")
Back to Journals » Clinical Ophthalmology » Volume 16
Orbital Fractures and Risk Factors for Ocular Injury
Authors Zhong E, Chou TY , Chaleff AJ, Scofield-Kaplan SM, Perzia BM, Naqvi J, Hou W
Received 25 September 2022
Accepted for publication 6 December 2022
Published 14 December 2022 Volume 2022:16 Pages 4153—4161
DOI https://doi.org/10.2147/OPTH.S391175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eric Zhong,1 Timothy Y Chou,1 Alec J Chaleff,1 Stacy M Scofield-Kaplan,1 Brittany M Perzia,1 Jaffer Naqvi,1 Wei Hou2
1Department of Ophthalmology, Renaissance School of Medicine at Stony Brook University, Stony Brook, NY, USA; 2Department of Epidemiology and Biostatistics, Renaissance School of Medicine at Stony Brook University, Stony Brook, NY, USA
Correspondence: Timothy Y Chou, Stony Brook University Medical Center, Department of Ophthalmology, HSC L2, Room 152, Stony Brook, NY, 11794, USA, Tel +1 631-444-1131, Fax +1 631-444-4089, Email [email protected]
Purpose: To identify factors predictive of serious ocular injury requiring urgent consultation by ophthalmology in patients presenting with blunt trauma orbital fractures.
Methods: This is a retrospective study of adult patients diagnosed with orbital fractures after blunt trauma at a university medical center emergency room. Patient records were examined over a three-year period. Data including mechanism of injury, fracture location, ocular symptoms, and examination findings were recorded. Ocular injuries were divided into three levels of severity: mild, moderate, and severe. Fracture characteristics, patient demographics, and examination findings were analyzed using multinomial regression to identify risk factors for more severe injury.
Results: One hundred and eighty-six patients met inclusion criteria. For 29.6% of patients, urgent ophthalmologic consultation was required. Ruptured globes occurred in 2.2% of injuries. There was a statistically significant association between severe ocular injury and three examination findings: poor vision (OR 14.5; p < 0.001), afferent pupillary defect (OR 44.8; p < 0.001), and abnormal pupillary reaction (OR 28.0; p < 0.001). Likewise, blurry vision (OR 3.6; p = 0.018), ocular pain (OR 3.7; p = 0.011), and facial pain (OR 4.4; p = 0.031) were also associated with an increased risk of severe ocular injury. Abnormal pupillary reaction was associated with moderate injury (OR 4.5; p = 0.041). Demographic factors, mechanism of injury, anti-coagulant use, fracture location, diplopia, no documented vision, subconjunctival hemorrhage, chemosis, and motility restriction were not associated with injury severity.
Conclusion: Most patients who presented to the emergency room with an orbital fracture did not require urgent ophthalmologic consultation. The presence of blurry vision, ocular pain, facial pain, poor vision, and afferent pupillary defect significantly increased the odds of severe injury. Abnormal pupillary reaction was associated with both moderate and severe injury.
Keywords: orbital fracture, ocular injury, globe rupture, ocular trauma
Introduction
From 2001 to 2014, trauma to the orbit accounted for 25% of inpatient admissions due to an ophthalmic disorder in hospitals throughout the United States.1 The incidence of orbital floor fractures in the US increased by 47%, from 2006 to 2017.2 The presence of severe ocular injury in patients with orbital fractures in an emergency setting ranges from 2.7% to 13.7%.3–7 This variability in incidence may be related to differences in the criteria for classifying severe ocular injury. For example, some papers define it as any injury with a risk of vision loss, while others list out every diagnosis that falls into the severe category. In general, the occurrence of severe ocular injury and the need for emergent surgery in the setting of orbital fracture is low.8,9 Proper identification of clinical factors predicting underlying severe ocular injury is important in an emergency setting since it can guide management decisions and therefore affect clinical outcome. Prior studies have investigated the predictive value of many exam findings. Poor visual acuity (VA) has been frequently cited as a risk factor for ocular injury; however, the precise cutoff of poor visual acuity varies from LogMAR VA worse than 0.2 to inability to count fingers.4,6,10,11 The presence of an afferent pupillary defect (APD) has also been identified as a risk factor for ocular injury.10 Findings on imaging, including the radiographic depth of fracture and location of the fracture, particularly if the fracture extends into the posterior third of the orbit or if it involves the medial wall and orbital floor, can be suggestive of ocular injury.10,12 Likewise, complex fractures, including Le Fort II and III fractures, identified on imaging have been noted to increase the risk of ocular injury.13 The mechanism of injury, specifically penetrating trauma, has also been associated with a greater likelihood of injury.10 Ocular symptoms such as blurry vision, pain, and photophobia have been evaluated more recently as predictive factors.14,15 Diplopia is one symptom that has long been thought of as an indicator of extraocular muscle entrapment and suggests ocular injury.11,16 More recent studies by Richani et al have suggested that pain with eye movements, blurry vision, and motility restriction were predictive of severe ocular injury.15 Rossin et al integrated poor VA, diplopia, mechanism of injury, and location of fracture into an algorithm that, when combined with additional findings of chemosis and conjunctival hemorrhage, can foretell a higher risk of “substantial” ocular injury, defined as injuries requiring urgent or close follow up.16 Though these studies have identified several risk factors for severe injury, they differ regarding which factors are considered the most prognosticative.
In this study, we examined the strength of association between ocular injuries and several predictive factors – including some less commonly studied characteristics, such as anti-coagulant (AC) and anti-platelet (APT) drug use and the absence of a VA on presentation – in patients diagnosed with orbital fractures in the Emergency Department (ED). Based on our analysis, we determined which patients are most likely to have severe ophthalmic injuries requiring urgent ophthalmologic consultation.
Materials and Methods
This study was approved by the Stony Brook University Institutional Review Board. It is Health Insurance Portability and Accountability Act compliant with protection of individually identifiable information and adheres to the tenets of the Declaration of Helsinki as amended in 2013. We retrospectively reviewed the medical records of patients who presented to the ED at Stony Brook University Hospital, a level I trauma center, with one or more orbital fractures between March 21, 2017 and March 21, 2020. A total of 1089 encounters were identified from a search of the electronic medical record using orbital fracture ICD-10 codes – any encounter coded with S02.12, S02.3, S02.83, S02.84, and all of the more specific codes below them were included. Patients were excluded if they were less than 18 years old, had a history of penetrating trauma, did not have an ophthalmologic evaluation within 24 hours of arrival, or if their fracture was not confirmed with computed tomography. Information on patient demographics, mechanism of injury, medication use, symptoms, fracture characteristics (including location and examination, number of walls), and immediate interventions was obtained from the initial ophthalmology consultation. Mechanisms of injury were classified as, “assault”, “falls”, “motor vehicle accident”, or “other blunt trauma.” “Other blunt trauma” included sports injuries, accidents caused by blunt objects, and injuries that did not fit into the previous three categories.
Patients were differentiated based on presence or absence of symptoms. “Symptomatic” patients had at least one of the following symptoms: blurry vision, a sensation of pressure, ocular pain, facial pain, facial numbness, pain specifically with extraocular movements, diplopia, nausea, floaters, or photopsias. Blurry vision, ocular pain, pain specifically with extraocular muscle movements, facial pain, headache, and diplopia were additionally studied as stand-alone symptoms. “Asymptomatic” patients lacked any of these complaints.
VA was measured at near with a Rosenbaum pocket vision screener. Consistent with prior studies, VA of 20/40 or worse was defined as poor vision.6,15 If the VA could not be obtained from the patient – due to intubation, lack of cooperation, or altered mental status – it was recorded as “no documented vision”. “Abnormal pupillary reaction” was defined as presence of an APD, a questionable APD on exam, or an unreactive pupil. If pupils were obscured, or the presence of an APD could not be determined, such patients were excluded from analysis. Orbital wall fractures were categorized by the location of the fracture (“floor”, “medial wall”, “lateral wall”, or “roof”), and by the number of walls fractured.
Acuity of consultation was based on injury severity, which was based on previous literature.14–16 Patients were categorized by their most severe injury. “Severe” injuries comprised hyphema, globe rupture, vitreous hemorrhage, traumatic optic neuropathy, and retrobulbar hemorrhage. Since these injuries are potentially vision-threatening or may require surgical intervention, “urgent” ophthalmologic consultation was felt to be needed, without delay. “Moderate” injuries (eyelid laceration, conjunctival laceration, corneal abrasion, traumatic iritis, microhyphema, iris sphincter tear, commotio retinae, retinal hemorrhage) required “expedited” ophthalmologic evaluation within a few hours, but not necessarily immediately.16 The remaining patients with “mild” injuries (periorbital swelling, periorbital ecchymosis, eyebrow laceration or abrasion, conjunctival injection, chemosis, and subconjunctival hemorrhage) could undergo more routine or “non-urgent” ophthalmologic consultation. Such non-urgent consultation should still be within 24 hours, in our estimation, for an eye specialist to confirm the initial impression of only mild ocular injury. At times in this paper, we have found it useful to refer to the combination of “severe” and “moderate” ocular injuries as “serious” injuries.
The incidences of injuries and specifically of globe rupture were determined. We further sought to ascertain if AC or APT drug use was associated with an increased risk of “severe ocular hemorrhage”, defined as presence of hemorrhagic chemosis, hyphema, vitreous hemorrhage, or retrobulbar hemorrhage. The relationship between different risk factors – age, race, mechanism of injury, AC or APT use, number of walls fractured, fracture location, subconjunctival hemorrhage, chemosis, motility restriction, and lack of a documented VA – and injury severity was analyzed for statistical significance using the Chi-Square test of independence or Fisher’s Exact Test. A multinomial logistic regression analysis was used to determine the odds ratios (OR) of the different risk factors for mild, moderate, and severe ocular injuries. For the multinomial analysis, mild injuries served as the reference category. All statistical analyses were performed using SPSS Version 28 for Windows (Armonk, NY, USA: IBM Corp).
Results
A total of 186 patients who presented to the ED with one or more orbital fractures met our study criteria. Patients were seen by an ophthalmologist, on average, within eight hours of presentation to the ED (range 0.5–24 hours). Demographic data and clinical characteristics of their injuries along are listed in Table 1 and the results of the multinomial regression analysis are listed in Table 2. Average patient age was 54.6 years (range 18–101 years), with 73.7% male and 76.3% Caucasian. Age, sex, and race were not statistically associated with an increased risk of ocular injury (p = 0.135, p = 0.567, and p = 0.323, respectively), despite all globe ruptures occurring in Caucasian patients over the age of 70. However, patients greater than 55 years of age did have a two-fold increase in the odds of severe injury (Table 2). The most common cause for an orbital fracture was fall (n = 82, 44.1%), followed by assault (n = 40, 21.5%), motor vehicle accident (n = 37, 19.9%), and other blunt trauma (n = 27, 14.5%). The various mechanisms of orbital trauma did not factor into severity of ocular injury (p = 0.255 for severe injuries; p = 0.331 for moderate injuries). Thirty-eight patients (20.4%) were taking some form of ACs or APTs – specifically, aspirin, apixaban, warfarin, ticagrelor, or clopidogrel – at the time of their injury. The use of ACs and APTs did not increase the odds of severe or moderate ocular damage (p = 0.872 and p = 0.415, respectively) or of severe ocular hemorrhage (OR 0.844; 95% CI: 0.288–3.127; p = 0.800).
 |
Table 1 Demographics and Clinical Characteristics of Patients with Orbital Fractures |
 |
Table 2 Multinomial Regression Analysis of Risk Factors for Ocular Injuries |
Symptomatic patients accounted for 47.8% of study patients, and had increased odds of severe ocular injury, with an OR of 4.1 (95% CI: 1.3–13.2; p = 0.016). When symptomatic patients were sub-divided by their reported complaints, only blurry vision (OR 3.6; 95% CI: 1.2–10.4; p = 0.018), ocular pain (OR 3.7; 95% CI: 1.3–10.0; p = 0.011), and facial pain (OR 4.4; 95% CI: 1.1–16.8; p = 0.031) were each significantly associated with severe ocular injury, necessitating urgent ophthalmologic consultation. None of the symptoms listed in Table 2, statistically, were associated with moderate injury; blurry vision, however, increased the odds of moderate injury 1.5-fold, ocular pain increased it 1.8-fold, and facial pain increased it 1.4-fold. Pain with extraocular movements and visual diplopia did not point to severe ocular injury (p = 0.660 and p = 0.623, respectively).
Poor vision was determined to be significantly associated with severe ocular injury, with an OR of 14.5 (95% CI: 3.9–54.2; p < 0.001). Poor vision also increased the chances for moderate injury, but by an amount that was not statistically significant (Table 1). Twenty-eight patients lacked a documented VA and were not included in the analysis of VA. Nevertheless, having no documented VA was calculated to increase the odds of severe ocular injury by 1.6 times (p = 0.087). Regarding the pupillary exam, 5.4% of patient had an APD, 1.6% had a questionable APD, and 1.6% of study patients had unreactive pupils. Further breakdown revealed that an APD was present in 1.5% of patients with mild injury, 3.1% with moderate injury, and 30.4% of patients with severe injury. A finding of APD was statistically associated with severe ocular injury with an OR of 44.8 (95% CI 8.2–244.8; p < 0.001), but not with moderate ocular injury (p = 0.559). Abnormal pupillary reaction, on the other hand, significantly correlated with both severe and moderate ocular injury, with an OR of 28.0 (95% CI 7.1–111.1; p < 0.001) and 4.5 (95% CI 1.1–19.1; p = 0.041), respectively; these patients required urgent and expedited consultation by ophthalmology. All patients requiring emergent surgical intervention had either an abnormal pupillary reaction or pupils that could not be evaluated. Like pain with eye movement and diplopia, motility restriction was not found to be statistically associated with injury severity (p = 0.716). Of note, extraocular muscle entrapment did not develop in any of the study patients.
The orbital floor was the most fractured site (53.5%), followed by the medial wall (21.6%), lateral wall (15.6%), and orbital roof (9.2%). Of the orbital floor fracture cases, 86 (46.2%) involved the left orbital floor, and 82 (44.1%) the right orbital floor, while 18 (9.7%) were bilateral. Just over half of injuries involved a single wall fracture, with the others involving multiple walls. The orbital floor had the lowest odds ratio of severe ocular injury at 0.6 (p = 0.291) and medial wall fractures had a relatively higher odds ratio of severe ocular injury at 1.5 (p = 0.416). The overall incidence of globe rupture was 2.2% in our study. Globe rupture only occurred in the setting of medial wall or orbital floor fractures; further, having a medial wall fracture doubled the odds of globe rupture (OR of 2.1; p = 0.468). Despite this predilection, there was ultimately no statistically significant relationship between location of fracture and seriousness of ocular injury. The number of walls involved, whether single or multiple, also did not affect the injury severity (p = 0.276).
Fifty-five patients (29.6%) sustained serious ocular injuries, of which twenty-three (12.4%) were severe, requiring urgent ophthalmologic consultation (Table 3). Hyphema (8%) was the leading type of severe injury. Five patients (2.7%) with severe injuries underwent emergent surgical intervention – four (2.2%) with ruptured globes and one with orbital compartment syndrome from retrobulbar hemorrhage, requiring a lateral canthotomy. Commotio retinae (5.9%) was the most frequent moderate injury diagnosed. Among patients with mild injury, nearly two-thirds had periorbital ecchymosis. The absence of the following – ocular symptoms (p = 0.016), poor vision (p < 0.001), APD (p < 0.001), or abnormal pupillary reaction (p < 0.001) – was significantly associated with mild injuries that did not necessitate urgent evaluation by ophthalmology.
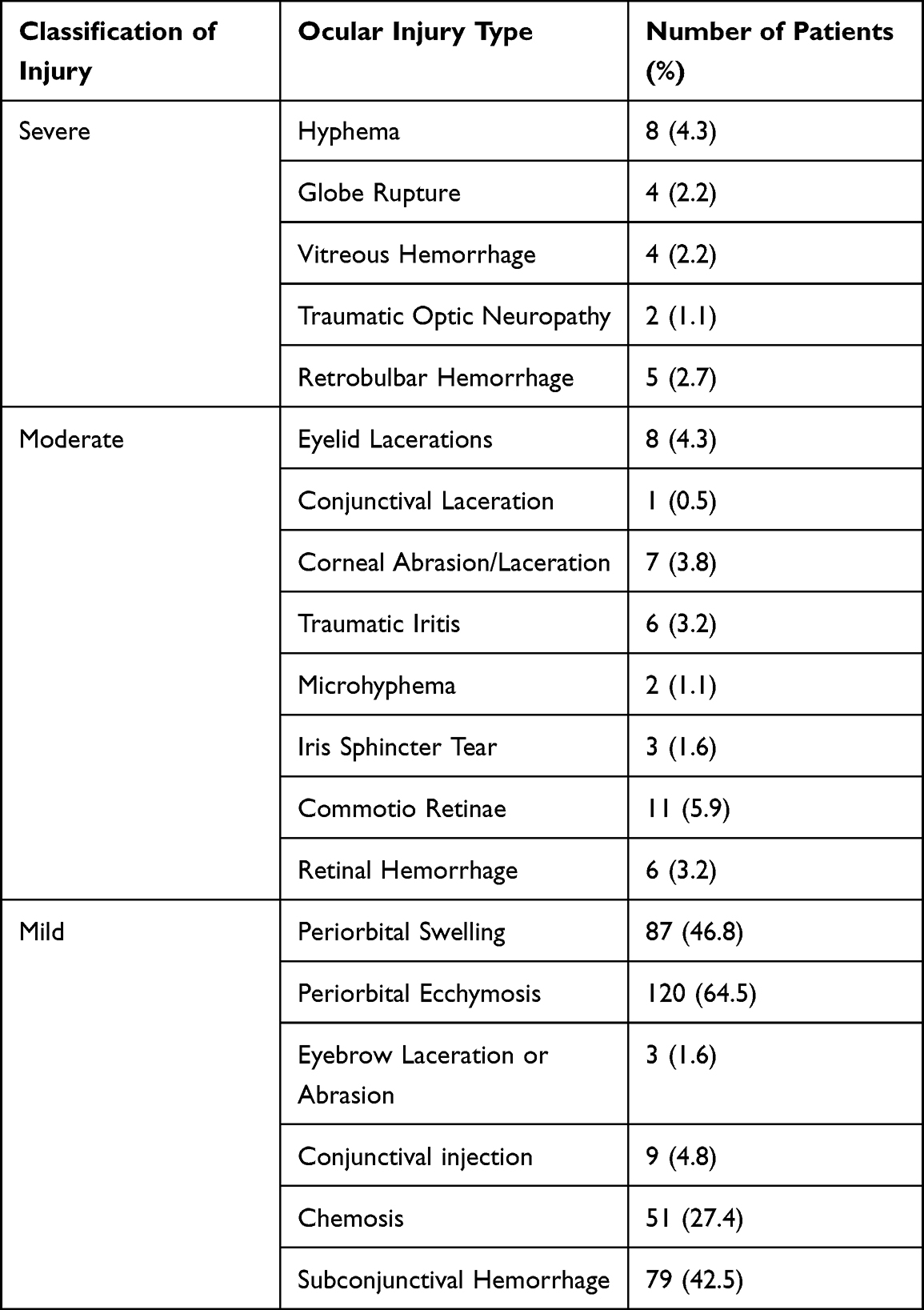 |
Table 3 Classification of Ocular Injuries into Severe, Moderate, and Mild |
Discussion
Although most orbital fractures are not associated with significant ocular injury, some can still lead to potentially vision-threatening complications. We have looked at a variety of factors in this study, including some less commonly studied patient risk factors, to determine if they might increase the chance of severe ocular injury. We found that our incidence of severe ocular injury (12.7%) and of globe rupture (2.2%) were similar to previously reported incidences.10,15,16 Certain specific symptoms, poor vision, and abnormal pupillary reaction are associated with severe ocular injury in patients with blunt mechanism orbital fracture. Such patients require urgent ophthalmologic consultation in order to be evaluated for associated intraocular injuries.
Our investigation reemphasizes the importance of considering patient symptoms when stratifying the urgency of ophthalmologic consultation in the setting of orbital fracture;17 visually asymptomatic patients were less likely to have severe ocular injury. “Blurry vision”, “ocular pain”, and “facial pain” were independently and significantly associated with severe ocular injury. Blurry vision, ocular pain, and facial pain additionally raised the odds ratio of moderate injury by 1.5, 1.8, and 1.4 times, respectively, though not reaching statistical significance. Poor vision is another independent risk factor for severe ocular injury. Although the definition of poor vision varies among studies, we have found that a VA of worse than 20/40 is associated with severe injuries. Many studies exclude patients that do not have a documented VA. In our study, we found that patients without documented VA have a more than two-fold increase in odds of severe ocular injury, and of moderate injury by 1.7 times. However, this was not to a level of statistical significance. Abnormalities on the pupillary exam are associated with greater odds of severe injury. These patients require urgent consultation by ophthalmology. Abnormal pupillary reaction was statistically associated with moderate injuries as well; consultation in these cases should still be without delay, due to the possibility of a more severe injury. An abnormal pupillary exam was also present in all study patients who needed emergent surgery. Absence of these factors was significantly associated with mild injury; ophthalmologic consultation for such patients can be provided on a non-urgent basis.
From our analysis we failed to identify an increased risk of ocular injury based on demographic factors, fracture characteristics, and mechanism of injury. These factors are therefore not as helpful in determining the need for ophthalmologic consultation. Fracture characteristics did not significantly affect the severity of ocular injury. We were unable to identify statistically significant associations based on location or complexity of fractures, such as a multiple wall orbital fracture. However, we determined that the orbital floor had the lowest odds of severe injury, while lateral wall fractures had a relatively higher odds of severe injury. The highest odds occurred with medial wall fractures. Our findings regarding predictive value of location are similar to those of Thurston et al.18
Although many of our findings are consistent with past studies, some of our risk factors did not have the same predictive value. Diplopia has been noted by some to potentially indicate more severe ocular injury.11,16 By contrast, when we analyzed diplopia as an isolated symptom, we did not establish this same association. Other investigators have suggested that pain with eye movements and restricted motility are predictive of severe ocular trauma.11,16 In our study, pain with eye movements and restricted motility were also not associated with severe injury, likely due to the absence of extraocular muscle entrapment in our cohort.
Several orbital fracture studies have determined injury mechanism to factor into severity of ocular injury, but with varying conclusions.10,15,16 Andrews et al observed that penetrating trauma caused severe ocular injury more often than blunt force trauma.10 Rossin et al identified blunt trauma with a foreign object as a risk factor in their algorithm for predicting substantial ocular injury.16 Contrary to these studies, we did not connect the mode of trauma to severity of ocular injury, perhaps due in part to our exclusion of penetrating trauma. AC and APT use also did not increase risk of severe ocular hemorrhage or serious ocular injury.
The design of this investigation includes a representative patient population, builds upon the use of symptoms to calculate risk, and quantifies the association of pertinent risk factors with the degree of injury in the setting of orbital fracture. It is the first study to our knowledge that additionally examines whether factors such as AC and APT use, or the state of being unable to have visual acuity measured, increase the likelihood of serious or severe ocular injury. Limitations of this study include that it is a retrospective analysis and possibly subject to selection bias. There is also a lack of longitudinal data, as no baseline or long-term ophthalmologic evaluations were included in the analysis. Future prospective studies with longitudinal data and meta-analyses may provide additional guidance for clinical decision-making in the setting of orbital fractures.
Conclusion
Most patients who present to the emergency room with an orbital fracture do not require immediate or urgent ophthalmologic consultation. This retrospective study identified, however, that the presence of blurry vision, ocular pain, facial pain, poor vision, and APD significantly increase the odds of a severe ocular injury. Abnormal pupillary reaction is associated with both severe and moderate injury. Presence of these findings should prompt an urgent consultation to ophthalmology. Ocular symptoms, VA, and the pupil exam should be a significant focus of the initial evaluation of a patient with blunt ocular trauma. Consideration of these factors can help in the triage of blunt trauma orbital fractures, by enabling clinicians to predict the likelihood of serious ocular injury and determine the acuity of ophthalmologic consultation.
Abbreviations
VA, Visual Acuity; APD, Afferent pupillary defect; ED, Emergency Department; AC, anticoagulant; APT, anti-platelet.
Ethics Approval and Informed Consent
This study was approved by the Stony Brook IRB (Stony Brook, NY, IRB# 2020-00203) and adhered to the tenets outlined in the Declaration of Helsinki. The study was HIPAA-compliant with protection of individually identifiable information. Patient data were de-identified prior to analysis.
Consent for Publication
We have not provided any images, videos, or recordings that require consent.
Acknowledgments
We would like to thank Chaowei Tsai for identifying patients in the EMR system.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; participated in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have reviewed and agreed on the journal to which the article has been submitted; have reviewed and agreed on all versions of the manuscript before submission and during revision; and agree to be accountable for all aspects of the work.
Funding
The authors have no sources of funding or financial interests to declare for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Iftikhar M, Junaid N, Lemus M, et al. Epidemiology of primary ophthalmic inpatient admissions in the United States. Am J Ophthalmol. 2018;185:101–109. doi:10.1016/j.ajo.2017.10.014
2. Iftikhar M, Canner JK, Hall J, et al. Characteristics of orbital floor fractures in the United States from 2006 to 2017. Ophthalmology. 2021;128:463–470. doi:10.1016/j.ophtha.2020.06.065
3. Luce EA, Tubb TD, Moore AM. Review of 1000 major facial fractures and associated injuries. Plast Reconstr Surg. 1979;63:26–30. doi:10.1097/00006534-197901000-00005
4. Al-Qurainy IA, Stassen LF, Dutton GN, El-Attar KFM, EI-Attar A. The characteristics of midfacial fractures and the association with ocular injury: a prospective study. Br J Oral Maxillofac Surg. 1991;29:291–301. doi:10.1016/0266-4356(91)90114-K
5. Ross M, El-Haddad C, Deschenes J. Ocular injury in orbital fractures at a level I trauma center. Can J Ophthalmol. 2017;52:499–502. doi:10.1016/j.jcjo.2017.01.013
6. Layton C. Factors associated with significant ocular injury in conservatively treated orbital fractures. J Ophthalmol. 2014;2014:412397. doi:10.1155/2014/412397
7. Ho TQ, Jupiter D, Tsai J, Czerwinski M. The incidence of ocular injuries in isolated orbital fractures. Ann Plast Surg. 2017;78:59–61. doi:10.1097/SAP.0000000000000748
8. Dal Canto AJ, Linberg JV. Comparison of orbital fracture repair performed within 14 days versus 15 to 29 days after trauma. Ophthalmic Plast Reconstr Surg. 2008;24:437–443. doi:10.1097/IOP.0b013e31818aac9b
9. Boyette JR, Pemberton JD, Bonilla-Velez JB. Management of orbital fractures: challenges and solutions. Clin Ophthalmol. 2015;9:2127–2137. doi:10.2147/OPTH.S80463
10. Andrews BT, Jackson AS, Nazir N, Hromas A, Sokol JA, Thurston TE. Orbit fractures: identifying patient factors indicating high risk for ocular and periocular injury. Laryngoscope. 2016;126:S5–11. doi:10.1002/lary.25805
11. Dutton GN, Al-Qurainy IA, Stassen LF, Titterington DM, Moos FK, El-Attar E. Ophthalmic consequences of mid-facial trauma. Eye. 1992;6:86–89. doi:10.1038/eye.1992.17
12. Khojastepour L, Moannei M, Eftekharian HR, Khaghaninejad MS, Majhoori-Ghasrodashti M, Tavanafar S. Prevalence and severity of orbital blowout fractures. Br J Oral Maxillofac Surg. 2020;58:e93–97. doi:10.1016/j.bjoms.2020.07.001
13. Petro J, Tooze FM, Bales CR, Baker G. Ocular injuries associated with periorbital fractures. J Trauma. 1979;19:730–733. doi:10.1097/00005373-197910000-00003
14. Mellema PA, Dewan MA, Lee MS, Smith SD, Harrison AR. Incidence of ocular injury in visually asymptomatic orbital fractures. Ophthal Plast Reconstr Surg. 2009;25:306–308. doi:10.1097/IOP.0b013e3181aa9a73
15. Richani K, Do T, Merrit HA, Pfeiffer ML, Chuang AZ, Phillips ME. Screening criteria for detecting severe ocular injuries in the setting of orbital fractures. Ophthal Plast Reconstr Surg. 2019;35:609–614. doi:10.1097/IOP.0000000000001422
16. Rossin EJ, Szypko C, Giese I, Hall N, Gardiner MF, Lorch A. Factors associated with increased risk of serious ocular injury in the setting of orbital fracture. JAMA Ophthalmol. 2021;139:77–83. doi:10.1001/jamaophthalmol.2020.5108
17. Etheridge T, Brintz BJ, Jensen MS, et al. Incidence and severity of asymptomatic ocular injury in adult and pediatric orbital fractures. Orbit. 2022;8:1–6. doi:10.1080/01676830.2022.2095648
18. Thurston TE, Jackson AS, Nazir N, Crowe D, Andrews BT. Risk assessment of Isolated single wall orbital fractures and eye injury. J Craniofac Surg. 2018;29:943–945. doi:10.1097/SCS.0000000000004412
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.