")
Back to Journals » Patient Preference and Adherence » Volume 18
Overview of Patients with Hemophilia in China: Demographics, Diseases, Treatment, and Health Status
Authors Zhang L, Zhang P , Chen W
Received 24 September 2023
Accepted for publication 6 January 2024
Published 13 January 2024 Volume 2024:18 Pages 101—109
DOI https://doi.org/10.2147/PPA.S441873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Luying Zhang,1,* Peng Zhang,2,* Wen Chen1
1School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China; 2School of Humanities, Shanghai Institute of Technology, Shanghai, 201418, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Chen, School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China, Email [email protected]
Background: In China, there were over 65,000 hemophilia patients according to estimations requiring overall description. However, former Chinese studies related to hemophilia were based on data of relatively small sample size from single-center or selected multi-centers in specific areas.
Objective: This study is aimed to provide an overview of patients with hemophilia in China and basic information for optimized hemophilia care and policy decisions in the future.
Methods: We cooperated with the biggest patient organization of hemophilia in China, Hemophilia Home, got access to over ten thousand registered patients with hemophilia and conducted a national representative online survey in 2021. Descriptive statistics were conducted to describe the mean and standard deviation for continuous variables and numbers and proportions for categorical variables.
Results: Nine hundred and fifty patients with hemophilia aged 0– 71 years were included in our analysis and divided into 538 children and 412 adults. Compared to international research, consistent results were found regarding the proportions of hemophilia types and hemophilia severity, while Chinese patients had less opportunity to receive the formal education and the lower rate to be employed or married. Although children with hemophilia had higher household income, timely treatment, and more prophylaxis treatment leading to better clinical outcomes and higher HRQoL than adults, there were still more annual bleeds, chronic pains, and lower EQ-VAS scores especially in adults than in other countries.
Conclusions and Recommendation: Our findings suggest the urgency for promoting hemophilia care and improving the social adaptation of hemophilia patients in China.
Keywords: hemophilia, treatment, clinical outcomes, health-related quality of life, China
Introduction
Hemophilia is a rare disease, which is X chromosome-linked bleeding disorder with missing or defective clotting factor.1 It causes spontaneous bleeding, pain, target joints or arthropathy, limitation of mobility or even disability, and even life-threatening intracranial hemorrhages.2 To minimize the adverse effects of hemophilia on patients’ physical well-being and quality of life, it is beneficial to provide lifelong care and ensure regular infusion of clotting factors.3 To further improve patient care, real-world data on demographics, diseases, treatment, health status, and so on are required to provide information for comprehensive understanding.
In China, a large country with a 1.41 billion population, it was estimated that there were over 65,000 hemophilia patients.4 China has been striving to improve hemophilia care for the past 40 years. The Hemophilia Treatment Center Collaborative Network of China has been formed gradually, beginning with the establishment of the national Hemophilia Cooperative group in 1985. Currently, a collaborative network across the country with 115 hemophilia treatment centers and six core hemophilia treatment centers is being developed to deliver timely diagnosis and standard care for the local patients.4 Additionally, Chinese guidelines on the treatment of hemophilia are published and renewed continually by the Chinese Society of Hematology Thrombus and Hemostasis Group and Chinese Hemophilia Cooperative Group to provide basic principles for clinical practice.5 Furthermore, to provoke awareness of the rare disease in 2018 hemophilia was listed as one of the first 121 rare diseases of the National Rare Disease in China. At the same time, to reduce the cost of treatment in 2019 the Basic Health Insurance expand coverage for hemophilia patients by reimbursing recombinant human clotting factor.6,7
Former Chinese studies related to hemophilia mainly focused on its epidemiology, diagnosis, and treatment based on data of relatively small sample size from single-center or selected multi-centers in specific areas.7–13 Recently, scholars pay attention to the clinical outcomes and health-related quality of (HRQoL) among Chinese patients.9,14–17 Nevertheless, the national studies mostly describe the progression of building networks, registry systems, and treatment centers in China.4,8,18 Scant evidence on the general status of hemophilia patients in mainland China, and these two studies are only limited to adults or shed light on specific types of hemophilia patients rather than all the hemophilia patients.19,20 There is an urgent need to describe the landscape of the whole hemophilia population in China, based on national representatives and a relatively big sample with patients’ self-reported real-world data, to reflect and update the overall status of their demographics, diseases, treatment, and health status.
The aim of this study is to comprehensively describe the current status of hemophilia patients in China based on patients’ self-reported real-world data from a national survey, including their demographics, socioeconomic status, hemophilia history and comorbidities, treatment, clinical outcomes, and HRQoL. Our study provides basic information on hemophilia patients in China for optimized hemophilia care and policy decisions in the future.
Materials and Methods
Study Design and Data Collection
A national representative, online survey was conducted in 2021 across mainland China. The questionnaire contained individual information on demographic (age, regional location, etc.), socioeconomic status (marital status, family income, employment status, education level, etc.), disease history (hemophilia and other comorbidities), treatment (first diagnosis and treatment age, and treatment regimens), clinical outcomes (bleedings, target joint, chronic and acute pain and disability) and HRQoL.
The largest patient organization of hemophilia in China, Hemophilia Home, provided support to get access to over ten thousand registered patients with hemophilia. Hemophilia Home is a dedicated organization established in 2012, providing education, resources, and support for hemophilia patients and their families. Hemophilia Home offers information on disease management, organizes community gatherings, and advocates for better healthcare and social support, and improves the quality of life for patients and empowers them through education, community engagement, and consulting services. Hemophilia Home has independently developed a user-friendly mobile application (APP) called “Hemophilia Home” to help patients and their families conveniently record information related to bleeding episodes, treatments, medical visits, and medication expenses. The app also provides quick access to the latest treatment options, healthcare policies, drug availability, and charitable support programs, ensuring easy access to important knowledge for patients. In our study, through Hemophilia Home’s APP, the target patients were sampled and invited with the invitation letter. After giving informed consent, the patients completed the questionnaire online. Children with hemophilia who were unable to read or understand were asked to finish the survey by their parents.
The study protocol was proved by the Institutional Review Board Ethics Committee of Fudan University approved (Ref no.: IRB#2022-02-0951).
Eligibility Criteria
The inclusion criteria for analysis in this study were (i) patients diagnosed with hemophilia with or without inhibitor, (ii) patients without cognitive impairments, (iii) patients who gave full informed consent, and (iv) Chinese.
Hemophilia Severity and Comorbidities
The severity of hemophilia was divided into three categories by factor VIII or factor IX level: (i) mild: factor level over between 6% and 40%; (ii) moderate: factor level between 1% and 5%; (iii) severe: factor level less than 1%. Comorbidities included infectious blood diseases such as hepatitis A, B, and C, HIV, etc. Body mass index (BMI) was calculated by the patient’s height and weight with overweight or obese with the classification of underweight (BMI<18.5 kg/m2), normal (18.5 kg/m2≤BMI≤23.9 kg/m2), overweight or obese (BMI≥23.9 kg/m2) in China.
Clinical Outcomes
Based on related definitions and standards in Chinese guidelines on the treatment of hemophilia (version 2020),5 the respondents were guided and reported their clinical outcomes. Annual bleeds and target joints were self-reported, and disability was determined as statutory disabled patients with a legal certificate. Chronic pain and acute pain due to hemophilia were classified into five levels by the frequency of occurrence: (i) never: 0% of the time; (ii) occasionally: ≤25% of the time; (iii) sometimes: 25–50% of the time; (iv) frequently: 50–75% of the time; (v) always: >75% of the time.
HRQoL
A widely used generic instrument of HRQoL, the five-level EuroQol five-dimensional (EQ-5D-5L), was embedded in the questionnaire. The EQ-5D-5L questionnaire consisted of two parts: EQ-5D-5L index utility score and visual analogue scale (EQ-VAS). The EQ-5D-5L index utility score was calculated by the scores of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression ranging from −0.391 to 1 in the Chinese value set.21 EQ-VAS indicated the patient’s health status from the worst to the best (from 0 to 100).
Statistical Analysis
Descriptive statistics were conducted to describe the mean and standard deviation for continuous variables and numbers and proportions for categorical variables. Fisher’s exact test was employed to compare the difference between two groups with the significance level of 0.05 (two-tailed). All the analyses were performed using the Statistics Data Analysis (STATA) software version 15.1 (StataCorp LLC, College Station, TX, USA).
Results
Demographics
Totally, 950 patients with hemophilia aged 0–71 years were included in our analysis, and the self-reported results of questionnaires were collected, and all of them were male. Among patients without inhibitors, 684 were hemophilia A (HA) and 149 were hemophilia B (HB). Other 117 patients had inhibitors. The characteristics among patients with hemophilia in China are shown in Table1; 538 respondents were children aged 0 to 17 years old, and 412 respondents were adults aged 18 to 71 years old. The mean age of the children group and the adult group were 7.21 and 33.14 years, respectively. Generally, China is divided into three regions based on geographical factors, economic development, and cultural customs and 47%, 26%, and 27% of children and 37%, 36%, and 27% of adults lived in the East, Mild, and West area, respectively.
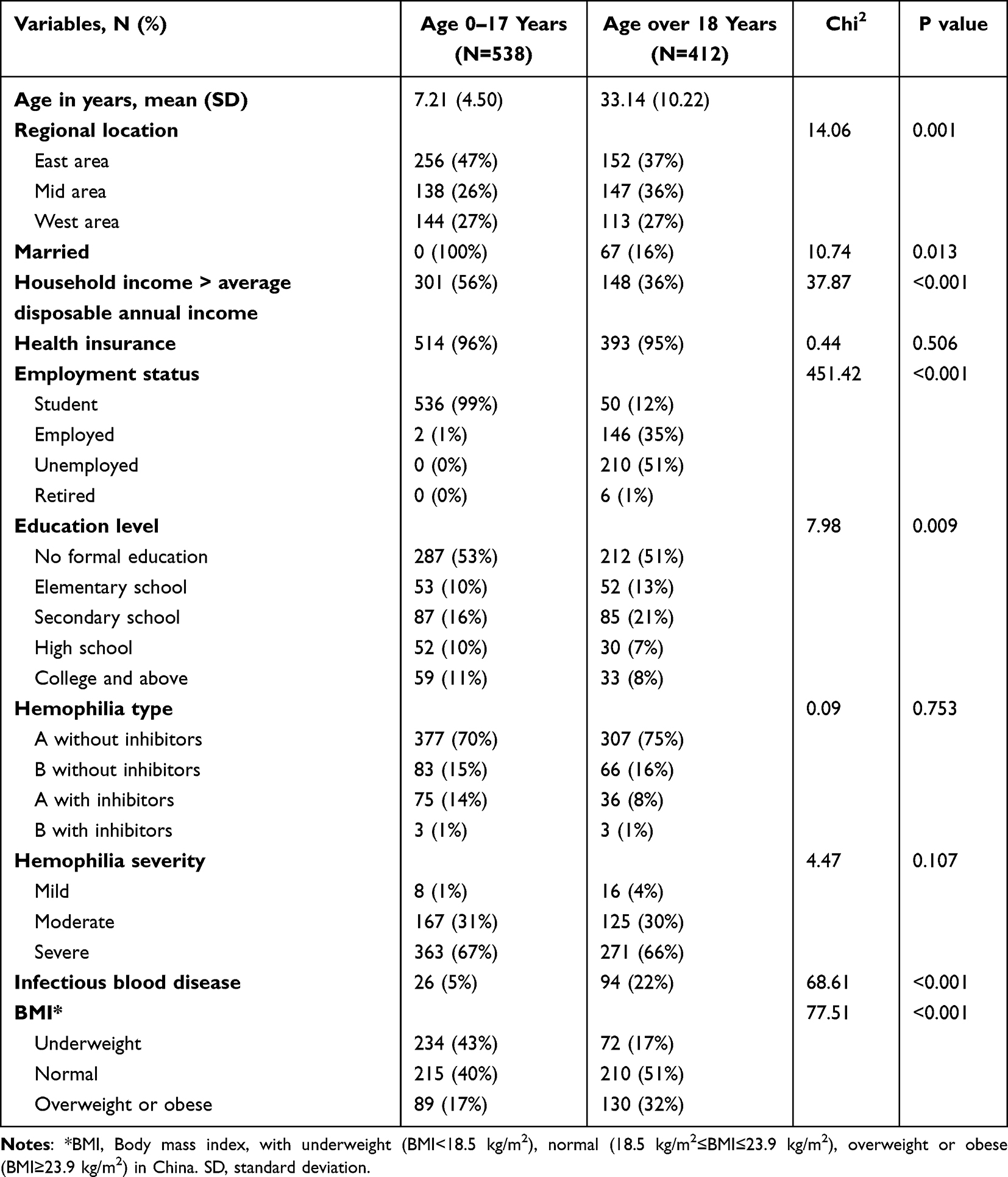 |
Table 1 Characteristics Among Patients with Hemophilia in China |
Socioeconomic Status
About 16% of adults were married. In 2020, the average disposable annual income of urban households in China was $6355 US dollars converted by the annual average rate ($1 US dollar =¥6.8974 RMB). In the children group, 56% of their households had higher disposable annual income than the average. About 36% of adults had higher disposable annual household income than the average. As for health insurance, China legally implements social health insurance, including the mandatory Urban-Rural Resident Basic Medical Insurance for employed individuals and the voluntary Urban Employee Basic Medical Insurance for residents. Therefore, while striving to achieve universal healthcare coverage, a small portion of the population may still not be covered by social medical insurance, and in our study, the insured rate in the group aged 0–17 years was 96% which was similar to the rate of 95%, in the group aged over 18 years.
About 16%, 10%, and 11% of children received education from secondary school, high school, and college, respectively. About 51% adult patients never received education from schools including the elementary level. Over half of adults (51%) with hemophilia did not receive formal education and 8% of them completed college. Most of the children were still students, and the other 2 of them were over 16 years old and employed. Among the adults, 51% were unemployed, and 35% had full-time or part-time jobs.
Hemophilia History and Comorbidities
In the group aged 0–17 years, 70% of them were HA without inhibitors, and 15% of them were HB without inhibitors. In the group aged over 18 years, 75% of them were HA without inhibitors, and 16% of them were HB without inhibitors. About 15% of children (14% HA and 1% HB) and 9% of adults (8% HA and 1% HB) had inhibitors. The proportions of moderate and severe hemophilia patients were 31% and 67% in children and 30% and 66% in adults.
About 5% of children and 22% of adults were infected by related blood diseases. The BMI showed that 17% of children and 32% of adults were overweight or obese, 43% of children and 17% of adults were underweight, and 40% and 51% of the two groups had normal BMI.
Treatment
Treatment among patients with hemophilia in China is shown in Table 2 The children tended to be first diagnosed at an earlier age (mean = 1.46) than the adults (mean = 8.47). The mean age at diagnosis was 4.12, 1.66, and 1.30, respectively, for mild, moderate and severe patients among children and 11.30, 8.18, and 7.18, respectively, for mild, moderate and severe patients among adults.
 |
Table 2 Treatment Among Patients with Hemophilia in China |
Children are also more likely to receive treatment sooner at an average age of 2.13, whereas the first treatment age of adults was 13.32 years old. The children also had a shorter time period between the first diagnosis and the first treatment, and on average they started treatment in the same year after being diagnosed. It took 5.10 years on average for adults to begin their first treatment after the first diagnosis.
Among patients without inhibitors, 54% of 460 children and 82% of 373 adults self-reported they were receiving on-demand treatment. The children (46%) were more likely to receive prophylaxis treatment than the adults (18%). Among patients with inhibitors, 29% of 78 children and 3% of 39 adults underwent immune tolerance induction (ITI) treatment.
Clinical Outcomes
As shown in Table 3, the children with hemophilia gained better clinical outcomes. Children had with fewer mean annual bleeds and lower annual mean bleed rate (32.93 and 2.81%, respectively) than in adults (51.92 and 4.54%, respectively). There were also lower number of mean target joints in children than adults (0.74 and 5.23 respectively). As a result, 5% of children and 72% of adults were disabled.
 |
Table 3 Clinical Outcomes and Health-Related Quality of Life Among Patients with Hemophilia in China |
The occurrence of chronic pain and acute pain is shown in Figure 1. For chronic pain, 31% and 43% of children never or occasionally had chronic pain, and 18%, 7%, and 1% of them sometimes, frequently, and always had chronic pain. About 4% and 36% of adults never or occasionally had chronic pain, and 34%, 18%, and 8% of them sometimes, frequently, and always had chronic pain. For acute pain, 40% and 45% of children never or occasionally had acute pain, and 11%, 3%, and 1% of them sometimes, frequently, and always had acute pain. About 21% and 53% of adults never or occasionally had acute pain, and 17%, 8%, and 1% of them sometimes, frequently, and always had acute pain.
 |
Figure 1 Self-reported chronic pain and acute pain among patients with hemophilia by age group. |
Health-Related Quality of Life (HRQoL)
The EQ-5D results in Table 3 showed that the mean utility score of children with hemophilia is 0.868 (SD = 0.197), and the mean utility score of adults was 0.584 (SD = 0.292). The results of the five dimensions of EQ-5D-5L are shown in Figure 2. For children, 47% of them had a different level of pain or discomfort. About 17% and 21% of them had a different level of mobility or usual activities. About 11% of children had an extreme problem of self-care, but none of them had an extreme problem relating to anxiety or depression. For adults, 87% of them had problems with pain or discomfort. About 85% and 78% of them had problems with mobility or usual activities, which were much higher than children. There was also a higher proportion of having extreme problem relating to anxiety or depression (5%) in adult. About 2% of adults had an extreme problem of self-care which was lower that this in children. The EQ-VAS in the group aged 0–17 years was 78.55 on average (SD = 23.07) and in the group aged over 18 years was 59.23 (SD = 23.39).
 |
Figure 2 The five dimensions of EQ-5D-5L among patients with hemophilia by age group. |
Discussion
Based on patients’ self-reported real-world data from a national survey, this descriptive study aimed to comprehensively reflect the current status of hemophilia patients and newly provide a general profile of their demographics, socioeconomic status, hemophilia history and comorbidities, treatment, clinical outcomes, and HRQoL.
Of 950 included patients in our study, 538 were children and 412 were adults, which were evenly distributed in the East, Mild, and West area. The proportion of patients with different hemophilia types was consistent with global studies with about 70% with HA and 15% with HB without inhibitors in two groups.22–24 The distribution of hemophilia severity was also similar in the two groups, and about two-thirds of patients had severe hemophilia like the study result in India.25 Fewer children were infected by related blood diseases or were overweight or obese than adults. However, overall, the infection rate of blood-related diseases is higher among Chinese hemophilia patients, especially for adults who have received long-term blood transfusions and had limited access to advanced medical conditions in their younger years. The challenges in blood product management have contributed to an increased risk of infection from other diseases among hemophilia patients, thereby raising the likelihood of associated health impairments.
Children with hemophilia had higher household income, timely treatment, and more prophylaxis treatment. Almost entirely of patients were insured (96% in children vs 95% in adults) due to the universal coverage of social health insurance in China. Nevertheless, with the development of the economy and hemophilia care in China in the past decades, children possessed more resources such as higher household income than adults. The mean first diagnosis age and first treatment age in the group aged 0–17 years were far earlier than in the group aged over 18 years (1.46 and 2.13 years old in children vs 8.47 and 13.32 years old in adults), and also after first diagnosis children received timely treatment within the same year on average. Adults began their first treatment 5.10 years later after their first diagnosis. Similarly, it was found in the former Chinese study of HA patients that there was a delay of 8.6 years from the first bleed to the first treatment.20 Furthermore, the proportion of children without inhibitors receiving prophylaxis treatment was higher than adults (46% in children vs 18% in adults), which was close to the proportion of young hemophilia patients aged 18–30 years in America (49%)24,26 and better than other developing countries.27 Children with hemophilia benefit from the increased adoption of prophylactic treatment, which leads to improved clinical outcomes and higher health-related quality of life.28 Additionally, with the advancement of treatment, earlier diagnosis and more timely intervention also contribute to these positive outcomes. As for patients with inhibitors, 29% of children and 3% of adults received ITI treatment.
As a result, children with hemophilia gained better clinical outcomes and higher HRQoL than adults but there was still room to promote Chinese hemophilia patients’ health status. Children had fewer annual bleeds (32.93 times in children vs 51.92 times in adults) and fewer target joints on average (0.74 in children vs 5.23 in adults). However, the mean annual bleeds among patients with hemophilia in Russia was 31.08 in all age groups,29 which indicated the urgency for the promotion of hemophilia care in adult patients. About 69% of children and 96% of adults had chronic pains, which was higher than the proportion of chronic pains among hemophilia patients in Brazil (36%).20 About 60% of children and 79% of adults suffered from any level of acute pain. The mean EQ-5D utility scores were higher in the group aged 0–17 years with 0.868 than 0.584 in the group aged over 18 years. As the most significantly negatively affected dimension with the highest proportion of extreme difficulties reported, self-care is most affected in children hemophilia patients, while mobility is most affected in adult hemophilia patients. Additionally, as the dimension most widely affected with the highest proportion of difficulties reported at any level, the dimension of pain is most widely affected in child hemophilia patients, and in contrast, the dimension of mobility remains the most widely affected for adult hemophilia patients. As patients’ age, their lifelong experience of pain leads to a significant increase in their tolerance for pain. However, due to delayed treatment, irreversible joint damage and disabilities occur, resulting in an increasingly pronounced negative impact on their mobility and functional abilities.30 The mean EQ-VAS scores showed the same tendency with 78.55 among children and 59.23 among adults, and the mean EQ-VAS scores among patients in all age groups in Russia was 60.9.31
Our results also provoke attention to improving the social adaptation of hemophilia patients. For children, 53% of them were lack of formal education even though they were supposed to be students. For adults, 51% of them did not receive formal education. Only 12% of them had full-time or part-time jobs, and 51% of them were unemployed. The unemployment rate was far higher than about 22% in America24,26 and 28% in Brazil.23 Additionally, 16% of hemophilia patients were married which was lower than the rate reported globally (22%).26 These all indicated the negative impact of hemophilia on education, employment, and interpersonal relationships and the necessity of increasing equity and social support for patients through multiple approaches.
The limitation of this study should be mentioned. A convenient sampling method was used to include more patients as possible. Also, a sample bias may exist because we conducted our survey on patients who registered in Hemophilia Home’s APP.
Conclusion
This study provided an overview of the status of hemophilia patients in China. Based on patients’ self-reported real-world data from a national survey, 950 patients’ demographics, socioeconomic status, hemophilia history and comorbidities, treatment, clinical outcomes, and HRQoL were comprehensively described. These findings provided basic information for related studies. The results emphasized the importance of optimizing hemophilia care such as timely and prophylaxis treatment, especially for adults, and the urgency of promoting health status and social adaptiveness for hemophilia patients in China.
Data Sharing Statement
The data that support the findings of this study are available from Haemophilia Home but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the author, LZ, upon reasonable request and with permission of Haemophilia Home.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board Ethics Committee of Fudan University (Ref no.: IRB#2022-02-0951) and conducted in correspondence with regional and relevant guidelines, which complied with the Declaration of Helsinki. Patient consent was obtained via tick box selection for the patient‑reported element of the study.
Acknowledgments
The authors would like to thank Mr. Tao Guan, Mr. Nan Zhao and colleagues from Haemophilia Home for their help and advice with data collection and interpretation. The authors have no competing interests.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Srivastava A, Brewer AK, Mauser-Bunschoten EP, Hemophilia TGWG. Guidelines for the management of hemophilia. Haemophilia. 2013;19:e1–47. doi:10.1111/j.1365-2516.2012.02909.x
2. World Federation of Hemophilia. Report on the Annual Global Survey 2020; 2021.
3. Oldenburg J. Optimal treatment strategies for hemophilia: achievements and limitations of current prophylactic regimens. Blood. 2015;125(13):23–27. doi:10.1182/blood-2015-01-528414
4. Yang R, Poon MC, Luke KH, Zhao Y, Wu J. Building a network for hemophilia care in China: 15 years of achievement for the hemophilia treatment center collaborative network of China. Blood Adv. 2019;3(Supplement 1):34–37. doi:10.1182/bloodadvances.2019GS121524
5. Chinese Society of Hematology Thrombus and Hemostasis Group, Chinese Hemophilia Cooperative Group. Chinese guidelines on the treatment of hemophilia (version 2020). Chin J Hematol. 2020;41:265–271. doi:10.3760/cma.j.issn.0253-2727.2020.04.001
6. Health Commission In China MOSA. The national rare disease in China; 2018.
7. Chen W, Zhang L. Reimbursement landscape and policy development for rare diseases in China: a case study of hemophilia. Value Health. 2013;16(3):A207–8. doi:10.1016/j.jval.2013.03.1049
8. Poon MC, Luke KH. Haemophilia care in China: achievements of a decade of world federation of hemophilia treatment centre twinning activities. Haemophilia. 2008;14(5):879–888. doi:10.1111/j.1365-2516.2008.01821.x
9. Huang SH, Li ZT, Liu Y, et al. Comparison of short-term tertiary prophylaxis at low-dose and intermediate-dose for adults with severe hemophilia a in China. Blood. 2015;126:23.
10. Zhao H, Yang L, Long C, et al. Hemophilia care in China: review of care for 417 hemophilia patients from 11 treatment centers in Shanxi Province. Expert Rev Hematol. 2015;8:543–550. doi:10.1586/17474086.2015.1043263
11. Hua B, Yan Z, Zhu T, Wang S, Zhao Y. The frequency of factor VIII inhibitors in hemophilia A patients in China: a single-center experience over seven years. Haemophilia. 2008;14:50–51. doi:10.1111/j.1365-2516.2007.01560.x
12. Fang Y, Zhang X, Li A, Zhang X, Teng B. Hemophilia patient databases at the Shandong Hemophilia Centre of China. Haemophilia. 2014;20:36. doi:10.1111/hae.12423
13. Dou XQ, Poon MC, Yang RC. Haemophilia care in China: achievements in the past decade. Haemophilia. 2020;26(5):759–767. doi:10.1111/hae.14101
14. Zhou T, Guan H, Liu GG, Ma A. Health-related quality of life for disease population in China based on EQ-5D: a systematic review. Chinese J Evidence-Based Med. 2016;16(2):135–142. doi:10.1186/s13020-021-00543-x
15. Zhang H, Huang J, Kong X, Ma G, Fang Y. Health-related quality of life in children with haemophilia in China: a 4-year follow-up prospective cohort study. Health Qual Life Outcomes. 2019;17(4):23–29. doi:10.1186/s12955-019-1083-3
16. Wu R, Sun J, Xiao J, et al. A prospective study of health-related quality of life of boys with severe haemophilia A in China: comparing on-demand to prophylaxis treatment. Haemophilia. 2017;23(3):430–436. doi:10.1111/hae.13198
17. Haque Q, Feng X, Li C. Assessment of intracranial hemorrhage demographics in children with hemophilia: a multicentre study in China. Blood. 2016;128(22):4981. doi:10.1182/blood.V128.22.4981.4981
18. Xue F, Yang R. Update on the national hemophilia registry of China. Haemophilia. 2014;20:33.
19. Sun J, Zhao Y, Yang R, et al. The demographics, treatment characteristics and quality of life of adult people with haemophilia in China – results from the HERO study. Haemophilia. 2017;23(1):89–97. doi:10.1111/hae.13071
20. Song X, Zhong J, Xue F, Chen L, Yang R. An overview of patients with haemophilia A in China: epidemiology, disease severity and treatment strategies. Haemophilia. 2020;2020:1.
21. Luo N, Liu G, Li M, et al. Estimating an EQ-5D-5L Value Set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
22. Mahlangu JN. Haemophilia care in South Africa: 2004–2007 look back. Haemophilia. 2009;15(1):135–141. doi:10.1111/j.1365-2516.2008.01807.x
23. Lorenzato CS, Santos RB, Fagundes GZZ, Ozelo MC. Haemophilia Experiences, Results and Opportunities (HERO study) in Brazil: assessment of the psychosocial effects of haemophilia in patients and caregivers. Haemophilia. 2019;25:640–650. doi:10.1111/hae.13774
24. Curtis R, Baker J, Riske B, et al. Young adults with hemophilia in the U.S.: demographics, comorbidities, and health status. Am J Hematol. 2015;90:S11–S16. doi:10.1002/ajh.24218
25. Jain A, Mehta S, Joshi M, et al. Patient reported outcomes to assess quality of hemophilia care in north India - results of a global partnership. Blood. 2016;128:22.
26. Witkop M, Guelcher C, Forsyth A, et al. Treatment outcomes, quality of life, and impact of hemophilia on young adults (aged 18–30 years) with hemophilia. Am J Hematol. 2015;90:S3–S10. doi:10.1002/ajh.24220
27. Qu Y, Zhan S, Dong P. The prevalence and treatment status of hemophilia in India, Russia, Taiwan and Turkey: a systematic review and meta analysis. Value Health. 2012;15(7):A679–A679. doi:10.1016/j.jval.2012.08.456
28. Zhang L, Zhang P, Chen W. Treatment regimens, patient reported outcomes and health-related quality of life in children with moderate and severe hemophilia A in China: using real-world data. Orphanet J Rare Dis. 2023;18(1). doi:10.1186/s13023-023-02835-x
29. Krasnova L, Vorobiev P, Vorobiev A. Epidemiology of hemophilia in Russia for 2007–2017: results of standardization use in therapy. Value Health. 2019;22:S342–S342. doi:10.1016/j.jval.2019.04.1670
30. McLaughlin P, Hurley M, Chowdary P, Stephensen D, Khair K. How does a lifetime of painful experiences influence sensations and beliefs about pain in adults with severe haemophilia? A qualitative study. Disabil Rehabil. 2022;44(26):8412–8419. doi:10.1080/09638288.2021.2018053
31. Krasnova L, Vorobiev P, Vorobiev A, Holownia M. Economics and quality of life of patients with hemophilia in Russia for 2007–2017: results of standardization use in therapy. Value Health. 2019;22:S341–S341. doi:10.1016/j.jval.2019.04.1667
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.