")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 14
Perceptions of the Intervention Utility and Effectiveness in Supporting and Reintegrating Youths Born of Genocidal Rape in Rwanda
Authors Nyirandamutsa F, Niyonsenga J , Gaju KL, Izabayo J, Kambibi E, Munderere S, Sebuhoro C, Muhayisa A, Sezibera V
Received 13 March 2023
Accepted for publication 8 September 2023
Published 12 September 2023 Volume 2023:14 Pages 141—151
DOI https://doi.org/10.2147/AHMT.S412300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Haiyan Qu
Fortunée Nyirandamutsa,1 Japhet Niyonsenga,1,2 Kethina Lisette Gaju,3 Josias Izabayo,4 Emilienne Kambibi,5 Samuel Munderere,5 Célestin Sebuhoro,1 Assumpta Muhayisa,1 Vincent Sezibera1,4
1Department of Clinical Psychology, University of Rwanda, Kigali, Rwanda; 2Department of Humanities and Social Sciences, University of Parma, Parma, Italy; 3Global Mental Health MSc Program, King’s College London and London School of Hygiene and Tropical Medicine, London, UK; 4Centre for Mental Health, University of Rwanda, Kigali, Rwanda; 5Department of Mental Health, Survivors Fund Rwanda, Kigali, Rwanda
Correspondence: Fortunée Nyirandamutsa; Japhet Niyonsenga, Tel +250784010477, Email [email protected]; [email protected]
Background: Birth through genocidal rape has a detrimental impact on the health of the offspring; however, there is scarce literature that focuses on efforts to support and reintegrate people born of this crime due to the lack of needs assessments that can inform policies and interventions.
Objective: This study sought to explore perceptions of the intervention utility and effectiveness in supporting and reintegrating offspring born of the 1994 genocidal rape against the Tutsi in Rwanda.
Methods: A purposive sample of 16 dyads of non-partnered mothers raped in the 1994 genocide against the Tutsi and their offspring participated in semi-structured qualitative interviews. The transcribed interview verbatims were uploaded to NVivo 12 and analyzed inductively using thematic analysis.
Results: The analysis resulted in several subthemes that were grouped into four main themes based on research questions. These themes included the reconstruction of a positive image (ie, hardworking, contribution to the community, supporting vulnerable people, etc.), the benefits of collaborating with peers in a similar situation (ie, a sense of belonging, self-acceptance, relieving distress and emotional pain, etc.), the support obtained from Survivors Fund Rwanda (ie, psychosocial support, financial support for school fees, support to get a job), and the intervention and strategies needed (ie, continuous psychosocial support, catch-up learning programs, accompaniment support, advocacy to get a job, supporting the parents, etc.).
Conclusion: Our results highlight how the youth born of genocidal rape are reconstructing a positive image and self-advocacy, their perception of obtained support, and the recommended intervention. These findings will help in initiating or strengthening interventions targeting this population, especially strategies to support and reintegrate them.
Plain Language Summary: The current study was conducted to explore the perceptions of intervention utility and effectiveness in supporting and reintegrating offspring born of the 1994 genocidal rape against the Tutsi in Rwanda, which can inform policies and interventions. To achieve this, a purposive sample of 16 dyads of non-partnered mothers raped in the 1994 genocide against the Tutsi and their offspring were selected to participate in semi-structured qualitative interviews. Our analysis resulted in several subthemes that were grouped into four main themes based on research questions. These themes that emerged included the reconstruction of a positive image and self-advocacy, the benefits of collaborating with peers in a similar situation, the support obtained, and the intervention and strategies needed. These findings will help in initiating or strengthening interventions targeting people born of genocidal rape, especially strategies to support and reintegrate them.
Keywords: genocidal rape, born of genocidal rape, needs assessment, intervention utilities, Rwanda, adolescent
Introduction
During the 1994 genocide against the Tutsi, rape was utilized as a weapon of war/genocide to violate and terrorize individual victims as well as cleanse the wider groups to which victims belonged.1,2 It is estimated that between 10,000 and 25,000 offspring were born as a result of genocidal rape in Rwanda.2 Being born from rape by genocide perpetrators exacerbates further difficulties, including rejection by society globally and the community of survivors, particularly in patriarchal settings like Rwanda.2 Offspring may have “the ethnic identities of two groups, but in a patriarchal society, children get their father’s ethnicity.1 This is why it is problematic for them to accept the attribution of Interahamwe, a Rwandan army group that planned and executed the genocide.1 The children represent a source of dispute among Rwandan families because they are commonly seen as a reminder of the genocide’s cruelty and suffering, as well as a hindrance to collective healing and communal harmony.2–4
The offspring are particularly dealing with identity and belonging, times of “truth-telling” about their origins, the pain of their mother’s trauma, internalized and externalized stigmatization, and abuse and abandonment, which may lead to life-long effects.1,5–7 They are frequently neglected or physically abused within the family, especially when they have stepfathers.3,6,8 Worryingly, children’s behaviors and identities were commonly linked to their fathers within their families and communities, leading to feelings of shame and rejection.1,8 The inability to prove their father’s name at school also led to bullying from other youngsters.1 The humiliation and stigma they faced might have led to feelings of worthlessness and despair, which, along with the questioning about their paternity and stigmatization, contributed to mental health issues as they got older and attended school.8 To deal with their challenging condition, some turned to substance abuse or sex work to act out their suffering.3,4,8,9
Though these offspring are a vulnerable population with a greater risk of experiencing stigma, mental disorders, substance abuse, and poor academic performance,1,5–7 many studies have generally focused on lived and mothering experiences,2,4,9–16 and mothers’ needs and intervention.3,17 Few studies of children have emphasised children’s challenges and psychosocial problems,11,18–21, experience of disclosure,22 and children’s needs.23 A study by Hogwood et al,22 primarily aimed at exploring how young people experienced the disclosure and how this affected their sense of identity revealed that the supported disclosure helped children to understand more fully themselves, their identity, and parentage, and to answer questions about their absent or unknown fathers and the way they had been treated in their families and the community. However, it also resulted in unpleasant feelings and terrible self-images, leading some of them to ponder suicide.22 Moreover, in a recent review of “What do we know about the children’s experiences and needs”, the authors identified four themes, such as “birth origin stories associated with the crime of the father; the fractured sense of belonging; the intergenerational legacy of trauma and family identity; and strategies to move forward, including knowing the truth about one’s origin, mental health, and peer support”.23
The review has highlighted a scarcity of studies documenting the needs of the children from their own perspective.23 This study, therefore, aimed to investigate perceptions of intervention utility and effectiveness in supporting and reintegrating the youth born of the 1994 genocide against the Tutsi. The study is also expected to identify discrepancies between needs and interventions and, therefore, describe other interventions needed from the youth’s point of view and perspectives. Currently, the Survivors Fund in Rwanda (SURF) is “assisting mothers who have children born of genocidal rape by offering psychosocial assistance, income generating opportunities, and educational support for their children”.22 SURF has established a network of community counselling groups around the nation to provide women with a safe space to chat with others in similar circumstances and consider how to answer their children’s inquiries.22 We found it imperative to explore the perceived utility and effectiveness of this intervention as well as the offspring’s needs. By conducting this study, we contribute to the scientific community and organizations working with youth born of genocidal rape in Rwanda, ‘a post-genocide country,’ and similar settings by initiating or strengthening effective intervention strategies.
Method
Study Design
The qualitative design of the current study involved individual semi-structured interviews rather than focus group discussions because the topic was very sensitive and highly personal. The respondents, therefore, might not be comfortable discussing the topic in front of people, or the discussion could lead to an emotional breakdown.
Participants
The present study included 16 offspring born of the 1994 genocidal rape against the Tutsi and their mothers. The respondents were the beneficiaries of the Survivors Fund Rwanda (SURF), a non-governmental organization supporting this population.24 Children were the primary focus of this study, but we found it relevant to include mothers for response validity purposes. We assumed that there would be a spillover effect on mothers when the offspring perceived the intervention utility and effectiveness. The inclusion criteria were (i) being or having a last-born offspring conceived from genocidal rape, and (ii) being single for offspring and having never been partnered since the rape for mothers because the needs of non-partnered individuals may differ from those who are partnered. The last might have experienced intimate partner violence or child abuse that would worsen their situation or otherwise received social support that would ameliorate it.1 The participants were excluded from the study if they had serious physical or mental illnesses that would impair their decision to participate. Women who were raped and regularly gave birth were excluded from this study because they were found to face additional social stigma in their community.3
A purposive sampling strategy25 was used to include mothers and their children in the current study. Even though the final sample size depended on the saturation of information, 34 participants were initially selected. A SURF counsellor who works with this population sent a letter to the eligible beneficiaries to invite them to participate in the interview. Seven days later, the counsellor called mothers and their offspring to determine their willingness to participate and to clarify any questions.
Data Collection
Before data collection, ethical approval was obtained from the Institutional Review Board (IRB) of the University of Rwanda, College of Medicine and Health Sciences (No. 174/CMHS IRB/2021). Participants who were invited to the SURF office provided both verbal and written consent. Two researchers, who were unknown to the participants, conducted face-to-face semi-structured interviews with 32 individuals with the help of a topic guide with predetermined questions (Box 1). As shown in Box 1, the same questions posed to offspring were paraphrased and posed to mothers too (a sample question is provided). During the interviews, an audiotape and field notes were used for data collection. The interview session lasted 30–40 minutes and was conducted separately for both mothers and offspring in individual counselling rooms. Participants had access to psychosocial support networks because the interviews might cause them to feel psychological distress again. Moreover, the research team, including a SURF psychologist, followed up with the participants after the interviews to see how they were doing.
 |
Box 1 Thematic Guide for Individual Interviews |
Data Analysis
The interviews were verbatim transcribed, but any identifiable details of the participants were eliminated. The interviews were transcribed and analyzed using codebook thematic analysis26 in Kinyarwanda and later translated into English. This choice was made because meaning would easily be lost in translation and the validity of the data may be compromised in this process.27 Thematic analysis was chosen since each interview consisted of the same set of questions for each participant, resulting in different replies to the same questions. The approach explores the participants’ perceptions, feelings, and lived experiences. It seeks to find meaning in events and interactions, clarifying how they make sense of the experiences.
Thereafter, the transcribed verbatims were uploaded to the NVivo 12 software to begin the process of inductively creating the initial codes from raw data.28 The coding process involved three researchers with a background in clinical psychology (the Fleiss kappa=0.802) and the discrepancies were resolved by discussion. Patterns were discovered by evaluating similarities and consolidating developing themes into bigger units, considering the frequency of the subjects and their purpose in the transcripts that led to subordinate themes. The same processes were used for the second and subsequent transcripts. Following the analysis, the themes and sub-themes were translated into English to obtain agreement on a better language.
Findings
Sociodemographic Characteristics
Participants in this study were 16 mother-child dyads (Table 1). The respondents came from all provinces of Rwanda, with a high proportion from the southern province (13/32), Kigali city (11/32) and western province (5/32). Most of the offspring were male (9/16) and all participants were non-partnered (32/32). Regarding age, the mean age for mothers was 55.5 years (SD=4.05) and all offspring were age 28 years old. For education, 7/16 of offspring completed university (7/16), TVET (Technical and Vocational Education and Training) school (3/16), and secondary school (5/16), whereas many mothers completed primary school (9/16), and TVET (5/16). All offspring had no child and most mothers had one child (9/16).
 |
Table 1 Sociodemographic Characteristics |
Thematic Analysis
As demonstrated in Table 2, the thematic analysis resulted in several subthemes that were grouped into four main themes based on research questions. These themes that emerged from the analysis included rebuilding a positive image and self-advocacy, benefits of collaborating with peers in a similar situation, support obtained from SURF, and the intervention and strategies needed.
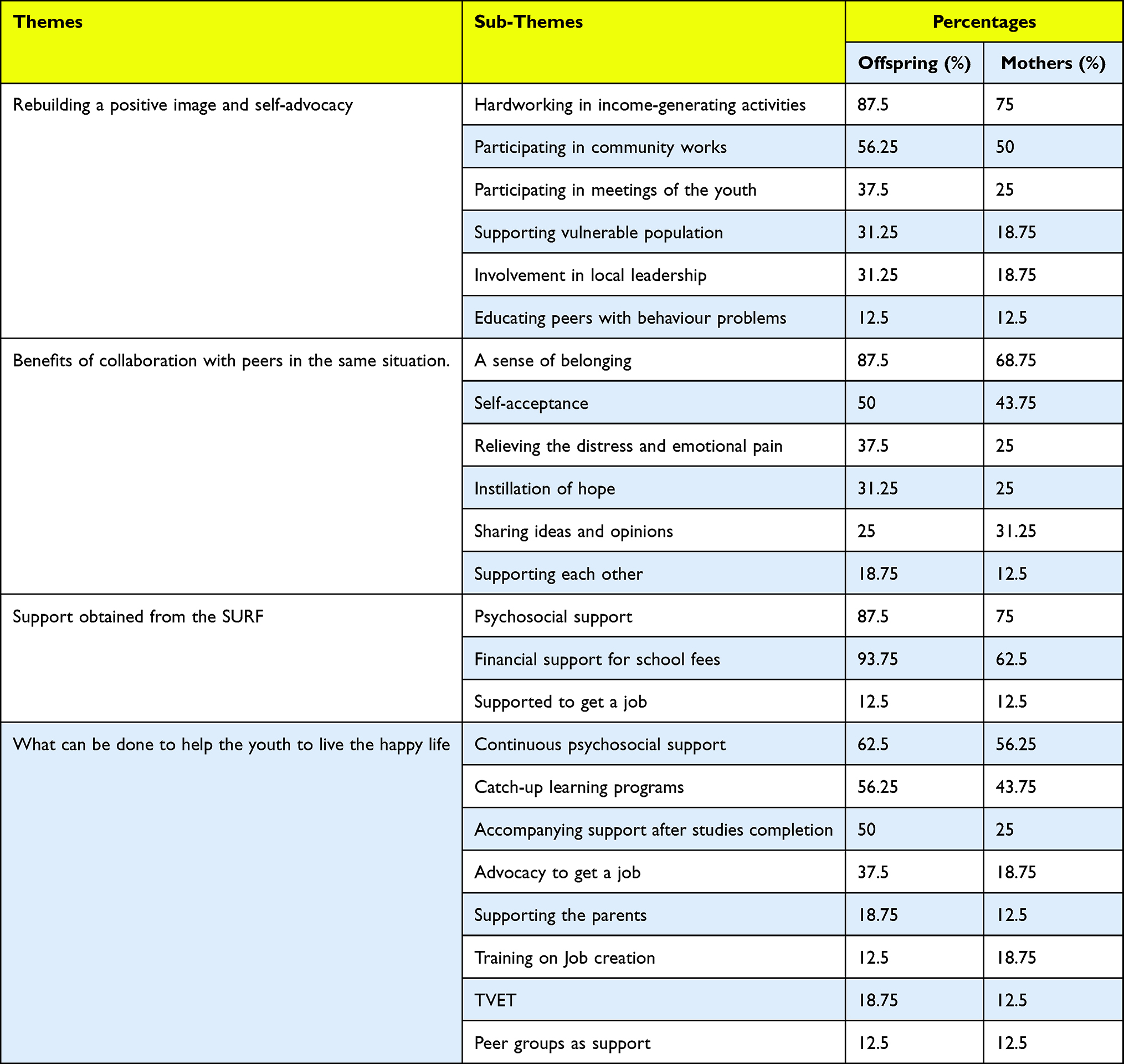 |
Table 2 Summary of the Themes and Sub-Themes |
Rebuilding a Positive Image and Self-Advocacy
Aiming at reconstructing a positive image and self-advocacy, the offspring have an eagerness to work hard, and they engage in many activities generating income, including but not limited to livestock farming (pigs, goats, and cows), saving groups known as Ibimina, TVET, small trading businesses, education and handcraft.
After learning that I was born from the rape suffered by my mother during the Tutsi genocide, I understood that I had to find a way to take care of my life as quickly as possible. This is why I attended a driving school to be able to find a job as soon as possible. I got a driving license and I have a permanent job as a driver, and I can assist my mother or others financially. In addition to that, I am now working as a teacher in driving school… A child born of rape (BR)-6.
After realizing how my mom always took care of me while she is a single and poor mother, I decided to find out how I can help her because I saw her tired. This is how I decided to do the embroidery and marketing training. With this training, I can satisfy my financial needs, those of my mother without forgetting the assistance that I bring to the poorest who need my support… BR-3.
As confirmed by their mothers, children born of genocidal rape have also attempted to build positive identities for themselves by participating in community work, participating in youth meetings, supporting vulnerable populations, participating in local leadership and educating peers with behavior problems.
Being born of the rape committed during the genocide does not stop me from having a patriotic spirit or fulfilling my obligations as a Rwandan citizen. I participate in community works with others and I join groups of young volunteers determined to do different activities needed by vulnerable people in our community. I feel useful and I like being valuable to others without any distinction…BR-13.
I always participate in community work, and I join others in different activities to support the poorest and most vulnerable people in our community. I am a member of a group of volunteers, and I am among the young people who took the first step as Youth Volunteers to prevent the Covid-19 Pandemic. Often, I congratulate myself on the fact that I am not afraid to take the risk of joining others when we must help people in need… BR- 15.
Like other people of my age, I participate in useful works for the community, and I am among the leaders in the choir of my church. Also, I took the initiative to raise awareness among young people in my neighborhood to fight against substance abuse. To continue to be useful in my community, I make free interventions in the field of information and communications technology. Often, I feel happy that I am on a good way of resilience and to see that my birth conditions do not prevent me from being useful to my community… BR-5.
However, few mothers reported that their offspring did not care about anything as they were still dependent on their mothers. We realized that a few offspring may try to deal with their problems by abusing alcohol probably as self-medication:
My child is behaving strangely, and she is not able to resolve any of her financial problems. She is often fired from her job because she is unable to perform her tasks and she is never serious about what she does. And even when she finds a job for a few days, she wastes all the money she has earned on alcohol or other unimportant things. I take care of all her needs; she still depends on me now while I am a single and poor mother! … Raped mother (RM)-1.
Benefits of Meeting with Peers in a Similar Situation
The analysis indicated that meeting with their peers in similar situations provided the offspring with a sense of belonging and self-acceptance, relieving distress and emotional pain, instilling hope, sharing ideas and opinions, and supporting each other. Here are the verbatims:
Being with my peers in the same situation is the best thing in my life. It shows me that I’m not the only one to suffer from the birth story and I feel relieved from my pain. When I am with them, I feel inner joy and peace because we all talk to each other freely. Their presence and interaction between us facilitate my steps towards resilience… BR-3
I feel filled with joy only when I am with my peers, with whom we share the same life history. When I am with them, I feel free from any burden because I share with them a lot of things concerning our lives in general and more particularly the story related to our birth conditions. With them, I share so many things without fear of being judged or criticized because the modalities of our lives are almost the same… BR-4
I like being with my peers who have the same life story as me because it allows us to talk easily about our future. When we are together, I feel happy because our dialogues are often about how to help each other but also how we can help our mothers to overcome their difficulties. Spending time with them reinforces in me the spirit of reconnection with them, but also it stimulates my sense of reconstruction for a better future… BR-5
The presence of my peers who have the same story as mine is the only thing that alleviates the distress that I often face in my life. With them, I sense a need for rebuilding for a better future and a sense of reconnection. Even if I was not able to complete my secondary studies, I managed to get a driving license and this thanks to our meetings and constructive dialogues… BR-6
Support Obtained from SURF Rwanda
One of the major forms of support that the offspring reported were psychosocial support (ie, individual, family, and group counselling by SURF), financial support for school fees, and support to get a job. Here are the verbatims quotes from the respondents:
There were times when my life was in total confusion because of family conflicts related to my birth conditions. My physical and mental living conditions were so bad that I had to go for consultations with mental health services. But with the psycho-social support from SURF, I was able to take control of my life. I was able to benefit from individual counselling, family counselling and group counselling with my peers. For the moment I feel a remarkable improvement and I have good results in the courses that I am following… BR-12.
For me, SURF is like a second parent because I don’t know what I would have become without their assistance. With this organization, I was able to do my studies because they supported my mother in getting my school fees up to the university. Their social assistance, counselling sessions and different pieces of training allowed me to overcome various difficulties in life and solve most of my financial problems. I thank them a lot because they made me who I am today, and they do everything like people who care about us… BR-3.
If I can be productive and useful to my community, I owe it to SURF because they took the initiative to play the role that should have been played by my father. They supported my mother to pay my school fees and I was even able to go to university. With their psycho-social support and various pieces of training, I was able to acquire different knowledge and I manage quite well. Also, SURF assisted me to find a job and I am now able to resolve my financial needs and to help others… BR-5.
Intervention and Strategies to Support and Reintegrate Offspring Born of Genocidal Rape
The analysis of the verbatims of the respondents indicated that the highly recommended intervention and strategies were continuous psychosocial support, catch-up learning programs, accompanying support, advocacy to get a job, supporting the parents, training on job creation, TVET and peer groups as support.
We are very happy for all kinds of assistance from SURF, and we will be always thankful to them. However, we still need their support to be able to become self-employed. Also, the continuation of psycho-Social Support is still needed, as many of us are continuing to experience some psycho-social problems. On my side, I would like to ask for a continuation of assistance to my mother because, in addition to the poverty, she also has one leg as she has been injured and lost her other leg during the genocide… BR-13.
I am very thankful to SURF because they assisted my mother in different ways for many years until now. For now, my wish is to have a continuation of assistance to finish university at A0 Level. Personally, individual and group counselling /psychotherapy is still needed to recover from trauma and fight against bad dreams that often happen to me…! If possible, being supported to start my own business as a Barista should be the best way which can allow me to obtain many positive changes for a better and happy life… BR- 14.
As a single and poor mother, I have always believed that our life will be better when my daughter finishes her studies because she will have a job with a good salary. I decided to never get married or to have another child to take care of her and contribute to her education. But even though she finished her university studies, she has not yet found a job. It’s really disturbing to think that I’m the one in charge of all her financial needs because she’s not yet financially stable. RM-2.
Discussion
To the best of our knowledge, this is the first study to explore the perceptions of intervention utility and effectiveness in supporting and reintegrating the youth born of rape during the 1994 genocide against the Tutsi. The study also identified discrepancies between needs and interventions and therefore described other interventions needed from the youth’s point of view and perspectives. Consistently, a recent review has indicated a scarcity of studies documenting the needs of the children from their own perspective.23 Youth born of rape in wartime were generally found to experience high stigma, mental disorders, substance abuse, and poor academic performance,1,5–7 but few studies have been conducted in the Rwandan context.23 Many studies have generally focused on lived and mothering experiences,2,4,9–16 and mothers’ needs and intervention.3,17
Few studies of children born of rape have emphasized the children’s challenges and psychosocial problems,11,18–21, the experience of disclosure22 and the children’s needs.23 The current study adds to the literature the needs and the perceptions of intervention utility and effectiveness in the adult offspring born of genocidal rape. As individuals born of this crime grow from childhood, adolescence to adulthood, there is a constant need to continue evaluating the needs and intervention utility and effectiveness. The key themes that emerged from the current study were rebuilding a positive image and self-advocacy, the benefits of meeting with peers in a similar situation, self-empowerment socio-economically, support obtained, and the intervention and strategies needed for continuous reintegration. The study findings highlighted that addressing one facet of the hardships experienced by children born of genocidal rape is insufficient; further attempts must address the wide range of issues they confront. Consistently, scholars have revealed that generic post-war psychosocial or reconciliation programs for traumatized communities are insufficient to address the marginalization of this specific population of children and their mothers.7,8 Efforts to support and reintegrate the offspring born of genocidal rape need the collaboration of intrapersonal, interpersonal, and societal paths.8
Our findings indicated that the youth were supported by the Survivors Fund (SURF) through the provision of individual, family and group psychotherapy as well as education. This initiative is in congruence with the recommendations of prior studies stressing a need for individual and group therapy among these offspring and their mothers.8 The SURF has established a network of community counselling groups around the nation to provide women with a safe space to chat with others in similar circumstances and consider how to answer their children’s inquiries including birth histories disclosure.22 In a study by Hogwood et al22 that primarily aimed to explore how young people experienced the disclosure and how this affected their sense of identity, the respondents testified to the benefits of the disclosure including fully understanding themselves, their identity, and parentage, and answers to questions about their fathers, and the way they had been treated in their families and the community. However, it also creates painful feelings and unfavorable self-images, leading some of them to contemplate suicide22 (but this was not the case for this study), which led to the idea of creating another group of these children by the SURF where they meet with others in a similar situation.
In this study, most of the interviewed offspring testified that they are benefiting from meeting with their peers in similar situations by providing them with a sense of belonging and self-acceptance, relieving distress and emotional pain, instilling hope, sharing ideas and opinions, and supporting each other. In congruence with our findings, several authors, despite the lack of empirical evidence, have suggested that meeting others in a similar situation may be very useful for youth born of genocidal rape since many assumed they were the only ones suffering from this condition.1,7,8,22,23 Similarly, Hogwood et al22 have suggested that interacting with and getting support from people in similar circumstances is a crucial approach for Rwandan youth to rebuild a positive identity.
Our analysis indicated that youth born of rape are working tirelessly to reconstruct a positive image and self-advocacy through participating in community work and youth meetings and supporting vulnerable populations etc. The same strategy was found in Uganda, where the children born of rape in wartime revealed how they overcome difficulties and challenged stigmatizing preconceptions via “useful activities such as education, working hard, and contributing to their communities”.29 In Rwanda, several genocide rape survivors made intentional efforts to avoid ethnic categorization, maintaining that they were “Rwandan” or “created in God’s image”3 and eager to play a central role in post-genocide reconciliation.8
Another unique and important theme that emerged from this study was the needed intervention and strategies which come with subthemes, including continuous psychosocial support by SURF, catch-up learning programs, accompanying support after studies completion, advocacy to get a job, supporting the parents, training on job creation, TVET and peer groups as support. These findings are in congruence with the previous studies suggesting that individual and group therapy among genocidal rape offspring and their mothers is a vital first step before economic support can prove useful.7,8 This study adds to the literature other recommendations that are crucial for the reintegration of the youth born of genocidal rape.
Study Strength and Limitation
The main strengths of this study were its inclusion of offspring born of genocidal rape and their mothers for response validity and a very low non-response rate. However, this study had some limitations. First, the inclusion of only non-partnered offspring and mothers limits the generalizability of our findings to those who were partnered. As such, future research is recommended to look at married mothers and compare them. Second, the sample may be overrepresented by “socioeconomically marginalized” mothers and their offspring since they were beneficiaries of SURF Rwanda. Therefore, there might be fewer perspectives from those from the “more privileged social class”. Therefore, future studies replicating this study in individuals from the high class and partnered offspring born of the genocidal rape are recommended.
Conclusion
Our findings highlight how the youth born of genocidal rape are striving to reconstruct positive identity and self-advocacy by hard work, contributing to the community, supporting vulnerable populations, and involving in youth meetings and local leadership, among others. The study findings also shed light on how the creation of spaces for youth born of genocidal rape as one of the culturally relevant interventions was a roadmap to recovering from their birth history. Most of the youth testified that meeting with their peers helped them get a sense of belonging, self-acceptance, relief from distress and emotional pain, and an instillation of hope. Despite the psychosocial support that the youth had received, they still need further psychosocial support, catch-up learning programs, accompaniment support, advocacy to get a job, and support for their parents for their continuous reintegration. Health professionals and other stakeholders working with the youth born of genocidal rape in Rwanda and similar settings should consider the creation of spaces and the recommended interventions and strategies while designing or strengthening their interventions aimed at supporting this population.
Data Sharing Statement
Data analyses performed during the current study (recordings and transcripts) are available from the corresponding authors on reasonable request.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Institutional Review Board of the University of Rwanda, CMHS (IRB-CMHS). Both verbal and written informed consent were obtained from the participants after clearly explaining the research objectives and research process. The participants informed consent included publication of anonymized responses. In addition, participants were informed that no benefits or risks were associated with their participation in the study. Finally, the Declaration of Helsinki was respected, that states that participants have the right to opt out of the study if they do not want to participate or if they change their minds.
Consent for Publication
The participants consented to publication of their anonymised responses.
Acknowledgments
We are very grateful to the participants of this study who willingly accepted to participate in the study. We are also grateful to SURF Rwanda for their continual support at the study site.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no competing interests in this work.
References
1. Denov M, Kahn S. ‘They Should See Us as a Symbol of Reconciliation’: youth Born of Genocidal Rape in Rwanda and the Implications for Transitional Justice. J Hum Rights Pract. 2019;11(1):151–170. doi:10.1093/jhuman/huz011
2. Woolner L, Denov M, Kahn S. “I Asked Myself If I Would Ever Love My Baby”: mothering Children Born of Genocidal Rape in Rwanda. Violence Against Women. 2019;25(6):703–720. doi:10.1177/1077801218801110
3. Denov M, Piolanti A. Mothers of children born of genocidal rape in Rwanda: implications for mental health, well-being and psycho-social support interventions. Health Care Women Int. 2019;40(7–9):813–828. doi:10.1080/07399332.2019.1571593
4. Mukamana D, Brysiewicz P. The Lived Experience of Genocide Rape Survivors in Rwanda. J Nursing Scholarship. 2008;40(4):379–384. doi:10.1111/j.1547-5069.2008.00253.x
5. Guterres A. Conflict related sexual violence: Report of the United Nations Secretary General. United Nations. 2019.
6. Neenan J. Closing the Protection Gap for Children Born of War–Addressing Stigmatisation and the Intergenerational Impact of Sexual Violence in Conflict. Centre for Women, Peace and Security, London School of Economics; 2018.
7. Rohwerder B. Reintegration of Children Born of Wartime Rape. Institute of Development Studies; 2019.
8. Kahn S, Denov M. “We are children like others”: pathways to mental health and healing for children born of genocidal rape in Rwanda. Transcult Psychiatry. 2019;56(3):510–528. doi:10.1177/1363461519825683
9. Nikuze D. Parenting style and its psychological impact on rape born children: case of raped survivors of the 1994 genocide perpetrated against Tutsi in Rwanda. Int J Dev Sustainability. 2013;2:1084–1098.
10. Denov M, Green A, Lakor AA, Arach J. Mothering in the aftermath of forced marriage and wartime rape: the complexities of motherhood in postwar northern Uganda. J Motherhood Initiative Res Commun Involvement. 2018.
11. Kahn S, Denov M. Transgenerational trauma in Rwandan genocidal rape survivors and their children: a culturally enhanced bioecological approach. Transcult Psychiatry. 2022;136346152210802. doi:10.1177/13634615221080231
12. Banyanga J, Björkqvist K, Österman K. The trauma of women who were raped and children who were born as a result of rape during the Rwandan genocide: cases from the Rwandan diaspora. Pyrex J African Studies Dev. 2017;3:31–39.
13. Mukangendo MC. Caring for Children Born of Rape in Rwanda. Born War Protecting Children Sexual Violence Survivors Conflict Zones. 2007;40–52.
14. Sharlach L. Rape as Genocide: Bangladesh, the Former Yugoslavia, and Rwanda. New Political Science. 2000;22(1):89–102. doi:10.1080/713687893
15. Clark JN. A Crime of Identity: rape and Its Neglected Victims. J Hum Rights. 2014;13(2):146–169. doi:10.1080/14754835.2014.886952
16. Kantengwa O. How Motherhood Triumphs Over Trauma Among Mothers With Children From Genocidal Rape in Rwanda. J Social Political Psychol. 2014;2(1):417–434. doi:10.5964/jspp.v2i1.334
17. Callender T, Dartnall L. Mental Health Responses for Victims of Sexual Violence and Rape in Resource-Poor Settings. Sexual Violence Research Initiative. 2002;1–12.
18. Denov M, Woolner L, Bahati JP, Nsuki P, Shyaka O. The Intergenerational Legacy of Genocidal Rape: the Realities and Perspectives of Children Born of the Rwandan Genocide. J Interpers Violence. 2020;35(17–18):3286–3307. doi:10.1177/0886260517708407
19. Torgovnik J. Intended Consequences: Rwandan Children Born of Rape. Aperture; 2009.
20. Mahmood S. Challenges of Children Born by ISIS Rape in Iraq. Geneva: University of Geneva; 2017.
21. van Ee E, Kleber RJ. Growing Up Under a Shadow: key Issues in Research on and Treatment of Children Born of Rape. Child Abuse Review. 2013;22(6):386–397. doi:10.1002/car.2270
22. Hogwood J, Mushashi C, Jones S, Auerbach C. “I Learned Who I Am”: young People Born From Genocide Rape in Rwanda and Their Experiences of Disclosure. J Adolesc Res. 2018;33(5):549–570. doi:10.1177/0743558417713302
23. Uwizeye G, DeVon HA, McCreary LL, et al. Children born of genocidal rape: what do we know about their experiences and needs? Public Health Nurs. 2022;39(1):350–359. doi:10.1111/phn.13023
24. Russell D Foundation Rwanda; 2022. Available from: https://foundationrwanda.org/.
25. Patton MQ. Qualitative Evaluation and Research Methods. SAGE Publications, inc; 1990.
26. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
27. Smith HJ, Chen J, Liu X. Language and rigour in qualitative research: problems and principles in analyzing data collected in Mandarin. BMC Med Res Methodol. 2008;8(1):44. doi:10.1186/1471-2288-8-44
28. QSR International. Best Qualitative Data Analysis Software for Researchers | NVivo. QSR International Preprint at; 2022.
29. Green A, Denov M. Mask-Making and Drawing as Method: arts-Based Approaches to Data Collection With War-Affected Children. Int J Qual Methods. 2019;18:160940691983247. doi:10.1177/1609406919832479
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.