")
Back to Journals » International Medical Case Reports Journal » Volume 17
Miscarriage-Related Acute Kidney Injury: A Case Report
Authors Kojima J, Ono M , Tasaki K, Nagai T , Nagao T, Rinno S, Kanno Y, Yoshida R, Suzuki T, Kuji N, Nishi H
Received 25 November 2023
Accepted for publication 28 March 2024
Published 6 April 2024 Volume 2024:17 Pages 295—300
DOI https://doi.org/10.2147/IMCRJ.S451790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Junya Kojima,1 Masanori Ono,1 Koichiro Tasaki,2 Takeshi Nagai,2 Toshitaka Nagao,2 Sho Rinno,3 Yoshihiko Kanno,3 Rie Yoshida,1 Tomoo Suzuki,1 Naoaki Kuji,1 Hirotaka Nishi1
1Department of Obstetrics and Gynecology, Tokyo Medical University, Tokyo, Japan; 2Department of Anatomic Pathology, Tokyo Medical University, Tokyo, Japan; 3Department of Nephrology, Tokyo Medical University, Tokyo, Japan
Correspondence: Masanori Ono, Department of Obstetrics and Gynecology, Tokyo Medical University, 6-7-1, Nishishinjuku, Shinjuku, Tokyo, 160-0023, Japan, Tel +81-3-3342-6111, Email [email protected]
Background: Pregnancy-related acute kidney injury (Pr-AKI) is associated with significant maternal and fetal morbidity and mortality, with a three- to four-fold increase in perinatal mortality. Pr-AKI can arise from various obstetric complications, such as hyperemesis gravidarum, septic abortion, hypertensive disorders of pregnancy, pyelonephritis, and antiphospholipid antibody syndrome. Therefore, early diagnosis and appropriate intervention, including the identification of the underlying etiology, are important to effectively manage Pr-AKI. Therefore, we report a case of Pr-AKI after early miscarriage in a patient without hyperemesis gravidarum or septic abortion whose renal function gradually improved postoperatively for miscarriage.
Case Presentation: A 34-year-old primigravid woman was referred to us for perinatal management at 6 weeks of gestation. Unfortunately, she was diagnosed with miscarriage 1 week later. The patient had no history of hyperemesis gravidarum or septic abortion; however, she developed oliguria, and her serum creatinine and blood urea nitrogen levels were abnormally increased. Consequently, she underwent a renal biopsy to evaluate renal dysfunction, which indicated tubulointerstitial damage. The patient also underwent manual vacuum aspiration for a miscarriage. Postoperatively, her urine output increased, and her renal function improved. She was determined to have experienced Pr-AKI due to her miscarriage.
Conclusion: Our patient had Pr-AKI after a miscarriage in the absence of other causes. This case report highlights the presence of unknown causes of Pr-AKI, warranting further research for the development of preventive interventions.
Keywords: pregnancy-related acute kidney injury, miscarriage, missed abortion, creatinine, renal insufficiency
Introduction
Pregnancy-related acute kidney injury (AKI) (Pr-AKI) is a significant cause of maternal and fetal morbidity and mortality.1 The major risk factors for Pr-AKI include diabetes mellitus, hypertensive disorders of pregnancy (HDP), thrombotic microangiopathy, heart failure, pyelonephritis, sepsis, placental abruption, and postpartum hemorrhage2–4 Additionally, the prevalence of Pr-AKI ranges between 1 and 2.4 cases per 10,000,5,6 with an associated maternal mortality rate of 4% and 4% of survivors requiring permanent hemodialysis.2,7,8 Another potential risk factor for Pr-AKI is the use of assisted reproductive technology, which causes multiple gestation.1,9 The kidney plays an important role in the excretion of iodide,10 and several studies have examined the association between hypothyroidism and AKI.11,12 Hypothyroidism can also lead to AKI.13 Recently, the incidence of AKI has increased, possibly attributed to the increase in maternal age, maternal comorbidities, and the incidence rates of HDP and obesity.14,15
In addition, significant hemodynamic changes occur during pregnancy due to increased blood volume and cardiac output and decreased systemic vascular resistance. Consequently, systemic blood pressure reductions reach their lowest value by 20 weeks of gestation. Moreover, the glomerular filtration rate increases by approximately 50%, resulting in a hyperfiltration state and physiological reduction in serum creatinine levels.16,17 Unfortunately, diagnosing Pr-AKI poses challenges because the AKI diagnostic criteria for the general population, such as the Risk, Injury, Failure, Loss of kidney function and End-stage renal disease (RIFLE) criteria, Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, and Acute Kidney Injury Network (AKIN) criteria, have not been validated in pregnant women.9,14,18
In the first trimester, hyperemesis gravidarum and sepsis can cause Pr-AKI; they can lead to volume depletion and hemodynamic compromise, which, if severe, can cause pre-renal AKI and ischemic acute tubular necrosis. However, in the second and third trimesters, acute tubular necrosis can be caused by abruptio placentae; acute fatty liver of pregnancy; severe preeclampsia; and hemolysis, elevated liver enzymes, and low platelets syndrome.19,20 Furthermore, acute cortical necrosis can occur during severe hypotension,21 and the increased risk of cortical necrosis during pregnancy might be attributed to the hypercoagulable state.
Here, we describe the case of a patient who experienced miscarriage at 7 weeks of gestation, in the absence of hyperemesis gravidarum or sepsis, and presented with Pr-AKI. This case is unique because the patient experienced symptoms of renal failure, such as oliguria, after miscarriage, and these symptoms resolved following manual vacuum aspiration.
Case Presentation
The patient was a 34-year-old primigravid Japanese woman who had hypothyroidism, for which she had been prescribed levothyroxine sodium hydrate (50 μg/day). She presented to another clinic with genital bleeding and a 2-week delay in menstruation and obtained a positive result on a urine pregnancy test 2 weeks later. The patient was referred to our hospital for perinatal care. At 6 weeks of gestation, she had mild abdominal pain and no genital bleeding. Examination using a vaginal speculum revealed cervical erosion and moderate white discharge. Transvaginal ultrasonography revealed a gestational sac, a 9-mm fetus with a heartbeat, and a subchorionic hematoma in the uterus.
At 7 weeks of gestation, the patient experienced a miscarriage. She had a fever of 37.0–37.5°C, and her white blood cell count was within the normal range, with a C-reactive protein level of 1.0–2.0 mg/dL. Ultrasonography showed a 3 cm subchorionic hematoma, and her hemoglobin level was 9.0–10.0 g/dL, indicating mild anemia but no bleeding. Laboratory test results showed abnormal serum albumin (3.2 g/dL) and creatinine (6.69 mg/dL) levels, whereas sodium, potassium, and chlorine levels were within the normal ranges. She was seronegative for the human immunodeficiency, hepatitis B, and hepatitis C viruses, as well as the cardiolipin, antinuclear, anti-glomerular basement membrane, and anti-neutrophil cytoplasmic antibodies (c-ANCA and p-ANCA). However, she was seropositive for lupus anticoagulant. Protein C and S activity levels were normal. The patient had no history of diabetes mellitus, heart failure, pyelonephritis, sepsis, or hyperemesis gravidarum. She also experienced no symptoms of systemic lupus erythematosus, such as malar rash, oral ulcers, arthritis, leukopenia, and thrombocytopenia. The patient experienced oliguria, and her serum creatinine and blood urea nitrogen levels were abnormally increased. Qualitative urine test results showed strong positivity for occult blood and white blood cells but exhibited negativity for protein. Urine sedimentation test results showed erythrocytes; leukocytes; other tubular epithelial cells; and vitreous, granular, and epithelial cylinders. N-acetyl-β-D-glucosaminidase and β2 microglobulin were also detected in the urine.
A renal biopsy was performed without any complications approximately 10 days after miscarriage. Optical microscopy revealed cytoplasmic vacuolar degeneration of the tubular epithelium throughout the cortex. Focal tubular epithelial cell shedding, necrotic debris in the tubular lumen, and medullary tubular epithelium degeneration were also observed. The tubular interstitium showed mild edema and occasional focal infiltration of inflammatory cells, which were predominantly lymphocytes mixed with neutrophils and eosinophils (Figure 1). Immunofluorescence analysis revealed negativity for immunoglobulin G, immunoglobulin A, immunoglobulin M, complement component 3, complement component 1q, and complement component 4. Notably, no glomerular lesions were observed on light or electron microscopy; that is, renal biopsy findings indicated only tubulointerstitial damage. She was diagnosed with stage III AKI according to the RIFLE, AKIN, and KDIGO criteria. However, she was not diagnosed with septic abortion or hyperemesis gravidarum.
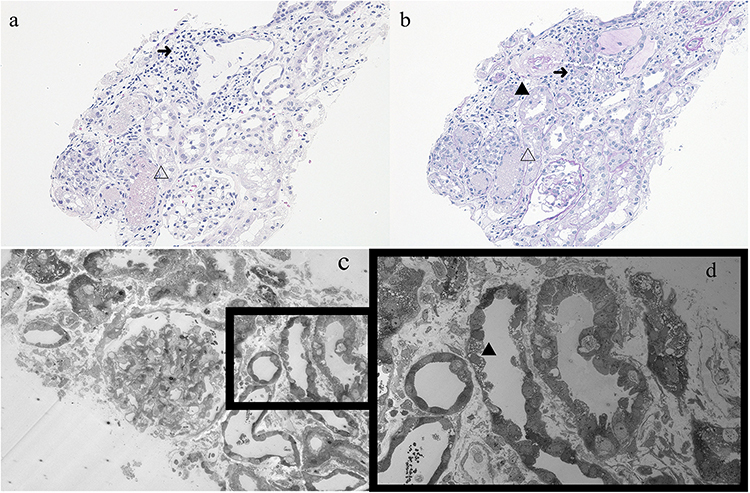 |
Figure 1 Light microscopy findings (×200). (a) Hematoxylin-eosin and (b) Periodic acid-Schiff-stained specimens show normal glomeruli and tubulointerstitial damage with tubular lymphocytic infiltration. (c and d) Electron microscopy findings. Normal glomeruli and nuclear and vacuolar degeneration in the tubules are observed (white arrows). Notes: ▲: cytoplasmic vacuolar degeneration of the tubular epithelium. Δ: necrotic debris of the tubular lumen. ➜: tubulointerstitial inflammation. |
The patient underwent manual vacuum aspiration under general anesthesia. At the time of surgery, her serum albumin and creatinine levels were 2.5 g/dL and 9.81 mg/dL, respectively. Urinalysis results showed a protein level of 0.28 g/dL and no white or red blood cells. Moderate bleeding occurred intra-operatively; however, the patient tolerated the procedure well. During the peri-operative period, the patient was treated with loop diuretics, and the urine output exceeded 0.5 mL/kg/h after treatment.
Notably, the patient’s urinary output and laboratory findings, including serum creatinine and blood urea nitrogen levels, improved without additional treatment. Urinalysis revealed no abnormalities. Histopathological examination of the resected endometrial tissue revealed decidual and implantation-related changes. Moreover, chorionic villi without enlargement, which consisted of syncytial trophoblast and cytotrophoblast cells, were observed. There were no findings indicative of molar pregnancy (Figure 2). After manual vacuum aspiration, the patient’s laboratory parameters and renal function recovered, and she had no complications (Figure 3). Antiphospholipid syndrome was ruled out as the lupus anticoagulant was negative postoperatively. The patient was discharged 3 days postoperatively.
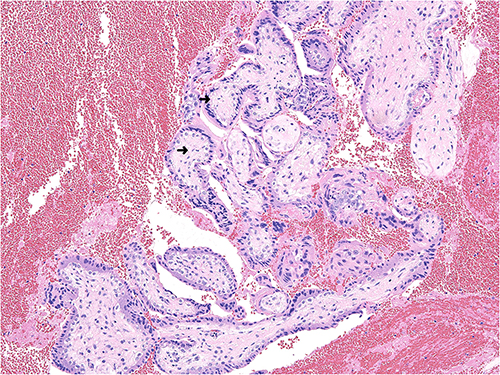 |
Figure 2 Light microscopy findings (×200). Hematoxylin-eosin–stained specimen shows chorionic villi without enlargement and decidua with hemorrhagic changes. Note: ➜: chorionic villi without enlargement. |
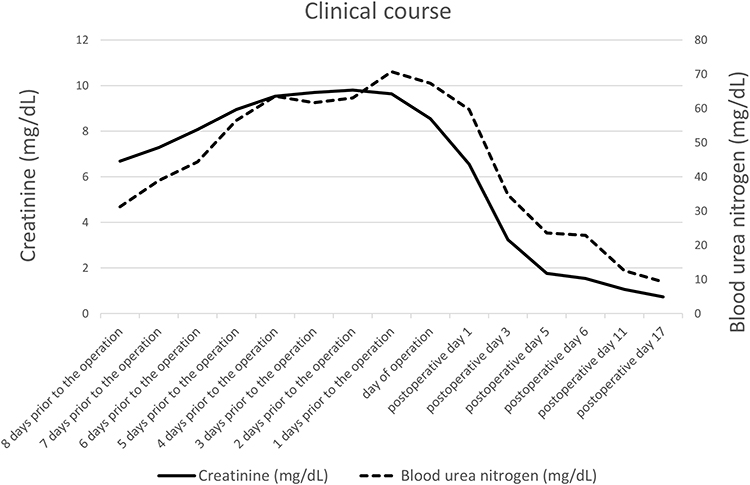 |
Figure 3 Blood urea nitrogen and serum creatinine levels during the peri-operative period. |
Discussion
The major risk factors for Pr-AKI include diabetes mellitus, HDP, thrombotic microangiopathy, heart failure, pyelonephritis, sepsis, placental abruption, and postpartum hemorrhage2,3 Malabsorption, septic abortion, and glomerulonephritis are the most common causes in the first trimester.22 Additionally, lupus nephritis and Sjogren’s syndrome, which can cause kidney injury during pregnancy, have been associated with miscarriages in the first trimester.23,24 Although acute cortical necrosis is an irreversible cause of intrarenal Pr-AKI, its exact pathogenesis remains unclear. The hypercoagulable state during pregnancy might lead to thrombus formation in interlobular and afferent arterioles, which is indicated by kidney biopsy findings of diffuse or patchy cortical necrosis.25 Generally, hyperthyroidism is known to result in a hypercoagulable state; however, some reports have revealed that hypothyroidism also leads to a prothrombotic state.26 Patients with hypothyroidism have increased fibrinogen levels and increased factor VII activity, which may have caused a prothrombotic tendency and resulted in Pr-AKI. However, more studies are needed to confirm whether the hypercoagulable state in early pregnancy leads to this pathology in the kidney.
The management of Pr-AKI requires close collaboration among clinicians, particularly nephrologists, obstetricians, and intensivists. Additionally, identifying the underlying etiology of Pr-AKI is crucial for appropriate treatment. Renal replacement therapy and pregnancy termination may be required to prevent further kidney injury. Moreover, most complications of Pr-AKI are treated similarly in pregnant and non-pregnant patients, involving the use of diuretics, cation-exchange resins, alkali therapy, and blood transfusion to treat volume overload, hyperkalemia, metabolic acidosis, and anemia, respectively. Although rare, the occurrence of Pr-AKI in the first trimester usually results from a septic abortion or prerenal azotemia secondary to hyperemesis gravidarum.27 However, these factors were not present in our patient.
Conclusion
To the best of our knowledge, Pr-AKI associated with miscarriage has not yet been reported. Our patient had Pr-AKI after miscarriage with retained products of conception at 7 weeks of gestation in the absence of sepsis or hyperemesis gravidarum. This report highlights the presence of unknown causes of Pr-AKI, warranting further research for the development of preventive interventions. Moreover, the management of Pr-AKI requires a multidisciplinary approach that involves nephrologists and obstetricians.
Abbreviations
HDP, hypertensive disorders of pregnancy; Pr-AKI, pregnancy-related acute kidney injury; AKI, acute kidney injury; RIFLE, Risk, Injury, Failure, Loss of kidney function, and End-stage renal disease; KDIGO, Kidney Disease: Improving Global Outcomes; AKIN, Acute Kidney Injury Network; ANCA, anti-neutrophil cytoplasmic antibodies.
Ethics Approval and Informed Consent
Institutional approval was not required to publish this case report.
Consent for Publication
The patient provided her written permission for the publication of her clinical information and clinical photos.
Acknowledgments
We are grateful to the patient and her family for their cooperation, and we acknowledge all our colleagues who helped us produce this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Grant-in-Aid for Scientific Research C (M Ono, 22K09556) and Grant-in-Aid for Early-Career Scientists (J Kojima, 22K16866) from the Ministry of Education, Culture, Sports, Science and Technology.
Disclosure
The authors declare no competing interests in this work.
References
1. Rao S, Jim B. Acute kidney injury in pregnancy: the changing landscape for the 21st century. Kidney Int Rep. 2018;3(2):247–257. doi:10.1016/j.ekir.2018.01.011
2. Hildebrand AM, Liu K, Shariff SZ, et al. Characteristics and outcomes of AKI treated with dialysis during pregnancy and the postpartum period. J Am Soc Nephrol. 2015;26(12):3085–3091. doi:10.1681/ASN.2014100954
3. Cooke WR, Hemmila UK, Craik AL, et al. Incidence, aetiology and outcomes of obstetric-related acute kidney injury in Malawi: a prospective observational study. BMC Nephrol. 2018;19(1):25. doi:10.1186/s12882-018-0824-6
4. Gurrieri C, Garovic VD, Gullo A, et al. Kidney injury during pregnancy: associated comorbid conditions and outcomes. Arch Gynecol Obstet. 2012;286(3):567–573. doi:10.1007/s00404-012-2323-5
5. Mehrabadi A, Dahhou M, Joseph KS, Kramer MS. Investigation of a rise in obstetric acute renal failure in the United States, 1999–2011. Obstet Gynecol. 2016;127(5):899–906. doi:10.1097/AOG.0000000000001374
6. Callaghan WM, Creanga AA, Kuklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. 2012;120(5):1029–1036. doi:10.1097/AOG.0b013e31826d60c5
7. Shah S, Meganathan K, Christianson AL, Harrison K, Leonard AC, Thakar CV. Pregnancy-related acute kidney injury in the United States: clinical outcomes and health care utilization. Am J Nephrol. 2020;51(3):216–226. doi:10.1159/000505894
8. Piccoli GB, Zakharova E, Attini R, et al. Acute kidney injury in pregnancy: the need for higher awareness. A pragmatic review focused on what could be improved in the prevention and care of pregnancy-related aki, in the year dedicated to women and kidney diseases. J Clin Med. 2018;7(10):318.
9. Suarez ML, Kattah A, Grande JP, Garovic V. Erratum regarding “Renal Disorders in Pregnancy: core Curriculum 2019” (Am J Kidney Dis. 2019;73[1]:119–130). Am J Kidney Dis. 2019;73(6):897. doi:10.1053/j.ajkd.2019.02.005
10. Pande A, Anjankar A. A narrative review on the effect of maternal hypothyroidism on fetal development. Cureus. 2023;15(2):e34824.
11. Bulur O, Dal K, Ertugrul DT, et al. Renal function improves with the treatment of hypothyroidism. Endocr Res. 2017;42(3):246–251. doi:10.1080/07435800.2017.1293686
12. Gondil VS, Chandrasekaran A, Rastogi A, et al. Proteinuria in severe hypothyroidism: a prospective study. J Clin Endocrinol Metab. 2021;106(2):e749–e756. doi:10.1210/clinem/dgaa871
13. Gou YL, Huang Y, Li JD, Chen H. Acute kidney injury induced by hypothyroidism: case reports and literature review. Asian J Surg. 2022;45(11):2347–2348. doi:10.1016/j.asjsur.2022.05.040
14. Taber-Hight E, Shah S. Acute kidney injury in pregnancy. Adv Chronic Kidney Dis. 2020;27(6):455–460. doi:10.1053/j.ackd.2020.06.002
15. Beers K, Wen HH, Saha A, et al. Racial and ethnic disparities in pregnancy-related acute kidney injury. Kidney360. 2020;1(3):169–178. doi:10.34067/KID.0000102019
16. Gonzalez Suarez ML, Kattah A, Grande JP, Garovic V. Renal disorders in pregnancy: core curriculum 2019. Am J Kidney Dis. 2019;73(1):119–130. doi:10.1053/j.ajkd.2018.06.006
17. Harel Z, McArthur E, Hladunewich M, et al. Serum creatinine levels before, during, and after pregnancy. JAMA. 2019;321(2):205–207. doi:10.1001/jama.2018.17948
18. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P; Acute Dialysis Quality Initiative workgroup. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204–R212. doi:10.1186/cc2872
19. Machado S, Figueiredo N, Borges A, et al. Acute kidney injury in pregnancy: a clinical challenge. J Nephrol. 2012;25(1):19–30. doi:10.5301/jn.5000013
20. Van Hook JW. Acute kidney injury during pregnancy. Clin Obstet Gynecol. 2014;57(4):851–861. doi:10.1097/GRF.0000000000000069
21. Prakash J, Pant P, Singh AK, Sriniwas S, Singh VP, Singh U. Renal cortical necrosis is a disappearing entity in obstetric acute kidney injury in developing countries: our three decade of experience from India. Ren Fail. 2015;37(7):1185–1189. doi:10.3109/0886022X.2015.1062340
22. Shah S, Verma P. Pregnancy-related acute kidney injury: do we know what to do? Nephron. 2023;147(1):35–38. doi:10.1159/000525492
23. Joshi A, O’Donoghue K, Mahmood U, Banerjee D, Banerjee A. Pregnancy outcomes in a patient with Sjogren’s disease with renal involvement. Obstet Med. 2013;6(4):175–178. doi:10.1177/1753495X13487323
24. Ku M, Guo S, Shang W, et al. Pregnancy outcomes in Chinese patients with Systemic Lupus Erythematosus (SLE): a retrospective study of 109 pregnancies. PLoS One. 2016;11(7):e0159364. doi:10.1371/journal.pone.0159364
25. Chugh KS, Jha V, Sakhuja V, Joshi K. Acute renal cortical necrosis--a study of 113 patients. Ren Fail. 1994;16(1):37–47. doi:10.3109/08860229409044846
26. Ordookhani A, Burman KD. Hemostasis in hypothyroidism and autoimmune thyroid disorders. Int J Endocrinol Metab. 2017;15(2):e42649.
27. Prakash J, Ganiger VC. Acute kidney injury in pregnancy-specific disorders. Indian J Nephrol. 2017;27(4):258–270. doi:10.4103/0971-4065.202406
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.