")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Mindfulness Through Storytelling for Mental Health of Primary School Children: Impact on Acceptability and Its Associations with Personality
Authors Matiz A, Fabbro F, Crescentini C
Received 23 September 2023
Accepted for publication 21 February 2024
Published 25 April 2024 Volume 2024:17 Pages 1757—1774
DOI https://doi.org/10.2147/PRBM.S441494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Alessio Matiz,1,2 Franco Fabbro,3 Cristiano Crescentini1,3
1Department of Languages and Literatures, Communication, Education and Society, University of Udine, Udine, Italy; 2Department of Psychology, Sapienza University of Rome, Rome, Italy; 3Institute of Mechanical Intelligence, School of Advanced Studies Sant’Anna, Pisa, Italy
Correspondence: Alessio Matiz, via Margreth, 3, Udine, 33100, Italy, Tel +39 0432 249893, Email [email protected]
Purpose: Acceptability of mindfulness-based programs (MBPs) in primary school settings seems to represent a critical factor influencing the intervention effects on children’s mental health. This study aims at assessing the acceptability of an MBP delivered through the technique of storytelling, as well as identifying which participants’ personality characteristics can influence it.
Participants and Methods: Italian children in grades 3-to-5 (n = 147, 47.6% girls) participated in a 24-session MBP, which included 225 minutes of formal mindfulness practices and was delivered by the pupils’ school teachers. Children’s personality traits were assessed with the junior Temperament and Character Inventory (jTCI), while their subjective experiences and acceptability of the program were investigated using a survey containing open-ended and closed-ended questions.
Results: Program acceptability was 2.9 ± 0.7 on a 0– 4 scale. Higher jTCI scores of persistence, cooperativeness, and self-transcendence were related to higher ratings in liking the program, finding it useful and engaging themselves in it. Moreover, 57.8% of the children generalized the mindfulness practices in daily life and 93.9% of them declared they would recommend the program to their friends/parents. Five main themes emerged from children’s answers on what they learned: “help for difficulties (emotional, mental, and physical)”, “calm, relax, tranquility”, “resilience, positiveness, personal growth”, “self-exploration, interoception”, and “attention, concentration, and here-and-now”.
Conclusion: Program acceptability was generally higher than in similar programs in the literature, and children reported personal gains in various areas related to psychological well-being. The study also suggests which children’s personality traits should be considered when proposing an MBP in order to improve its acceptability and utility.
Keywords: mindfulness training, mental health, children, storytelling, thematic analysis, personality
Introduction
In the last forty years, mindfulness-based programs (MBPs) are increasingly being used and investigated through western scientific methods as secular and present-day adaptations of techniques rooted in the teachings of Siddhārtha Gautama, also known as the Buddha.1 During these programs, individuals are usually trained to regulate attention, observe interoceptive signals, and develop meta-cognition.2–4 The vast interest on MBPs is considerably due to the evidence of their effects on individuals’ psychological well-being, obtained in particular in adult samples. Various meta-analytic reviews have indeed highlighted the association between participation in these programs and self-reported improvements in anxiety, depression, and stress symptoms.5–7 These results are empirically supported from studies on the functional and structural brain changes associated with participation in these programs, more consistently observed in brain regions involved in the regulation of attention, emotion, and self-awareness.8,9
A couple of decades after the first studies on MBPs for adults, similar programs for children and adolescents began to be developed, mostly as adaptations for the youth of the original programs for adults.10 The progressive and rapid application of these programs in school and educational contexts anticipated more complete and better-founded theoretical and empirical proposals of these interventions for the youth, which have appeared only recently.11 Nowadays in this field, it is indeed possible to observe a proliferation of different MBPs for various educational contexts and age groups (pre-school and school children, pre-adolescents, and adolescents) combined with a generally low quality and inconclusive evidence of the effects of MBPs coming from the most comprehensive and recent reviews of the literature.12–15 It is nonetheless possible to observe that, despite the various limitations present in the reviewed research,16 MBPs may have positive impacts on measurements of anxiety or stress symptoms in children and, importantly, that the heterogeneity in study outcomes is moderate-to-large.11,15 In sum, it seems necessary to admit that “[w]e still know relatively little about which kinds of programs and practices, for which kinds of outcomes, for which students, at which ages, work best”.16
From this body of knowledge, it emerges in particular that the characteristics of programs, instructors, participants, and intervention settings appear to influence the outcomes of MBPs for the youth more than in adult samples: for example, it was found that MBPs’ effects on mental health and well-being of youth participants were generally greater14,15 when: i) the programs were delivered by a trained educator/teacher vs an outside facilitator, ii) selective vs general MBPs (eg, targeting individuals with a common clinical/subclinical condition vs the whole population group, such as a class or a school) were employed. The findings also showed that the younger vs older age of participants and the low vs high dose of practice during MBPs were aspects differently associated with distinct mental health outcomes.15
Arguably, one of the key difference between MBPs for adults vs youth participants may concern initial motivation to engage in such programs, whose practices require a considerable level of physical and attentional effort, especially during the initial training weeks.17 The primary role of motivation is recognized in the Liverpool Mindfulness Model as one of the core components that are involved in mindfulness practice.18 Adults normally choose to participate in an MBP and therefore may have an intrinsic motivation to engage in the practices. Dissimilarly, in particular during general vs selective approaches, the youth receive these programs from their teachers or therapists, who thus need to motivate them to accept and engage in this activity. Within current research on MBPs for the youth, motivation appears to be scarcely considered.
An effective way to provide meaning to an activity, thus motivating participants’ engagement and improving intervention acceptability (defined as the degree to which participants perceive an intervention as appropriate19), may be through the technique of storytelling. For humans, whose minds work within a narrative framework,20 this is an approach rooted in antiquity. For children, it is an instrument widely employed in educational and therapeutic settings.21–24 However, the use of storytelling for delivering MBPs is still almost unexplored, particularly in children, both in theoretical and experimental terms.25–27 It seems therefore relevant to explore from the point of view of students receiving the program the acceptability of an MBP delivered through storytelling. High intervention acceptability can indeed have a positive influence on its effectiveness, while low levels of acceptability can negatively affect intervention effectiveness. This has recently been shown in the largest-ever study on MBPs for the youth (n = 8376), which failed to show the superiority of a 10-week MBP delivered at school over a teaching-as-usual condition in promoting adolescents’ mental health:28 in this study, more than half of adolescents rated MBP acceptability below the 5.5 midpoint of a 0–10 scoring system,28 supplement G.
Besides the research question regarding global program acceptability, another issue appears to be critical for MBPs for youth, namely which participants’ characteristics can influence program acceptability. Besides individuals’ characteristics such as age, gender, and ethnicity, which can combine with intervention and instructor characteristics to influence program acceptability, a major role is probably played by participants’ personality. A large body of research in youth development has shown that this psychological construct influences children’s and adolescents’ social behavior, as well as their cognitive and school performance, eating behavior, physical activity, externalizing and internalizing psychopathological symptoms, and life satisfaction.29–35 Personality can thus clearly be a mediator of individual responses to any proposed activity. Therefore, knowledge about the relationship between young participants’ personality profiles and MBPs acceptability to them can be advantageous, for example, for mindfulness instructors to modulate their interventions in the presence of children or adolescents with specific personality traits that can undermine program acceptability.
This study focused on primary school children, who received a 24-session MBP delivered from their teachers through the technique of storytelling. The primary aim of the study was to investigate the acceptability of this MBP, measured by administering students with a post-intervention survey with both closed-ended questions (about how much children liked the program, how difficult they found it, how useful they found it, how much they were engaged in it) and open-ended questions (about what children learned from the program, whether and when they used one of its techniques in a difficult moment of their daily life, whether and why they would recommend it to their friends or parents). The secondary aim was to highlight which participants’ personality characteristics could influence intervention acceptability. This study, although carried out between 2020 and 2021, stands in the current fervid debate on the utility of MBPs for mental health promotion within school contexts.11,36–41
Materials and Methods
Procedure
The present study was realized in the context of teaching and research project funded in 2019 by the Prevention Department of the Italian autonomous region Friuli-Venezia Giulia (FVG) (see also42,43) and was carried out in collaboration with the local Public Healthcare System (ASUFC). The project was aimed at promoting psychological well-being at school through MBPs. The project was structured in four phases: i) 8-week Mindfulness-Oriented Meditation (MOM) training programs for teachers (from October 2019 to April 2020), ii) monthly booster sessions with teachers for supporting their individual daily MOM practice (from May to October 2020; see42), iii) training on the junior Mindfulness-Oriented Meditation (j-MOM) protocol for interested teachers (in September and October 2020), iv) j-MOM training programs for primary school children (delivered by their teachers under the supervision of the personnel responsible for the project who was also involved in phases i to iii) from October 2020 to April 2021). The present study focuses on the last phase of the project.
The study was conducted in 8 public schools (with 50–250 students each) of villages/small cities (1000–10,000 inhabitants) in the North-Eastern part of Italy (province of Udine in the Friuli-Venezia Giulia region). Eleven primary school teachers (all women), who had participated in phases (i)-(iii) of the project, took part in phase (iv) and were willing to collaborate in the study on the effects of the j-MOM program on their pupils. These teachers, who were requested to meditate daily for the entire duration of the project, delivered the j-MOM intervention to their pupils following the structure and contents of the j-MOM program during school time. In accordance with teacher and school organization, the interventions lasted from 8 to 24 weeks. In the weeks of these trainings, school activities were hampered by the second wave of Covid-19 infections in Italy: face masks were compulsory at schools, distance learning was usually guaranteed to infected or quarantined children and interruption of school activities for 1–2 weeks in separate classes was common. During the delivery of the j-MOM intervention, teachers were given support by experienced MOM trainers via in-presence meetings (wherever possible, due to the restrictions linked to the Covid-19 pandemic), phone calls, or electronic messages.
Before the beginning of the j-MOM training, the children were assessed at school with a personality questionnaire, the junior Temperament and Character Inventory.44 At the end of the j-MOM program, the children were asked during school time to fill a post-intervention survey containing four closed-ended and three open-ended questions (see Measures section and Table 1).
 |
Table 1 Feedback Form Given Out to the Children at the End of the j-MOM Program |
School managers agreed to the study. Parents of all participants provided written informed consent for their children’s inclusion in the study prior to study commencement. The study was approved by the Ethics Committee of the University of Udine, and all procedures performed in the study were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments. Finally, all data were analyzed anonymously, and data confidentiality was ensured.
Participants
The group of study participants consisted of 147 primary school children (3rd, 4th, and 5th graders from 12 classes). Participant demographics are presented in Table 2. These children were a subgroup of the 194 pupils who received the 24-session junior Mindfulness-Oriented Meditation (j-MOM) training programs that globally ran between October 2020 and April 2021 and were included in the research project described in the Procedure section. Children for whom informed consent to participate in the research was not obtained (n = 25) or that did not have a complete and valid assessment (n = 22) were excluded from the study.
Measures
Assessment of Program Acceptability
It was carried out using four closed-ended and three open-ended questions proposed to pupils at the end of their participation in the j-MOM program (see Table 1). Closed-ended questions were introduced by the following sentence, which made reference to Sid, the main character of the story told to the children during the j-MOM program (see below in Mindfulness-based program section): “What do you think of the course with Sid in which you have participated in the last weeks? Please answer the questions below by ticking each line. There are no right or wrong answers”.
Then, similarly to what was done for assessing acceptability of a MOM program for a sample of female school teachers in 2020,42 the following closed-ended questions were presented: q1) “Did you like it?”, q2) “How difficult was it?”, q3) “How useful was it for you?”, q4) “How much did you engage in it?”. Each question was rated on a 5-point Likert-type scale (0 = not at all, 4 = extremely). Questions q1, q3, and q4 provided direct measures of program acceptability, while question q2 provided an indirect measure of it (ie, it is a reversed item).
Then, the following open-ended questions were presented: q5) “What did you learn from Sid’s story?”, q6) “Did it happen that you used, in a difficult moment, the techniques that the good animals taught to Sid? If yes, which one did you use and when?”, and q7) “Would you recommend Sid’s story to your friends and parents? Why?”.
Personality
The Italian version of the junior Temperament and Character Inventory (jTCI)44,45 was used to assess the children’s personality profiles. This tool, developed and validated on 9- to 12-year-old children, is the child version of the widely used TCI personality inventory.46 It consists of 108 true/false items (105 scale items and 3 validity items). The jTCI is designed to assess seven scales, four reflecting temperamental traits (Novelty Seeking, NS, 18 items; Harm Avoidance, HA, 22 items; Reward Dependency, RD, 9 items; Persistence, P, 6 items) and three considering different facets of character (Self-Directedness, SD, 20 items; Cooperativeness, C, 20 items; Self-Transcendence, ST, 10 items). According to the psychobiological model of Cloninger et al,46 p. 266 temperament refers to “the automatic associative responses to emotional stimuli that determine habits and moods”, which are “moderately heritable and stable from childhood through adulthood”, whereas character can be seen as “the self-aware concepts that influence our voluntary intentions and attitudes”, and is “weakly heritable, but moderately influenced by sociocultural learning”. Example items are as follows: “Often I’m scared to try things I wish I could do” (HA), “I often try new things for fun or thrills” (NS), “I don’t open up much even with friends” (RD), “I work long after others give up” (P), “I feel strong enough, to master everything somehow” (SD), “I take good care not to hurt somebody with my actions” (C), “I believe in a higher force connecting all living beings” (ST). Cronbach’s alphas for the present study were in line with those reported in the validation study of the Italian jTCI (see Table 2 of 44) and reflected on average moderate (acceptable) reliability (mean values for the present study for the seven scales: 0.57 ± 0.16; mean values for the validation study44 for the seven scales for the 9- to 12-year group: 0.59 ± 0.09).
 |
Table 2 Participant Demographics |
Mindfulness-Based Program
The j-MOM program is an MBP delivered in group format for third to fifth graders. It was adapted for children from the Mindfulness-Oriented Meditation (MOM) training program for adults.47,48 The MOM training program is an 8-week MBP repeatedly studied in the last decade with psychological self-reports, as well as psychophysiological and neuroimaging techniques, in the general population49–57 and in clinical settings.58,59 The meditations during this program are practiced for 30 minutes a day while sitting, remaining still with eyes closed and include mindfulness of breathing (ānāpānasati), mindfulness of bodily sensations (body scan), and mindfulness of mental processes, such as thoughts or emotions (vipassanā). A previous adaptation for children of the MOM training program was studied on healthy and ADHD primary school pupils.60,61
The j-MOM intervention included the same practices of the MOM program (mindfulness of breathing, bodily sensations, and mental processes; see Table 3), proposed while the children were asked to remain seated on chairs while keeping a still and dignified posture, and with eyes closed. The duration of the practices for the children was shorter than in the adult MOM program, starting from 3 minutes during the first j-MOM session to 18 minutes during the last j-MOM session, for a total of 225 minutes of formal practice across the 24 sessions of the program. The meditation practices were proposed to the children through the reading of a fictional story entitled “Sid and the eight spheres of light”.62 In this story, the main character was a child named Sid; he needed to collect eight spheres of light, which were owned by eight wise animals (the dolphin of awakening, the frog of smile, the butterfly of feeling, the black forest deer, the wolf of emotion, the turtle of spontaneity, the monkey of time, the owl); in order to receive each sphere, the child had to engage in a mindfulness practice taught by the animal. The children participating in the intervention practiced the mindfulness exercises when the animals guided Sid in his practices. The speeches that the animals addressed to Sid allowed school teachers to convey to the children some theoretical aspects connected to mindfulness practice (see column“Theme” in Table 3), as is usually done during MBPs for adults. After mindfulness practices, the animals also inquired Sid of his meditative experience and the children listening to the story were invited to do the same, sharing their experiences with the class group.
 |
Table 3 Structure of the Junior Mindfulness Oriented Meditation (j-MOM) Program |
The j-MOM intervention was delivered by school teachers in their classes in 24 separate sessions, by following the 24 sections of the book “Sid and the eight spheres of light”.62 Each session lasted about 45 minutes (for a total of about 18 hours for the complete j-MOM program) and included the following activities: (i) listening to an introductory part of the story, (ii) mindfulness practice, (iii) experience sharing, (iv) listening to a concluding part of the story. The children were not asked to practice mindfulness at home (homework assignments were not a component of the j-MOM program).
Analysis
For the closed-ended questions q1, q2, q3, and q4 of the post-intervention survey, descriptive statistics were obtained. For each child, an Acceptability score was obtained from the q1, q2, q3, and q4 items (q1, q3, and q4 being direct items and q2 reversed item), by summing q1, (4 – q2), q3 and q4 divided by the number of items (ie, 4). Acceptability scores ranged, therefore, between 0 and 4.
For closed-ended questions q5 and q7, a thematic analysis was performed using the inductive approach proposed by Braun and Clarke.63,64 This is a manualized six-step method, which involves 1) familiarizing with the data, 2) generating initial codes (ie, labels for a feature of the data), 3) searching for themes, 4) reviewing potential themes, 5) defining and naming themes, 6) producing a report. For question q5, this analysis was employed for describing what the children declared they had learnt during the j-MOM program, while for q7 it was employed for describing why children would recommend the j-MOM training to their friends or parents.
For open-ended questions q6 and q7, descriptive statistics were obtained for highlighting how many children declared they had used, in a moment of difficulty, the techniques taught during the j-MOM program, which technique they had used, and when they had used it (q6), as well as for highlighting how many children declared they would recommend the j-MOM training to their friends or parents (q7).
Personality raw scores in the 7 scales of the jTCI questionnaire were converted to z-scores using the age- and gender-matched average scores of a normative sample studied during the validation of this questionnairein Italy.44 Questionnaires with a validity score equal or greater than 2 were excluded (this score was computed adding one point for each invalid response in the 3 validity items). In the present article, the relationship between these scores and the children’s answers in questions q1, q2, q3, and q4, as well as their Acceptability scores, were analyzed by means of Kendall’s correlation, which is a non-parametric statistic for non-normal distributions with a large number of tied ranks.
Finally, ratings in questions q1, q2, q3, and q4, Acceptability scores, as well as personality scores in the 7 scales of the jTCI questionnaire, were compared between the children who declared in question q6 that they used, in a moment of difficulty, the techniques taught during the j-MOM program and the children who declared they did not use them. These comparisons were performed using Welch's two samples t-test, which is robust to non-normality in data samples. Given the exploratory nature of these last comparisons, we decided not to use any correction for multiple comparisons when interpreting significant effects.
Data analysis was conducted using R, version 3.6.3.
Results
Closed-Ended Questions on Program Acceptability
Results of the children’s responses to questions q1-q4 are summarized in Figure 1 and Table 4. The Acceptability score had an average value of 2.9 (SD = 0.7).
 |
Table 4 Distribution of the Children’s Responses (n = 147) to Closed-Ended Questions q1-q4, their Resulting Statistics, and Statistics of Acceptability Score |
 |
Figure 1 Frequency plot of the children’s responses to closed-ended questions q1-q4 (left pane) and resultant Acceptability score (right pane). Notes: Response levels for questions q1-q4 (left pane): 0 = not at all, 1 = a little, 2 = moderately, 3 = a lot, 4 = extremely. The Acceptability score (right pane), for which question q2 is a reversed item, is computed as (q1 + 4 − q2 + q3 + q4)/4. |
Liking
In question q1, regarding how much the children liked the j-MOM training, most of them (75.5%) answered “a lot” or “extremely”, 15.0% “moderately”, 7.5% “a little”, and 2.0% “not at all”.
Difficulty
In question q2, regarding how difficult the j-MOM training was, most of the children (63.9%) answered “not at all” or “a little”, 24.5% “moderately”, 7.5% “a lot”, and 4.1% “extremely”.
Usefulness
In question q3, regarding how much the children found the j-MOM training useful, most of them (85.7%) answered “moderately”, “a lot”, or “extremely”, 9.5% “a little”, and 4.8% “not at all”.
Engagement
In question q4, regarding how much the children engaged in the j-MOM training, most of them (94.6%) answered “moderately”, “a lot”, or “extremely”, 3.4% “a little”, and 2.0% “not at all”.
Open-Ended Questions on Program Acceptability
What the Children Learned
In question q5, from the thematic analysis of the children’s responses (n = 147) on what they had learnt from the j-MOM program, five main themes emerged (see Table 5 and Supplementary Material Table S1).
 |
Table 5 Themes Emerging from the Children’s Responses (n = 147) to Question q5, Regarding What They Learned During the j-MOM Program |
Theme 1: calm, relax, and tranquility. The most recurrent theme emerging from the children’s answers was reported by 36.7% of them. Children reported that they learned “to calm down”, “to remain more calm”, “to keep calm”, “to become more tranquil”, “to relax”, “to stay relaxed”.
Theme 2: help for difficulties (emotional, mental, and physical). In the second theme, reported by 36.1% of the children, they reported that they learned techniques useful for managing their difficulties, mostly of emotional nature, but also mental and physical. They wrote, for example, that they learned “exercises useful for difficulty or anxiety”, “how to manage emotions in difficult times”, “not to get angry and to make a smile”, “that in the moments of fear or anxiety, I can use these techniques”, “when there is stress, anxiety and nervousness, you have to stay calm and meditate”, “to bear physical pain”, “to remove bad thoughts from the body”, “to keep thoughts at bay”.
Theme 3: resilience, personal growth, positiveness. This theme was reported by 26.5% of the children. Resilience and personal growth emerged when the children reported that they learned “not to give up”, “to engage”, “to get up again”, “to face difficulties”, “to face what we fear”, “to face pain”, “to be brave”, and that “everything can be overcome”. Positiveness emerged from the children’s answers as they wrote they learned “to forgive myself”, “to be serene”, “to be kind with everyone”, “to stay well”, “to think about when we will get better”, “to have fun”, “to smile”.
Theme 4: self-exploration, interoception. This theme was reported by 23.8% of the children. In their answers, they reported that they learned to listen to the body, or that it is necessary to listen to it, and to listen to emotions. This was expressed both in general (“I need to stay in touch with my body”, “you have to listen to your body”, “to feel if the body is good or bad”, “to listen to the breath and the body”, “to feel my emotions well”, “to feel emotions in the body”, “to listen to me more”), and in relation to a particular situation (“to feel my body when I was stressed or angry”, “to listen to my body and relax in the most difficult moments”, “that listening to your body is important especially when you feel bad or in difficulty”).
Theme 5: attention, concentration, and “here and now”. This theme was reported by 13.6% of the children. Regarding attention and concentration, they wrote that they learned “to concentrate”, “to keep my concentration”, “to manage distractions”, “not to get distracted”, “to stay still”. Regarding “here and now”, they wrote that they learned “not to think about the future, not to be in a hurry”, “not to be in a hurry, not to think too much about the future”, “not to think about the past/future”, “to think about here and now”.
The remaining answers were vague (from 3 children) or contained salient but infrequent topics (from 20 children), such as “to clean the mind”, “to reflect”, “to let thoughts go”, “to see how things really are”. A child did not answer the question.
Use of mindfulness techniques in daily life
In question q6, whose answers are summarized in Table 6, the children were asked whether, in a moment of difficulty in their daily life, they used the techniques taught during the j-MOM program. More than half of the children (57.8%) answered yes, 38.1% of them answered no, four children gave vague answers, and two children did not answer the question.
Moreover, the children that declared they used the techniques in daily life (ie, outside the j-MOM training) were asked which technique they used and when. The most employed technique was mindfulness of breath (54.1% of the children who declared they used the techniques in daily life), followed by mindfulness of thoughts (14.1%), and mindfulness of body, in particular regarding unpleasant sensations (11.8%). In relation to when these techniques were used, the following categories were identified: children reported that they used the techniques in the presence of negative emotions (“when I’m anxious or angry”, “when I go on a rampage with my sister”, “in moments of nervousness”, “to keep calm even if someone makes me angry”, “when my grandmother made me angry”), physical pain (“when my knee hurt”, “when some part of my body hurts”, “when I felt bad”, “[when] I had a headache”), tests or difficulty (“for school tests”, “when I got distracted”, “in difficult situations”, “in difficult times to concentrate better”, “at night at home to fall asleep”), agitation (“to stay calm, not to fret”, “when I am agitated”), and challenging thoughts (“when I had bad thoughts”, “when I had too many thoughts in my head”, “when I have too many thoughts in mind”).
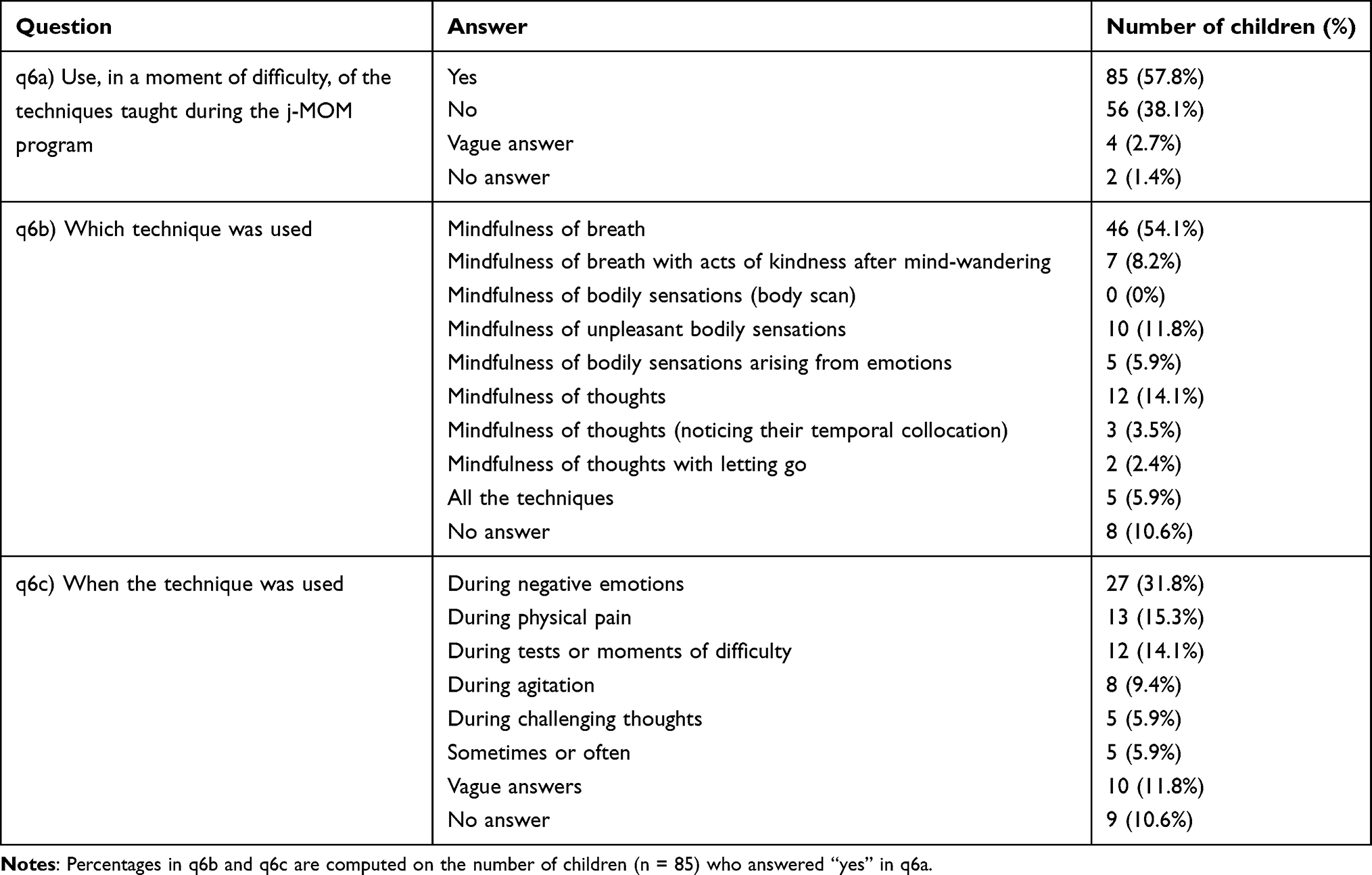 |
Table 6 Summary of the Children’s Answers to Question q6, Regarding Whether They Used in a Moment of Difficulty the Techniques Learned During the j-MOM Program, and, in Case, Which Technique and When |
The children who declared in question q6 that they used in daily life the techniques taught during the j-MOM program were compared with the children who declared they did not use these techniques in daily life in terms of their answers in questions q1, q2, q3, and q4, as well as Acceptability scores. The children who declared they used the mindfulness techniques in daily life had higher scores in questions q1 (“liking”; t = 4.0, p < 0.001) and q3 (“usefulness”; t = 3.7, p < 0.001), as well as in the Acceptability score (t = 3.2, p = 0.002) (see Table 7). These two groups were also compared in terms of jTCI personality traits (see below Section Associations of program acceptability with personality traits).
 |
Table 7 Comparison of Ratings in the Answers to Questions q1, q2, q3, q4, and Acceptability Scores Between the Children Who Answered “Yes” (n = 85) and the Children Who Answered “No” (n = 56) in Question q6, Regarding Whether They Used, in a Moment of Difficulty, the Techniques Taught During the j-MOM Program |
Recommendation of the Program to Friends and Parents
In question q7, whose answers are summarized in Table 8 (see also Supplementary Material Table S2), the children were asked whether and why they would recommend the j-MOM program to their friends and parents. Most of the children (93.9%) answered that they would recommend it, six children (4.1%) answered that they would not, a child answered “maybe”, a child gave an indefinite answer, and a child did not answer. Regarding the reason for which the children would recommend the j-MOM program, four themes emerged.
 |
Table 8 Summary of the Children’s Answers to Question q7, Regarding Whether and Why They Would Recommend the j-MOM Program to Their Friends and Parents |
Theme i: negative emotions, negative thoughts, stress, pain, conflict, and difficulties. This was the most recurrent theme, reported by 34.7% of all 147 children. They wrote that they would recommend the j-MOM program “to my parents because they are often under stress from work, because mom has to clean the house or because they have to work all day” “to my mom because in these months she is very nervous and these exercises could perhaps help her”, “to my grandmother because she has so much pain”, “because it helps so much to remove bad thoughts”, “because breathing is recommended for the agitated and those with many ugly and evil thoughts”, “to my parents because they always fight and get angry”.
Theme ii: calm, tranquility, relax, and well-being. This theme was reported by 29.3% of the children. They wrote that they would recommend the j-MOM program “because it calms you down”, “because it teaches you to stay calm when you’re sad or angry”, “because it can help them calm down when they fight”, “to keep them relaxed and quiet”, “because it would make everyone feel good”.
Theme iii: helpful, educative, transformative. This theme was reported by 27.2% of the children. They wrote that that they would recommend the j-MOM program “because it gives you really useful techniques”, “because it is very useful in times of stress”, “because it could be useful in a moment of anger, depression or difficulty”, “because it teaches techniques that can be used every day”, “because it serves for life”, “because it makes you learn a lot about your behavior”, “because I have changed and I would recommend it”.
Theme iv: beautiful, interesting, funny. This theme was reported by 25.2% of the children. They wrote that that they would recommend the j-MOM program “because it is very beautiful” “because it was very informative, nice and intelligent”, “because it’s a very inspiring and funny story”, “because the story is wonderful for everyone (big and small)”, “because I loved it”.
The remaining answers of children that declared they would recommend the j-MOM program were vague (from three children) or contained salient but infrequent topics (from eleven children), such as “to develop concentration”, “to check whether the body is well or bad”, “to listen to the body”, “it teaches you to overcome every obstacle”. Eight children who would recommend the j-MOM program did not give reasons for their answer. Among the six children that declared they would not recommend the j-MOM program, three found it uninteresting (“it’s a bit boring and so I don’t want to bore others”, “they won’t be interested”, “because none of my family members or friends care”), two found it useless (“I don’t think it can help someone”, “we are not afraid of anything”), and one wrote “because I do not have the courage to tell it [to my parents] and I am ashamed”.
Associations of Program Acceptability with Personality Traits
The personality profiles of the study participants with valid jTCI questionnaires (n = 147) were close to the reference population:44 for all the seven jTCI scales, z-scores fell within 0.38 standard deviations above or below the average population scores (see Supplementary Material Table S3).
In the correlations between the children’s answers in questions q1, q2, q3, q4, Acceptability score, and scores in the jTCI scales, the following results emerged, as summarized in Table 9. Higher scores in the degree of liking the j-MOM program (question q1) were associated with higher jTCI scores in persistence (r = 0.226, p < 0.001), cooperativeness (r = 0.196, p = 0.002), and self-transcendence (r = 0.140, p = 0.029). Higher ratings of usefulness of the j-MOM program (question q3) were associated with higher jTCI scores in cooperativeness (r = 0.125, p = 0.046). Higher degree of self-engagement during the j-MOM program (question q4) was associated with higher jTCI scores in persistence (r = 0.138, p = 0.034) and cooperativeness (r = 0.246, p < 0.001). Similarly, higher Acceptability scores were associated with higher jTCI scores in persistence (r = 0.157, p = 0.009) and cooperativeness (r = 0.179, p = 0.002).
 |
Table 9 Correlation Matrix Between the Children’s Answers to Questions q1, q2, q3, q4, Acceptability Score, and jTCI Scores in Its Scales (n = 147) |
Moreover, when jTCI scores were compared between the children who declared in question q6 that they used, in a moment of difficulty, the techniques taught during the j-MOM program and the children who declared they did not use them, it emerged that the children who declared they used the mindfulness techniques in daily life had higher scores in the jTCI scale of self-transcendence (t = 2.0, p = 0.043) (see Table 10).
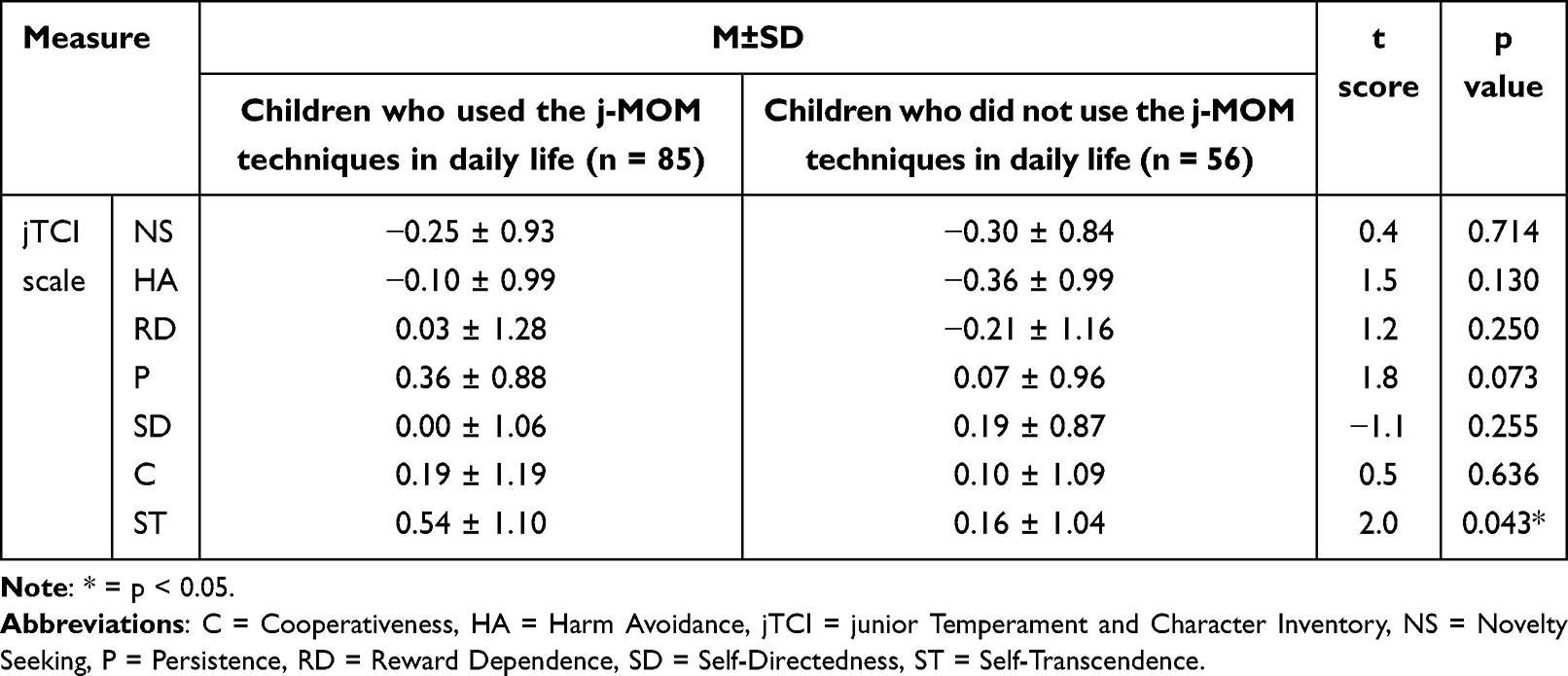 |
Table 10 Comparison of Scores in the jTCI Scales Between the Children Who Answered “Yes” (n = 85) and the Children Who Answered “No” (n = 56) in Question q6, Regarding Whether They Used, in a Moment of Difficulty, the Techniques Taught During the j-MOM Program |
Discussion
In this study, a sample of 147 primary school children was assessed as they participated in a 24-session MBP, ie the j-MOM program. In this program, formal mindfulness practices were proposed in the framework of a story of a fictional character. The children were assessed with both quantitative and qualitative tools, namely the jTCI personality questionnaire and a survey with ad hoc closed-ended and open-ended questions on programs’ acceptability. The aims of the study were to evaluate (i) how an MBP delivered through the technique of storytelling and by the school teachers could be accepted by the schoolchildren, and (ii) how the children’s evaluations of the program could be related to their personality traits.
In the first four closed-ended questions (q1, q2, q3, q4), it emerged that the j-MOM program was well accepted by the children: most of them liked it from moderately to extremely (90.5% of the participants), found it not at all or a little difficult (63.9%), found it to be moderately to extremely useful (85.7%), and engaged in it from moderately to extremely (94.5%). Comparing these acceptability data with those reported in previous researches, the j-MOM program appeared to be as much appreciated, in terms of liking (q1), as the MindUP program, the well-known MBP for children and adolescents,65 which was rated from “ok” to “liked a lot” (ie, from 2 to 4 on a 0–4 Likert scale, as in questions q1-q4 of the present study) by 88% of the 189 grade 4 to 7 students at the end of their 12-week program. In another study on an 8-week mindfulness program (Paws b), 76% of the 33 grade 2 to 4 students liked the program they followed (the remaining children disliked the program or did not mind practicing mindfulness at school).66
In terms of usefulness, the j-MOM program was seemingly more appreciated than the MindUP program assessed in the study just described,65 as 78% of the students involved in this study in 2014 answered “more than a little”, “quite a few things”, or “a lot” (ie, from 2 to 4 on a 0–4 Likert scale, as in questions from q1 to q4 of the present study) when asked how much they learned in the MindUP program. Regarding difficulty or engagement, there are no previous studies, to the best of our knowledge, that assessed these aspects in the context of MBPs for primary school children. The Acceptability score, obtained from questions q1, q2, q3, and q4, reached an average of almost 3 on the 0–4 scale, which is a much better score than the score of 4.7 on a 0–10 scale obtained in the recent large trial of Kuyken et al,28 which failed, as mentioned in the Introduction section, to show the superiority of a 10-week MBP delivered at school over a teaching-as-usual condition in promoting adolescents’ mental health. In general, program ratings in our study revealed that children had a positive experience of the j-MOM program. Together with the effectiveness of an intervention, having a positive experience of it seems to be very important for school climate, as well as for children’s possible future experience with mindfulness techniques for mental health in their adolescent or adult life.67
The survey given to the children participating in the j-MOM program also contained three open-ended questions. In the first of these (question q5), the children were asked what they learned from the j-MOM program. A thematic analysis of their responses, performed following the standard procedure of Braun and Clarke,63 highlighted five main themes (each reported by at least 13% of the children): 1) calm, relax, tranquility; 2) help for emotional, mental, and physical difficulties; 3) resilience, positiveness, personal growth; 4) self-exploration and interoception; and 5) attention, concentration, and “here and now”. All these themes regarding the children’s gains in terms of improvement of well-being, personal growth, and self-knowledge are consistent with the general aims of MBPs and have already emerged from previous qualitative research on other mindfulness programs for children65,68,69 and for adults (eg,70). Moreover, all these themes were related to the topics transmitted to the children during the j-MOM training (through the teachings of the animals to Sid, the main character of the story told to the children).
From the second open-ended question (q6) included in the survey, it emerged that more than half of the participating students (57.8%) used the techniques learned during the program in daily life, in particular during a moment of personal difficulty. Unsurprisingly, in comparison with their schoolmates who did not use the techniques in daily life, these children had a significantly higher Acceptability score (resulting from higher ratings in questions q1 and q2, regarding liking the program and finding it useful). These children revealed that when they used mindfulness techniques in daily life, they mostly employed mindfulness of breath (54.1% of the times) for managing difficult emotions (31.8% of the times). As the j-MOM program did not include the request to practice the mindfulness exercises outside the program sessions at school, this means that many children spontaneously tried to generalize the techniques to their daily lives, which is a key aspect for the effectiveness of MBPs for well-being.71 Moreover, the result on the children’s preference for using mindfulness of breath seems to be consistent with the result found for a MOM training delivered to young adult students.57 In this study, the authors found that breath mindfulness had a better impact on improving psychological correlates of emotional distress (ie, ruminative thoughts) relative to mindfulness of bodily sensations and mindfulness of thoughts. In the present study, we also found that the children who used mindfulness techniques in their daily life had higher scores in liking the program and in finding it useful than the children who did not use mindfulness outside the school sessions.
In the last open-ended question (q7) of the post-intervention survey, almost all children (93.9%) declared that they would recommend the j-MOM program to their friends and parents. Although few studies posed this question to children after completion of an MBP, this seems a remarkable result: for example, in a pilot study on 25 children in grades four to six with academic problems, only 59% of them indicated that they would have recommended the program to their friends.72 In this study, a 12-week MBP based on MBCT-C (Mindfulness-Based Cognitive Therapy for Children) was used. The high percentage of students in the current study who reported the intention to recommend the j-MOM program to their friends and parents appears to further and strongly suggest that the program was very well accepted by the children. The main reasons reported by the children for recommending the program were ascribed to the management of negative emotions, negative thoughts, stress, pain, conflict, difficulties (34.7% of the times), the promotion of calm, tranquility, relax, and well-being (29.3%), the potentiality of the program to be helpful, educative, transformative (27.2%), and the general attractiveness of the program (25.2%). The first three reasons are directly connected to the themes reported by the children in the question (q5) regarding what children learned during the j-MOM program, while the last reason is beyond usefulness and resides in the domain of enjoyment, which is an influential factor for educational achievement.73,74
The information collected with the post-intervention survey was related to children’s pre-intervention jTCI personality traits. First of all, jTCI scores were put into relation with the aspects of liking, difficulty, usefulness, and engagement, covered in the first closed-ended questions (q1, q2, q3, q4) of the post-intervention survey, as well as with the resulting Acceptability score. With this analysis, it was shown that liking the j-MOM program (question q1) was positively related to the jTCI dimensions of persistence, cooperativeness, and self-transcendence; the same jTCI dimensions of persistence and cooperativeness were positively related to children’s ratings in the aspects of usefulness and engagement (questions q3 and q4, respectively). Therefore, the children who evaluated themselves as diligent, hard-working, and perseverant (for the dimension of persistence),75 and empathic, helpful, and socially tolerant (for the dimension of cooperativeness)75 liked the program more, found it more useful, and engaged themselves more than the children with opposite characteristics of personality. In general, a higher Acceptability score was positively related to the jTCI dimensions of persistence and cooperativeness. The aspect of liking the program was also related to self-evaluations of spiritual, creative, wise, and patient characteristics of personality (ie, the dimension of self-transcendence75). In our study, children with higher scores in the self-transcendence dimension of personality also tended to use more the techniques learned during the j-MOM in daily life (in particular during moments of personal difficulty; question q6 of the post-intervention survey). Self-transcendence was therefore related to both liking the program and generalizing it to daily life.
On the other hand, when focusing on low acceptability, which emerged in our study in children with low persistence and low cooperativeness, a number of aspects need to be considered. During the initial phases of an MBP such as the j-MOM, mindfulness practices may be inherently demanding and effortful,8,76 and this may be challenging for participants with low persistence profiles. Moreover, all the activities of the program happen in a group context and this may be difficult for persons with low cooperativeness. The present study therefore gives specific indication as to which pre-intervention personal characteristics can be related to acceptability outcomes (in terms of liking the program and finding it useful and engaging). This information seems very interesting as this kind of research on MBPs is indeed still in its infancy even for adult samples,77–79 in particular regarding personality.80
Limitations
Some limitations can be acknowledged in the present study. The first limitation pertains to the fact that the described results on children’s acceptability of the j-MOM program could not be complemented and associated with a pre-post assessment of the psychological impact of the program: this should be carried out in future studies in order to test whether the excellent acceptability shown by this program effectively reverberates on the promotion of children’s well-being. The second limitation is the absence of a control group, by means of which the high satisfaction expressed by the children for the overall program could be better linked with one or both of the two main components of the j-MOM program, namely the mindfulness practices or the storytelling activity. The third limitation is the different duration of the j-MOM programs delivered by the various teachers engaged in the study, as this can influence the tiredness and motivation of the children, their understanding of the program itself, and the overall results of the study: further studies, conducted during times free from pandemic restrictions, should focus on the same program conducted in a fixed number of weeks. The last limitation concerns the lack of detailed information about teachers delivering the MBP, for instance regarding their teaching experience, professional trainings, and exact amount of mindfulness practice before and during the MBP: various studies have indeed underlined the role of the MBP instructor for obtaining significant outcomes on mental health with pupils,81 or linked the teacher’s practice of mindfulness to such outcomes.14 Future studies can therefore consider these aspects in relation to children’s acceptability of MBPs.
Conclusion
This study showed that the j-MOM program, in which formal mindfulness practices were proposed to primary school children through the technique of storytelling by their teachers, was generally well accepted by the children, who reported personal gains in various areas related to psychological well-being and self-regulation skills (calm, help for emotional/mental/physical difficulties, resilience, interoception, attention). Most of the children generalized the use of the mindfulness techniques in their daily life, mainly for managing negative emotions, physical pain or moments of general difficulty, and mindfulness of breath was the technique most employed in these circumstances. Almost all the participating children also declared that they had suggested or would suggest the j-MOM program to their friends/parents. The study also suggests which children’s personality traits should be considered when proposing a mindfulness-based program in order to improve its acceptability and perceived utility: in particular, the temperamental trait of persistence and the character trait of cooperativeness were positively related with acceptability of the j-MOM program. Moreover, the character trait of self-transcendence was related to both liking the j-MOM program and generalizing it to daily life.
Data Sharing Statement
The data supporting the conclusions of this article will be made available by the corresponding author upon request.
Funding
This research was funded by the Prevention Department of Regione Autonoma Friuli-Venezia Giulia (Italy) in collaboration with the local Public Healthcare System (ASUFC).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bodhi B. What does mindfulness really mean? A canonical perspective. Contemp Buddhism. 2011;12(1):19–39. doi:10.1080/14639947.2011.564813
2. Shapiro SL, Carlson LE, Astin JA, Freedman B. Mechanisms of mindfulness. J Clinic Psychol. 2006;62(3):373–386. doi:10.1002/jclp.20237
3. Bishop SR, Lau M, Shapiro S, et al. Mindfulness: a proposed operational definition. Clin Psychol Sci Pract. 2004;11(3):230.
4. Gibson J. Mindfulness, interoception, and the body: a contemporary perspective. Front Psychol. 2012;10:475917.
5. Hofmann SG, Sawyer AT, Witt AA, Oh D. The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. J Consult Clinic Psychol. 2010;78(2):169. doi:10.1037/a0018555
6. Goyal M, Singh S, Sibinga EM, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(3):357–368. doi:10.1001/jamainternmed.2013.13018
7. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness-based stress reduction for healthy individuals: a meta-analysis. J Psychosomatic Res. 2015;78(6):519–528. doi:10.1016/j.jpsychores.2015.03.009
8. Tang YY, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015;16(4):213–225. doi:10.1038/nrn3916
9. Pernet CR, Belov N, Delorme A, Zammit A. Mindfulness related changes in grey matter: a systematic review and meta‐analysis. Brain Imaging Behav. 2021;15:2720–2730. doi:10.1007/s11682-021-00453-4
10. Greenberg MT, Harris AR. Nurturing mindfulness in children and youth: current state of research. Child Develop Perspec. 2012;6(2):161–166. doi:10.1111/j.1750-8606.2011.00215.x
11. Roeser RW, Greenberg MT, Frazier T, Galla BM, Semenov AD, Warren MT. Beyond all splits: envisioning the next generation of science on mindfulness and compassion in schools for students. Mindfulness. 2023;14(2):239–254. doi:10.1007/s12671-022-02017-z
12. Maynard BR, Solis MR, Miller VL, Brendel KE. Mindfulness‐based interventions for improving cognition, academic achievement, behavior, and socioemotional functioning of primary and secondary school students. Campbell Syst Rev. 2017;13(1):1–144. doi:10.1002/CL2.177
13. Klingbeil DA, Renshaw TL, Willenbrink JB, et al. Mindfulness-based interventions with youth: a comprehensive meta-analysis of group-design studies. J School Psychol. 2017;63:77–103. doi:10.1016/j.jsp.2017.03.006
14. Carsley D, Khoury B, Heath NL. Effectiveness of mindfulness interventions for mental health in schools: a comprehensive meta-analysis. Mindfulness. 2018;9:693–707. doi:10.1007/s12671-017-0839-2
15. Dunning D, Tudor K, Radley L, et al. Do mindfulness-based programmes improve the cognitive skills, behaviour and mental health of children and adolescents? An updated meta-analysis of randomised controlled trials. BMJ Ment Health. 2022;25(3):135–142.
16. Roeser RW, Galla BM, Baelen RN. Mindfulness in the Schools: Evidence on the Impacts of School-Based Mindfulness Programs on Student Outcomes in P–12 Educational Settings. PA: Policy Brief for Robert Wood Johnson Foundation. University ParkEdna Bennett Pierce Prevention Research Center, The Pennsylvania State University.; 2022.
17. Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends in Cognitive Sciences. 2008;12(4):163–169. doi:10.1016/j.tics.2008.01.005
18. Malinowski P. Neural mechanisms of attentional control in mindfulness meditation. Front Neurosci. 2013;7:8. doi:10.3389/fnins.2013.00008
19. Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):1–13. doi:10.1186/s12913-017-2031-8
20. Martinez-Conde S, Alexander RG, Blum D, et al. The storytelling brain: how neuroscience stories help bridge the gap between research and society. J Neurosci. 2019;39(42):8285–8290. doi:10.1523/JNEUROSCI.1180-19.2019
21. Haigh C, Hardy P. Tell me a story—a conceptual exploration of storytelling in healthcare education. Nurse Education Today. 2011;31(4):408–411. doi:10.1016/j.nedt.2010.08.001
22. Lucarevschi CR. The role of storytelling on language learning: a literature review. Work Pap Linguistics Circ. 2016;26(1):24–44.
23. Remein CD, Childs E, Pasco JC, et al. Content and outcomes of narrative medicine programmes: a systematic review of the literature through 2019. BMJ open. 2020;10(1):e031568. doi:10.1136/bmjopen-2019-031568
24. Pulimeno M, Piscitelli P, Colazzo S. Children’s literature to promote students’ global development and wellbeing. Health Promo Perspect. 2020;10(1):13. doi:10.15171/hpp.2020.05
25. Burrows L. Transforming ‘The Red Beast’within through mindfulness and therapeutic storytelling: a Case Study. J Psychol Counsel Schools. 2013;23(2):172–184.
26. Delgado JJV. Storytelling mindfulness: Storytelling Program for meditations. In: Peña-Acuña B, editor. Narrative Transmedia. Rijeka, HR: IntechOpen; 2019.
27. McDonald D. Investigating intentionality and mindfulness of storytelling as pedagogy. In: Bohan CH, editor. Curriculum & Teaching Dialogue. Charlotte, NC: Information Age Publishing; 2019:97–110.
28. Kuyken W, Ball S, Crane C, Ganguli P, Jones B, Montero-Marin J; MYRIAD Team. Effectiveness and cost-effectiveness of universal school-based mindfulness training compared with normal school provision in reducing risk of mental health problems and promoting well-being in adolescence: the MYRIAD cluster randomised controlled trial. BMJ Ment Health. 2022;25(3):99–109.
29. Rothbart MK, Ahadi SA, Hershey KL. Temperament and social behavior in childhood. Merrill-Palmer Quarterly. 1982;21–39.
30. Rindermann H, Neubauer AC. The influence of personality on three aspects of cognitive performance: Processing speed, intelligence and school performance. Pers Individ Dif. 2001;30(5):829–842. doi:10.1016/S0191-8869(00)00076-3
31. De Bruijn GJ, Kremers SP, Van Mechelen W, Brug J. Is personality related to fruit and vegetable intake and physical activity in adolescents? Health Educ Res. 2005;20(6):635–644. doi:10.1093/her/cyh025
32. Muris P, Meesters C, Blijlevens P. Self-reported reactive and regulative temperament in early adolescence: Relations to internalizing and externalizing problem behavior and “big three” personality factors. J Adoles. 2007;30(6):1035–1049. doi:10.1016/j.adolescence.2007.03.003
33. Hiramura H, Uji M, Shikai N, Chen Z, Matsuoka N, Kitamura T. Understanding externalizing behavior from children’s personality and parenting characteristics. Psychiatry Res. 2010;175(1–2):142–147. doi:10.1016/j.psychres.2005.07.041
34. Poropat AE. A meta‐analysis of adult‐rated child personality and academic performance in primary education. British J Educ Psychol. 2014;84(2):239–252. doi:10.1111/bjep.12019
35. Weber M, Huebner ES. Early adolescents’ personality and life satisfaction: a closer look at global vs. domain-specific satisfaction. Pers Individ Dif. 2015;83:31–36. doi:10.1016/j.paid.2015.03.042
36. Cuijpers P. Universal prevention of depression at schools: dead end or challenging crossroad? BMJ Ment Health. 2022;25(3):96–98.
37. Wilkinson E. Mindfulness training in schools does not improve children’s mental health. BMJ. 2022;378(1819).
38. Montero-Marin J, Allwood M, Ball S, Crane C, De Wilde K, Hinze V; MYRIAD Team. School-based mindfulness training in early adolescence: what works, for whom and how in the MYRIAD trial? BMJ Ment Health. 2022;25(3):117–124.
39. Farias M. DEBATE: the inevitable decline of mindfulness. Child Adoles Mental Health. 2022;27(4):422–423. doi:10.1111/camh.12600
40. Schonert-Reichl KA. Encouraging advances in the science on mindfulness and compassion in schools: current research, lingering questions, and future directions. Mindfulness. 2023;14(2):300–306. doi:10.1007/s12671-023-02070-2
41. Weare K. Where have we been and where are we going with mindfulness in schools? Mindfulness. 2023;1–7.
42. Matiz A, Fabbro F, Paschetto A, Cantone D, Paolone AR, Crescentini C. Positive impact of mindfulness meditation on mental health of female teachers during the COVID-19 outbreak in Italy. Int J Environ Res Public Health. 2020;17(18):6450. doi:10.3390/ijerph17186450
43. Matiz A, Fabbro F, Paschetto A, et al. The impact of the COVID-19 pandemic on affect, fear, and personality of primary school children measured during the second wave of infections in 2020. Front Psychiatry. 2022;12:2558. doi:10.3389/fpsyt.2021.803270
44. Urgesi C, Romanò M, Fornasari L, Brambilla P, Fabbro F. Investigating the development of temperament and character in school-aged children using a self-report measure. Comprehensive Psychiatry. 2012;53(6):875–883. doi:10.1016/j.comppsych.2012.01.006
45. Luby JL, Svrakic DM, McCallum K, Przybeck TR, Cloninger CR. The junior temperament and character inventory: Preliminary validation of a child self-report measure. Psychol Rep. 1999;84:1127–1138. doi:10.2466/pr0.1999.84.3c.1127
46. Cloninger CR. Temperament and personality. Curr Opin Neurobiol. 1994;4(2):266–273. doi:10.1016/0959-4388(94)90083-3
47. Fabbro F, Muratori F. La mindfulness: un nuovo approccio psicoterapeutico in età evolutiva (mindfulness: a new psychotherapeutic approach in developmental age). Giornale di Neuropsichiatria dell’Età Evolutiva. 2012;32:248–259.
48. Fabbro F, Crescentini C. La meditazione orientata alla mindfulness (MOM) nella ricerca psicologica (mindfulness-oriented meditation in psychological research). Ricerche di Psicologia. 2016;4:457–472.
49. Campanella F, Crescentini C, Urgesi C, Fabbro F. Mindfulness-oriented meditation improves self-related character scales in healthy individuals. Comprehensive Psychiatry. 2014;55(5):1269–1278. doi:10.1016/j.comppsych.2014.03.009
50. Crescentini C, Urgesi C, Campanella F, Eleopra R, Fabbro F. Effects of an 8-week meditation program on the implicit and explicit attitudes toward religious/spiritual self-representations. Conscious Cognition. 2014;30:266–280. doi:10.1016/j.concog.2014.09.013
51. Crescentini C, Chittaro L, Capurso V, Sioni R, Fabbro F. Psychological and physiological responses to stressful situations in immersive virtual reality: differences between users who practice mindfulness meditation and controls. Comp Human Behav. 2016;59:304–316. doi:10.1016/j.chb.2016.02.031
52. Tomasino B, Fabbro F. Increases in the right dorsolateral prefrontal cortex and decreases the rostral prefrontal cortex activation after-8 weeks of focused attention based mindfulness meditation. Brain Cognition. 2016;102:46–54. doi:10.1016/j.bandc.2015.12.004
53. Tomasino B, Campanella F, Fabbro F. Medial orbital gyrus modulation during spatial perspective changes: pre-vs. post-8 weeks mindfulness meditation. Consciousness and Cognition. 2016;40:147–158. doi:10.1016/j.concog.2016.01.006
54. Matiz A, Fabbro F, Crescentini C. Single vs. group mindfulness meditation: Effects on personality, religiousness/spirituality, and mindfulness skills. Mindfulness. 2018;9:1236–1244. doi:10.1007/s12671-017-0865-0
55. Matiz A, Crescentini C, Fabbro A, Budai R, Bergamasco M, Fabbro F. Spontaneous eye movements during focused-attention mindfulness meditation. PLoS One. 2019;14(1):e0210862. doi:10.1371/journal.pone.0210862
56. Matiz A, Crescentini C, Bergamasco M, Budai R, Fabbro F. Inter-brain co-activations during mindfulness meditation. Implications for devotional and clinical settings. Conscious Cognition. 2021;95:103210. doi:10.1016/j.concog.2021.103210
57. Feruglio S, Matiz A, Grecucci A, Pascut S, Fabbro F, Crescentini C. Differential effects of mindfulness meditation conditions on repetitive negative thinking and subjective time perspective: a randomized active-controlled study. Psychol Health. 2021;36(11):1275–1298. doi:10.1080/08870446.2020.1836178
58. Crescentini C, Matiz A, Fabbro F. Improving personality/character traits in individuals with alcohol dependence: the influence of mindfulness-oriented meditation. Journal of Addictive Diseases. 2015;34(1):75–87. doi:10.1080/10550887.2014.991657
59. Crescentini C, Matiz A, Cimenti M, Pascoli E, Eleopra R, Fabbro F. Effect of mindfulness meditation on personality and psychological well-being in patients with multiple sclerosis. Int j MS Care. 2018;20(3):101–108. doi:10.7224/1537-2073.2016-093
60. Crescentini C, Capurso V, Furlan S, Fabbro F. Mindfulness-oriented meditation for primary school children: Effects on attention and psychological well-being. Frontiers in Psychology. 2016;7:805. doi:10.3389/fpsyg.2016.00805
61. Santonastaso O, Zaccari V, Crescentini C, et al. Clinical application of mindfulness-oriented meditation: a preliminary study in children with ADHD. Int J Environ Res Public Health. 2020;17(18):6916. doi:10.3390/ijerph17186916
62. Matiz A, Paschetto A. Sid e le Otto Sfere Di Luce. Come Insegnare la Meditazione Mindfulness Ai Bambini. [Sid and the Eight Spheres of Light. How to Teach Mindfulness Meditation to Children]. (Italy): Mimesis, Milano-Udine; 2022.
63. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
64. Braun V, Clarke V. Thematic analysis. In: Cooper H, Camic PM, L. Long D, T. Panter A, Rindskopf D, Sher KJ, editors. APA Handbook of Research Methods in Psychology: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological. Washington, DC: American Psychological Association; 2012:57–71.
65. Maloney JE, Lawlor MS, Schonert-Reichl KA, Whitehead J. A mindfulness-based social and emotional learning curriculum for school-aged children: the MindUP program. In: Schonert-Reichl KA, Roeser RW, editors. Handbook of Mindfulness in Education: Integrating Theory and Research into Practice. Cham: Springer; 2016:313–334.
66. Vickery CE, Dorjee D. Mindfulness training in primary schools decreases negative affect and increases meta-cognition in children. Frontiers in Psychology. 2016;6. doi:10.3389/fpsyg.2015.02025
67. Crandall A, Miller JR, Cheung A, et al. ACEs and counter-ACEs: How positive and negative childhood experiences influence adult health. Child Abuse Negl. 2019;96:104089. doi:10.1016/j.chiabu.2019.104089
68. Ager K, Albrecht N, Cohen M. Mindfulness in schools research project: Exploring students’ perspectives of mindfulness-what are students’ perspectives of learning mindfulness practices at school? Psychology. 2015;6(7):896–914. doi:10.4236/psych.2015.67088
69. Sapthiang S, Van Gordon W, Shonin E. Health school-based mindfulness interventions for improving mental health: a systematic review and thematic synthesis of qualitative studies. J Child Fam Stud. 2019;28:2650–2658. doi:10.1007/s10826-019-01482-w
70. Shapiro DH. A preliminary study of long term meditators: Goals, effects, religious orientation, cognitions. J Transpersonal Psychol. 1992;24(1):23–39.
71. Tart CT. Extending mindfulness to everyday life. J Humanistic Psychol. 1990;30(1):81–106. doi:10.1177/0022167890301005
72. Lee J, Semple RJ, Rosa D, Miller L. Mindfulness-based cognitive therapy for children: results of a pilot study. J Cognit Psychotherap. 2008;22(1):15. doi:10.1891/0889.8391.22.1.15
73. Diamond A, Ling DS. Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Develop Cognitive Neuroscience. 2016;18:34–48. doi:10.1016/j.dcn.2015.11.005
74. Morris TT, Dorling D, Davies NM, Davey Smith G. Associations between school enjoyment at age 6 and later educational achievement: evidence from a UK cohort study. Npj Science of Learn. 2021;6(1):18. doi:10.1038/s41539-021-00092-w
75. Garcia D, Lester N, Cloninger KM, Robert Cloninger C. Temperament and character inventory (TCI). In: Encyclopedia of Personality and Individual Differences. Cham: Springer International Publishing; 2020:5408–5410.
76. Malinowski P. Mindfulness as psychological dimension: Concepts and applications. The Irish J Psychol. 2008;29(1–2):155–166. doi:10.1080/03033910.2008.10446281
77. Shapiro SL, Brown KW, Thoresen C, Plante TG. The moderation of mindfulness‐based stress reduction effects by trait mindfulness: results from a randomized controlled trial. J Clinic Psychology. 2011;67(3):267–277. doi:10.1002/jclp.20761
78. Elwafi HM, Witkiewitz K, Mallik S, Thornhill TA IV, Brewer JA. Mindfulness training for smoking cessation: Moderation of the relationship between craving and cigarette use. Drug Alcohol Depend. 2013;130(1–3):222–229. doi:10.1016/j.drugalcdep.2012.11.015
79. Kuyken W, Warren FC, Taylor RS, et al. Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: an individual patient data meta-analysis from randomized trials. JAMA psychiatry. 2016;73(6):565–574. doi:10.1001/jamapsychiatry.2016.0076
80. de Vibe M, Solhaug I, Tyssen R, et al. Does personality moderate the effects of mindfulness training for medical and psychology students? Mindfulness. 2015;6:281–289. doi:10.1007/s12671-013-0258-y
81. Roeser RW, Schonert-Reichl KA, Jha A, et al. Mindfulness training and reductions in teacher stress and burnout: results from two randomized, waitlist-control field trials. J Educ Psychol. 2013;105(3):787. doi:10.1037/a0032093
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.