restrictive versus liberal strategy for red blood-cell transfusion in Hip fracture patients: a systematic review and meta-analysis. Medicine. 2019;98(32):e16795. doi:10.1097/MD.0000000000016795
26. Alsaleh K, Alotaibi GS, Almodaimegh HS, Aleem AA, Kouroukis CT. The use of preoperative erythropoiesis-stimulating agents (ESAs) in patients who underwent knee or Hip arthroplasty: a meta-analysis of randomized clinical trials. J Arthroplasty. 2013;28(9):1463–1472. doi:10.1016/j.arth.2013.01.024
27. Xie J, Feng X, Ma J, et al. Is postoperative cell salvage necessary in total Hip or knee replacement? A meta-analysis of randomized controlled trials. International Journal of Surgery. 2015;21:135–144. doi:10.1016/j.ijsu.2015.07.700
28. Inbar T, Dann EJ. Preoperative anemia and blood transfusion requirement during hip surgery: synthetic and real patient cohort data. Blood. 2019;134(Supplement_1):3693. doi:10.1182/blood-2019-125252
29. Duarte GC, Catanoce AP, Zabeu JL, et al. Association of preoperative anemia and increased risk of blood transfusion and length of hospital stay in adults undergoing Hip and knee arthroplasty: an observational study in a single tertiary center. Health Sci Rep. 2021;4(4):e448. doi:10.1002/hsr2.448
30. Grandone E, Mastroianno M, De Laurenzo A, et al. Mortality and clinical outcome of Italian patients undergoing orthopaedic surgery: effect of peri-operative blood transfusion. Blood Transfusion = Trasfusione Del Sangue. 2021;19(4):284–291. doi:10.2450/2020.0059-20
31. To J, Sinha R, Kim SW, et al. Predicting perioperative transfusion in elective hip and knee arthroplasty: a validated predictive model. Anesthesiology. 2017;127(2):317–325. doi:10.1097/ALN.0000000000001709
32. Jakuscheit A, Schaefer N, Roedig J, Luedemann M. Modifiable individual risks of perioperative blood transfusions and acute postoperative complications in total hip and knee arthroplasty. J Person Med. 2021;11(11). doi:10.3390/jpm11111223
33. Shin HW, Park JJ, Kim HJ, You HS, Choi SU, Lee MJ. Efficacy of perioperative intravenous iron therapy for transfusion in orthopedic surgery: a systematic review and meta-analysis. PLoS One. 2019;14(5):e0215427. doi:10.1371/journal.pone.0215427
34. Lu Q, Peng H, Zhou GJ, Yin D. Perioperative blood management strategies for total knee arthroplasty. Orthopaedic Surgery. 2018;10(1):8–16. doi:10.1111/os.12361
35. Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012;4(4):1.
36. Carson JL, Stanworth SJ, Roubinian N, et al. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2016;10(10):Cd002042. doi:10.1002/14651858.CD002042.pub4
37. Butcher A, Richards T, Stanworth SJ, Klein AA. Diagnostic criteria for pre-operative anaemia-time to end sex discrimination. Anaesthesia. 2017;72(7):811–814. doi:10.1111/anae.13877
38. Munting KE, Klein AA. Optimisation of pre-operative anaemia in patients before elective major surgery - why, who, when and how? Anaesthesia. 2019;74(Suppl 1):49–57. doi:10.1111/anae.14466
39. Melesse DY, Chekol WB. The management of patients with coronavirus disease 2019 in intensive care unit (ICU) in low income countries: a review article. Clinical Nutrition Open Science. 2021;37:60–72. doi:10.1016/j.nutos.2021.05.001
40. Kendoff D, Tomeczkowski J, Fritze J, Gombotz H, von Heymann C. Preoperative anemia in orthopedic surgery: clinical impact, diagnostics and treatment. Der Orthopade. 2011;40(11):1018–20, 23–5, 27–8. doi:10.1007/s00132-011-1789-3
41. Wang X, Huang Q, Pei F. Incidence and risk factors for blood transfusion in simultaneous bilateral total Hip arthroplasty. Joint Diseases and Related Surgery. 2021;32(3):590–597. doi:10.52312/jdrs.2021.333
42. Stoicea N, Bergese SD, Ackermann W, et al. Current status of blood transfusion and antifibrinolytic therapy in orthopedic surgeries. Frontiers in Surgery. 2015;2:3. doi:10.3389/fsurg.2015.00003
43. Chang X, Li Q, Tang H. Use of preoperative erythropoietin therapy to facilitate autologous blood donation in orthopedic surgery: a meta-analysis. Medicine. 2020;99(2):1.
44. García-Dobarganes-Barlow FE, Romo-Aguilera IJ, Negrete-Corona J, Guevara Álvarez A, Garcini-Munguía FA, Téllez-Hoyos S. Effectiveness of tranexamic acid for decreased allogenic blood transfusion in total Hip arthroplasty. Acta ortopedica mexicana. 2020;34(1):6–9.
45. Kaufner L, von Heymann C, Henkelmann A, et al. Erythropoietin plus iron versus control treatment including placebo or iron for preoperative anaemic adults undergoing non-cardiac surgery. Cochrane Database Syst Rev. 2020;8(8):Cd012451. doi:10.1002/14651858.CD012451.pub2
46. Amin RM, Puvanesarajah V, Chaudhry YP, et al. Reducing unnecessary crossmatching for Hip fracture patients by accounting for preoperative hemoglobin concentration. World Journal of Orthopedics. 2021;12(5):292–300. doi:10.5312/wjo.v12.i5.292
47. Duramaz A, Bilgili MG, Bayram B, et al. The role of intraoperative cell salvage system on blood management in major orthopedic surgeries: a cost–benefit analysis. Eurn J of Orthop Surg and Traumatol. 2018;28(5):991–997. doi:10.1007/s00590-017-2098-2
48. Li X, Yin L, Chen Z-Y, et al. The effect of tourniquet use in total knee arthroplasty: grading the evidence through an updated meta-analysis of randomized, controlled trials. Eurn J of Orthop Surg and Traumatol. 2014;24(6):973–986. doi:10.1007/s00590-013-1278-y
49. Iseki T, Tsukada S, Wakui M, Yoshiya S. Intravenous tranexamic acid only versus combined intravenous and intra-articular tranexamic acid for perioperative blood loss in patients undergoing total knee arthroplasty. Eurn J of Orthop Surg and Traumatol. 2018;28(7):1397–1402. doi:10.1007/s00590-018-2210-2
50. Soranoglou V, Poultsides LA, Triantafyllopoulos GK, De Martino I, Memtsoudis SG, Sculco TP. Optimizing intraoperative blood management for one-stage bilateral total Knee arthroplasty. HSS Journal: the Musculoskeletal Journal of Hospital for Special Surgery. 2018;14(2):202–210. doi:10.1007/s11420-017-9590-4
51. Pan P, Song K, Yao Y, Jiang T, Jiang Q. The impact of intraoperative hypothermia on blood loss and allogenic blood transfusion in total knee and hip arthroplasty: a retrospective study. Bio Med ResIntern. 2020;2020:1096743. doi:10.1155/2020/1096743
52. Yuan M, Ding Z, Ling T, Zhou Z. Perioperative blood management for total Hip/knee arthroplasty]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi = Zhongguo xiufu chongjian waike zazhi =. Chinese Journal of Reparative and Reconstructive Surgery. 2020;34(12):1612–1618. doi:10.7507/1002-1892.202002162
53. Levent A. Does tourniquet use decrease blood loss following primary total knee arthroplasty in Jehovah’s Witness patients? Joint Diseases and Related Surgery. 2020;31(3):419–425. doi:10.5606/ehc.2020.76244
54. Moonen AFCM, Neal TD, Pilot P. Peri-operative blood management in elective orthopaedic surgery. A critical review of the literature. Injury. 2006;37:S11–S6. doi:10.1016/S0020-1383(07)70006-2
55. Bian FC, Cheng XK, An YS. Preoperative risk factors for postoperative blood transfusion after Hip fracture surgery: establishment of a nomogram. J Orthop Surg Res. 2021;16(1):406. doi:10.1186/s13018-021-02557-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.