")
Back to Journals » Patient Related Outcome Measures » Volume 14
NIH Toolbox Emotion Battery Findings Among People with HIV: Normative Comparisons and Clinical Associations
Authors Brody LA , Kamalyan L, Karcher K, Guarena LA, Bender AA , McKenna BS, Umlauf A, Franklin D, Marquine MJ, Heaton RK
Received 12 October 2022
Accepted for publication 28 January 2023
Published 15 February 2023 Volume 2023:14 Pages 15—30
DOI https://doi.org/10.2147/PROM.S391113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Lilla A Brody,1,2 Lily Kamalyan,2,3 Kayle Karcher,2 Lesley A Guarena,2 Alexis A Bender,4 Benjamin S McKenna,2 Anya Umlauf,2 Donald Franklin,2 Maria J Marquine,5 Robert K Heaton2
1Division of Geriatrics and Palliative Medicine, Weill Cornell Medicine, New York, NY, USA; 2Department of Psychiatry, HIV Neurobehavioral Research Program, San Diego, CA, USA; 3Joint Doctoral Program in Clinical Psychology, San Diego State University/University of California, San Diego, CA, USA; 4Division of Geriatrics & Gerontology, Department of Medicine, Emory University, Atlanta, GA, USA; 5Division of Geriatrics, Department of Medicine, Duke University School of Medicine, Durham, NC, USA
Correspondence: Robert K Heaton, Department of Psychiatry, UCSD School of Medicine, 9500 Gilman Drive, La Jolla, San Diego, CA, 92093-0603, USA, Tel +1 619 497-6659, Fax +1 619 260-8437, Email [email protected]
Purpose: Depression and other aspects of emotional health in people with HIV (PWH) can affect functional independence, disease progression, and overall life quality. This study used the NIH Toolbox Emotion Battery (NIHTB-EB), which assesses many features of emotional health, to more comprehensively investigate differences among adults living with and without HIV, and to identify factors associated with emotional health for PWH.
Patients and Methods: Participants (n=1451; age: M=50.19, SD=16.84; 47.90% women) included 433 PWH living in southern California seen from 2003 to 2021 (64.72% AIDS, 92.25% on antiretroviral therapy) and 1018 healthy participants from NIHTB-EB national normative cohort. Participants completed the NIHTB-EB and PWH underwent comprehensive HIV disease and psychiatric evaluations. We investigated differences in emotional health by HIV status via independent samples t-tests (continuous scores) and Chi2 tests (“problematic” emotional health scores). Multivariable linear regression models examined correlates of emotional health among PWH.
Results: PWH had significantly worse emotional health than people without HIV across Social Satisfaction (Cohen’s d=0.71, p< 0.001), Psychological Well-Being (Cohen’s d=0.49, p< 0.001) and Negative Affect (Cohen’s d=0.19, p< 0.01) summary T-scores, and most component scales. PWH also had higher rates of “problematic” emotional health, particularly in Social Satisfaction (45% vs 17%, p< 0.0001). Poor emotional health among PWH was associated with lifetime Major Depressive and Substance Use Disorders, relationship status (lost relationship versus in relationship), unemployment, and cognitive difficulties and loss of functional independence.
Conclusion: The NIHTB-EB identified that difficulties with multiple aspects of emotional health are common among PWH, and appear to be relatively independent of cognitive impairment as well as HIV disease and treatment history, but are strongly associated with everyday functioning. Given the cross-sectional nature of this study, longitudinal studies should be employed to evaluate causality pertaining to predictors of emotional health in PWH. These findings may inform interventions to promote emotional wellbeing in PWH.
Keywords: social relationships, depression, emotional health, positive factors, HIV infection
Introduction
Though modern antiretroviral treatment (ART) has vastly improved HIV-associated medical morbidity and mortality, people with HIV (PWH) still contend with the ramifications of the condition. Depression and anxiety are common among PWH, with reported rates across these conditions being two- to four-fold higher than for people without HIV (PWoH).1,2 Similarly, studies have shown that PWH report greater loneliness and perceived stress, as well as lower levels of meaning and purpose.3–5 Various factors may contribute to the increased likelihood of poorer emotional health among PWH. Adverse HIV-disease characteristics, such as delays in diagnosing infection and initiating antiretroviral therapy, have been associated with significantly higher odds of neurobehavioral difficulties that include both cognitive and emotional features.6,7 These features may not be independent, as HIV-associated neurocognitive disorder (HAND) and poorer daily functioning, both common among PWH, have been linked to worse depressive symptoms.8,9
Sociodemographic characteristics of PWH, including older age, unemployment, being born outside the US, and Black race/ethnicity have been associated with greater odds of depression.6,10 Further, there are various socioemotional and psychological factors prevalent in PWH that are known to increase the likelihood of depressive symptoms, such as prior trauma, experience of HIV-related stigma, sleep disturbance, perceived stress, lack of access to healthcare, and lower self-efficacy.11–17 On the other hand, several protective factors may mitigate the impact of living with HIV on adverse emotional health. For example, sense of belonging and perceived collective resilience, higher individual resilience, HIV-related optimism, and social support are factors that have been linked to better emotional health among PWH.3,6,18
Examining emotional health in PWH is important in relation to HIV treatment, particularly medication adherence. A meta-analysis of 29 studies involving PWH suggested that prevalence of mental health diagnoses and specifically having depression were associated with worse adherence to HIV treatment, and that receiving mental health treatment for depression was associated with greater likelihood of ART adherence than those who do not receive depression treatment.19,20 Higher positive affect in PWH is also associated with an increased likelihood in seeking HIV treatment, improved pain management, and viral suppression.20–22 While these prior studies provide important information about emotional health in PWH, they tend to use non-comprehensive measures, such as short-form scales or focus solely on negative aspects of emotion without addressing the effects of positive emotion. There may be aspects of emotion that short-form or negative emotion-centered measures do not capture well.
The NIH Toolbox Emotion Battery (NIHTB-EB) is an efficient, computer administered tool that evaluates a wide range of emotional functions. It consists of 17 individual scales and three summary scales that assess both positive and negative aspects of emotional functioning.23 The Toolbox could prove useful in efficiently detecting the presence of both poor emotional health, as well as emotional strengths in PWH.
To our knowledge, no research has yet assessed whether the NIHTB-EB summary scores or individual scales are comparable between healthy controls and PWH, or investigated the prevalence of problematic emotional health scores in a large sample of PWH. Therefore, we aimed to: 1) compare average and problematic emotional health (summary scores for Negative Affect, Social Satisfaction, Psychological Well-Being, and associated individual scales) between PWH and healthy adults; and 2) identify neurocognitive, sociodemographic and psychiatric factors that are associated with emotional health and risk of problematic emotional health among PWH. Due to high rates of depression, stigma, and other adverse socioemotional factors associated with living with HIV, we hypothesized that PWH would have significantly lower psychological well-being and social satisfaction summary T-scores, significantly higher levels of negative affect, and a higher prevalence of problematic emotional health than healthy controls. We also hypothesized that minority racial/ethnic identity, lower education level (a possible proxy for lower socioeconomic status and associated stress risk), more advanced HIV disease, and lifetime history of psychiatric comorbidities would predict worse emotional health among PWH.
Materials and Methods
Participants
Participants included 433 PWH and 1018 healthy adults. PWH were adults ages 18 to 87 enrolled in cohort studies at the University of California San Diego HIV Neurobehavioral Research Program (HNRP) between 2003 and 2021 who had completed the NIHTB-EB as part of their respective studies. All study procedures were approved by the UCSD Human Subject Protection Program (Study #s: 171024, 141702, 151568, 182064, 172092, 160075). Written informed consent was obtained from all study participants. Recruitment criteria were similar across studies, but where most studies excluded for severe confounds (ie Severe LOC > 30 minutes, non-HIV neurologic disorders), two studies did not. Despite this difference, PWH participants did not differ by study on the three summary scores (Negative Affect, Social Satisfaction, Psychological Well-Being). Exclusion criteria for PWH in the present analyses were missing data for more than one of the three summary scores in the NIHTB-EB and not being primarily English-speakers. All study participants were compensated for their participation. Compensation was based on the extent and number of studies procedures completed.
Healthy controls were participants from the NIH Toolbox national normative sample, ages 18–85.23 As part of the recruitment efforts of the normative study, these participants were healthy, community dwelling individuals randomly selected through databases compiled by market research companies and screened for being able to complete all of the NIHTB toolbox batteries, including emotion, cognition, sensory, and motor (with or without assistive devices), and able to follow directions in English (for further details see Babakhanyan et al, 2018; Beaumont et al, 2013). Participants were compensated for their participation.
Materials and Procedures
Demographic information (ie, age, sex/gender, race/ethnicity, and years of education) was gathered via self-report for all participants. PWH completed comprehensive and standardized HIV disease, neurocognitive, and psychiatric evaluations. All data included in this manuscript were obtained in compliance with the Helsinki Declaration and approved by the ethics committee of the UCSD Institutional Review Board. Participants provided written informed consent prior to their enrollment in the study.
NIH Toolbox Emotional Health
Emotional Health was measured by the NIHTB-EB.23,25 This battery is comprised of 17 scales, which assess different aspects of emotional and social wellbeing. The majority of the individual scales were combined into three summary scores through factor analysis in prior research: Psychological Well-Being (Positive Affect, General Life Satisfaction, and Meaning and Purpose), Social Satisfaction (Emotional Support, Instrumental Support, Friendship, and reverse coded Loneliness and Perceived Rejection), and Negative Affect (Sadness, Perceived Stress, Fear Affect, Anger Affect, Anger Hostility).25 Four other individual scales did not fit into the summary score models and are considered supplemental: Perceived Hostility, Fear/Somatic Arousal, Self-Efficacy, and Anger/Physical Aggression. Individual NIHTB-EB scales that are intended to measure positive aspects of emotional health include Positive Affect, General Life Satisfaction, Meaning and Purpose, Self-Efficacy, Friendship, Emotional Support, and Instrumental Support; negative aspects are tapped by Sadness, Perceived Stress, Loneliness, Perceived Rejection, Perceived Hostility, Anger-Affect, Anger-Hostility, Anger-Physical Aggression, Fear-Affect, and Fear-Somatic Arousal. Descriptions of these individual scales can be found in23 or under “NIH Toolbox Emotion Measures” on the website: www.healthmeasures.net.
Raw scores for each individual scale were converted into T-scores using 2010 US census-weighted demographic data for the average English speaker in the US.24 The T-scores therefore reflect an individual’s socioemotional health as compared to an average English-speaking adult in the US. To generate summary scores, researchers weighted each individual scale score by the confirmatory factor analysis loadings, then averaged across scales in that latent domain.23 Our primary analyses considered the three NIHTB-EB summary scores and 17 individual component subscales as outcomes. Summary T-scores beyond one standard deviation from the normative mean in the negative direction (Psychological Well Being T < 40, Negative Affect T > 60, Social Satisfaction T < 40) were categorized as “problematic” as in Babakhanyan et al, 2018 and used as outcomes in order to assess findings in a more clinically significant manner.23
Neurobehavioral Assessments of PWH
PWH completed the Composite International Diagnostic Interview (CIDI) (Version 2.1).26 Diagnoses for current and lifetime Major Depressive Disorder or Substance Use Disorders were assigned based on Diagnostic and Statistical Manual-Fourth Edition (DSM-IV) classifications. Participants who met criteria for current and/or lifetime abuse and/or dependence for the following substances were diagnosed with Substance Use Disorder by substance: alcohol, cannabis, opioids, methamphetamine, cocaine, sedatives and hallucinogens. The Beck Depression Inventory (Second Edition) (BDI-II) was used to evaluate presence and severity of current depressive symptoms.27 The BDI-II is a self-report measure on a 4-point scale, with higher scores indicating more severe depressive symptoms. Participants also completed self-report measures of everyday functioning, including the Patient’s Assessment of Own Functioning Inventory (PAOFI) and the modified Instrumental Activities of Daily Living scale (IADL).28,29 The PAOFI asks participants to assess cognitive functioning difficulties experienced in their everyday lives with cognitive functioning across multiple domains, using a 6-point scale from “almost never” to “almost always” with higher scores indicating more cognitive difficulties. The PAOFI measure also contains a question pertaining to employment, which was used to assess associations of NIHTB-EB scores with current employment status. The modified IADL scale asks participants to indicate whether they need more assistance now than they did at their best in 13 aspects of everyday functioning; it can be scored as a continuous variable, or as “IADL dependent” if the participant reports needing and obtaining more help with two or more activities of daily living. It is scored categorically for our analyses. As part of their parent studies at the HNRP, PWH completed a comprehensive test battery sensitive to HIV-associated neurocognitive impairment.30,31 Raw test scores were calculated and converted to demographically adjusted T-scores. Individual test T-scores were then converted into individual deficit scores ranging from 0 to 5.32 Deficit scores were averaged across all tests in the battery to compute a global deficit score (GDS) to categorize neurocognitive impairment among PWH (ie, GDS ≥ 0.5 as globally impaired; GDS < 0.5 as unimpaired).
HIV Disease Characteristics of PWH
HIV disease-related assessments included a standardized medical interview and neurological examination, as well as a blood draw, cerebrospinal fluid (CSF) collection from a consenting subset, and urine sample collection to screen for recent substance use. AIDS status, nadir and current CD4 levels, estimated years of infection, ART treatment status and regimen, and months of exposure to ART were gathered by self-report. Clinical chemistry panels, complete blood counts, rapid plasma reagin, Hepatitis-C (HCV) antibody, and CD4+ T cells (flow cytometry) were run. HIV RNA levels in plasma were measured by reverse transcriptase polymerase-chain reaction (Roche Amplicor, v. 1.5, lower limit of quantitation 50 copies per milliliter) in a CLIA-certified clinical laboratory. The Veterans Aging Cohort Study Index (VACS Index) was generated; this index uses HIV disease characteristics (eg, HIV-1 RNA, CD4 count), biomarkers (ie, hemoglobin, viral hepatitis C infection), and age to predict mortality risk, but it also has been associated with risk of neurocognitive impairment.33,34
Statistical Analyses
Differences in sociodemographic characteristics between groups (age, education, gender, ethnicity/race) were assessed using independent sample t-tests or Chi2 tests, as appropriate. Further characteristics regarding HIV disease, psychiatric history, and IADL status were evaluated for participants with HIV. For Aim 1, we employed independent sample t-tests and effect sizes (Cohen’s d) to examine differences in average NIHTB-EB scores (summary and individual scales) by HIV status, using an alpha of p < 0.01 due to our large sample sizes. Chi2 tests were used to assess differences in problematic summary T-score prevalence between groups. To investigate sociodemographic, clinical and functional variables associated with emotional health among PWH in Aim 2, we first ran univariable analyses for associations between individual sample characteristics (ie, sociodemographic, HIV disease, neurocognitive, psychiatric) and each of the three emotional summary T-scores, with an alpha of p < 0.01. For the factors showing univariable associations with any NIHTB-EB summary T-score, we ran separate multivariable linear regression models on each emotional outcome to identify any two-way interaction effects p < 0.01. Three final multivariable linear regression models were run for predicting NIHTB-EB summary scores, including variables that were univariably associated with the emotional health outcome of interest and any significant two-way interactions among these variables. Interaction terms and variables that were not significantly associated with the emotional health summary score at p < 0.01 were removed and the model was re-run. Significant interaction terms at p < 0.05 in the final models were followed up by stratified models to clarify these relationships. Analyses were completed using JMP software package (version 16.0.0). R version 3.5.0 was used to create figures.
Results
Descriptive Statistics
Comparisons of demographic information by HIV status are provided in Table 1. While the groups had comparable levels of education, PWH were older and had higher prevalence of male gender and Hispanic ethnicity than PWoH (ps < 0.01). However, none of these variables were associated with NIHTB-EB summary scores within the sample of PWH (Table 2).
 |
Table 1 Demographic Characteristics of the Study Cohort by HIV Status |
 |
Table 2 Univariable Associations Between Sample Characteristics and Each Emotional Summary T-Score Outcome Among PWH (n=433) |
Additional characteristics for PWH are presented in Table 3. The estimated mean duration of HIV infection was approximately 18 years, and the majority of these participants had an AIDS classification. The median nadir CD4 cell count was 175/μL (IQR, 31–304 μL), while current CD4 count was 617/μL. Most of the participants were on ART and, among those participants, a high percent had undetectable plasma and CSF HIV viral loads. Of the 289 participants who provided relationship status, over 60% had lost a relationship due to death of partner (41.52%) or separation/divorce (20.42%), whereas 23.53% were currently married or in a relationship and 14.53% described themselves as “single.” A majority of participants (71.87%) met criteria for lifetime histories of a Substance Use Disorder (SUD), the most prevalent of which were Alcohol Use Disorder and Methamphetamine Use Disorders; only 6% of the sample met criteria for a Current SUD. The majority also met criteria for lifetime Major Depressive Disorder (MDD) (60.05%), with less than 10% having current MDD (Table 3). Almost half (47.11%) of PWH were IADL dependent, with a similar proportion meeting criteria for neurocognitive impairment (44.06%) based upon the GDS. The average PAOFI Total score was 5.18 and only about one third of PWH were currently employed.
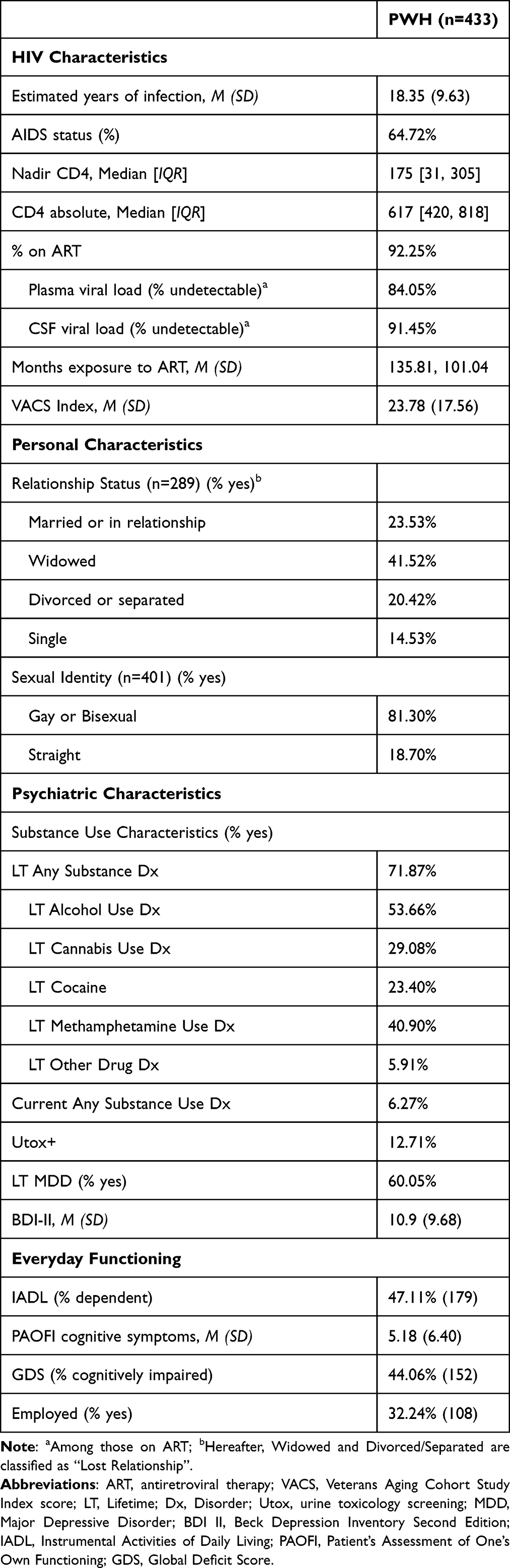 |
Table 3 HIV Disease, Substance Use, and Psychiatric Characteristics of the PWH Group |
Analyses of Emotional Health (NIHTB-EB) Summary T-Scores and Individual Scale T-Scores by HIV Status
Table 4 depicts emotional health summary scores and individual scale scores by HIV status. Compared to the healthy control group, PWH reported having marginally higher Negative Affect (p < 0.01) with a quite small effect size, but substantially lower Social Satisfaction (p < 0.001) with a medium-to-large effect size (d = 0.71), and Psychological Well-Being (p < 0.001, d = 0.49) with a small-to-medium effect size.
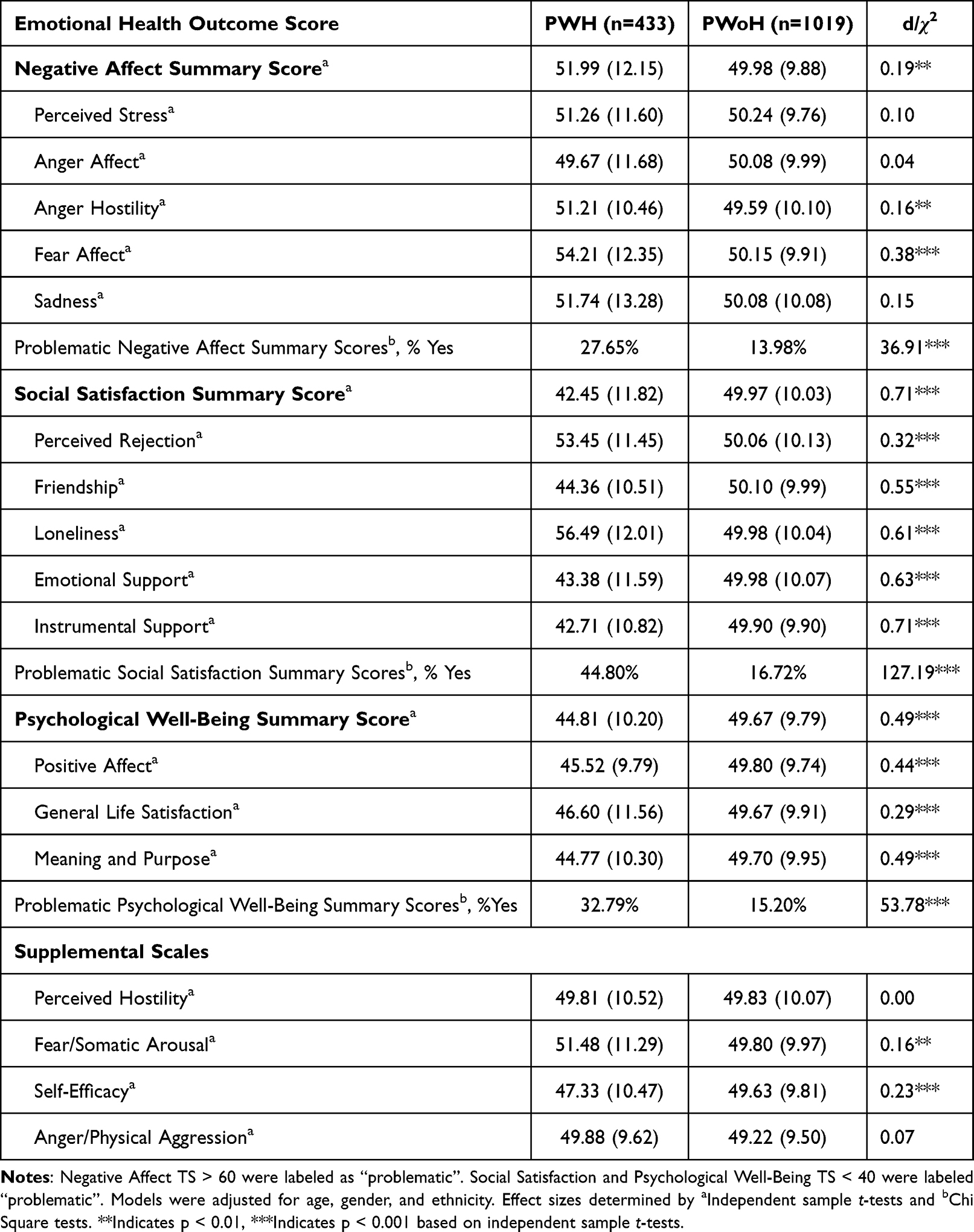 |
Table 4 Comparisons of NIHTB-EB Summary and Individual T-Scores by HIV Status |
In terms of the individual scales within the Negative Affect domain, PWH had higher Fear/Affect (related to anxiety) with a small effect size; Anger Hostility was statistically different, but the effect size was minimal. Within the Social Satisfaction domain, most individual scales evidenced medium effect sizes (Friendship, Loneliness, and both Emotional and Instrumental Support), with only Perceived Rejection showing a small but significant group difference (d = 0.32). Among scales within the Psychological Well-Being category, PWH were worse with small-to-medium effects on Positive Affect and Meaning and Purpose, with a smaller effect (d = 0.29) of lower General Life Satisfaction for the PWH. Among the supplemental scales, only Self-Efficacy was worse for PWH, with a small effect size (d = 0.23).
Given the demographic differences between HIV status groups, a subset of PWoH was randomly selected (n = 433) and matched with PWH based on age, gender, and ethnicity, and analyses were re-run. Results of the analyses across the matched groups were comparable to those of the larger unmatched sample.
Analyses of Problematic T-Scores by HIV Status
Substantially higher percentages of PWH obtained NIHTB-EB scores in a range that is considered “problematic” (potentially clinically significant) on the Social Satisfaction (44.8% vs 16.7%), and Psychological Well-Being (32.8% vs 15.2%) summary scores; the difference for Negative Affect was only slightly smaller (27.7% vs 14.0%) (all ps < 0.01) (Figure 1).
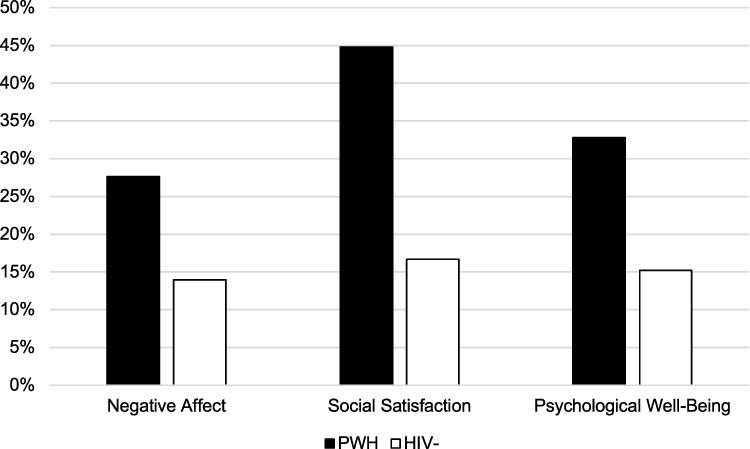 |
Figure 1 Prevalence of problematic emotional summary T-scores by HIV status. |
Univariable Analyses of Associations Between Individual Characteristics and NIHTB-EB Summary T-Scores Among PWH
For PWH, Table 2 presents results of univariable analyses between emotional health summary scores and sociodemographic, HIV disease, psychiatric and neurocognitive characteristics, as well as measures of everyday functioning. Sociodemographic information, HIV disease characteristics, and neurocognitive impairment were not significantly associated with any of the emotion summary T-scores. Having a history of lifetime, major depressive disorder was significantly associated with worse scores on all three NIHTB summary measures. Worse NIHTB-EB Negative Affect also was related to worse current depressed mood (higher BDI-II), as well as with IADL dependence and experience of cognitive difficulties in everyday life. IADL dependence and cognitive symptoms were significantly associated with all three summary scores. The group of PWH (14.53%) who described themselves as “single” did not have significant differences in Social Satisfaction from those either in or who have lost a relationship, and thus were excluded from multivariable analyses to further investigate the significant differences seen between those who were currently in a relationship and those who had lost one. Having a history of lifetime Any Substance Use Diagnosis was related to significantly lower Psychological Well-Being than those without such a history. Finally, being employed was significantly associated with greater Social Satisfaction and Psychological Well-Being summary scores.
Interactions Between Characteristics on Summary T-Scores in PWH
An interaction between depressed current mood (BDI-II) and IADL dependence was found to be significant for both Negative Affect (b = −0.36, 95% CI = −0.56 to −0.16, p<0.001) and Psychological Well-Being (b = 0.42, 95% CI = 0.23 to 0.61, p<0.001). For Negative Affect, individuals with independent IADLs had a stronger correlation between BDI-II and Negative Affect (b = 1.06, 95% CI =0.91 to 1.21, p < 0.0001) than those with dependent IADLs (b = 0.70, 95% CI =0.56 to 0.84, p < 0.0001) (Figure 2). Similarly, for PWH who were either independent or dependent in their IADLs, an increase in BDI-II was associated with a decrease in Psychological Well-Being, but those with independent IADLs had an even stronger correlation between BDI-II and Psychological Well-Being (b = −0.86, 95% CI =−1.00 to −0.71, p < 0.0001) than those with dependent IADLs (b = −0.44, 95% CI = −0.56 to −0.31, p < 0.0001) (Figure 3). No significant interactions were found for Social Satisfaction. Significant interactions for Negative Affect and Psychological Well-Being were included in their respective multivariable models.
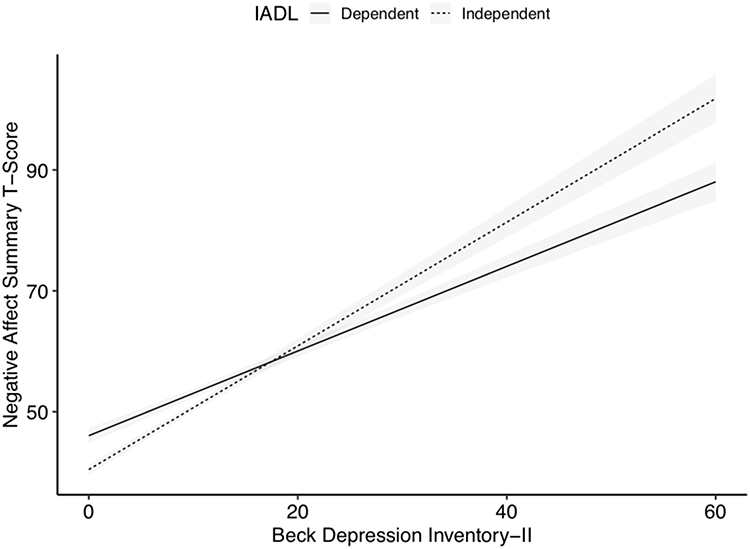 |
Figure 2 Interaction between IADL status and BDI-II score on Negative Affect summary score. Abbreviation: IADL, Instrumental Activities of Daily Living. |
 |
Figure 3 Interaction between IADL status and BDI-II score on Psychological Well-Being summary score. Abbreviation: IADL, Instrumental Activities of Daily Living. |
Multivariable Models with Interaction and Main Effects on Summary T-Scores in PWH
Table 5 presents results of the three final multivariable prediction models for the NIHTB-EB summary scores. The initial model for Negative Affect included all variables and the interaction term associated with this summary T-Score. We then removed PAOFI Total as it was not significant (p = 0. 58) within the context of the multivariable model, and the model was re-run. In the final model on Negative Affect summary scores, a history of lifetime Major Depressive Disorder was associated with worse current Negative Affect, and there was a significant interaction between IADL and BDI-II, which is depicted graphically in Figure 2. A follow-up stratified model by IADL status indicated that, for those who reported dependence in their IADLs, higher BDI-II resulted in significantly higher Negative Affect (R2 = 0.43, b = 0.70, 95% CI = 0.56 to 0.84, p < 0.001); however, for those with independent IADLs, there was an even stronger positive association between BDI-II and Negative Affect (R2 = 0.55, b = 1.03, 95% CI = 0.88 to 1.18, p < 0.001).
 |
Table 5 Multivariable Linear Models Predicting Emotional Summary T-Score Outcome by Sample Characteristics and Two-Way Interactions |
For Social Satisfaction, the first model included all variables univariably associated with Social Satisfaction. We removed PAOFI Total, decreases in IADL independence, lifetime MDD and employment status, as they were not significantly and uniquely associated with Social Satisfaction (ps > 0.05), and re-ran the model. Final results (Table 5) shows that BDI-II was negatively associated with Social Satisfaction (p < 0.001), and people who had lost romantic relationships (ie, Divorced, Separated, or Widowed) reported lower Social Satisfaction than those who were in relationships (ie, Married/in a relationship) (p < 0.01) (Table 5).
Finally, Table 5 shows the results of the multivariable model for Psychological Well-Being. We removed PAOFI Total and employment status due to lack of independent significance (ps > 0.05). In the final model, diagnoses of lifetime MDD and lifetime Any Substance Diagnosis were independently associated with significantly lower Psychological Well-Being, and there was a
significant interaction between IADL status and BDI-II (depicted graphically in Figure 3). For those with dependent IADLs, greater BDI-II was related to lower Psychological Well-Being (R2 = 0.30, b = −0.43, 95% CI = −0.55 to −0.32, p < 0.001), but an even stronger negative relationship existed for those with independent IADLs (R2 = 0.48, b= −0.79, 95% CI = −0.94 to −0.64, p < 0.001).
Discussion
We hypothesized that on the NIHTB-EB, PWH would have lower Social Satisfaction, lower Psychological Well-Being, higher Negative Affect, and a higher prevalence of problematic summary scores than people without HIV. Our analyses indicated that across all three summary scores of the NIHTB-EB, PWH reported poorer emotional health and had consistently higher rates of problematic emotional health scores than people without HIV. We found similar differences between HIV status among most of the 17 individual scales of the NIHTB-EB. A notable exception is that the PWH in this sample did not evidence adverse findings on the NIH-TB Sadness, Anger Affect and Perceived Stress components of the “Negative Affect” factor, nor on the Perceived Hostility or Anger/Physical Aggression supplemental scales. In particular, the lack of problematic “Sadness” would not have been expected given the high rate of lifetime MDD and evidence of currently depressed mood on the BDI-II; however, few of the PWH in this sample met criteria for current MDD, and scores on the NIHTB-EB Sadness scale were positively related to those on the BDI-II (r = 0.68, p < 0.0001).
To our knowledge, this is the first study that has used the full NIHTB-EB to examine patterns of emotional health and their predictors in PWH. The current findings generally support prior research indicating that PWH have more problematic emotional health than their peers within the general population.4,35,36 The fact that the PWH evidenced much more difficulty on some NIHTB-EB scales (eg, those reflecting problems and unhappiness with their social relationships) than others (eg, reflecting anger and hostility) speaks to the apparent specificity of individual scales and the potential clinical value of measuring a broad range of emotional health factors. As a further example of specificity of the NIHTB-EB components, relationship status among PWH was strongly related to Social Satisfaction, but was essentially unrelated to Negative Affect or Psychological Well Being. This suggests that relationship status is specifically related to Social Satisfaction, rather than tied to mental health more broadly.
The present study found that for those who are dependent in their IADLs, as compared to those who are independent in their IADLs, a higher level of depressed mood is less strongly associated with poor Negative Affect and Psychological Well-Being. Previous work within PWH has examined the relationship between functional status and depression, demonstrating that reported IADL dependence and depression are associated with unemployment and disability.37 As depression is a common comorbidity found in PWH, it would be important to further investigate its relationship to functional status and emotional health. Our analyses also illustrated significant associations with each summary score and lifetime diagnosis of psychiatric comorbidities, specifically lifetime Major Depressive Disorder and any Substance Use Disorder. The NIHTB-EB measures were shown to be related to these diagnostic conditions but still capture features outside of these clinical diagnoses, illustrating that the NIH Toolbox can give a broader understanding of emotional health, one which includes both positive and negative emotion. Lastly, as discussed above, we found that relationship status (In Relationship versus Lost Relationship) was related to Social Satisfaction. To our knowledge, no prior research has assessed the correlation between self-reports of relationship status and Social Satisfaction in PWH. However, some previous research has indicated that quality of personal relationships is associated with level of perceived social support, which is in turn related to mental health.38,39 If, as this research indicates, not being in a relationship significantly reduces Social Satisfaction, specifically or especially in PWH, future research should develop psychosocial interventions that might be used to improve social functioning aspects of emotional health in this population.
We also hypothesized that minority racial/ethnic identity, lower education level and more advanced HIV disease progression would predict worse emotional health among PWH. Contrary to these expectations, differences in racial/ethnic identity, education level, and HIV disease variables were not significantly related to emotional health summary scores. A majority (63%) of our participants living with HIV were Non-Hispanic (NH) Whites, but minorities were also well represented (N = 160; Table 1) and they did not evidence any worse emotional health than did their NH White counterparts (Table 2). Finally, over 80% of our sample living with HIV were on virally suppressive ART, reflecting a level of well-managed HIV disease, which may have contributed to lack of association between HIV disease characteristics in our sample and lower levels of emotional health.
This study has limitations. Our data for PWoH only consisted of the NIHTB-EB and basic demographic variables; thus, we could not compare other factors such as psychiatric comorbidities, IADLs and relationship status between HIV status groups, and observed associations between these factors and emotional health cannot be considered to be specific to PWH. Additionally, our samples were limited to English-speaking individuals and therefore our results cannot be generalized beyond this group of PWH. Future studies should examine these differences in populations of primary Spanish speakers and people with other language backgrounds, many of whom may face exacerbating factors pertaining to HIV. For example, Spanish-speaking Hispanic PWH have been found to face more stigma, and are more likely to have HIV diagnosed and treated later in their disease progression.40–42 These cumulative factors can impact HIV trajectories, so examining emotional health in minority and non-English speaking populations is vital.45 In the current analyses, we used individual scale scores and summary scores based on factor analysis in a normative population sample.43,44 Future research should examine the factor structure among PWH to ensure the generalizability of the factors identified in the national normative group. As our study was not focused on understanding the intersection between various identities (ie gender, sexual orientation, race/ethnicity, socioeconomic status) and associated differences in emotional health among diverse PWH, we recommend additional research to investigate these relevant combinations. Also, future longitudinal cohort studies should be conducted in order to better establish the directionality of our findings in PWH, particularly of the predictors of emotional health in this population. Despite these limitations, this study had numerous strengths, including the large sample size for both PWH and PWoH, and comprehensive data for PWH regarding neurocognitive and functional status, history of HIV disease and treatment, as well as psychiatric and substance use history.
Conclusion
Results of this study suggest that PWH experience a higher risk of emotional health difficulties and higher rates of problematic emotional health conditions than people without HIV. Specifically, psychiatric comorbidities, functional status, and relationship status were related to worse self-rated emotional health in PWH, which in turn may be manifested as poorer everyday functioning and quality of life. Future longitudinal studies should compare predictors of emotional well-being between people with and without HIV, particularly addressing causal effects of the associations reported here. These findings, as well as the assessments from the NIH Toolbox Emotion Battery, may inform future psychosocial interventions to promote wellbeing in people with HIV.
Acknowledgments
The HIV Neurobehavioral Research Center (HNRC) is supported by Center award P30MH062512 from NIMH. The San Diego HIV Neurobehavioral Research Center [HNRC] group is affiliated with the University of California, San Diego, the Naval Hospital, San Diego, and the Veterans Affairs San Diego Healthcare System, and includes: Director: Robert K. Heaton, Ph.D., Co-Director: Igor Grant, M.D.; Associate Directors: J. Hampton Atkinson, M.D., Ronald J. Ellis, M.D., Ph.D., and Scott Letendre, M.D.; Center Manager: Jennifer Iudicello, Ph.D.; Donald Franklin, Jr.; Melanie Sherman; NeuroAssessment Core: Ronald J. Ellis, M.D., Ph.D. (P.I.), Scott Letendre, M.D., Thomas D. Marcotte, Ph.D, Christine Fennema-Notestine, Ph.D., Debra Rosario, M.P.H., Matthew Dawson; NeuroBiology Core: Cristian Achim, M.D., Ph.D. (P.I.), Ana Sanchez, Ph.D., Adam Fields, Ph.D.; NeuroGerm Core: Sara Gianella Weibel, M.D. (P.I.), David M. Smith, M.D., Rob Knight, Ph.D., Scott Peterson, Ph.D.; Developmental Core: Scott Letendre, M.D. (P.I.), J. Allen McCutchan; Participant Accrual and Retention Unit: J. Hampton Atkinson, M.D. (P.I.) Susan Little, M.D., Jennifer Marquie-Beck, M.P.H.; Data Management and Information Systems Unit: Lucila Ohno-Machado, Ph.D. (P.I.), Clint Cushman; Statistics Unit: Ian Abramson, Ph.D. (P.I.), Florin Vaida, Ph.D. (Co-PI), Anya Umlauf, M.S., Bin Tang, M.S. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, nor the United States Government. This work was supported by grants from the National Institutes of Health: K01DA053985-01A1, T32AA013525 and T32DA031098.
Disclosure
Dr Maria J Marquine reports grants from University of California San Diego, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Heissel A, Zech P, Rapp MA, et al. Effects of exercise on depression and anxiety in persons living with HIV: a meta-analysis. J Psychosom Res. 2019;126:109823. doi:10.1016/j.jpsychores.2019.109823
2. Mendez NA, Mayo D, Safren SA. Interventions addressing depression and HIV-related outcomes in people with HIV. Curr HIV/AIDS Rep. 2021;18(4):377–390. doi:10.1007/s11904-021-00559-w
3. Heywood W, Lyons A. HIV and elevated mental health problems: diagnostic, treatment, and risk patterns for symptoms of depression, anxiety, and stress in a national community-based cohort of gay men living with HIV. AIDS Behav. 2016;20(8):1632–1645. doi:10.1007/s10461-016-1324-y
4. Pérez-Santiago J, Marquine MJ, Cookson D, et al. Gut microbiota dysbiosis is associated with worse emotional states in HIV infection. J Neurovirol. 2021;27(2):228–238. doi:10.1007/s13365-020-00933-1
5. Sikkema KJ, Kalichman SC, Hoffmann R, Koob JJ, Kelly JA, Heckman TG. Coping strategies and emotional wellbeing among HIV-infected men and women experiencing AIDS-related bereavement. AIDS Care. 2000;12(5):613–624. doi:10.1080/095401200750003798
6. Fisal ZAM, Minhat HS, Mohd Zulkefli NA, Ahmad N. Biopsychosocial approach to understanding determinants of depression among men who have sex with men living with HIV: a systematic review. PLoS One. 2022;17(3):e0264636. doi:10.1371/journal.pone.0264636
7. Heaton RK, Clifford DB, Franklin DR, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology. 2010;75(23):2087–2096. doi:10.1212/WNL.0b013e318200d727
8. Bryant VE, Whitehead NE, Burrell LE, et al. Depression and apathy among people living with HIV: implications for treatment of HIV associated neurocognitive disorders. AIDS Behav. 2015;19(8):1430–1437. doi:10.1007/s10461-014-0970-1
9. Kamat R, Morgan E, Marcotte TD, et al. Implications of apathy and depression for everyday functioning in HIV/AIDS in Brazil. J Affect Disord. 2013;150(3):1069–1075. doi:10.1016/j.jad.2012.11.040
10. Rueda S, Raboud J, Mustard C, Bayoumi A, Lavis JN, Rourke SB. Employment status is associated with both physical and mental health quality of life in people living with HIV. AIDS Care. 2011;23(4):435–443. doi:10.1080/09540121.2010.507952
11. Irwin MR, Archer G, Olmstead R, et al. Increased risk of depression in non-depressed HIV infected men with sleep disturbance: prospective findings from the Multicenter AIDS Cohort Study. EBioMedicine. 2018;36:454–460. doi:10.1016/j.ebiom.2018.09.028
12. Li J, Mo PKH, Kahler CW, et al. Prevalence and associated factors of depressive and anxiety symptoms among HIV-infected men who have sex with men in China. AIDS Care. 2016;28(4):465–470. doi:10.1080/09540121.2015.1118430
13. Murphy PJ, Garrido-Hernansaiz H, Mulcahy F, Hevey D. HIV-related stigma and optimism as predictors of anxiety and depression among HIV-positive men who have sex with men in the United Kingdom and Ireland. AIDS Care. 2018;30(9):1173–1179. doi:10.1080/09540121.2018.1445827
14. Rubin LH, Cook JA, Weber KM, et al. The association of perceived stress and verbal memory is greater in HIV-infected versus HIV-uninfected women. J Neurovirol. 2015;21(4):422–432. doi:10.1007/s13365-015-0331-5
15. Tao J, Vermund SH, Lu H, et al. Impact of depression and anxiety on initiation of antiretroviral therapy among men who have sex with men with newly diagnosed HIV infections in China. AIDS Patient Care STDS. 2017;31(2):96–104. doi:10.1089/apc.2016.0214
16. Wang N, Wang S, Qian HZ, et al. Negative associations between general self-efficacy and anxiety/depression among newly HIV-diagnosed men who have sex with men in Beijing, China. AIDS Care. 2019;31(5):629–635. doi:10.1080/09540121.2018.1549721
17. Watson CWM, Sundermann EE, Hussain MA, et al. Effects of trauma, economic hardship, and stress on neurocognition and everyday function in HIV. Health Psychol. 2019;38(1):33–42. doi:10.1037/hea0000688
18. McGowan JA, Brown J, Lampe FC, Lipman M, Smith C, Rodger A. Resilience and physical and mental well-being in adults with and without HIV. AIDS Behav. 2018;22(5):1688–1698. doi:10.1007/s10461-017-1980-6
19. Sin NL, DiMatteo MR. Depression treatment enhances adherence to antiretroviral therapy: a meta-analysis. Ann Behav Med. 2014;47(3):259–269. doi:10.1007/s12160-013-9559-6
20. Addington EL, Cheung EO, Moskowitz JT. Positive affect skills may improve pain management in people with HIV. J Health Psychol. 2020;25(10–11):1784–1795. doi:10.1177/1359105318769355
21. Carrico AW, Moskowitz JT. Positive affect promotes engagement in care after HIV diagnosis. Health Psychol. 2014;33(7):686–689. doi:10.1037/hea0000011
22. Wilson TE, Weedon J, Cohen MH, et al. Positive affect and its association with viral control among women with HIV infection. Health Psychol. 2017;36(1):91–100. doi:10.1037/hea0000382
23. Babakhanyan I, McKenna BS, Casaletto KB, Nowinski CJ, Heaton RK. National Institutes of Health Toolbox Emotion Battery for English- and Spanish-speaking adults: normative data and factor-based summary scores. PROM. 2018;9:115–127. doi:10.2147/PROM.S151658
24. Beaumont JL, Havlik R, Cook KF, et al. Norming plans for the NIH toolbox. Neurology. 2013;80(11, Supplement 3):S87–S92. doi:10.1212/WNL.0b013e3182872e70
25. Salsman JM, Butt Z, Pilkonis PA, et al. Emotion assessment using the NIH toolbox. Neurology. 2013;80(11, Supplement 3):S76–S86. doi:10.1212/WNL.0b013e3182872e11
26. Andrews G, Peters L. The psychometric properties of the composite international diagnostic interview. Soc Psychiatry Psychiatr Epidemiol. 1998;33(2):80–88. doi:10.1007/s001270050026
27. Beck AT, Steer RA, Brown G. Beck depression inventory–II. Psychol Assess. 2011. doi:10.1037/t00742-000
28. Chelune GJ, Heaton RK, Lehman RAW. Neuropsychological and personality correlates of patients’ complaints of disability. In: Goldstein G, Tarter RE, editors. Advances in Clinical Neuropsychology. Springer US; 1986:95–126. doi:10.1007/978-1-4613-2211-5_4
29. Heaton RK, Marcotte TD, Mindt MR, et al. The impact of HIV-associated neuropsychological impairment on everyday functioning. J Inter Neuropsych Soc. 2004;10(3). doi:10.1017/S1355617704102130
30. Cysique LA, Franklin D, Abramson I, et al. Normative data and validation of a regression based summary score for assessing meaningful neuropsychological change. J Clin Exp Neuropsychol. 2011;33(5):505–522. doi:10.1080/13803395.2010.535504
31. Heaton RK, Franklin DR, Ellis RJ, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol. 2011;17(1):3–16. doi:10.1007/s13365-010-0006-1
32. Carey CL, Woods SP, Gonzalez R, et al. Predictive validity of global deficit scores in detecting neuropsychological impairment in HIV infection. J Clin Exp Neuropsychol. 2004;26(3):307–319. doi:10.1080/13803390490510031
33. Justice AC, Freiberg MS, Tracy R, et al. Does an index composed of clinical data reflect effects of inflammation, coagulation, and monocyte activation on mortality among those aging with HIV? Clin Infect Dis. 2012;54(7):984–994. doi:10.1093/cid/cir989
34. Marquine MJ, Sakamoto M, Dufour C, et al. The impact of ethnicity/race on the association between the Veterans Aging Cohort Study (VACS) Index and neurocognitive function among HIV-infected persons. J Neurovirol. 2016;22(4):442–454. doi:10.1007/s13365-015-0411-6
35. Nguyen AL, Sundermann E, Rubtsova AA, et al. Emotional health outcomes are influenced by sexual minority identity and HIV serostatus. AIDS Care. 2021;33(9):1127–1132. doi:10.1080/09540121.2020.1785998
36. Vance DE. Self-rated emotional health in adults with and without HIV. Psychol Rep. 2006;98(1):106–108. doi:10.2466/pr0.98.1.106-108
37. Sadek JR, Vigil O, Grant I, Heaton RK; the HNRC Group. The impact of neuropsychological functioning and depressed mood on functional complaints in HIV-1 infection and methamphetamine dependence. J Clin Exp Neuropsychol. 2007;29(3):266–276. doi:10.1080/13803390600659384
38. Cederbaum JA, Rice E, Craddock J, Pimentel V, Beaver P. Social networks of HIV-positive women and their association with social support and depression symptoms. Women Health. 2017;57(2):268–282. doi:10.1080/03630242.2016.1157126
39. Reich WA, Lounsbury DW, Zaid-Muhammad S, Rapkin BD. Forms of social support and their relationships to mental health in HIV-positive persons. Psychol Health Med. 2010;15(2):135–145. doi:10.1080/13548501003623930
40. Chen NE, Gallant JE, Page KR. A systematic review of HIV/AIDS survival and delayed diagnosis among Hispanics in the United States. J Immigr Minor Health. 2012;14(1):65–81. doi:10.1007/s10903-011-9497-y
41. Gray KM, Valverde EE, Tang T, Siddiqi AA, Hall I. Diagnoses and prevalence of HIV infection among Hispanics or latinos — United States, 2008–2013; 2015. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6439a2.htm.
42. Levison JH, Levinson JK, Alegría M. A critical review and commentary on the challenges in engaging HIV-infected latinos in the continuum of HIV care. AIDS Behav. 2018;22(8):2500–2512. doi:10.1007/s10461-018-2187-1
43. Centers for Disease Control and Prevention. About HIV; 2022. Available from: https://www.cdc.gov/hiv/basics/whatishiv.html.
44. Lam A, Mayo NE, Scott S, Brouillette MJ, Fellows LK. HIV-related stigma affects cognition in older men living with HIV. JAIDS. 2019;80(2):198–204. doi:10.1097/QAI.0000000000001898
45. Guareña LA, Kamalyan L, Watson CW, et al. Associations of emotional health and neurocognition in Hispanic and non-Hispanic white persons with HIV. J Int Neuropsychol Soc. In press.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.