")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Obstacles in Basic Health Service When Dealing with COVID-19: A Reflection for Improvement
Authors Eyanoer PC , Zaluchu F
Received 30 November 2023
Accepted for publication 25 March 2024
Published 17 April 2024 Volume 2024:17 Pages 1671—1679
DOI https://doi.org/10.2147/JMDH.S446298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Putri Chairani Eyanoer,1 Fotarisman Zaluchu2
1Department of Community and Preventive Medicine, Faculty of Medicine, Universitas Sumatera Utara, Medan, North Sumatera, Indonesia; 2Social Anthropology Department, Universitas Sumatera Utara, Medan, North Sumatera, Indonesia
Correspondence: Putri Chairani Eyanoer, Department of Community and Preventive Medicine, Faculty of Medicine, Universitas Sumatera Utara, Kompleks ICON 3 No. B5, Jalan Abdul Hakim, Medan, North Sumatera, 20131, Indonesia, Tel +6281370232513, Email [email protected]
Background & Aims: COVID-19 has been in control since mass vaccination and other coordinated efforts have been conducted. The WHO has even made an announcement to stop the public health emergency of international concern (PHEIC) toward COVID-19. Because of the very massive impacts of COVID-19, it is necessary to have a reflection toward what we have gone through to obtain information from inside the health service by interviewing the health officers who were the frontliners in fighting the disease during the pandemic. This research attempts to reveal the practical experiences of the officers when the COVID-19 pandemic took place.
Methods: This research conducted in-depth interviews with the Heads of Puskesmas (a Public Health Center) and the staff of Puskesmas in Medan. The total sample number of informants is 30 people. The data were managed by preparing the suitable themes with the inductive approach.
Results: There are three main themes obtained from the analysis results. Those three themes are 1) the condition of Puskesmas, 2) the impacts of the health service, and 3) the COVID-19 control. Those three themes show the fundamental problems affecting the efforts to overcome COVID-19. It is revealed that funding, personnel quantity, and bureaucracy cause the effort to overcome COVID-19 to have been impeded. Meanwhile, based on external factors, the officers had to deal with negative issues on COVID-19. Therefore, whether we like it or not to admit the fact, the health service has not been conducted maximally.
Conclusion: It is necessary to have comprehensive revision and change to evaluate the condition of health service, particularly in Puskesmas. A wider and deeper reflection is required so that the pandemic preparation in the future can be improved further.
Keywords: Puskesmas, reflection of COVID-19, basic service, to overcome COVID-19, Indonesia
Background
It has been announced that COVID-19 no longer becomes the public health emergency of international concern (PHEIC).1 In the three years of the pandemic, many became the victims, from both the common people and the medical workers. There were at least 770 million cases reported and almost seven million mortality cases occurring during the pandemic.2
Although the WHO has determined the COVID-19 handling procedure since the beginning when the pandemic occurred, every country certainly has its own uniqueness in suppressing the spreading of COVID-19. In Indonesia, the effort to control the COVID-19 has been conducted by applying many ways. When the pandemic started to happen, there were public movement restrictions. Afterwards, there was an effort to integrate the healthy life style application with sufferer detection strengthening. The last effort conducted was to carry out mass vaccination to all the population, starting from the vulnerable groups.3 Despite all those efforts, during the pandemic (2020–2023), in Indonesia there were around 6 million cases reported with as many as 162,000 people became the casualties of this SARS-CoV-2 virus.2
The COVID-19 handling in Indonesia often obtained negative critiques from many parties. Six months since the pandemic started, the coordination and transparency of the COVID-19 handling were considered as a big problem for the government.4,5 Even the local community considered that the COVID-19 handling was very bad; moreover, the health service applied was considered very insufficient.5
The WHO has informed that the health service reform is really required.6 The necessary emphasis has to be conducted in terms of prevention, remote service, and technological use.7 The message from the World Economic Forum is also clear, namely that the health service, particularly the primary care, should be the health reform frontliner in the future because all this time the primary care – in Indonesia it is translated as Puskesmas (Public Health Centre) – is the weakest part in the health service structure of a country.8 Hence, ready or not, the health service should be the focus for the change and even the investment of every country in the post-pandemic era.
Those recommendations are required to be responded by carrying out the restructuring of the health service as the focus of the pandemic prevention effort in the future. Therefore, every country indeed must perform rearrangement of the health service at the frontliners. In Indonesia, the improvement recommendations have indeed been conducted by involving the experts and academicians.9 However, as far as we know, the one that involves resources from inside the health service is still nonexistent.
For that, it is necessary to have the approach which digs out the problems in the primary care sector, which should come from the health workers as the frontliners of the service. During the pandemic period, the health workers were often the reliable party in handling the COVID-19. They have the information and their experience interacting with the real condition and the “world” during the pandemic, and those are valuable. Thus, making them as the information sources in order to reconstruct the policy change is a strategical effort. The qualitative approach will provide the information as the new insights, which are certainly for completing other evaluation efforts that might have been carried out.
The critical point of this is that whether the COVID-19 control so far has been the most optimal performance of the health service or whether there are still strategical points that we can improve. Of course, the experience of every country in reflecting the post-pandemic situation is different, one from another.10–12 Thus, in Indonesia, we need a local evaluation to discover the direct or indirect causes on cases and deaths occurring during the pandemic. The narration from the health workers will really clarify the focus of the problems that must be fixed.13
Method
The qualitative approach in evaluating the health service, particularly at the primary care level, has been applied many times.14,15 In-depth information from the qualitative technique will help reveal the obstacles which might occur due to the ability to elaborate problems from different points of view.16,17 The WHO even stated that by using the qualitative approach, the health policy can be evaluated better because of involving the experience of those being researched.18
Study Setting and Samples
We have gathered information coming from the Puskesmas in Medan, Indonesia. The research population is all the heads of Puskesmas and Puskesmas staff in 41 Puskesmas in Medan. However, the samples were purposively selected, and there were six Puskesmas chosen. In all those six Puskesmas, the sample selection was conducted; there were six heads of Puskesmas selected in the chosen Puskesmas, and there were five staff in each Puskesmas selected so that the total sample number of Puskesmas staff is 30 people.
The study was conducted in Medan by considering a) the area with the highest number of the COVID-19 cases in North Sumatera Province; b) having the health facilities (Puskesmas) usually found in big cities with the second-level reference facilities which are considered quite complete so that it is assumed that the COVID-19 handling should have been more easily coordinated; c) having the technological and academic environment as well as the situation that should have enabled the managerial system development.
Data
Questions posed use the semistructured interview, and its list of questions has been prepared. The interview topic is the experience of the health officers particularly in overcoming COVID-19, especially about the responsibility they carried out, the difficulties in conducting their tasks, and the task implementation in accordance with their main tasks as the Puskesmas staff. The interview usually lasted for 60 to 90 minutes, was recorded, and was then transcribed. The research procedure has obtained the ethic approval from Ethical Committee for Research in Health, Universitas Sumatera Utara No.596/KEP/USU/2021 and translated version Ethical Clearance numbered 191/KEPK/USU/2024, where it is stated all the conditions reviewed by the committee, and the study is conducted in accordance with the Declaration of Helsinki.
The interview was conducted in each Puskesmas by obeying the health protocol applied when the research was carried out. To maintain the confidentiality of the Puskesmas and informants, then since the beginning of the research, the files and names of the informants have been changed into codes. Prior to the interview, informed consent was distributed and that all participants provided informed consent which included publication of anonymized responses.
Data Analysis
To manage the research data that have been transcribed, we use the thematic analysis.19,20 The transcribed narration was coded using NVivo to prepare early codes so that we obtained the broad range of the existing data. Afterwards, we again conducted the analysis in a form of adjustment toward the themes and suitability between the codes and the research objective. From there we then prepared the final codes. These final codes are the ones we present in Table 1.
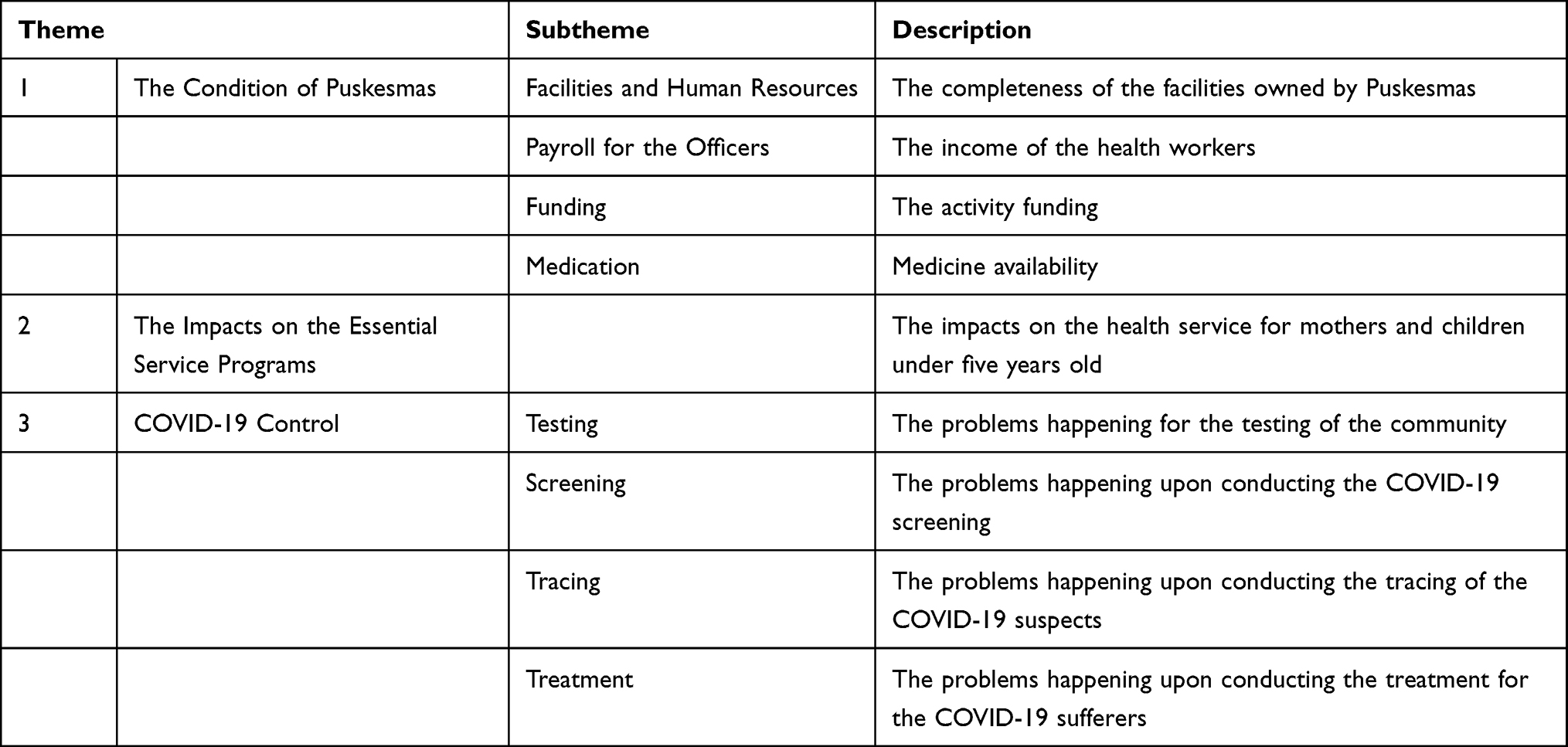 |
Table 1 Recapitulation of the Research Themes |
Results
After coding was made, the appearing themes in this research were recapitulated in the following table.
Theme 1: The Condition of Puskesmas
Facilities and Human Resources
To handle COVID-19 really requires adequate facilities so that every control action can be carried out well and has the impact toward the maximal performance of the health workers. However, the reality is many Puskesmas complained that their facilities were very minimum and required much more attention. Like the problem happening to one of the health officers, it was very hard to input data due to the problem of the network.
In terms of data input, there were still many obstacles actually… the network here is often off, so when we input the data for the vaccination that had been conducted, for example, we could only input that in the evening due to the problem of the network. Then the blackout also often happens lately here. (Informant A)
The condition obviously gave a lot of trouble to the officers in doing their job. Consequently, this condition could not provide new information and had the risk to deliver wrong data due to the cut off of the communication when data were put into the system.
The same happened with the equipment limitation that was experienced by the health workers who at that time were asked to trace the suspects of COVID-19 sufferers.
When doing testing using the antigen testing swab tools, those should have been provided by the Local Health Department. We should have obtained the tools from the Local Health Department first, but at the beginning the tools had not yet been distributed. What we meant was there were no antigen testing swab tools from the Local Health Department, so automatically Puskesmas also did not have any antigen testing swab tools. Thus, testing became a problem. (Informant B)
Besides that, as the limitation in health workers, particularly the officers as the laboratory analysts, was getting worse, this led to the impact toward very high work load.
The number of the analysts was enough actually, but during the pandemic the analysts were needed a lot as the number of the patients confirmed with COVID-19 was high, so those analysts became exhausted. It was hard to find the substitutes for those exhausting analysts. (Informan C)
Payroll for the Officers
The payroll for the health officers became one of the interesting issues. The government had indeed issued the policy to provide incentives for health officers involved in handling COVID-19. However, the health officers stated that the incentive given was not sufficient for their daily life (Informant A). Even the incentive for their performance was late to be given to those health officers (as stated by Informant B).
The more detailed statements can be read in the narrations below.
Our payment here was just IDR 650,000 for a doctor…well how could I work maximally? While I had to have two jobs automatically as that income was not enough. Hence, in the end I had to pass such work [related to COVID-19]. Everyday I had to come to Puskesmas, so no work [in relation to COVID-19] could be handled completely. (Informant A)
Not every work was getting paid. We had to work for a long time first, then we could claim the payment. The payment would be processed after being claimed. (Informant B)
Funding
The efforts to overcome COVID-19 could not be separated from funding. With sufficient funding that was properly distributed to the right targets, it could accelerate the performance to overcome COVID-19. However, there were obstacles in the funding to deal with this disease. Ironically, the main problems were the claim, and disbursement of the funding was late (as stated by Informant A and Informant B), and the difficulty to manage the funding (as stated by Informant D).
The more detailed statement can be seen in the narration below.
The problem with the late financing might be caused by the unfinished report on COVID-19; hence, there was no disbursement yet. (Informan D)
As a result, there was a problem too in the funding to buy medicine.
Oh, from the problem with the funding, it led to the running out of the medicine availability for the patients of COVID-19. (Informan E)
Indeed, the disbursement of COVID-19 funding was problematic due to the complicated and long bureaucracy or red tape procedure. Occasionally, the health officers that should have played an important role in clinical handling were also involved in the administrative process.
Being a medical doctor means having the hustle and bustle in their work here; besides the medical doctors, the nurses were also very busy and they had the most difficult time during the pandemic as the funding is from the local government [so they worked extra without extra income]. They both had to submit the data [on COVID-19 patients] since that was the regulation we all had to obey during the pandemic. (Informant F)
Medication
Medication is also included as an important element in handling COVID-19. With the medication, it can accelerate the recovery of a patient. However, there were some obstacles in providing medicine in Puskesmas. The informants stated the following.
… The availability of medicine was very limited here. There were many basic types of medicine that were not available at that time. I don’t really know what the problem was. (Informant G)
Even for the treatment of COVID-19 patients, the stock of medicine was also running out. This is exactly what happened according to the statement of Informant B.
The problem was the running out of the medicine availability for COVID-19 patients. (Informant H)
It cannot be denied that the availability of medicine for COVID-19 patients turned out to be a big problem.
Theme 2: The Impacts on the Essential Service Programs
Puskesmas in Indonesia develops programs having the orientation toward the community. The community service has had significant impacts. The limitation of the number of people and activity reduction caused the routine programs to be less active.
The health programs have the orientation toward preventive and promotive actions. The Puskesmas activities experiencing the most impacts happened to the groups that are the most vulnerable, who are pregnant women and children under five-year old.
Unlike the time before the COVID-19 pandemic, for example, there was a class for pregnant women, whose number of participants was 10 per group, but then the number was reduced. Then, the programs for community health (called UKM in Indonesian) that were established before the pandemic, such as the program to detect health problems of children, were also abolished during the pandemic. (Informant I)
It is true that those programs of community health were still carried out, but the purpose was just to maintain the health protocol, and it was not allowed to be conducted with the crowd or with a lot of people unlike before the COVID-19 pandemic; one of the programs that were still being carried out, for instance, was Posyandu (Integrated Service Post), where it held the class for pregnant women with a fewer number of the participants. The number could not be as many as before the pandemic in order to obey the health protocol. So some of the programs were still conducted but in a fewer number of participants. (Informant J)
Theme 3: COVID-19 Control
Testing
Testing is an element of the 3T principles determined by the government to cut the chain of COVID-19 transmission. In some cases of testing, there were still many people that did not want to be tested, and this happened because those many people still did not believe that there was such a disease called COVID-19 (as stated by Informant C). The officers had trouble convincing many people to check themselves as they were not willing to take the rapid test for COVID-19. This occurred due to the fact that during the pandemic many people thought that the positive result from the testing for COVID-19 would lead to negative consequences; for example, they would be isolated, and if they passed away, they would be buried in a place that they did not choose.
The health officers also relied on the workforce from outside the health sector. The workforce from outside the health sector is the police and military officers, as stated by Informant C as follows.
And many people at the beginning still did not believe that COVID-19 was a disease that could infect them; once there was one family showing the symptoms of COVID-19, yet they were not willing to take the test like the antigen test. Then we had to involve the police and military officers to make them do the test; it was the only way to make them give up and willing to take the test. Thus, the testing had to involve the police and military officers. (Informant C)
In addition, the testing results could not also be obtained right away. The informants complained that the testing results were usually conducted in phases, from the rapid antigen test to the obligation to make confirmation using PCR, even involving a complicated procedure and causing clashes with the community to happen. The testing procedure, which took a long time, made the officers unable to do anything when the community stated their protest or objection to be retested. Similarly, the officers were unable to force people when they did not allow their family members to be tested, even though they were suspected to be infected by COVID-19.
Screening
With the good testing, it was expected that the screening could also be carried out well in order to suppress the wider spread of COVID-19. However, the fact was that the Puskesmas itself did not do the testing to the community in order to carry out the screening well, despite the fact that screening was part of the government program that had to be carried out by Puskesmas.
Two informants stated that problem in the narrations below.
Screening here refers to a screening process of COVID-19 sufferers, but in this Puskesmas the screening process was not really conducted. It means this Puskesmas hadn’t conducted the screening, although it was already been planned to be carried out by the Puskesmas. The reality is that it was not really conducted. (Informant K)
I believe that every patient that came to Puskesmas had to do the antigen test, to do the screening, but that was not happening in this Puskesmas. The patient needed to be infected by COVID-19 first to be tested. (Informant L)
Both narrations above show that the screening was not really conducted in reality.
Tracing
Tracing could also be very helpful for Puskesmas to see the interaction map of the COVID-19 patients. With the tracing, it could prevent the transmission in the community that had the interaction with the patients.
However, many people refused to let the Puskesmas do the tracing. The informants stated that many people were not willing to be tested, although they had connection with certain cases of infected COVID-19 patients. Consequently, the officers felt that it was hard for them to work maximally.
If people had been cooperative, there would not have been a problem. If they had been willing to do the antigen test when we asked them to or if they had completed their data and sent them to us, everything would have been smooth. However, sometimes the people infected with COVID-19 did not want to send their data; they promised to send the data, but in the end they didn’t. That was the problem. (Informant A)
Such a condition clearly drained the energy of the health officers. On the one hand, the officers had to apply the principle of controlling COVID-19, but, on the other hand, the reality was not that easy.
When we get infected by COVID-19, we need to trace 15 people or 5 houses surrounding us because of having close contact or living in the same environment. Nonetheless, those neighbors were being difficult, especially for being dishonest about whether they just recently met people infected with COVID-19. They would say that they had not met those patients for a long time or they never met those patients in spite of being their neighbors. Thus, we still needed to do the tracing despite their answers because we believe as neighbors they must have been in contact somehow. Hence, we still did the tracing and we did the antigen test from one house to another. (Informant D)
Treatment
After there were testing and tracing, then treatment was required to be conducted by Puskesmas toward the patients infected with COVID-19. By conducting treatment, the COVID-19 transmission could be hampered as early as possible, before it occurred. However, it turned out there were obstacles in this treatment process. Informant A stated that the treatment they did just used vitamins they had at that time because Puskesmas did not receive suitable medicine with the standard. The narration below will provide the explanation.
The treatment for COVID-19 in Puskesmas was not done maximally since the medication comes from the Local Health Department, so when the Local Health Department did not have the medicine, then Puskemas also did not have the medicine. Thus, at the beginning our treatment just relied on vitamins found in Puskesmas, unless the patients could buy the medicine outside. We would prescribe the medicine that was in accordance with the standard, but if the patients could not afford the medicine and did not want to buy the medicine by themselves, then they would just take the vitamins for their treatment. Now we have the medicine, so the treatment can be carried out according to the standard. (Informant A)
The perspective on the medication limitation delivered by Informant A confirms what has been previously stated by Informant G.
Discussion
The facts above show us the narrations expressing basic issues when the COVID-19 pandemic occurred, particularly in Indonesia. Although the health policy had been formulated and stipulated by the government, the reality that happened in the field was very far different.
The fact about the health service in Indonesia is in an insufficient condition has been known before.21 There are many health services whose scope of use is quite good, but the health services that are not utilized are also found to be very significant in number22–24. This condition certainly indicates the disparity in the health service quality and uncovers the basic condition that really determines the health service responses toward a disease. The service scope difference reflecting this service quality is determined by the socio-demographical profile of a community.25 However, it cannot be denied that as stated by the informants these differences happen because the equipment and human resources in every health service unit have experienced problems for a long time. Important and basic conditions have often been ignored since a long time ago25 so that this leads to disaster when a disease spreads fast and intensively like the COVID-19 pandemic. Before the pandemic hit the world, the position of Indonesia in terms of its health service was still far behind the positions of other countries,26 and its position became even worse after experiencing the strike of the pandemic.
The information from the field recorded in an interview with the informants shows that the access of the community to the health service, particularly on COVID-19, was hampered because of the internal factor in the health service itself. COVID-19 handling indeed required extra hard efforts. Indonesia was one of the countries having difficulties in controlling COVID-19 due to the vast geographical distribution. Nevertheless, the issues faced were not just about the distrust and nonacceptance from the community.27 However, the big obstacles seen in this research come from the internal condition of the health service both before the pandemic and even worse during the pandemic.
The adequate medicine availability, the presence of the officers conducting the testing, and funding are three crucial things that should be available actually to carry out the health service,28 including for maintaining one’s health from a disease of COVID-19. In contrast, those three things were not easily deployed. The government bureaucracy mechanism prevented the fast and best service to be realized. Instead of becoming the mechanism that accelerates service, the bureaucracy procedure often hampered the performance of the health officers.
As in other places, even though it could be very effective, the tracing of COVID-19 cases was often refused by a community.29–32 The condition of Puskesmas with the lack of capacity eventually caused the health officers to be unable to play an active role. Even sometimes, the health officers also had to become the victims of negative perception. All of this existed in the insufficient environment for Puskesmas to be proactive. The uncertainty in many things hampered and slowed down the interaction and anticipation efforts that had to be carried out by Puskesmas.33
From the discussion aforementioned above, it is obvious that it is necessary to have an action that is more comprehensive and concrete based on the data to improve the ability of the health service at the highest level so that it can face the pandemic that we will never know when it appears and how its form will be. The pandemic that we have experienced has taught us to enhance the health system whether we like it or not,34 especially at the level of Puskesmas. Therefore, the studies that attempt to research the weaknesses of the health service need to be intensified to be conducted particularly now that when the pandemic is over, even though we will never know when the next pandemic strikes. The key to resistance toward any pandemic is the adequate preparation.35 Without the vaccine invention, the pandemic that we have gone through and hit the basic health service system might not be over.
This research was only conducted in one of the provinces in Indonesia. It might seem to reflect the condition in Indonesia. However, more research in detail is required to be conducted in every region to explore the issues specifically. This research also does not discuss the performance of the health officers specifically due to the time limitation in conducting the research.
Conclusion
This research concludes that the basic condition of Puskesmas in Indonesia requires improvement. The equipment to work on the report and the infrastructure to support the task were not really sufficient so that this led to the low performance in the field while overcoming COVID-19. The unsuitable early condition caused the efforts to fight against the spread of COVID-19 to be less effective and obtain negative critiques. The implementation of tracing the COVID-19 sufferers and the efforts of its medication is not easily conducted since the funding was lacking, the health workers also had to deal with the lack of medicine and equipment supplies. Consequently, the Puskesmas programs were often not suitable with the field reality. The analysis in this paper shows us that overcoming the COVID-19 pandemic was carried out in the far-from-ideal Puskesmas availability capacity. This condition, if not improved, will create serious problems when another pandemic strikes in the future.
Due to that condition, the health officials must immediately review all of the Puskesmas condition and restore the basic minimum service (both the equipment and the human resources) by calculating the workload after the pandemic. This reform has to be conducted properly, not only on the paper. If required, the reform policy of the primary health care has to be carried out by one person in charge nationally collaborating with all regions. Furthermore, the effort to optimize the reform needs to be performed by implementing specific simulation toward the equipment readiness and human resources. The simulation aims to discover the vulnerable points that need to be improved.
This research is still limited in the area scope, even though Medan can represent all urban areas in Indonesia. Besides that, the sample limitation also has the consequence on the limited research perspective, which might cause many other perspectives of health workers to have not been recorded. Such limitations could be the focus of the future research, as it is necessary to have research comparing area variation, so that information becomes more comprehensive. Moreover, it is crucial for future research to study the change dynamics or the adoption of the existing health service with the purpose to obtain the best performance of the primary care.
Acknowledgment
The writers are grateful to the Rector of Universitas Sumatera Utara via the Research Institution of Universitas Sumatera Utara that has funded this activity (No.6789/UN5.1 R/PPM/2021, dated16 June 2021). The writers would also like to express their gratitude to the Local Health Department of Medan and the Heads of Puskesmas involved in this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Statement on the fifteenth meeting of the IHR (2005) emergency committee on the COVID-19 pandemic; 2023a. Available from: https://www.who.int/news/item/05-05-2023-statement-on-The-fifteenth-meeting-of-The-international-health-regulations-(2005)-emergency-committee-regarding-The-coronavirus-disease-(covid-19)-pandemic?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQjwl8anBhCFARIsAKbbpyQCP7CqGizWMO3jy9WeJhTUZwRNRRX06ZWD6TCjrXFF5feUsryycwEaAtIJEALw_wcB.
2. World Health Organization. WHO Coronavirus (COVID-19) dashboard; 2023b. Available from: https://covid19.who.int/.
3. Satgas Penanganan Covid-19. Regulasi; 2024. Available from: https://covid19.go.id/p/regulasi.
4. Ayuningtyas D, Haq HU, Utami RRM, Susilia S. Requestioning the Indonesia government’s public policy response to the COVID-19 pandemic: black box analysis for the period of January–July 2020. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.612994
5. Djalante R, Lassa J, Setiamarga D, et al. Review and analysis of current responses to COVID-19 in Indonesia: period of January to March 2020. Prog Disaster Sci. 2020;6:100091. doi:10.1016/j.pdisas.2020.100091
6. World Health Organization. WHO’s 7 policy recommendations on building resilient health systems; 2021. Available from: https://www.who.int/news/item/19-10-2021-who-s-7-policy-recommendations-on-building-resilient-health-systems.
7. Jazieh AR, Kozlakidis Z. Healthcare transformation in the post-Coronavirus pandemic era. Front Med. 2020;7. doi:10.3389/fmed.2020.00429
8. World Economic Forum. (, July 19,). Why the world needs to rethink primary healthcare after the pandemic; 2021. Available from: https://www.weforum.org/agenda/2021/07/fixing-healthcare-after-covid/.
9. Mahendradhata Y, Lestari T, Djalante R. Strengthening government’s response to COVID-19 in Indonesia: a modified delphi study of medical and health academics. PLoS One. 2022;17(9):e0275153. doi:10.1371/journal.pone.0275153
10. Chen S, Li Y, Zheng Y, Wu B, Bardhan R, Wu L. Technical efficiency evaluation of primary health care institutions in Shenzhen, China, and its policy implications under the COVID-19 pandemic. Int J Environ Res Public Health. 2023;20(5):4453. doi:10.3390/ijerph20054453
11. Karreinen S, Rautiainen P, Keskimäki I, Satokangas M, Viita-aho M, Tynkkynen L-K. Pandemic preparedness and response regulations in Finland: experiences and implications for post-COVID-19 reforms. Health Policy. 2023;132:104802. doi:10.1016/j.healthpol.2023.104802
12. Sankar D H, Joseph J, Benny G, Nambiar D. Of primary health care reforms and pandemic responses: understanding perspectives of health system actors in Kerala before and during COVID-19. BMC Primary Care. 2023;24(1):59. doi:10.1186/s12875-023-02000-0
13. Moynihan R, Sanders S, Michaleff ZA, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. 2021;11(3). doi:10.1136/bmjopen-2020-045343
14. Donaghy E, Huang H, Henderson D, et al. Primary care transformation in Scotland: qualitative evaluation of the views of national senior stakeholders and cluster quality leads. Br J Gen Pract. 2023;73(728):e231–e241. doi:10.3399/BJGP.2022.0186
15. Kwan BM, Hamer MK, Bailey A, Cebuhar K, Conry C, Smith PC. Implementation and qualitative evaluation of a primary care redesign model with expanded scope of work for medical assistants. J Gen Intern Med. 2022;37(5):1129–1137. doi:10.1007/s11606-021-07246-x
16. Pope C. Qualitative methods in research on healthcare quality. Qual Saf Health Care. 2002;11(2):148–152. doi:10.1136/qhc.11.2.148
17. Pope C, Mays N. Qualitative Research in Health Care. Blackwell Publishing Ltd; 2006.
18. World Health Organization. Using qualitative research to strengthen guideline development; 2019. Available from: https://www.who.int/news/item/08-08-2019-using-qualitative-research-to-strengthen-guideline-development.
19. Merriam SB, Tisdell EJ. Qualitative Research.
20. Silverman D. Doing Qualitative Research. Statewide Agric Land Use Baseline. 2013;2015:870. doi:10.1007/s13398-014-0173-7.2
21. Paramita SA, Yamazaki C, Setiawati EP, Koyama H. Distribution trends of Indonesia’s health care resources in the decentralization era. Int J Health Plann Manag. 2018;33(2):e586–e596. doi:10.1002/hpm.2506
22. Limato R, Tumbelaka P, Ahmed R, et al. What factors do make quality improvement work in primary health care? Experiences of maternal health quality improvement teams in three Puskesmas in Indonesia. PLoS One. 2019;14(12):1–18. doi:10.1371/journal.pone.0226804
23. Mulyanto J, Kunst AE, Kringos DS. Geographical inequalities in healthcare utilisation and the contribution of compositional factors: a multilevel analysis of 497 districts in Indonesia. Health Place. 2019;60(August):102236. doi:10.1016/j.healthplace.2019.102236
24. Sarumpaet S, Hutahaean MM, Zaluchu F. An analysis of factors affecting pregnant woman’s use of prevention of mother-to-child transmission services in urban setting. Indian J Public Health Res Dev. 2018;9(10):780–785.
25. Mulyanto J, Kunst AE, Kringos DS. The contribution of service density and proximity to geographical inequalities in health care utilisation in Indonesia: a nation-wide multilevel analysis. Glob J Health Sci. 2020;10(2):020428. doi:10.7189/jogh.10.020428
26. World Health Organization. World Health Statistics 2020: Monitoring Health for the Sdgs, Sustainable Development Goals; 2020.
27. Sarumpaet S, Zaluchu F, Eyanoer PC, Simanjuntak NH. Fighting against COVID-19 and Fighting against Stigma: a. Open Access Maced J Med Sci. 2020;8(T1):522–525.
28. Herawati MH, Idaiani S, Veruswati M, Hoekstra K, Asyary A. Health information system concept in health services in the national health insurance (JKN) era in Indonesia: an environment and one health approach. Front Public Health. 2022;10(952415). doi:10.3389/fpubh.2022.952415
29. Braithwaite I, Callender T, Bullock M, Aldridge RW. Automated and partly automated contact tracing: a systematic review to inform the control of COVID-19. Lancet Digital Health. 2020;2(11):e607–e621. doi:10.1016/S2589-7500(20)30184-9
30. James A, Plank MJ, Hendy S, et al. Successful contact tracing systems for COVID-19 rely on effective quarantine and isolation. MedRxiv. 2020;0–20. doi:10.1101/2020.06.10.20125013
31. Juneau CE, Briand AS, Pueyo T, Collazzo P, Potvin L. Effective contact tracing for COVID-19: a systematic review. MedRxiv. 2020;1–25. doi:10.1101/2020.07.23.20160234
32. Kucharski AJ, Klepac P, Conlan AJK, et al. Effectiveness of isolation, testing, contact tracing, and physical distancing on reducing transmission of SARS-CoV-2 in different settings: a mathematical modelling study. Lancet Infect Dis. 2020;20(10):1151–1160. doi:10.1016/S1473-3099(20)30457-6
33. Kretzschmar ME, Rozhnova G, Bootsma MCJ, van Boven M, van de Wijgert JHHM, Bonten MJM. Impact of delays on effectiveness of contact tracing strategies for COVID-19: a modelling study. Lancet Public Health. 2020;5(8):e452–e459. doi:10.1016/S2468-2667(20)30157-2
34. Sachs JD, Karim SSA, Aknin L, et al. The Lancet Commission on lessons for the future from the COVID-19 pandemic. Lancet. 2022;400(10359):1224–1280. doi:10.1016/S0140-6736(22)01585-9
35. Bollyky TJ, Hulland EN, Barber RM, et al. Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet. 2022;399(10334):1489–1512. doi:10.1016/S0140-6736(22)00172-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.