")
Back to Journals » Patient Preference and Adherence » Volume 13
Patients’ Perceptions To Reduced Orthodontic Treatment Time In Saudi Arabia
Authors Linjawi AI , Abushal AM, Al-Zahrani AM , Bakhamis BA
Received 7 July 2019
Accepted for publication 19 October 2019
Published 19 November 2019 Volume 2019:13 Pages 1973—1981
DOI https://doi.org/10.2147/PPA.S222181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Amal I Linjawi,1 Amal M Abushal,1 Amal M Al-Zahrani,2 Bushra A Bakhamis2
1Orthodontic Department, Faculty of Dentistry, King Abdulaziz University, Jeddah 21589, Saudi Arabia; 2Undergraduate Program, Faculty of Dentistry, King Abdulaziz University, Jeddah 21589, Saudi Arabia
Correspondence: Amal I Linjawi
Orthodontic Department, Faculty of Dentistry, King Abdulaziz University, P.O. Box 80209, Jeddah 21589, Saudi Arabia
Tel +966 504155573
Email [email protected]
Purpose: To evaluate patients’ perceptions regarding orthodontic treatment duration, cost, and willingness to undergo different procedures and techniques available to accelerate orthodontic tooth movement in Saudi Arabia.
Patients and methods: A cross-sectional survey was conducted in Saudi Arabia from January to March 2019. Patients from multiple centers were electronically surveyed regarding their perception of orthodontic treatment duration, acceptance of appliances and techniques available to shorten the duration of orthodontic treatment, and how much increase in fees they were willing to pay for those appliances and techniques. Descriptive and group comparison statistics were conducted, and the significance level was set at p<0.05.
Results: The response rate was 200/400 (50%): 50.5% were (>18–25 years old), 67.5% female, 80% Saudi, 67.5% self-pay and 52% with annual income <10,000 SR. A total of 83% of the participants agree that orthodontic treatment takes too long, and 55.5% wish it takes less than 6 months. The preferences for additional procedures were ranked in the following order: customized wires ranked 1 by 52.5%, followed by FDA (Food & Drug Administration) approved teeth vibrators by 40.5%, FDA approved drug injections by 33.5%, piezocision by 32.5%, and corticotomies by 46% of the participants. No significant differences in ranking between the groups according to age and annual income (p>0.05). 47.5% of the participants were able to pay for additional procedures. An increase in treatment fees was reported for up to (30–40%) for FDA approved teeth vibrators by 59% of the participants, followed by FDA approved drug injections by 33% of the participants. A significant difference in responses between the groups was reported according to gender and annual income (p<0.05).
Conclusion: Most of the patients strongly agreed that orthodontics treatment takes too long. The highest percentages of patients perceived customized wires as the most acceptable technique to undergo to shorten orthodontic treatment duration, followed by teeth vibrators.
Keywords: corticotomy, drug injection, orthodontic treatment duration, piezocision, rapid orthodontics, teeth vibrator
Introduction
The number of people requesting for orthodontic treatment is increasing because of multiple reasons. However, the prolonged duration of orthodontic treatment time, as well as the increased treatment charges, could be a concern for patients seeking orthodontic treatment. In addition, root resorption and white spot lesions as sequelae of prolonged orthodontic treatment are considered major risks of concern to both patients and professions.1–3
Multiple techniques and procedures have been reported to accelerate orthodontic tooth movement, and thus, shorten treatment duration, thereby, reducing the potential treatment risks.2–9 Varied biological, mechanical, and physical effects of such procedures that also varied in their level of invasiveness.2,4,7,9
Orthodontic treatment coupled with the use of teeth vibrator devices for physical stimulation by vibratory forces is one of the recommended techniques.4,6,7,9 Woodhouse et al, compared patients’ pain expression between conventional fixed orthodontic appliances and the use of supplemental vibrational devices and found no significant difference in pain between both methods.8 Mechanical stimulation by customized wires designed and manufactured according to the desired movement and the formulated treatment plan was also reported to reduce the treatment time significantly.6,10,11 Despite the non-invasiveness of these mechanical techniques, the increase in treatment costs has been considered an issue.4,6,7,9,10
Procedures reported to have biological effects included: one-time surgical procedures and drug injections. The one-time surgical procedures reported include corticotomies and piezocisions.4,9,12–14 These procedures are based on the principle of induced inflammatory effect induced on bone leading to accelerated osteoclastic effect and thus, accelerate tooth movement.4,7,9,12–16 Corticotomies were considered invasive, reported to be accompanied with some reported postoperative pain.12–14,16 In contrast, piezocision appeared to be an effective method to reduce the orthodontic treatment time without any unwanted sequelae.5 It was also reported to have a high level of acceptance and satisfaction among patients.14
The drug injection method includes the injection of exogenous inflammatory mediators and hormones into the periodontal tissues to induce bone resorption.7 Multiple mediators have been assessed including vitamin D and parathyroid hormones with positive reported effects on orthodontic tooth movement.17 However, most studies assessing these mediators have been animal studies.4,9
Among the different techniques, the less-invasive ones were reported to be more accepted by adult and adolescent patients as well as orthodontists as reported by Uribe et al.2
Patients’ perceptions toward orthodontic treatment modalities have been reported to be influenced by different factors such as age, gender, nationality, treatment cost, level of income and level of education.1–3,18,19 According to a report by Uribe et al, patients were willing to pay up to 20% increase in the treatment cost, for any procedure that could reduce their orthodontic treatment duration.2 Bindayel, in 2018, assessed the awareness and preferences of patients in Saudi Arabia to different orthodontic treatment modalities and payment options. He found that treatment costs and payment plan affected patients’ preferences for the different orthodontic treatment modalities.19 In addition, Sayers and Newton also found that ethnic background had a significant effect on patients’ expectation of orthodontic treatment.20
To the best of our knowledge, patients’ perceptions of the need for reduced orthodontic treatment time as well as their acceptance to the different procedures claimed to accelerate orthodontic tooth movement have not been assessed in Saudi Arabia.
The aim of this study was to evaluate patients’ perceptions regarding orthodontic treatment duration, cost, and willingness to undergo different procedures and techniques available to accelerate the rate of orthodontic tooth movement in Saudi Arabia.
Materials And Methods
This was a cross-sectional survey conducted in Saudi Arabia from January to March 2019. The study was approved by the Ethical committee at King Abdulaziz University, Faculty of Dentistry, Jeddah, Saudi Arabia.
The questionnaire was adopted from the study conducted by Uribe et al, 2014.2 It consisted of multiple-choice questions, 5-Likert scale questions and rank-order questions.
The questions were designed to assess the following variables:
- Demographic data including age, gender, nationality, education, annual income and methods of payment for orthodontic treatment
- Preferences for orthodontic treatment duration.
- Willingness to undergo additional procedures and techniques available to shorten the duration of orthodontic treatment. The assessed procedures included: customized wires, corticotomies (described as bone cuts), FDA approved teeth vibrators, piezocision (described as gum cuts), and FDA approved drug injections.
- Ability to pay to reduce orthodontic treatment time, willingness to pay for the different procedures and techniques available to shorten the duration of orthodontic treatment, and how much increase in fees they were willing to pay for the reduction in treatment time.
Patients undergoing orthodontic treatment from multiple private and governmental dental centers in Jeddah, Saudi Arabia were included in the study. The electronic survey was given to 400 orthodontic patients by self-administering or sending messages with links to the survey and their responses were recorded. Accordingly, a clear introduction and definitions of the various procedures and techniques proposed to reduce orthodontic treatment time were described in the questionnaire. All participants provided written informed consent, and the survey was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
Data were collected using Google Forms. Descriptive statistics were calculated for frequencies and percentages. Group comparisons were conducted using the Mann–Whitney U-test for gender and Kruskal Wallis test for age and annual income comparisons. Data were analyzed using Excel (Microsoft Excel 2007, Microsoft Corporation, Redmond, WA, USA) and SPSS (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp, USA). The significance level was set at (p<0.05).
Results
The questionnaire was sent to 400 patients, out of which, only 200 (50%) patients responded.
Sample Distribution
The sample characteristics including age, gender, nationality, education, annual income and methods of payment for orthodontic treatment are represented in Table 1. Out of the total number of participants, 50.5% were from the age group of >18–25 years old, 67.5% were female, 80% were Saudi, 67.5% were self-pay and 52% had an annual income <10,000 SR.
 |
Table 1 Characteristics Of Participants (N = 200) |
Preferences For Orthodontic Treatment Duration
The participants responses to perceptions towards the duration of orthodontic treatment are presented in Table 2. Eighty-three percent of the participants believed that orthodontic treatment takes too long (56% strongly agreed and 27% somewhat agreed). A significant difference in their perception was reported according to gender (female more than male) and according to annual income (mainly from participants with income <10,0000) (p<0.05). Forty-six percent expected orthodontic treatment to take less than 12 months, while 31% expected it to take 12–18 months. However, 55.5% wished it took less than 6 months and 30% wished it took 6–12 months for orthodontic treatment to complete. A significant difference in their wishes was reported according to gender only (female more than male) (p<0.05).
 |
Table 2 Frequencies And Percentages Of Responses To Perceptions Towards The Duration Of Orthodontic Treatment (N = 200) |
Willingness To Undergo Additional Procedures And Techniques
The participants’ responses to the preferences for additional procedures for a 25% to 30% reduction in treatment time are presented in Table 3. The highest responses for each procedure were as follows: customized wires were ranked first by 52.5% of the participants, FDA approved teeth vibrators were ranked second by 40.5%, FDA approved drug injections were ranked third by 33.5%, piezocision was ranked fourth by 32.5%, and corticotomies were ranked fifth by 46% of the participants. No significant differences in ranking were observed between the groups according to age, gender and annual income were reported (p>0.05).
 |
Table 3 Frequencies, Percentages, And Group Comparison According To Age, Gender And Annual Income Of Responses To Ranking The Preferences For Additional Procedures For A 25% To 30% Reduction In Treatment Time (N = 200). Significance Level Set At p<0.05 |
The participants' responses to the preferences for additional procedures with the given estimated reduction in treatment time for each procedure are presented in Table 4. The highest responses for each procedure were as follows: customized wires were ranked first by 57% of the participants, FDA approved teeth vibrators were ranked second by 32% and ranked first and third by equal responses (24.5%), piezocision was ranked fourth by 32%, and corticotomies were ranked fifth by 38% of the participants. No significant differences in ranking were observed between the groups according to age, and annual incomes were reported (p>0.05). However, a significant difference in ranking was reported according to gender (female more than male) for corticotomoies and piezocision only (p<0.05).
 |
Table 4 Frequencies, Percentages, And Group Comparison According To Age, Gender And Annual Income Of Responses To Ranking The Preferences For Additional Procedures With The Estimated Reduction In Treatment Time As Shown In The Table (N = 200). Significance Level Set At p<0.05 |
Ability And Willingness To Pay For Additional Procedures And Techniques
The participants' responses to the ability to pay to reduce orthodontic treatment time are presented in Table 5. Results indicated that 47.5% of the participants were able (17% very able, and 30% somewhat able) to pay for additional procedures to reduce orthodontic treatment time. No significant differences in responses were reported between the groups according to age for all procedures (p>0.05), while significant differences in responses between the groups were reported according to gender (female more than male) and annual income (mainly from the income 10,000–30,000) (p<0.05).
 |
Table 5 Frequencies, Percentages And Group Comparison According To Age, Gender And Annual Income Of Responses To Ability To Pay To Reduce Orthodontic Treatment Time (N = 200). Significance Level Set At p<0.05 |
Furthermore, the responses to the willingness to pay for each additional procedure assessed are presented in Table 6. The highest responses for each procedure were as follows: 60.5% of the participants were willing to pay for customized wires (40.5% most willing and 20% somewhat willing), 53.5% of the participants were willing to pay for FDA approved teeth vibrators (23.5% most willing and 30% somewhat willing), and 45% of the participants were willing to pay for FDA approved drug injections (27% most willing and 18% somewhat willing). In contrast, 49.5% of the participants were unwilling to pay for corticotomies (40.5% most unwilling and 9% somewhat unwilling), and 49.5% of the participants were unwilling to pay for piezocision (23.5% most unwilling and 26% somewhat unwilling). No significant differences in responses between the groups according to age and gender were reported for all procedures (p>0.05). However, for the annual income, a significant difference in responses was reported for the FDA approved teeth vibrators (mainly from the income <10,000) and the FDA approved drug injections (mainly from the income 10,000–30,000) only (p<0.05).
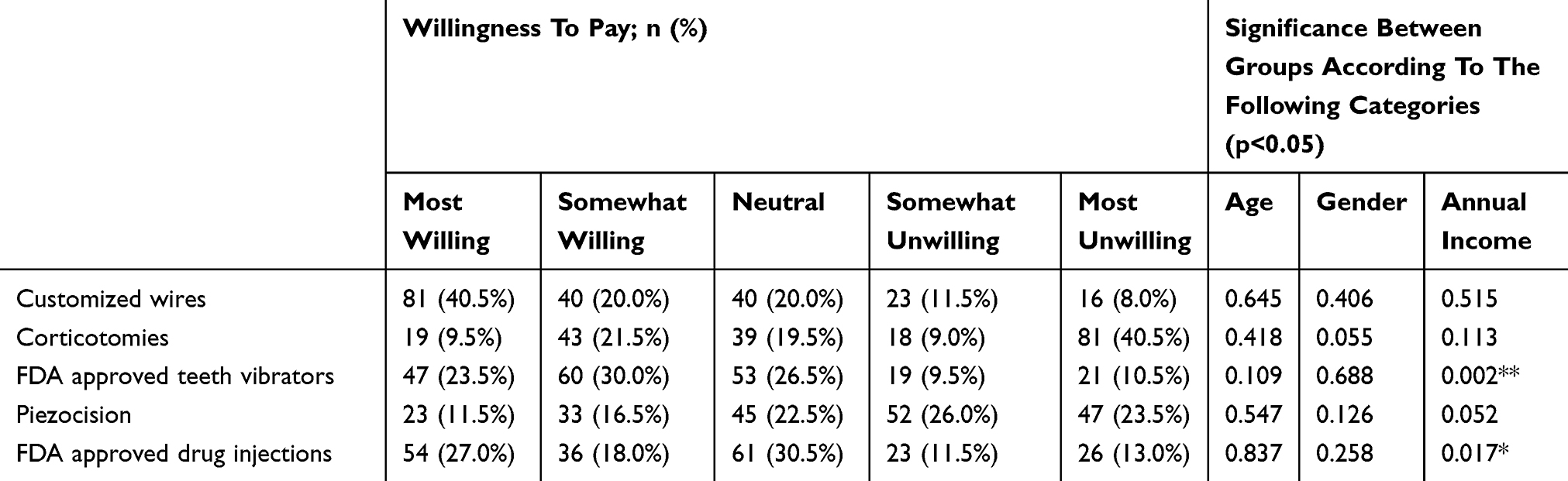 |
Table 6 Frequencies, Percentages, And Group Comparison According To Age, Gender And Annual Income Of Responses To Willingness To Pay For Each Procedure Assessed (N = 200). Significance Level Set At p<0.05 |
The responses to the willingness to pay for the estimated percentage increase in treatment fees for each additional procedure claimed to reduce treatment time are presented in Table 7. The highest responses for each procedure varied. For customized wires, 60% of the participants were ready to pay 10–20% increase in treatment fees. For corticotomies, 80% of the participants were ready to pay 10–20% increase in fees. For FDA approved teeth vibrators, 59.5% of the participants were ready to pay 10–20% increase in fees and 59% were ready to pay 30–40% increase in fees. For piezocision, 79.5% of the participants were ready to pay 10–20% increase in fees. For FDA approved drug injections, 58.5% of the participants were ready to pay 10–20% increase in fees and 33% were ready to pay 30–40% increase in fees. No significant difference in responses between the groups according to age was reported for all procedures (p>0.05). However, for the gender, a significant difference in responses was reported for the customized wires and the FDA approved teeth vibrators only with females more than males (p<0.05). For the annual income, a significant difference in responses was reported for the customized wires, FDA approved teeth vibrators and the FDA approved drug injections only (mainly for income <10,000) (p<0.05).
 |
Table 7 Frequencies, Percentages, And Group Comparison According To Age, Gender And Annual Income Of Responses To Willingness To Increase In Treatment Fees For Each Additional Procedure Claimed To Reduce Treatment Time (N = 200). Significance Level Set At p<0.05 |
The responses to the percentage of fee increase for a particular reduction in treatment time are presented in Table 8. For 10% reduction in treatment time, 83.5% of the participants were willing to pay 10–20% increase in treatment fees. For 20% reduction in treatment time, 80% of the participants were willing to pay 10–20% increase in treatment fees. For 30% reduction in treatment time, 58.5% of the participants were willing to pay 10–20% increase in treatment fees and 38% were willing to pay 30–40% increase in treatment fees. For 40% reduction in treatment time, 57% of the participants were willing to pay 10–20% increase in treatment fees and 40% were willing to pay 30–40% increase in treatment fees. For 50% reduction in treatment time, 52.5% of the participants were willing to pay 10–20% increase in treatment fees and 29% were willing to pay 50% increase in treatment fees. No significant difference in responses between the groups according to age and gender was reported for all procedures (p>0.05). However, for the annual income, a significant difference in responses was reported for the 40% reduction in treatment time only (mainly for income <10,000) (p<0.05).
 |
Table 8 Frequencies, Percentages, And Group Comparison According To Age, Gender And Annual Income Of Responses To Increase In Treatment Fees For A Specified Reduction In Treatment Time (N = 200). Significance Level Set At p<0.05 |
Discussion
The aim of this study was to evaluate patients’ perceptions regarding orthodontic treatment duration, cost, and willingness to undergo different procedures and techniques available to accelerate the rate of orthodontic tooth movement in Saudi Arabia. The age group interested in the subject of the survey was mainly from the middle-aged. Similarly, Kim, in 2005, assessed patients’ perceptions towards orthodontic treatment among adults categorized according to age, sex, and area of living. Similar to our study, he found that the middle-aged group had a relatively higher percentage of interest in orthodontic treatment. He also found that neither gender nor area of living was significantly associated with the positive interest in orthodontic treatment.3
More than half of the participants agreed that orthodontic treatment was time-consuming, and they wished it took less than 6 months, which is similar to the findings reported by Uribe et al.2 However, the expectation of the participants in the current study about how long orthodontic treatment should take was in accordance with their wishes, which is in contrast to the finding of Uribe et al.2
The results showed that customized wires followed by FDA approved teeth vibrators and FDA approved drug injections were the most preferred procedures to undergo among different procedures and techniques. In contrast, participants were mostly unwilling to undergo corticotomies and piezocisions. The same ranking was reported both when the advice was for 20–30% reduction in treatment time for all procedures and when each procedure was estimated to reduce the treatment time, even though corticotomies were suggested to result in 50% reduction of treatment time. The same findings were reported by Uribe et al.2 It was not surprising to find that patients preferred the less-invasive nonsurgical procedures as also reported by many other studies.12–14 Current findings indicated no significant effect of age, gender and annual income in the reported preferences for the procedures assessed.
Results also indicated that 47.5% of the participants were able to pay for additional procedures to reduce orthodontic treatment time, while 27% were neutral in their response. Their willingness to pay according to procedure preferences were as follows: 60.5% of the participants were willing to pay for customized wires, 53.5% for FDA approved teeth vibrators, and 45% of the participants were willing to pay for FDA approved drug injections. On the other hand, 49.5% of the participants were unwilling to pay for corticotomies, and 49.5% were unwilling to pay for piezocision. However, when they were asked for the percentage increase in treatment fees, their responses to their preferred non-invasive procedures were as follows: for customized wires, 60% of the participants were ready to pay but only for a 10–20% increase in treatment fees. On the other hand, for FDA approved teeth vibrators, 59.5% of the participants were ready to pay 10–20% increase in fees and 59% were ready to pay 30–40% increase in fees. For FDA approved drug injections, 58.5% of the participants were ready to pay 10–20% increase in fees and 33% were ready to pay 30–40% increase in fees. However, responses of the participants for willingness to pay were significantly affected by gender and annual income variables in the current study. This supports the finding of Wall and Bindayel who reported that the treatment modality choice is affected by financial measures.18,19
The current findings indicated that participants were willing to pay an increase of only up to 10–20% in the treatment fees, despite the reduction in treatment time, except if there was 50% reduction in treatment time, where 52.5% of the participants were willing to pay 10–20% increase in treatment fees and 29% were willing to pay even up to 50% increase in treatment fees. In contrast to the findings of Uribe et al, the percentage reduction in time was not matched with the percentage increase in fees.2 Current findings also indicated no significant effect of age, gender and annual income in most of the reported responses for the increase in treatment fess for a specific reduction in treatment time.
Limitations
As the study design was a cross-sectional survey, the major limitations were causal interference and information bias. Also, the external validity could be limited to Jeddah as the patients evaluated were only from the multiple centers of Jeddah.
Conclusion
- The age group interested in the subject of the survey was mainly from the middle-aged.
- More than half of the participants agreed that orthodontic treatment takes too long, and they wished it takes less than 6 months.
- The non-invasive, non-surgical procedures: customized wires followed by FDA approved teeth vibrators and FDA approved drug injections were the most preferred procedures to undergo as well as willing to pay among different procedures and techniques.
- Almost half of the participants were able to pay for additional procedures to reduce orthodontic treatment time.
- Participants were only willing to pay up to 10–20% increase in fees for most procedures. However, for FDA approved teeth vibrators and FDA approved drug injections, participants were ready to pay up to 30–40% increase in treatment fees.
- The participants were willing to increase treatment fees only up to 10–20% despite the reduction in treatment time, except for the 50% reduction in treatment time where participants were willing to pay for up to 50% increase in treatment fees.
- No significant effect of age, gender and annual income on the reported preferences to undergo the additional procedures, while gender and annual income did have an effect on the willingness to pay extra fees for those procedures.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Segal GR, Schiffman PH, Tuncay OC. Meta-analysis of the treatment-related factors of external apical root resorption. Orthod Craniofac Res. 2004;7(2):71–78. doi:10.1111/ocr.2004.7.issue-2
2. Uribe F, Padala S, Allareddy V, Nanda R. Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time. Am J Orthod Dentofacial Orthop. 2014;145(4):S65–S73. doi:10.1016/j.ajodo.2013.12.015
3. Kim Y. Study on the perception of orthodontic treatment according to age: a questionnaire survey. Korean J Orthod. 2017;47(4):215–221. doi:10.4041/kjod.2017.47.4.215
4. Nimeri G, Kau CH, Abou-Kheir NS, Corona R. Acceleration of tooth movement during orthodontic treatment-a frontier in orthodontics. Prog Orthod. 2013;14(1):42. doi:10.1186/2196-1042-14-42
5. Alfawal AMH, Hajeer MY, Ajaj MA, Hamadah O, Brad B. Evaluation of piezocision and laser-assisted flapless corticotomy in the acceleration of canine retraction: a randomized controlled trial. Head Face Med. 2018;14(1):4. doi:10.1186/s13005-018-0161-9
6. Darendeliler MA, Zea A, Shen G, Zoellner H. Effects of pulsed electromagnetic field vibration on tooth movement induced by magnetic and mechanical forces: a preliminary study. Aust Dent J. 2007;52(4):282–287. doi:10.1111/j.1834-7819.2007.tb00503.x
7. Leethanakul C, Phusuntornsakul P, Pravitharangul A. Vibratory stimulus and accelerated tooth movement: a critical appraisal. J World Fed Orthod. 2018;7:106–112. doi:10.1016/j.ejwf.2018.07.005
8. Woodhouse NR, DiBiase AT, Papageorgiou SN, et al. Supplemental vibrational force does not reduce pain experience during initial alignment with fixed orthodontic appliances: a multicenter randomized clinical trial. Sci Rep. 2015;5:17224. doi:10.1038/srep17224
9. Ganesh ML, Pandian SK. Acceleration of tooth movement during orthodontic treatment-a frontier in orthodontics. Int J Pharm Sci Rev Res. 2017;9(5):741.
10. Alford TJ, Roberts WE, Hartsfield JK
11. Sachdeva RCL, Aranha SLT, Egan ME, et al. Treatment time: sureSmile vs conventional. Orthodontics. 2012;13:72.
12. Aboul-Ela SM, El-Beialy AR, El-Sayed KMF, Selim EMN, El-Mangoury NH, Mostafa YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthod Dentofacial Orthop. 2011;139(2):252–259. doi:10.1016/j.ajodo.2009.04.028
13. Cohen G, Campbell PM, Rossouw PE, Buschang PH. Effects of increased surgical trauma on rates of tooth movement and apical root resorption in foxhound dogs. Orthod Craniofac Res. 2010;13(3):179–190. doi:10.1111/(ISSN)1601-6343
14. Gibreal O, Hajeer MY, Brad B. Evaluation of the levels of pain and discomfort of piezocision-assisted flapless corticotomy when treating severely crowded lower anterior teeth: a single-center, randomized controlled clinical trial. BMC Oral Health. 2019;19(1):57. doi:10.1186/s12903-019-0758-9
15. Baloul SS, Gerstenfeld LC, Morgan EF, Carvalho RS, Van Dyke TE, Kantarci A. Mechanism of action and morphologic changes in the alveolar bone in response to selective alveolar decortication facilitated tooth movement. Am J Orthod Dentofacial Orthop. 2011;139(4):S83–S101. doi:10.1016/j.ajodo.2010.09.026
16. Buschang PH, Campbell PM, Ruso S. Accelerating tooth movement with corticotomies: is it possible and desirable? Semin Orthod. 2012;18:286–294. doi:10.1053/j.sodo.2012.06.007
17. Collins MK, Sinclair PM. The local use of vitamin D to increase the rate of orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 1988;94(4):278–284. doi:10.1016/0889-5406(88)90052-2
18. Wall T, Nasseh K, Vujicic M. Most important barriers to dental care are financial, not supply related. Health Policy Institute Research Brief-American Dental Association; 2014.
19. Bindayel NA. Awareness of orthodontic modalities and preference of appliance and payment options in Saudi Arabia. Saudi J Oral Sci. 2018;5(2):98. doi:10.4103/sjos.SJOralSci_5_18
20. Sayers MS, Newton JT. Patients expectations of orthodontic treatment: part 2 findings from a questionnaire survey. J Orthod. 2007;34(1):25–35. doi:10.1179/146531207225021888
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.