")
Back to Journals » International Medical Case Reports Journal » Volume 17
Minimally Invasive Resection of a Foraminal Lumbar Root Schwannoma
Authors Lee CC, Chuang HY, Chang CC, Lin HL, Cheng CH
Received 3 November 2023
Accepted for publication 5 February 2024
Published 12 February 2024 Volume 2024:17 Pages 125—129
DOI https://doi.org/10.2147/IMCRJ.S445098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Video abstract of “Foraminal Root Schwannoma” [445098].
Views: 37
Chien-Ching Lee,1,2 Hao-Yu Chuang,3,4 Che-Chao Chang,3,5 Hung-Lin Lin,6 Cheng-Hsin Cheng3,7
1Department of Anesthesia, An Nan Hospital, China Medical University, Tainan, 70965, Taiwan; 2Department of Medical Sciences Industry, Chang Jung Christian University, Tainan, 71101, Taiwan; 3Department of Neurosurgery, An Nan Hospital, China Medical University, Tainan, 70965, Taiwan; 4Department of Neurosurgery, China Medical University Beigang Hospital, Yunlin County, 65152, Taiwan; 5Neurophysiology Laboratory, Department of Surgery, National Cheng Kung University Medical Center and Medical School, Tainan, 70101, Taiwan; 6Department of Neurosurgery, China Medical University Hospital, Taichung, 40447, Taiwan; 7Graduate Institute of Medical Sciences, Chang Jung Christian University, Tainan, 71101, Taiwan
Correspondence: Cheng-Hsin Cheng, Department of Neurosurgery, An Nan Hospital, China Medical University, No. 66, Sec. 2, Changhe Road, Annan District, Tainan City, 70965, Taiwan, Email [email protected]
Background and Importance: This video article reports a rare case of a right L5/S1 foraminal root schwannoma that presents the natural course of the disease, imaging findings, treatment protocol, operative procedure, and highlights some of the possible surgical complications.
Clinical Presentation: Magnetic resonance imaging (MRI) revealed an intradural, extramedullary, well-enhanced mass at the right L5/S1 level. The operative procedure involved a right minimal L5/S1 laminotomy/foraminotomy posteriorly to open the right L5 root. The facet joints were preserved to prevent spinal instability. The tumor was located along the root after opening the right L5/S1 foramen. Intraoperative electromyography (IOM) was conducted to detect any nerve injury in the patient. After opening the dura, the tumor was carefully separated from the normal root nerve under IOM monitoring. The mass was removed piece-by-piece using mini-forceps.
Conclusion: Histopathological examination confirmed the diagnosis of a schwannoma. The patient recovered without incident after surgery with minimal soreness and numbness in the right leg.
Keywords: foraminal sacral root, foraminotomy, intradural extramedullary schwannoma, laminotomy, Schwannoma, spine tumor
Background and Importance
Surgical intervention should be considered for symptomatic lesions. Surgical results are related to the preoperative neurologic status. It may not be ideal to follow the tumor until the neurological defect has progressed. Tumor removal is indicated in patients with compressive symptoms of radiculopathy and myelopathy. A conventional T2-weighted magnetic resonance imaging (MRI) radiograph showed a mass lesion in the patient within the dura of the nerve root that was compressing the root nerve fiber (Figure 1A and B). It was diagnosed as a type B3 tumor according to the Nanda classification.1 Follow-up imaging for asymptomatic lesions was carried out to assess the risk of neurological deficit after surgery.
 |
Figure 1 The T2-weighted magnetic resonance imaging (MRI) radiographs are shown in sagittal (A) and axial view (B). The tumor compresses the nerve root to cause right L5 radiculopathy (arrow). |
Operating Room Preparation
Equipment Required
- Radiolucent operating room table
- Intraoperative fluoroscopy (C-arm).
- Television monitor.
- High-speed bur with 3mm and 4mm matchstick tip.
- Microscope.
- Dural patch and dural sealant gel.
- Intra-Operative Neuromonitoring (ION) to monitor motor-evoked and somatosensory evoked potentials of the lower limbs.
- Intraoperative ultrasonography equipment.
Positioning
The surgical procedure was performed under general anesthesia and the patient required full ventilator support for prone positioning. The patient was well-padded to prevent pressure sores and securely taped to avoid undesirable movements. The advantages of the prone position are as follows: 1) familiar anatomy for spine surgeons in this position and 2) more stable position with less movement during procedures; and 3) a more comfortable position for surgeons. Another important surgical position is the lateral-oblique or sitting position. Proper positioning reduces the operative time and C-arm radiation exposure. The C-arm and table positions should be carefully considered when switching between the anteroposterior and lateral views.
Surgical Technique
This operative procedure included separating the right L5 lamina from the midline and creating more space for the procedure through laminotomy and foraminotomy. Midline structures and muscle attachments should be preserved to reduce instability and postoperative pain. The facet joint should be preserved to prevent postoperative instability and back pain. If the right facet must be sacrificed to extend the surgical space, a transpedicular screw should be considered for rigid fixation. Patients should be preoperatively informed of the possibility of screw fixation if spinal instability occurs.
Step 1: Checking Patient Position, Wound Incision and Dissection
The classic posterior approach to the lumbar spine was employed with the patient in the prone position under general anesthesia. The location of the spinal tumor was identified with a K-wire using a C-arm before skin sterilization. The upper and lower ends of the tumor site were marked for proper operative wound incision. After proper surgical drape coverage, the skin was incised to a marked level. An electrocautery system was used to separate spinal bony structures. The avascular layer of the paraspinal musculature (spinal process and lamina) was maintained at the midline. The muscular component was separated from the lamina via subperiosteal dissection up to the medial aspect of the facet joint. After muscular dissection, the spinal location was confirmed using the C-arm. Once the exposure field had been confirmed, laminotomy and foraminotomy were performed using a 40 mm high-speed electrical burr. A high-speed burr was used until the flavum ligament was reached. The bony defect extended to the upper and lower levels of the flavum ligament. The Kerrison punches were carefully applied to remove the flavum ligament and the bony edge. The epidural fat and ligamentum were excised and the dural tissue was uncovered. Spinal root holes should be visible to ensure a better operative field. Bone wax was applied to the bone edge to prevent blood from oozing into the microscopic field of vision.
Step 2: Opening the Dura and Extending the Dural Defect
Before the durotomy, ultrasonography was helpful in confirming the tumor location and reducing the size of the dural opening. Using an operating microscope, a dural incision was made in the lesion area using a number 11 sharp knife (Figure 2). After a small durotomy, micro-ring forceps were used to split the dura and enlarge the dural defect. The tumor mass was exposed. Microdissection was used to check the upper and lower margins of the tumor and expose the dural defect until the normal nerve fiber was visible.
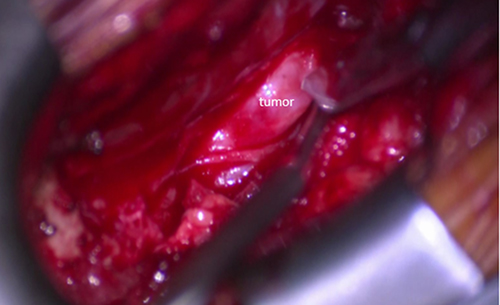 |
Figure 2 The right L5 root tumor is exposed. A number 11 sharp knife was used to make a small hole to open the dura. |
Step 3: Tumor Excision and Dural Defect Repair
The tumor was carefully separated from the normal nerve root fiber with a dissector and right-angle hook (Figure 3). A nerve stimulating monitor is useful to check the area of “safe zone” where the capsule can be removed without going through nerve tissue. First, the tumor was debulked internally to reduce its size. The adhesion band between the tumor and the nerve fiber was incised using microscissor. The spinal tumor was carefully released from the nerve fiber and displaced from the upper and lower end. Extensive dissection was carried out by gently lifting the tumor and examining the underlying root fiber. After releasing the partial tumor, better observation was possible on the ventral side of the tumor where the nerve root had been compressed. The nerve root may appear as a light greyish, necrotic gliotic nerve fiber due to severe compression; however, it is critical to realize that it may preserve functional nerve fibers and needs to be preserved. When there is doubt, it is helpful to check nerve function using an intraoperative monitor. Removing the tumor piecemeal by using micro-forceps is another good option if the tumor is too large to remove en bloc (Figure 4). Monitoring of the somatosensory and motor-evoked potential was carried out to confirm the preservation of nerve function after tumor excision.
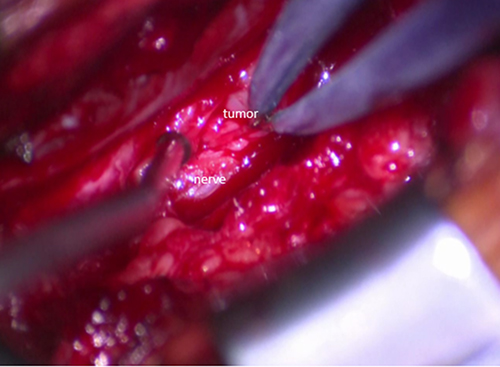 |
Figure 3 The lower margin of the tumor compared to normal nerve tissue. |
 |
Figure 4 A micro-forceps was used to remove the tumor piecemeal. |
Step 4: Closure
Since the dura is thin and short in the nerve root area, closing the sutures is difficult. The sandwich procedure (sequential use of the dura sealant gel, artificial dural graft, and dura sealant gel) was carried out without dura closure. First, a thin layer of the dura sealant gel was gently sprayed onto the nerve root. Subsequently, the artificial dural graft completely covers the dural gap. We employed the bovine pericardium in this patient, but other artificial dura products may be appropriate as long as they slide easily between the dura and the nerve root. It should be ensured that the artificial patch extends beyond the dural defect. Finally, another layer of the dura gel was placed on the dura patch for fixation. The levels of muscle, fascia, subcutaneous tissue, and skin were subsequently tightly closed layer-by-layer. The drainage tube was not used at the end of the procedure for this patient.
Complications
- Nerve root damage: this can happen during tumor separation and tissue coagulation.
- Leakage of cerebrospinal fluid (CSF) from the dural defect.
- Postoperative neurological deficit due to postoperative hematoma.
- Wound infection.
Discussion
The main purpose of surgery is to decrease nerve compression while lowering operative risk and provide symptomatic relief, prevent progressive neurological deficits, and avoid recurrence.2 In addition to MRI, and computed tomography (CT), CT myelography may also be useful for diagnosing spinal tumors and herniated discs. Preservation of the facet joint is key to preventing postoperative instability. However, damage to one side of the facet may not cause spinal spondylolisthesis or damage to the lower back. The fixation of transpedicular screws should be considered and prepared for prior to surgery, if it is necessary to remove the facet for better decompression and securing a wider operative field.3
For this patient, the dura in the root area was thin and short. The dural edge usually disappears after surgery when the root tumor is removed. Therefore, direct repair using the suture technique is difficult. The sandwich procedure is helpful in decreasing CSF leakage through compression and provides a waterproof layer. In addition, the CSF pressure in the root area for this patient was relatively lower than that in the spinal canal. CSF leakage is uncommon during manipulation of nerve root tumors.4 ION enables surgeons to check early warning signals of sensory and motor dysfunction accurately and quickly during surgery. This decreases the possibility of nerve damage.5
Conclusion
This is a case of lumbar root schwannoma with a video demonstration of the surgical procedure. We hope that this will serve as a detailed flow chart for those surgeons who deal with spinal tumors.
Compliance with Ethical Standards
The written informed consent was provided by the patient to have the case details and any accompanying images published. This study was exemption of Institutional Review Board (IRB) by Tainan Municipal An-Nan Hospital, China Medical University.
Consent Statement
The patient signed informed consent and publication of the data was authorized.
Funding
This work was supported by the Tainan Municipal An-Nan Hospital, China Medical University (ANHRF111-49). The funder had no role in the organization of the research, in the decision to publish the research data, in the writing of the article content, or in the interpretation of the results, analysis, or data collection.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Nanda A, Kukreja S, Ambekar S, Bollam P, Sin AH. Surgical strategies in the management of spinal nerve sheath tumors. World Neurosurg. 2015;83(6):886–899. doi:10.1016/j.wneu.2015.01.020
2. Antonopoulos C, Lilimpakis C, Karagianni M, Daskalopoulou D, Kyriakou T, Vagianos C. Ancient schwannoma of lumbar spine and review of the literature on paraspinal tumors, the role of preoperative biopsy: a case report. Cases J. 2009;2(1):9325. doi:10.1186/1757-1626-2-9325
3. Moses ZB, Barzilai O, O’Toole JE. Benign intradural and paraspinal nerve sheath tumors: advanced surgical techniques. Neurosurg Clin N Am. 2020;31(2):221–229. doi:10.1016/j.nec.2019.11.002
4. Safaee MM, Ames CP, Deviren V, Clark AJ. Minimally invasive lateral retroperitoneal approach for resection of extraforaminal lumbar plexus schwannomas: operative techniques and literature review. Oper Neurosurg. 2018;15(5):516–521. doi:10.1093/ons/opx304
5. Yilmaz B, Eksi MS, Toktas ZO, Kepoglu U, Konya D, Demir MK. Foraminal lumbar root schwannoma. Spine J. 2016;16(9):e595–596. doi:10.1016/j.spinee.2016.02.007
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.