")
Back to Journals » Open Access Surgery » Volume 17
Open Wound Reconstruction of the Thumb Tip: A Review of Current Literature and Case Reports
Authors Cortes R , Datiashvili RO
Received 7 September 2023
Accepted for publication 21 February 2024
Published 23 February 2024 Volume 2024:17 Pages 43—53
DOI https://doi.org/10.2147/OAS.S417999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Ricardo Cortes, Ramazi O Datiashvili
Department of Surgery, Division of Plastic Surgery, Rutgers New Jersey Medical School, Newark, New Jersey
Correspondence: Ricardo Cortes, Tel +8059106232, Email [email protected]
Abstract: The thumb is regarded as the most important digit of the hand, accounting for approximately 40% of the entire function of the hand, loss of a functional thumb leads to loss of key functions and patient autonomy. When the nature of the injury and the amputated part allow it, replantation is the standard of care. However, in cases of tip injury, where the amputated tissue is destroyed or otherwise rendered unusable, other reconstructive methods are used. It is imperative to maintain as much function and sensation as possible while restoring as much lost function and sensation as possible. This includes preservation of the interphalangeal (IP) joint, achieving good soft tissue coverage and restoring motor and sensory functions. With a variety of techniques described in the literature, thumb reconstruction proves to be a formidable task. Moreover, the technique selected must minimized complications associated with reconstruction such as hypersensitivity, contracture deformities, poor aesthetics, limited range of motion and insufficient coverage. We review and summarize the techniques of revision amputation, Moberg advancement flap, FDMA flaps, free tissue transfer from the great toe and non-operative management. We include case reports that highlight the benefits and limitations of some of these techniques.
Keywords: thumb reconstruction, replantation, amputation, thumb flaps
Introduction
The thumb is regarded as the most important digit of the hand, accounting for approximately 40% of the entire function of the hand.1 Three finger pinch, key pinch, grip strength and opposition help to accomplish many tasks of routine daily life; loss of a functional thumb leads to loss of patient autonomy.2 In 2018, the CDC reported that approximately 13% of all emergency department visits, over 3 million total, were due to injuries of the wrist, hand and fingers.3 Clearly, there is a profound need to properly reconstruct thumb injuries.
Key functional components of the thumb include adequate length, joint stability, range of motion, tactile sensation, intact nailbed, soft tissue coverage, and well-controlled pain.4,5 Failure to address any one of these components leads to significant functional impairment and constitutes a serious injury. For instance, preserving thumb sensation requires the preservation or restoration of a high density of Vater-Pacini, failure to consider this fact will lead to a loss of the specific sensory ability of the thumb.6
Replantation is the standard of care when there is sufficient tissue to replant and when the nature of the injury is amenable to it.7 However, in cases of tip injury, where the skin and soft tissue are lost or destroyed (ie, crush injuries) other reconstructive methods must be employed. Furthermore, there may not be blood vessels of adequate caliber to allow reliable blood vessel anastomosis.
Goals of reconstruction follow the principles of repairing like with like, especially with regard to the unique nature of glabrous volar thumb skin. It is imperative to maintain all intact key functional components, and to restore as many lost key functional components as possible. Here, some of the most popular and effective methods are reviewed along with case reports outlining our preferred techniques and applications.
Cases
Patient Case 1—FDMA Flap
This 44-year-old patient initially presented with a total thumb tip amputation. After explanation of risks and benefits, the patient decided to move forward with an attempt at replantation. Upon replantation, only arterial anastomosis was possible; no veins were anastomosed due to their extremely small diameter. Postoperatively, IV heparin was given to establish growth of new vessels into the thumb for provision of venous outflow. The patient remained hospitalized to monitor the progress of the tip.
On the 8th day post operation, the patient became concerned of the socio-economic impact that a prolonged hospitalization would have on him and so he desired the thumb tip amputated despite its viability. After deliberation and discussion with the patient, we moved forward with an operative amputation of the thumb tip, after which the patient was discharged.
A week after discharge, the patient presented to our clinic and was offered reconstruction of the open wound of his thumb stump utilizing the FDMA kite flap. The wound to be covered measured 2.5 cm × 2.5cm with some bony exposure (Figure 1A).
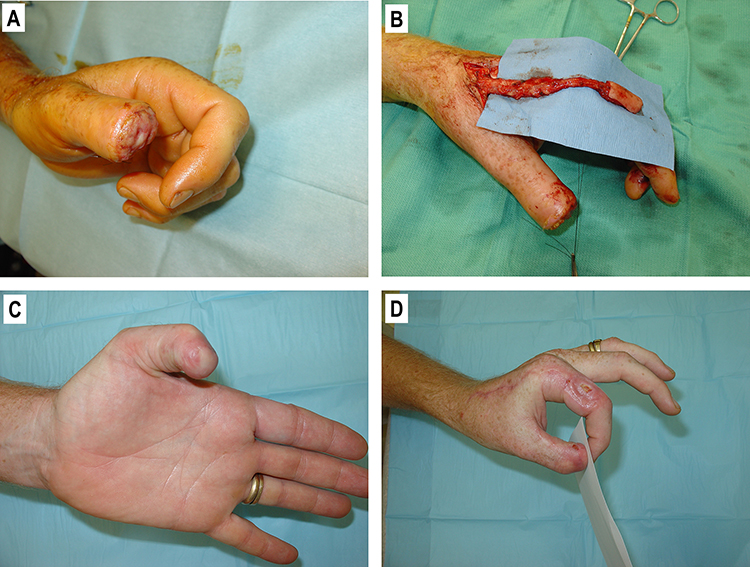 |
Figure 1 (A) Open wound of the tip of the thumb, 2.5cm x 2.5cm. (B) The kite flap raised over the dorsal index finger. (C) View of the thumb 32 days after surgery. (D) Patient is able to perform pinch and opposition. |
The patient was taken to the OR where a 2.5 cm × 3 cm flap was traced out over the dorso-radial skin of the proximal phalanx of the index finger and the flap dissected. An incision was then extended proximally towards the metacarpal region. Micro scissors were used to dissect the subcutaneous tissue, and a neurovascular pedicle of approximately 8cm was mobilized (Figure 1B).
Dissection of the thumb recipient site was carried out with #15 blade: skin edges were gently raised on all sides of the defect. A tunnel extending from the metacarpal area to the base of the thumb was created, and incision was made along the ulnar side of the thumb to pass the vascular pedicle of the flap through to the recipient site. The flap was inset, and skin flaps along the thumb incision were mobilized to avoid compression of the vascular pedicle. Closure of the skin along the incisions and around the flap was achieved with 4–0 nylon.
The left groin area was then utilized as a donor site for the full thickness skin graft to the index finger. A 3cm incision was made and a scalpel used to raise a graft. The groin site was closed primarily with 4–0 nylon sutures and dressed. The full thickness skin graft was then sutured into the donor site on the index finger utilizing 4–0 nylon sutures. A bolster of mineral oil-soaked cotton and petrolatum/bismuth tribromophenate impregnated dressing (Xeroform) was tethered down over the graft with 4–0 nylon sutures. 4×4 gauze and gauze wrap was used to cover the hand and an ace bandage was used as a protective dressing.
The patient was seen in the clinic at regular intervals and, for the final time, 32 days post-operation. The patient showed excellent range of motion and strength in all joints as well as good soft tissue coverage of the tip of the thumb (Figure 1C). The IP joint was preserved, allowing good opposition and pinch abilities (Figure 1D). The full thickness skin graft partially failed; however, the donor site healed well by secondary intention without any functional donor site morbidity.
Patient Case 2—Free Tissue Transfer from the Great Toe
A 55-year-old patient presented with a large posttraumatic open wound/defect to the right thumb pulp as a result of a work-related accident. The defect measured 3.5cm × 2.5cm in size (Figure 2A). If this defect was not repaired, it would compromise the entire function of the thumb, and therefore, the entire function of the hand. In choosing reconstructive options, a free flap from the right great toe was selected as it would adequately restore contour and sensation to the pulp.
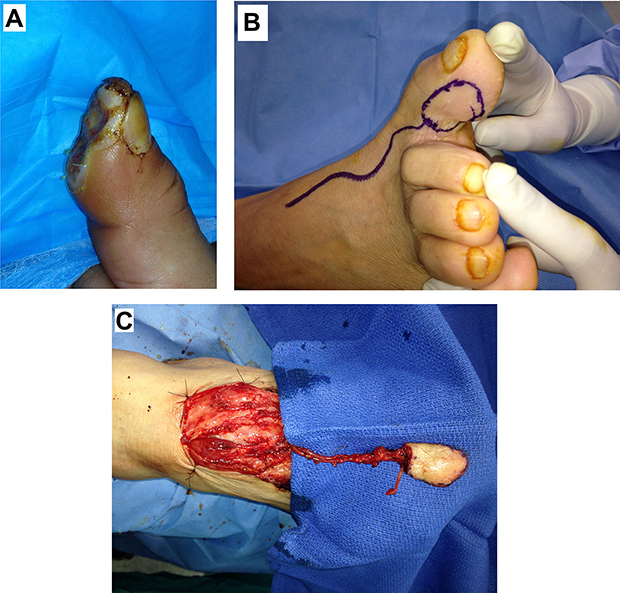 |
Figure 2 (A) Large skin-soft tissue defect of the pulp of the right thumb, 3.5×2.5cm. (B) The template of the flap and course of the supplying vessels. (C) The flap elevated with vascular pedicle dissected. |
The operation began by debriding an open wound on the right thumb. Then its ulnar digital nerve was mobilized. An incision was made along the first web space down to the anatomic snuff box to isolate the radial artery and cephalic vein. A template of the wound was created and marked on the inner aspect of the right great toe. The course of the first metatarsal artery was traced back, about 10 cm, along to the dorsalis pedis artery, utilizing a Doppler probe (Figure 2B). The flap was incised along the markings. The first metatarsal artery was dissected down as well as a branch of the great saphenous vein and a branch of the plantar digital nerve (Figure 2C).
The flap was then divided off the foot on its neurovascular pedicle. The wound at the donor site was closed primarily with 4–0 nylon. 8–0 nylon was used to anastomose the artery of the flap to the radial artery in the anatomic snuff box end-to-side, the vein of the flap to the cephalic vein end-to-end and was also used to coapt the plantaris digital nerve to the ulnar digital nerve all under operative microscopic magnification. Flap perfusion was confirmed, and the flap was inset with 4–0 nylon. Upon the closure of the incisions, it was determined that the wound over the vascular pedicle at the base of the flap, about 1cm2 area, could not be closed without compromising it. A porcine dermal collagen-nylon-silicone (Biobrane) membrane was used to cover that area temporarily, as primary closure of that area without compromising the pedicle was not possible. The wounds were then dressed.
After the patient returned to clinic on the 88th day post-operation, the wound was assessed for the final time. The thumb was found to have full coverage of glabrous skin with full restoration of the nearly completely lost pulp (Figure 3A). Range of motion and strength in pinch and grip were found to be excellent and well restored (Figure 3B). Moreover, the donor site showed some scarring as the only residual donor site morbidity (Figure 3C).
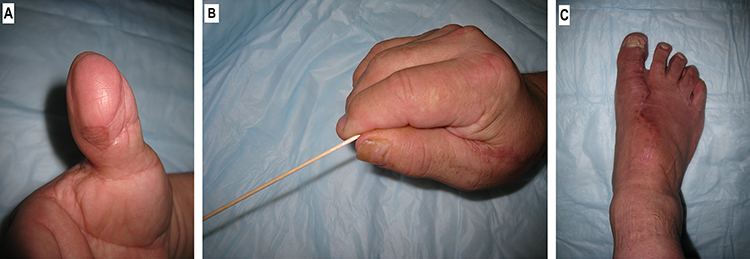 |
Figure 3 (A) View of the right thumb after reconstruction. (B) Patient is able to perform pinch with good strength. (C) View of the right great toe donor site. |
Patient Case 3—Free Tissue Transfer from the Great Toe
A 52-year-old male patient presented with a 5cm × 2.5cm injury to the thumb after a machine crushed it at work. The injury occupied the entire volar surface of the thumb pulp and half of the area over the proximal phalanx with exposure of the bone and flexor tendon (Figure 4A and B). Given the character and size of the wound, a decision was made to perform free tissue transfer from the left great toe to the thumb.
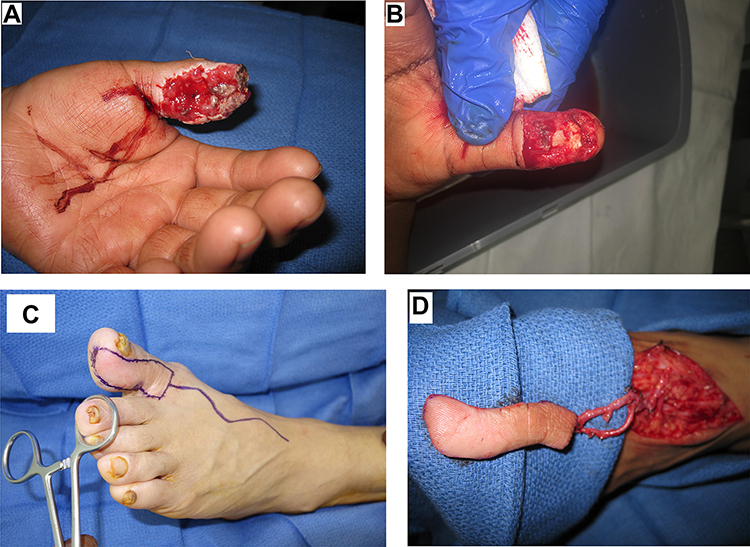 |
Figure 4 (A) Open wound / soft-tissue defect of the left thumb 3.5×2.5cm with exposure of distal phalanx and flexor tendon. (B) Wound after debridement. (C) The template of the flap and course of the supplying vessels. (D) The flap elevated with vascular pedicle dissected. |
The operation began by debriding the thumb of devitalized tissues. The ulnar digital nerve of the thumb was identified and mobilized. An incision was made along the first web space down to the anatomic snuff box to isolate and mobilize the radial artery and the cephalic vein. A template of the defect was created.
The wound template was then traced over the inner aspect of the left great toe from its tip to the base of the web space (Figure 4C). A lazy-S incision was then made on the foot followed by dissection of the vascular pedicle consisting of the first metatarsal artery, the dorsalis pedis artery, and the saphenous vein. The edges of the flap were then incised along the markings, and the flap mobilized (Figure 4D). It was determined upon the harvesting of the flap, that the digital nerve of the great toe could not be incorporated into the flap as it was located far more plantarly. Additionally, the branch of the dorsal digital nerve was too small in diameter to be used for coaptation.
This donor site was then templated, and the template traced over the calf. An approximately 7cm × 3cm full thickness skin graft was then traced and harvested. The calf donor site was closed in two layers using 3–0 polyglactin (Vicryl) then 4–0 poliglecaprone (Monocryl) sutures. The graft was then preserved off the table in moist gauze.
The recipient site vessels were then prepared under microscopic magnification. The flap was divided at the vascular pedicle and end-to-side anastomosis was performed using 9–0 nylon suture. After this, focus shifted back to the foot donor site where the full thickness graft was set in place using 4–0 polyglactin (Vicryl) and 4–0 nylon, in two layers. A vacuum assisted closure device was then placed over this site to function as both a bolster and to function as an incisional vacuum. Once the graft was finished, attention shifted back to the thumb where the flap edges were inset using 4–0 nylon. Due to excess tension on the flap, a small area on the radial aspect of the tip of the thumb was left open to heal by secondary intention. The nailbed was stented open with a foil stent, and the thumb wrapped in petrolatum cellulose acetate dressing (Adaptic) and gauze.
On the 134th day post-operation, the patient returned to clinic for the last time. Excellent soft tissue coverage with well vascularized skin was achieved (Figure 5A). The patient only reported some weakness in heavy pushing exercises, but otherwise had fully functional thumb pulp. The patient had restoration of pinch function (Figure 5B) and was able to use his thumb to accomplish most all his tasks of daily life and was cleared to work two weeks after this visit.
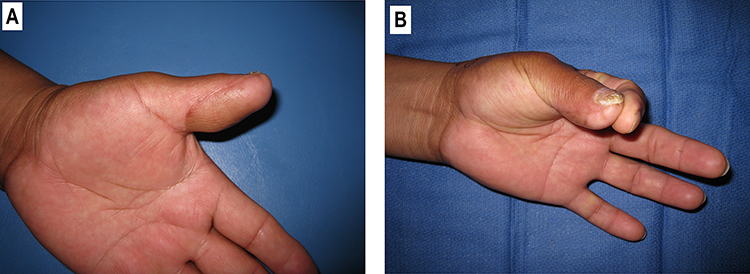 |
Figure 5 (A) View of the left thumb after reconstruction. (B) Restoration of pinch. |
Patient Case 4—Non-Operative
We have performed a total of 13 non-operative fingertip repairs utilizing the following method. 4 of these cases were thumbs with patients ranging in age from 7 to 60 years old.
This patient presented to the emergency department with traumatic amputation of the thumb tip. This wound was approximately 2cm in diameter and was transverse across the tip, orthogonal to the phalanx, and spanned the pulp and part of the nail, a classic Allen class II amputation (Figure 6A). To avoid unnecessary surgery, and since surgery might not produce better results, we decided to treat conservatively. The wound was irrigated and cleaned thoroughly, after which debridement of any unviable tissue and debris was performed. The wound was then covered with a semi-occlusive polyurethane film (Tegaderm) without any sort of ointment beneath the dressing. Soft cotton cling dressing was then used to cover the dressing, being sure not to obstruct range of motion at the IP joint and encouraging the patient to maintain mobility of their thumb. The patient was then instructed to return to the clinic every week to have the dressing changed.
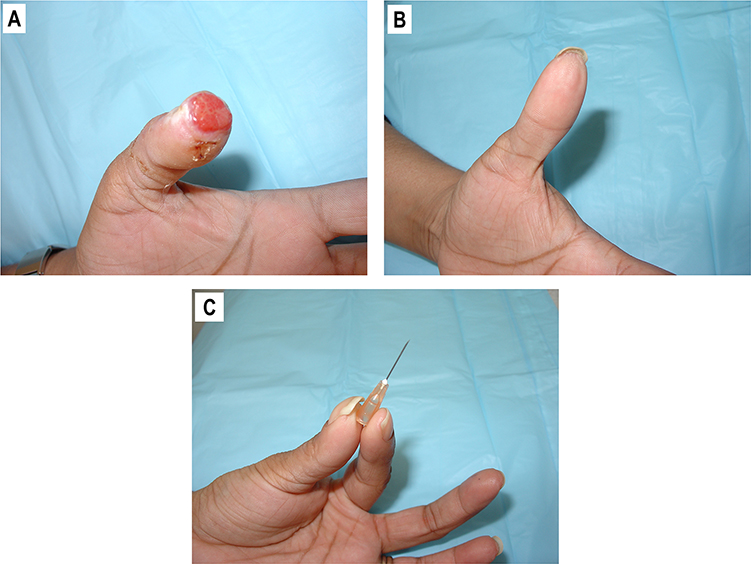 |
Figure 6 (A) Open wound at the tip of the left thumb, 2 x 2cm. (B) Wound healed by secondary intention upon semi-occlusive dressings treatment. (C) Restoration of pinch function. |
Changing the dressing involved removing the old dressing, allowing the wound to dry and aerate for 10–15 minutes, then reapplying the same style of dressing. The dressing is applied to allow free mobility of all joints and the patient is encouraged to keep their thumb mobile.
On the 38th day after the first evaluation, the patient returned to the clinic for the final time. The thumb tip showed excellent healing with full restoration of the pulp, the nail, and the fingerprint (Figure 6B). Range of motion and pinch were restored to their normal levels (Figure 6C) and cosmesis was superb.
Discussion
Revision Amputation
Revision amputation is a procedure commonly used to eradicate infections, neoplasia, tissue with vascular compromise, functionally compromised tissues, and neuromas. While the procedure of revision amputation is relatively simple to perform, a skillful approach must be taken when addressing the thumb, so as to avoid delayed healing, pain, nail deformities, poor aesthetics, hyperesthesia, motor function impairment and stiffness.5
A key consideration is length, since reducing the length of the bone at the tip of the thumb results in significantly reduced strength in key pinch grip and 3-point pinch grip.6 Therefore, revision amputation should only be considered as a last resort option where there is a clear benefit that outweighs the loss of either soft or bony tissue at the tip of the thumb.
Moberg flap / Palmar advancement flap
In 1964 Moberg introduced a method to advance a volar neurovascular flap from the thumb itself to close defects at the tip. Tissue proximal to the defect at the end of the thumb is dissected off the base of the thumb, sufficient to reach the most distal end of the defect.8 This reconstructive modality has been shown to have satisfactory results in sensory (2-point discrimination), range of motion (opposition and flexion at the IP joint), grip strength and DASH (disabilities of the arm, shoulder and hand) questionnaire categories.9,10
There are, however, major problems with this flap with some of the most common complaints including cold intolerance, nail deformities, pulp instability, pain, neuropraxia, and difficulty with buttoning.9,10 There is also a significant risk of permanent flexion contracture and of potential loss of part or of all the thumb, in cases where the flap fails. In most cases, the advancement flap places the thumb in at least a slightly flexed position, with greater flexion being required in repairing larger tip defects. Excess tension established by aggressive advancements can lead to skin necrosis, as well as thumb contracture.2,11
Another limitation is that good coverage can only be achieved in defects up to 2 cm in size. A modification described by O’Brien islandizes the flap and allows coverage of larger defects.12 To further extend the reach of the flap while providing relief of flexion at the base of the thumb, z-plasties,11,13 V-Y advancements14–17 and skin grafting12 have been described. Skin grafting brings problems with scar contracture, instability and color mismatch.4 Dellon demonstrated that defects up to 3cm can be closed via utilization of an islandized flap similar to O’brien, but with donor site closure utilizing two rotational flaps, an option that provides satisfactory closure but necessitates a technically challenging procedure that may unnecessarily prolong surgery.15
FDMA Flaps: Foucher Flap & Holevich flap
In 1979, the eponymous Foucher, along with Braun, described and popularized the kite flap,18 a flap based on the first dorsal metacarpal artery (FDMA or DMCA), on previous versions described by Hilgenfeldt in 195019 and by Holevich in 1963.20 Foucher utilized these two previous concepts and islandized the flap.
This kite flap can also be harvested with a sensory branch of the radial nerve to help restore immediate sensation, obviating the need for nerve coaptation.6 Excellent tactile gnosis has been reported by Small and Brenan in 1988.21 Zhang et al in 2011 reported an improvement in the 2-point discrimination of the flap by performing neurorrhaphy between the sensory branch of the radial nerve, included in the flap, and the proper digital nerve of the thumb; a technique that is technically demanding but can be considered when the patients’ occupational needs or personal goals demand higher levels of sensation.22
The flap can provide good coverage of both dorsal and volar defects and can bring significant volume to fix large pulp defects.5 The donor site is then usually covered with a full thickness skin graft.18,19 Despite the need for skin grafting, significant donor site morbidity remains low; and pain, sensory, range of motion (Kapandji scores) and aesthetics are favorable.23 Average FDMA flap sizes reported in the literature range from 5.89 cm2 (reported by Ghoraba et al)24 to 6.46cm2 (reported by Satish)25 to 7.1 cm2 (reported by Günay et al).23
In comparison to the Moberg flap, Durgut et al directly found the Moberg flap to be superior in avoiding cold intolerance and in finer static 2-point discrimination.26 This improvement must give careful consideration to the limitations of the Moberg flap, which the FDMA flap can overcome, namely in closure of dorsal and larger defects.
Modifications of the FDMA flap have been described throughout the literature: Tan et al proposed the radial proper palmar digital artery as a supplement to the FDMA in cases where a larger flap is needed, or if the FDMA is insufficient, unavailable, or damaged.27 El-Khatib describes success in extending the FDMA flap beyond the territory of skin directly supplied by the FDMA, extending distally into the dorsal skin of the distal portion of the proximal phalanx and the skin over the middle phalanx. Though this skin does not have direct supply by the FDMA, El-Khatib suggests that the strong dermal-subdermal plexus that is part of this skin is sufficient to ensure its viability. In this way, the FDMA flap can be used to cover even larger thumb wounds.28 Recently, Couceiro et al extended the flap by adding a lobe supported on the second dorsal metacarpal artery, producing a bilobed flap, which is used to close very large defects of the thumb.29
The Holevich flap is a modification of the Hilgenfeldt flap that utilizes the same FDMA as both Foucher and Hilgenfeldt, but with an attached racquet of skin extending from the dorsal hand to the proximal index finger. This skin allows immediate restoration of sensation to the lateral or medial thumb as well as the part of the tip that was injured. It is otherwise functionally similar to the FDMA flap.20
In a small case series directly comparing the Foucher and Holevich flaps, Couceiro et al, reports that the Holevich flap appears to have better outcomes in terms of less venous congestion, less cold intolerance, and less flap necrosis.30 Each group only had 5 cases and thus definitive conclusions cannot be drawn; however, it would support the thought that the racquet style flap might be less prone to vascular compromise due to less compression of the neurovascular bundle, in comparison to the Foucher flap.31,32
Free Flap from the Great Toe
Free tissue transfer can provide an effective solution when there is a large defect that requires substantial coverage, and when local or regional flaps are unsuitable or unavailable. Trauma can damage structures that would otherwise serve as donors to thumb defects, in these cases, free tissue transfer would be the treatment of choice. Free tissue transfer is especially useful in larger pulp defects, where local tissue is insufficient, or has been simultaneously lost, especially given the importance of functional, painless thumb pulp.33 Some examples include free flaps from the lateral forearm,5 groin,5 medial plantar surface,34 and great toe.
The great toe shares many similarities to the thumb in the arrangement of both internal and external structures, as well as similarities in subcutaneous tissue and glabrous skin. It can be transferred entirely to replace a non-viable and/or fully amputated thumb,4 or as a partial tissue transfer to cover partial amputations.35 The first full great toe transfer was done in 1968 by Cobbett.36 The transfer of a neurovascular free flap from the great toe was first described in 1979 by Buncke and Rose to improve results of the regional flaps that were traditionally being used. They demonstrated improved two-point discrimination, less hyperesthesia, less donor site anesthesia and obviated the need for cortical re-orientation.37–39 The flap is also preferred if aesthetic appearance is of high importance, as there are no donor site scars on the hands.40 Furthermore, the donor site morbidity to the foot is minimal, usually with no functional and minimal aesthetic impairment. Variations of free tissue transfer from the great toe are numerous, including transferring any part of the skin, nail, bone and joint or pulp.41
There should be a careful consideration as to the amount of bulk taken from the great toe in order to avoid re-operations.40 Moreover, the transfer of free tissue is not without risk, and in patients of advanced age, should be limited due to the increased risk of flap failure or poor sensory recovery.42 As with any microsurgical free flap, this is a technically demanding procedure and anastomotic failure can happen, leading to rapid flap loss or necrosis.43 Absolute contraindications to free tissue transfer include injured donor tissue, compromised donor or recipient vasculature or infections affecting either donor or recipient sites.44
Non-Operative Methods
Reconstruction of the open wounds/skin defects of the thumb tip is technically difficult. In certain instances non-operative management provides a low-skill treatment alternative that provides quite adequate healing of the wound.45 Healing by secondary intention allows preservation of the thumb length, with epithelialization that restores near normal skin with satisfactory sensation.5 The cost of non-operative management of tip injuries is substantially lower than even the simplest surgical procedures.46 There is also a lack of evidence showing a clear benefit in healing or function with surgical intervention over non-operative methods in management of the thumb tip wounds.47
Defects that have no bony exposure, and are limited in size (consensus usually lands on <2cm2) are ideally managed with non-operative methods.5 Special care should be taken in wounds where the size of the defect is larger, since secondary intention does not restore volume to the thumb tip, which can lead to impairment of precision grip and 3 finger pinch, as well as hyperesthesia, and cold intolerance.2,5
Bone exposed to the level of the defect is not an absolute contraindication to non-operative management and Quadlbauer et al describe good results in such cases, though special care must be taken to ensure adequate soft tissue coverage.48
One review found that as much as 6% of tip injuries result in nail deformities47 thus care must be given to defects that involve the nailbed or eponychia, as damage to these structures can lead to suboptimal cosmesis or even functional impairment and pain.45
Various techniques have been reported in the literature to achieve wound healing. Semi-occlusive45,46,48 and occlusive dressings49 allow the wound to retain the proper environment for healing while reducing the number of dressing changes that some older techniques, like paraffin gauze, required.5
Lee et al report treatment of 156 fingertips with a hyphecan biopolymer, a semi-occlusive dressing that requires no dressing changes, healed in an average of 32 days, and demonstrated good healing with only 4 cases of clinically minimal infections.50 Semi-occlusive polyurethane film (Opsite) has been used by Mennen & Weise with good results resulting in healing times ranging from 20 to 30 days though this method required weekly dressing changes.51 More recently, Ng et al describe a method utilizing a custom molded thermoplastic fenestrated finger cap with underlying UrgoTal semi-occlusive dressing that demonstrated a low-cost technique that required bi-weekly evaluation and has similar healing times to other semi-occlusive dressing methods.46
Downsides of fully occlusive methods involve inevitable maceration of the surrounding skin, and difficulty in assessing progression—especially if sulfadiazine cream is used.52 Healing times are long, and dressings usually require weekly changes for as long as the wound takes to heal. It is also important to make patients aware of a potential foul, yet benign, odor that may come from the wound exudate.6
Our experience shows that the most successful application of non-operative management is for superficial skin/soft tissue defects with a minimal component of contusion. Using weekly semi-occlusive dressing changes with polyurethane semi-occlusive dressings (Tegaderm), we were able to achieve secondary healing with satisfactory aesthetic and functional results in simple wounds of up to 6 cm2. However, more complicated wounds, up to 4 cm2, can also be successfully managed with this method after an initial conservative debridement. Healing time varied from 4 to 5 weeks.
We have overall found this technique can produce excellent results and can obviate the need to surgically repair certain defects. This is especially true of injuries to the tip, which is may otherwise prove a technically demanding reconstruction.
Conclusion
There are numerous methods, operative and non-operative, to manage skin/soft tissue defects of the thumb (Figure 7). We advocate for an individual approach, selecting the best option based on the size, location, and other characteristics of the defect, as well as the general condition of the patient. Free flap transfer from the great toe is an excellent method of restoration for large, post-traumatic, open wounds of the thumb. Non-operative methods should likely be utilized more frequently, especially to avoid the significant risks related to surgery.
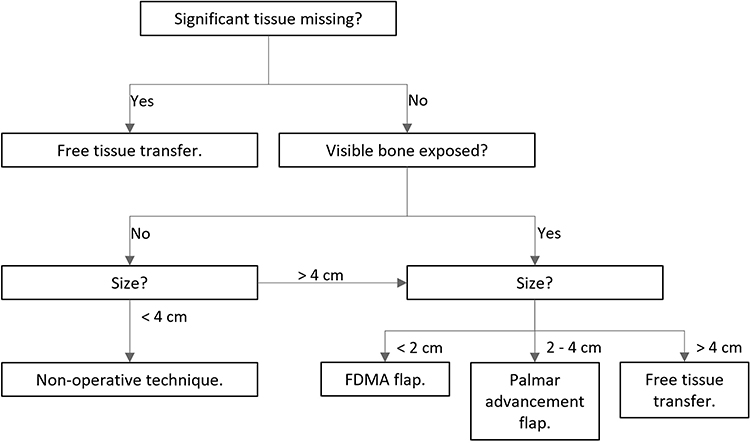 |
Figure 7 General algorithm for the selection of reconstructive method, may vary based on specific patient considerations. |
Ethical Considerations
This set of case reports is not considered research under the IRB requirements of what is research, therefore IRB review is not required. All patients provided written informed consent to use their de-identified case details and images as part of this case series.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dewey WS, Richard RL, Hedman TL, et al. Opposition splint for partial thumb amputation: a case study measuring disability before and after splint use. J Hand Ther. 2009;22(1):
2. Ayyala HS, Condé-Green A, Datiashvili R. Great Toe-to-Thumb Hemi-Pulp Transfer. Eplasty. 2016;16:ic33. PMID: 27602177; PMCID: PMC4993034.
3. National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey. National Center for Health Statistics; 2018.
4. Yassin AM, Dash S, Nikkhah D. Workhorse flaps for thumb reconstruction. Plast Aesthet Res. 2022;9:56. doi:10.20517/2347-9264.2022.36
5. Blair JW, Moskal MJ. Revision amputation achieving maximum function and minimizing problems. Hand Clin. 2001;17(3):457–471. PMID: 11599213. doi:10.1016/S0749-0712(21)00524-2
6. Germann G, Rudolf KD, Levin SL, Hrabowski M. Fingertip and thumb tip wounds: changing algorithms for sensation, aesthetics, and function. J Hand Surg. 2017;42(4):274–284. doi:10.1016/j.jhsa.2017.01.022
7. Ono S, Chung KC. Efficiency in digital and hand replantation. Clin Plast Surg. 2019;46(3):359–370. PMID: 31103081; PMCID: PMC6527348. doi:10.1016/j.cps.2019.03.002
8. Moberg E. Aspects of sensation in reconstructive surgery of the upper extremity. J Bone Joint Surg Am. 1964;46(4):817–825. PMID: 14161094. doi:10.2106/00004623-196446040-00011
9. Foucher G, Delaere O, Citron N, Molderez A. Long-term outcome of neurovascular palmar advancement flaps for distal thumb injuries. Br J Plast Surg. 1999;52(1):64–68. PMID: 10343593. doi:10.1054/bjps.1997.3005
10. Baumeister S, Menke H, Wittemann M, Germann G. Functional outcome after the Moberg advancement flap in the thumb. J Hand Surg Am. 2002;27(1):105–114. PMID: 11810623. doi:10.1053/jhsu.2002.30921
11. Thibaudeau S, Tremblay DM, Tardif M, Chollet A. Moberg modification using the first web space: thumb reconstruction following distal amputation. Hand. 2012;7(2):210–213. PMID: 23730245; PMCID: PMC3351517. doi:10.1007/s11552-012-9406-4
12. O’Brien B. Neurovascular island pedicle flaps for terminal amputations and digital scars. Br J Plast Surg. 1968;21(3):258–261. PMID: 4877607. doi:10.1016/s0007-1226(68)80033-5
13. Mutaf M, Temel M, Günal E, Işık D. Island volar advancement flap for reconstruction of thumb defects. Ann Plast Surg. 2012;68(2):153–157. PMID: 21629080. doi:10.1097/SAP.0b013e318216e6b1
14. Elliot D, Wilson Y. V-Y advancement of the entire volar soft tissue of the thumb in distal reconstruction. J Hand Surg Br. 1993;18(3):399–402. PMID: 8345278. doi:10.1016/0266-7681(93)90073-o
15. Dellon AL. The extended palmar advancement flap. J Hand Surg Am. 1983;8(2):190–194. PMID: 6833729. doi:10.1016/s0363-5023(83)80014-8
16. Bang H, Kojima T, Hayashi H. Palmar advancement flap with V-Y closure for thumb tip injuries. J Hand Surg Am. 1992;17(5):933–934. PMID: 1401811. doi:10.1016/0363-5023(92)90473-3
17. Russell RC, Casas LA. Management of fingertip injuries. Clin Plast Surg. 1989;16(3):405–425. PMID: 2673624. doi:10.1016/S0094-1298(20)31311-0
18. Foucher G, Braun JB. A new island flap transfer from the dorsum of the index to the thumb. Plast Reconstr Surg. 1979;63(3):344–349. PMID: 368837. doi:10.1097/00006534-197903000-00008
19. Hilgenfeldt O. Operativer Daumenersatz, Enkeverslag, Stuttgart. 1950.
20. Holevich J. A new method of restoring sensibility to the thumb. J Bone Joint Surg Br. 1963;45(3):496–502. PMID: 14058323. doi:10.1302/0301-620X.45B3.496
21. Small JO, Brennen MD. The first dorsal metacarpal artery neurovascular island flap. J Hand Surg Br. 1988;13(2):136–145. PMID: 3385287. doi:10.1016/0266-7681_88_90122-2
22. Zhang X, Shao X, Ren C, Zhang Z, Wen S, Sun J. Reconstruction of thumb pulp defects using a modified kite flap. J Hand Surg Am. 2011;36(10):1597–1603. PMID: 21831533. doi:10.1016/j.jhsa.2011.06.033
23. Günay AE, Tatlisu K, Çavuş M, Kahraman M. Mid-term results of the first dorsal metacarpal artery flap for thumb defects. J Hand Surg Asian Pac Vol. 2022;27(5):834–838. PMID: 36285757. doi:10.1142/S2424835522500801
24. Ghoraba SM, Mahmoud WH. Outcome of thumb reconstruction using the first dorsal metacarpal artery island flap. World J Plast Surg. 2018;7(2):151–158. PMID: 30083496; PMCID: PMC6066707.
25. Satish C, Nema S. First dorsal metacarpal artery islanded flap: a useful flap for reconstruction of thumb pulp defects. Indian J Plast Surg. 2009;42(1):32–35. PMID: 19881017; PMCID: PMC2772290. doi:10.4103/0970-0358.53003
26. Durgut F, Ozdemir A, Ergin M, Güleç A, Acar MA. Comparison of the modified moberg flap versus first dorsal metacarpal artery flap for thumb pulp reconstruction. Ann Plast Surg. 2022;88(3):277–281. PMID: 34387579. doi:10.1097/SAP.0000000000002972
27. Tan HL, Tan DY, Zhao JK. Treatment of thumb soft-tissue defects using a bipedicle island flap of the index finger: anatomical basis and clinical application. Arch Orthop Trauma Surg. 2013;133(5):721–728. PMID: 23443528. doi:10.1007/s00402-013-1704-y
28. El-Khatib HA. Clinical experiences with the extended first dorsal metacarpal artery island flap for thumb reconstruction. J Hand Surg Am. 1998;23(4):647–652. PMID: 9708378. doi:10.1016/S0363-5023(98)80050-6
29. Couceiro J, De la Red-Gallego M, Yeste L, et al. The bilobed racquet flap or extended seagull flap for thumb reconstruction: a case report. J Hand Surg Asian Pac Vol. 2018;23(1):128–131. PMID: 29409406. doi:10.1142/S2424835518720050
30. Couceiro J, Sanmartín M. The Holevich flap revisited: a comparison with the Foucher flap, case series. Hand Surg. 2014;19(3):469–474. PMID: 25155709. doi:10.1142/S0218810414970090
31. Fernandez MS. Macrosurgery for fingertip amputations. BMC Proc. 2015;9(Suppl 3):A58. PMCID: PMC4445494. doi:10.1186/1753-6561-9-S3-A58
32. Al Lahham S, Ahmed MB, Aljassem G, Sada R, Alyazji ZTN, Thomas J. A modification to enhance the survival of the Island FDMA flap by adding a skin bridge. Plast Reconstr Surg Glob Open. 2021;9(2):e3434. PMID: 33680678; PMCID: PMC7929644. doi:10.1097/GOX.0000000000003434
33. Del Piñal F. The indications for toe transfer after ”minor” finger injuries. J Hand Surg Br. 2004;29(2):120–129. PMID: 15010156. doi:10.1016/j.jhsb.2003.12.004
34. Lai CH, Lai CS, Huang SH, Lin SD, Chang KP. Free medial plantar artery perforator flaps for the resurfacing of thumb defects. Ann Plast Surg. 2010;65(6):535–540. PMID: 21042191. doi:10.1097/SAP.0b013e3181d376df
35. Li X, Viviano S, Datiashvili R. Salvage of thumb with a free skin flap from the great toe. Eplasty. 2018;18:ic15. PMID: 30206463; PMCID: PMC6108156.
36. Cobbett JR. Free digital transfer. Report of a case of transfer of a great toe to replace an amputated thumb. J Bone Joint Surg Br. 1969;51(4):677–679. PMID: 5371970. doi:10.1302/0301-620X.51B4.677
37. Buncke HJ, Rose EH. Free toe-to-fingertip neurovascular flaps. Plast Reconstr Surg. 1979;63(5):607–612. PMID: 372990. doi:10.1097/00006534-197905000-00001
38. Logan A, Elliot D, Foucher G. Free toe pulp transfer to restore traumatic digital pulp loss. Br J Plast Surg. 1985;38(4):497–500. PMID: 4052709. doi:10.1016/0007-1226(85)90007-4
39. Stern PJ. Free neurovascular cutaneous toe pulp transfer for thumb reconstruction. Microsurgery. 1987;8(3):158–161. PMID: 3670038. doi:10.1002/micr.1920080310
40. Deglise B, Botta Y. Microsurgical free toe pulp transfer for digital reconstruction. Ann Plast Surg. 1991;26(4):341–346. PMID: 1872539. doi:10.1097/00000637-199104000-00008
41. Koshima I, Inagawa K, Urushibara K, Okumoto K, Moriguchi T. Fingertip reconstructions using partial-toe transfers. Plast Reconstr Surg. 2000;105(5):1666–1674. PMID: 10809096. doi:10.1097/00006534-200004050-00011
42. Tsai TM, Jupiter JB, Wolff TW, Atasoy E. Reconstruction of severe transmetacarpal mutilating hand injuries by combined second and third toe transfer. J Hand Surg Am. 1981;6(4):319–328. PMID: 7252101. doi:10.1016/s0363-5023(81)80034-2
43. Gu JX, Pan JB, Liu HJ, et al. Aesthetic and sensory reconstruction of finger pulp defects using free toe flaps. Aesthetic Plast Surg. 2014;38(1):156–163. PMID: 24441759. doi:10.1007/s00266-013-0260-8
44. Troisi L, Mazzocconi L, Mastroiacovo A, et al. Beauty and Function: the Use of Trimmed Great Toe in Thumb and Finger Reconstruction. Plast Reconstr Surg Glob Open. 2022;10(9):e4540. PMID: 36203737; PMCID: PMC9529065. doi:10.1097/GOX.0000000000004540
45. Chow SP, Ho E. Open treatment of fingertip injuries in adults. J Hand Surg Am. 1982;7(5):470–476. PMID: 7130656. doi:10.1016/s0363-5023(82)80042-7
46. Hjh N, Sim J, Tey VHT, Selvaganesh S, Rebosura CKP, Rajaratnam V. Experience with the use of splint caps for the management of fingertip amputation injuries. J Hand Surg Asian Pac Vol. 2020;25(2):199–205. PMID: 32312214. doi:10.1142/S242483552050023X
47. Krauss EM, Lalonde DH. Secondary healing of fingertip amputations: a review. Hand. 2014;9(3):282–288. PMID: 25191157; PMCID: PMC4152443. doi:10.1007/s11552-014-9663-5
48. Quadlbauer S, Pezzei C, Jurkowitsch J, et al. Der Okklusionsverband zur Behandlung von Allen III und IV Fingerkuppenverletzungen als Alternative zu lokalen Lappenplastiken [The semi-occlusive dressing in treating Allen III and IV fingertip injuries as an alternative to local skin flaps]. Unfallchirurg. 2017. 120(11):961–968. German. PMID: 27638553. doi:10.1007/s00113-016-0237-6
49. de Boer P, Collinson PO. The use of silver sulphadiazine occlusive dressings for finger-tip injuries. J Bone Joint Surg Br. 1981;63B(4):545–547. PMID: 7298681. doi:10.1302/0301-620X.63B4.7298681
50. Lee LP, Lau PY, Chan CW. A simple and efficient treatment for fingertip injuries. J Hand Surg Br. 1995;20(1):63–71. PMID: 7759939. doi:10.1016/s0266-7681(05)80019-1
51. Mennen U, Wiese A. Fingertip injuries management with semi-occlusive dressing. J Hand Surg Br. 1993;18(4):416–422. PMID: 8409649. doi:10.1016/0266-7681(93)90139-7
52. Williamson DM, Sherman KP, Shakespeare DT. The use of semipermeable dressings in fingertip injuries. J Hand Surg Br. 1987;12(1):125–126. PMID: 3553385. doi:10.1016/0266-7681_87_90077-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.