")
Back to Journals » Integrated Blood Pressure Control » Volume 15
Medication Adherence and Blood Pressure Control Among Hypertensive Outpatients Attending a Tertiary Cardiovascular Hospital in Tanzania: A Cross-Sectional Study
Authors Pallangyo P , Komba M, Mkojera ZS, Kisenge PR, Bhalia S, Mayala H, Kifai E, Richard MK, Khanbhai K , Wibonela S, Millinga J, Yeyeye R, Njau NF, Odemary TK, Janabi M
Received 23 May 2022
Accepted for publication 8 July 2022
Published 10 August 2022 Volume 2022:15 Pages 97—112
DOI https://doi.org/10.2147/IBPC.S374674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Turgay Celik
Pedro Pallangyo,1,2 Makrina Komba,1 Zabella S Mkojera,1 Peter R Kisenge,1,2 Smita Bhalia,2 Henry Mayala,3 Engerasiya Kifai,3 Mwinyipembe K Richard,2 Khuzeima Khanbhai,1,2 Salma Wibonela,4 Jalack Millinga,4 Robert Yeyeye,4 Nelson F Njau,3 Thadei K Odemary,3 Mohamed Janabi2
1Unit of Research and Training, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania; 2Directorate of Cardiology, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania; 3Directorate of Clinical Support Services, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania; 4Directorate of Nursing, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania
Correspondence: Pedro Pallangyo, Unit of Research and Training, Jakaya Kikwete Cardiac Institute, Dar es Salaam, Tanzania, Email [email protected]
Background: Notwithstanding the availability of effective treatments, asymptomatic nature and the interminable treatment length, adherence to medication remains a substantial challenge among patients with hypertension. Suboptimal adherence to BP-lowering agents is a growing global concern that is associated with the substantial worsening of disease, increased service utilization and health-care cost escalation. This study aimed to explore medication adherence and its associated factors among hypertension outpatients attending a tertiary-level cardiovascular hospital in Tanzania.
Methods: The pill count adherence ratio (PCAR) was used to compute adherence rate. In descriptive analyses, adherence was dichotomized and consumption of less than 80% of the prescribed medications was used to denote poor adherence. Logistic regression analyses was used to determine factors associated with adherence.
Results: A total of 849 outpatients taking antihypertensive drugs for ≥ 1 month prior to recruitment were randomly enrolled in this study. The mean age was 59.9 years and about two-thirds were females. Overall, a total of 653 (76.9%) participants had good adherence and 367 (43.2%) had their blood pressure controlled. Multivariate logistic regression analysis showed; lack of a health insurance (OR 0.5, 95% CI 0.3– 0.7, p< 0.01), last BP measurement > 1 week (OR 0.6, 95% CI 0.4– 0.8, p< 0.01), last clinic attendance > 1 month (OR 0.4, 95% CI 0.3– 0.6, p< 0.001), frequent unavailability of drugs (OR 0.6, 95% CI 0.3– 0.9, p = 0.03), running out of medication before the next appointment (OR 0.6, 95% CI 0.4– 0.9, p = 0.01) and stopping medications when asymptomatic (OR 0.6, 95% CI 0.4– 0.8, p< 0.001) to be independent associated factors for poor adherence.
Conclusion: A substantial proportion of hypertensive outpatients in this tertiary-level setting had good medication adherence. Nonetheless, observed suboptimal blood pressure control regardless of a fairly satisfactory adherence rate suggests that lifestyle modification plays a central role in hypertension management.
Keywords: medication adherence, nonadherence, drug adherence, hypertension, blood pressure control
Background
Hypertension, which affects over a quarter of the global population, is currently the leading cause of non-communicable diseases (NCDs) and the main contributor to disability adjusted life years (DALYs) worldwide.1,2 In a span of just 3 decades, the World Health Organization (WHO) African region has witnessed a dramatic upsurge of hypertension prevalence from 9.7% in 1990 to 46% in 2020, making it the most affected WHO region.2–7 While the last national representative survey conducted in Tanzania found that 26% of the adult population were hypertensive, a rate of nearly 50% reported by a more recent population-based study conducted in the island of Mafia potentially imply a significantly higher burden of hypertension in this East African nation.8,9 So to prevent hypertension-related complications and deaths, optimal control of blood pressure (BP) is paramount.10–13 Nonetheless, with just 7% of the hypertensive population having controlled BPs in sub=Saharan Africa (SSA), Africans have the worst hypertension control rates and superior hypertension-related complications compared to their Caucasian counterparts.7,14
Notwithstanding the availability of effective treatments, asymptomatic nature and the interminable treatment length, adherence to medication remains a substantial challenge among patients with hypertension. Moreover, in spite of numerous advances made in adherence research (ie identification of nonadherence determinants and exploration of impact of interventions to improve adherence), rates of suboptimal adherence have remained more or less the same over the years.15,16 According to the WHO, over a half of persons with hypertension discontinue their antihypertensives entirely within the first year of diagnosis and at most a half of those staying on medications consume ≥80% of their prescribed regimens.17 As a consequence approximately three-quarters of patients do not attain optimum BP control thus making poor adherence a prominent cause of uncontrolled hypertension globally.18 Furthermore, apart from it being the noticeable cause of apparent resistant hypertension, nonadherence is accountable for the substantial worsening of disease, increased service utilization and health-care cost escalation.19–24 Considering the rapidly growing burden of hypertension in Tanzania, this study aimed to explore medication adherence and its associated factors among hypertension outpatients attending a tertiary-level cardiovascular hospital in Tanzania.
Methodology
Study Design, Recruitment Process, and Definition of Terms
Between April 2021 and October 2021 a hospital-based cross-sectional study was conducted at a tertiary care public teaching hospital (ie Jakaya Kikwete Cardiac Institute [JKCI]) in Dar es Salaam, Tanzania. A simple random sampling method was utilized to recruit consented hypertensive outpatients during their scheduled clinic visit. A structured questionnaire bearing variables pertaining to a study’s objective was utilized in this study. Prior to its use in this study, the data collection tool was subjected to evaluation and validation. Informed consent was sought from every participant prior to enrolment. Patients aged ≥18 years on antihypertensive medications for ≥30 days prior to recruitment were eligible for participation in this present study.
Prior to commencement of the study, a list of hypertensive patients with their respective clinic appointments for the entire study duration was obtained from the medical records department. Data on the previously prescribed antihypertensive medications was fetched from the hospital management information system (HMIS). A day prior to their scheduled clinic visit, potential participants were phoned and asked to come with their medication bottles/boxes. Utilizing a pill-count form, number of remaining antihypertensive pills in the bottle/box was recorded upon recruitment. The pill count adherence ratio (PCAR) (ie (pills consumed divide by pills prescribed during the last visit) × 100) was used to compute adherence rate. In descriptive analyses, adherence was dichotomized and consumption of less than 80% of the prescribed medications was used to denote poor adherence.25,26 This cut off (ie ≥80% consumption) has been shown to achieve BP control and correlate well with cause-specific hospitalization in hypertensive patients.27–29 Furthermore, following an extensive literature search coupled with its overarching objectives, this study assessed a total of 13 potential barriers to adherence including; cost, side effects, forgetfulness, negligence, unavailability of drugs, pill burden, treatment fatigue, disease fatigue, “healed through prayers” belief, “medications not helpful” belief, unawareness of treatment length, running out of medications, and stopping medications when asymptomatic.
Physical Activity Vital Sign (PAVS)30 questionnaire was employed in the assessment of physical activity. Reported moderate-vigorous physical activity of 0 min/week, <150 min/week, or ≥150 min/week was used to classify participants as inactive, underactive or active respectively. Body mass index (BMI) cut-off values of <18.5 kg/m2, 18.5–24.9 kg/m2, 25.0–29.9 kg/m2, ≥30.0 kg/m2 was used to categorize individuals as underweight, normal weight, overweight or obese.31 Regarding smoking, participants with a negative history of smoking were regarded as never-smokers while use of cigarettes within the last 6 months or self-reported quitting smoking was used to denote current smokers and ex-smokers respectively. Consumption every week of an alcoholic beverage was used to define a drinker. Awareness of risk factors for hypertension was assessed using an open ended question. Participants were prompted to mention as many risk factors as they know and the correct responses were marked against the predesigned checklist in the questionnaire.
Two BP readings (roughly 2 minutes apart) were taken using an OMRON HEM-7156 digital automated sphygmomanometer and systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg was used to indicate uncontrolled BP.32,33 A fasting blood glucose (FBG) ≥7 mmol/L, glycated hemoglobin (HbA1c) of ≥6.5% or use of glucose-lowering agents was used to define diabetes while a one touch select plus glucometer was utilized in blood glucose concentration measurements.34 A 2-dimensional echocardiography (ECHO) was utilized for cardiac assessment with an ejection fraction (EF) ≤40% used to signify systolic heart failure.35 The Modification of Diet in Renal Disease (MDRD) equation was utilized in the estimation of renal functions and an estimated glomerular filtration rate (eGFR) value of <60 mL/min/1.73 m2 was used to denote renal dysfunction.36 Hemoglobin (Hb) concentration of <13.0 g/dL and <12.0 g/dL for males and females respectively was used to diagnose anemia.37 Low-density lipoprotein (LDL) cut-off levels of 3.5 mmol/L was used to categorize hypercholesterolemia.38
Statistical Analysis
STATA v11.0 software was employed in all statistical analyses. Summaries of continuous variables and categorical variables are presented as means (± SD) and frequencies (percentages) respectively. Pearson Chi square and Student’s t-test techniques were used in comparison of categorical and continuous variables respectively. Logistic regression analyses was used to determine factors associated with adherence. Factors included in our logistic regression model included age, sex, education level, marital status, employment status, residence, health insurance possession status, last clinic attendance, last BP measurement, hospitalization, traditional medicine use, BP control, and potential barriers (ie cost, unavailability of drugs, treatment fatigue, healed belief, running out of drugs, and stopping medications when asymptomatic). Statistically significant variables in the multivariate regression model were assessed following a stepwise and forward inclusion method. The multivariate model was fitted with baseline covariates associated with adherence by bivariate analysis at the <0.05 significance level. Odd ratios (OR) with 95% confidence intervals and p-values are reported. All tests were 2-sided and p<0.05 was used to signify a statistical significance.
Results
Characteristics of the Study Participants
Table 1 displays the sociodemographic and clinical characteristics of the 849 enrolled study participants. The mean age was 59.9 and just over a half of all participants were aged above 60 years. Females constituted nearly two-thirds (65.7%) of participants and 60.7% had attained at most primary education. About a half (50.1%) of participants were either jobless or retired, almost two-thirds (64.8%) were living with a partner and nearly three-quarters (74.1%) had health insurance. Roughly 0.3%, were current smokers, 5.9% alcohol consumers, 74.0% were insufficiently active and 80.2% had excess body weight (ie overweight 32.0% and obese 48.2%). Regarding comorbidity history, 14.4% had a history of type 2 diabetes, 16.0% had renal dysfunction, 38.2% had hypercholesterolemia, 11.4% had heart failure, 49.6% had anemia and 11.7% had a history of stroke. With reference to awareness of risk factors for hypertension; excess salt intake was acknowledged by 38.2% of participants, excess fat intake by 67.4%, overweight by 16.8%, physical inactivity by 12.7%, smoking by 3.9%, excess alcohol intake by 10.3% and positive family history by 3.2%; Figure 1.
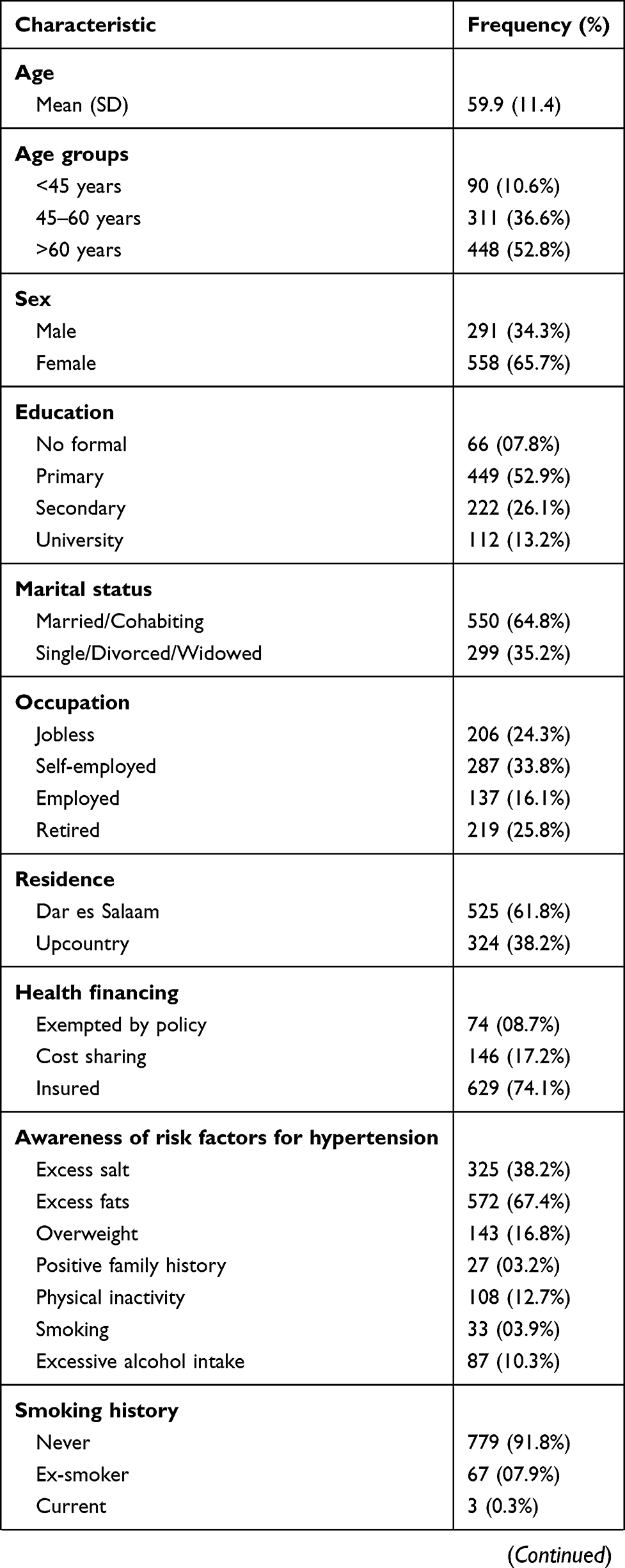 | 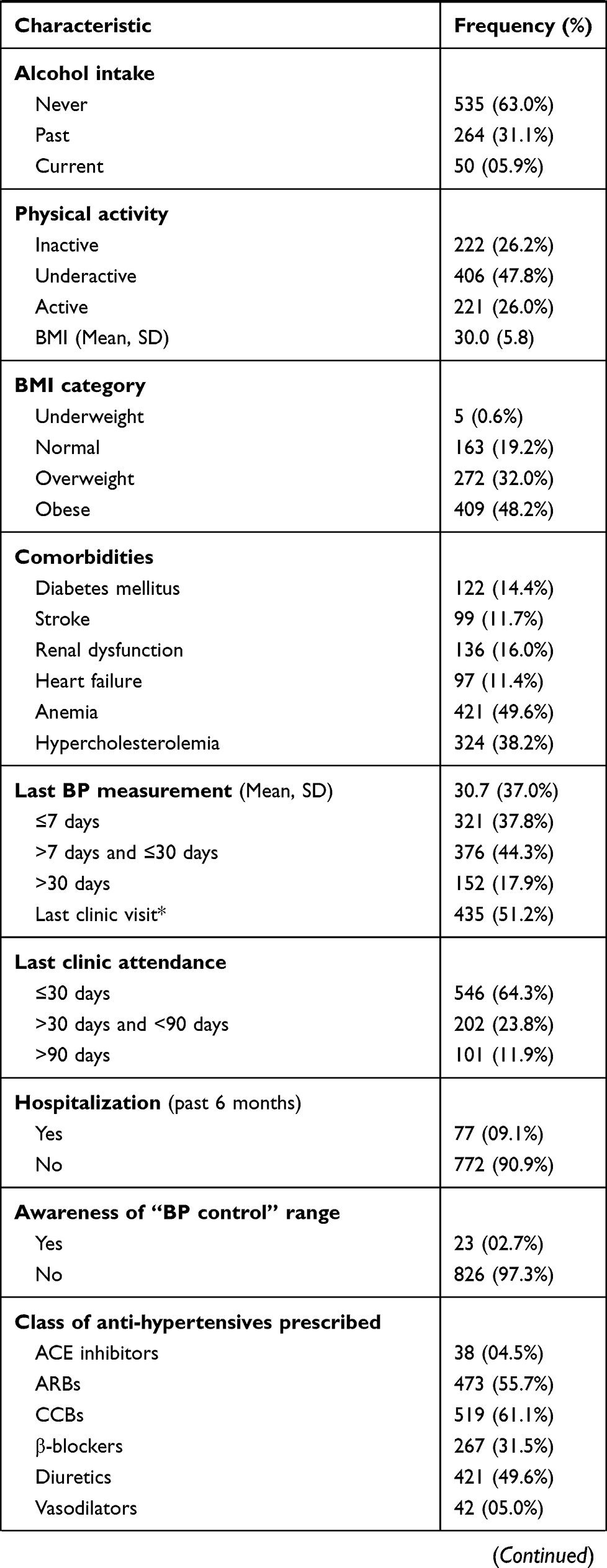 |  |
Table 1 Sociodemographic and Clinical Characteristics of Study Participants (N = 849) |
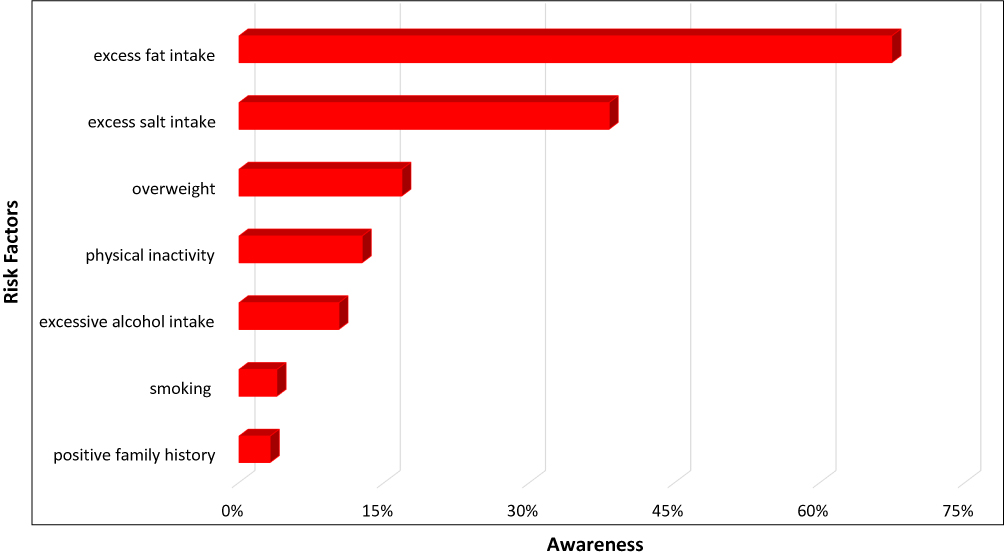 |
Figure 1 Bar graph displaying participant’s awareness of various risk factors for hypertension. |
Pattern of Antihypertensives Prescribed, Adherence and BP Control
About two-thirds of participants (64.3%) had attended a hypertension clinic within one month prior to enrolment in this present study and 2.7% could state the BP control range (ie <140/90 mmHg) correctly. Participants with a within one month outpatient visit displayed superior adherence rates compared to their counterparts whose last visit was over a month ie 83.5% vs 65.0%, p<0.001. Over a third (37.8%) of participants had measured their BPs within a week prior to their scheduled clinic visit and overall 51.2% of participants’ last BP was taken during their previous clinic visit. Participants who had measured their BPs within a week prior to recruitment displayed higher adherence rates compared to their counterparts ie 83.5% vs 72.9%, p<0.001.
Nearly 10% of participants had a hypertension-related hospitalization within 6 months of recruitment to the study. Participants with a recent history of hospitalization displayed similar adherence rates to their nonhospitalized counterparts, ie 81.8% vs 76.4%, p = 0.3. A total of 106 (12.5%) participants had ever used traditional medicine for treating hypertension and 6.4% were current users. However, there was no difference in adherence between current traditional medicine users and non-users ie 72.2% vs 77.2%, p = 0.4. Individuals with ≤primary school education displayed inferior adherence rates compared to their ≥secondary education counterparts ie 74.6% vs 80.5%, p = 0.04. Moreover, similar adherence rates were observed across age (≤60 vs >60 years) ie 76.8% vs 77.1%, p = 0.9. Likewise, males had similar adherence to females ie 75.6% vs 77.6%, p = 0.5. Nonetheless, participants with health insurance displayed superior adherence rates compared to their uninsured counterparts ie 79.3% vs 70.0%, p<0.01. Overall, a total of 653 (76.9%) participants had consumed at least 80% of their last prescribed drugs (ie good adherence).
Generally, 270 (31.8%) participants were on monotherapy, 304 (35.8%) on a double-combination regimen, 210 (24.7%) were on a triple-combination regimen and 65 (7.6%) were on more than three antihypertensive agents of different classes. Calcium channel blockers (CCBs) [61.1%] were the most prescribed class, followed by angiotensin receptor blockers (ARBs) [55.7%], diuretics [49.6%], beta-blockers (β-blocker) [31.5%], vasodilators [5.0%] and angiotensin converting enzyme (ACE) inhibitors [4.5%]. Diuretic plus ARB [91 (10.7%)] was the most frequently prescribed double-combination regimen, followed by ARB plus CCB [66 (7.8%)] and CCB plus diuretic [48 (5.7%)]. With regard to triple-combination regimens, ARB plus CCB plus diuretic [76 (9.0%)] and ARB plus β-blocker plus diuretic [65 (7.7%)] were the commonest.
A total of 367 (43.2%) participants had their BP under control. Age (>60 vs ≤60: 46.2% vs 41.9%, p = 0.2) and sex (male vs females: 41.2% vs 45.7%, p = 0.2) differences displayed similar BP control rates. Individuals with at least secondary school education displayed higher BP control rates compared to their ≤primary education counterparts ie 49.4% vs 40.8%, p = 0.01. Insured participants exhibited superior BP control rate compared to their uninsured equivalents, ie 46.9% vs 36.4%, p<0.01. Furthermore, participants with current use of traditional medicine displayed similar BP control rates compared to non-users ie 51.9% vs 43.7%, p = 0.2. Similarly, participants with good adherence had comparable BP control rates to those with poor adherence ie 45.3% vs 40.3%, p = 0.2.
Barriers to Adherence and Associated Factors
Overall, 96.3% of participants had mentioned at least one barrier to their adherence while nearly three-quarters (73.1%) reported three or more barriers. Disease fatigue (58.3%) was the most reported barrier, followed by “run out of medication before next appointment” (39.9%), forgetfulness (38.3%), “stop medications when symptom-free” (36.6%), and cost of drugs (33.2%). Other barriers included “unaware of treatment length” (29.2%), side effects (18.9%), treatment fatigue (17.7%), “medications not helpful belief” (10.3%), pill burden (9.3%), “healed through prayers belief” (8.8%), unavailability of drugs (8.1%) and negligence (6.7%); Figure 2.
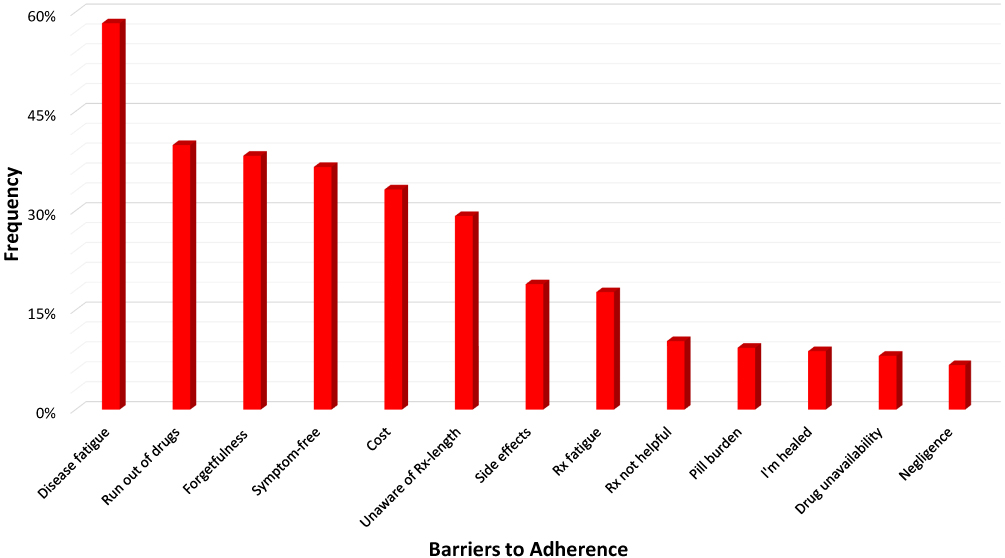 |
Figure 2 Bar graph displaying frequency and pattern of barriers towards medication adherence. |
Comparatively (Table 2); the subgroup with poor adherence displayed a significantly higher proportion of participants with the following reported barriers: cost (44.9% vs 29.7%, p<0.001), unavailability of drugs (14.3% vs 6.3%, p<0.001), medication run out (53.1% vs 36.0%, p<0.001), and stopping of drugs when symptom-free (47.4% vs 33.4%, p<0.001). On the other hand, participants with good adherence had a higher proportion of participants with treatment fatigue (19.1% vs 12.8%, p = 0.01) and those who believed they had been healed through prayers (10.3% vs 4.1%, p<0.001).
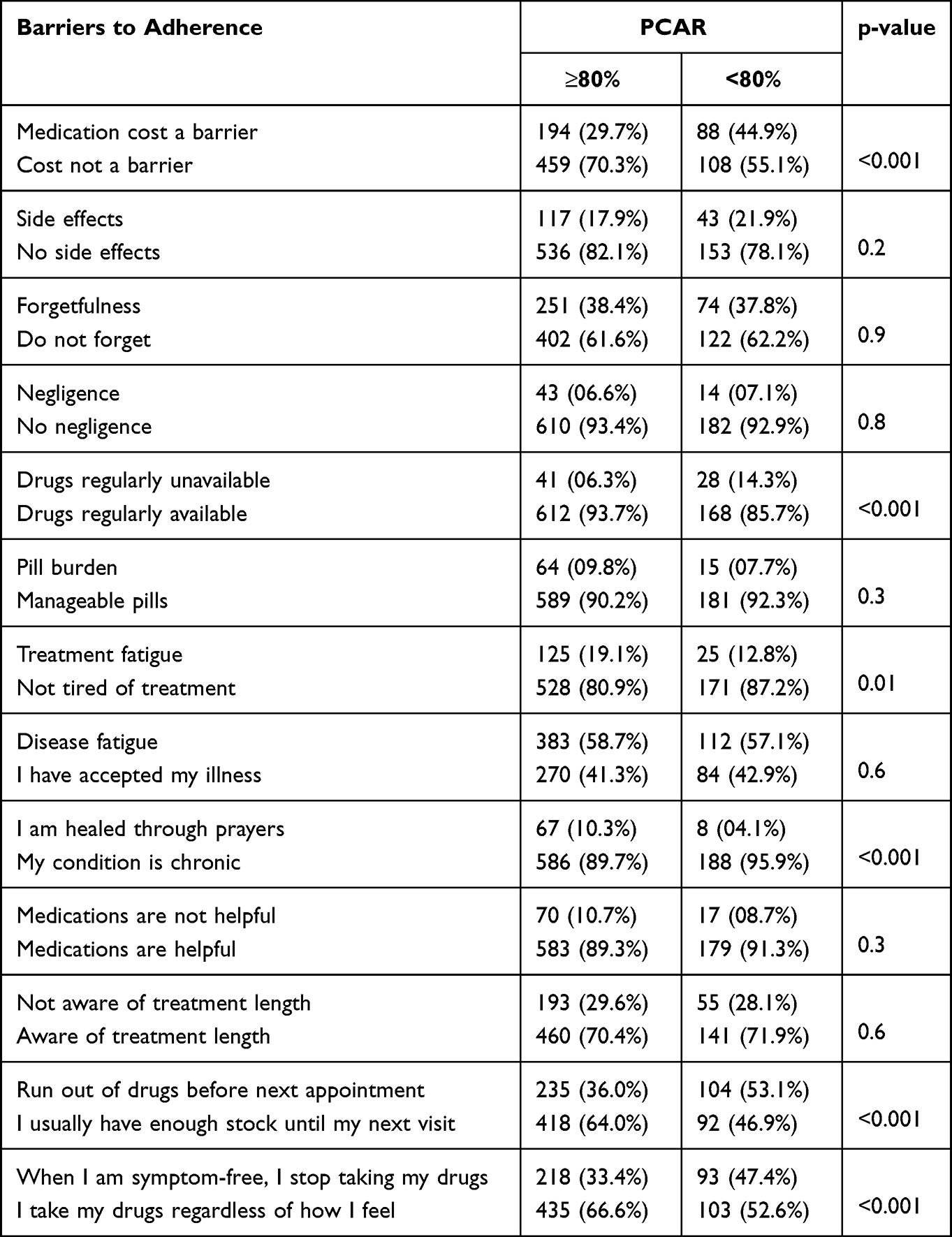 |
Table 2 Distribution of Adherence Barriers According to PCAR |
Table 3 shows results of logistic regression analysis for factors associated with adherence. During bivariate analysis in a logistic regression model consisting of eighteen characteristics, ten attributes (ie education, insurance possession, last BP measurement, last clinic attendance, cost of medications, frequent unavailability of drugs, treatment fatigue, healed belief, running out of medication before next appointment and stopping medications when asymptomatic) showed significance. However, after controlling for confounders (multivariate logistic regression), six characteristics, ie lack of a health insurance (OR 0.5, 95% CI 0.3–0.7, p<0.01), last BP measurement >1 week (OR 0.6, 95% CI 0.4–0.8, p<0.01), last clinic attendance >1 month (OR 0.4, 95% CI 0.3–0.6, p<0.001), frequent unavailability of drugs (OR 0.6, 95% CI 0.3–0.9, p = 0.03), running out of medication before next appointment (OR 0.6, 95% CI 0.4–0.9, p = 0.01) and stopping medications when asymptomatic (OR 0.6, 95% CI 0.4–0.8, p<0.001), remained independent associated factors for poor adherence.
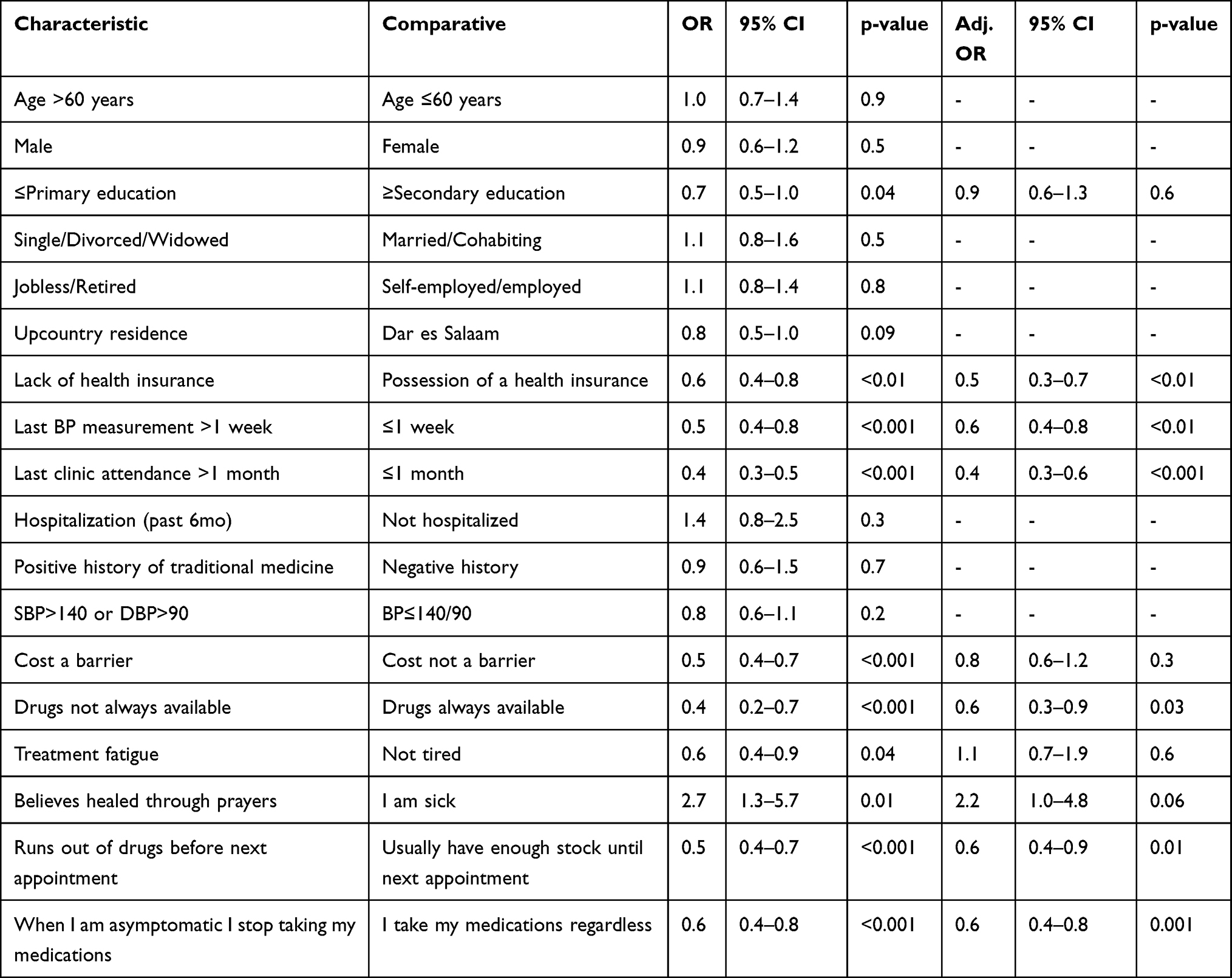 |
Table 3 Associated Factors for Adherence (Logistic Regression Analysis) |
Discussion
Despite the remarkable progress in BP measurement methods and the extensive availability of effective pharmacotherapies coupled with the proven prophylactic effects of lifestyle modification, the burden of hypertension continues to rise and its control remains a considerable challenge for health systems across the globe.39–42 Suboptimal adherence to BP-lowering agents is a growing global concern that constitutes a significant barrier to effective, economical and safe use of medications.43,44 Impressively, about three-quarters of participants in this present study were categorized as having good adherence to prescribed antihypertensive drugs. Compared with studies that utilized a similar assessment method, variable rates are reported across the literature. In unison to our findings, studies conducted in Pakistan and USA revealed adherence rates between 73.7% and 76.7%.45–47 However, a couple of studies from Ethiopia, Namibia, Saudi Arabia and Scotland revealed somewhat better adherence rates (84.0% to 87.7%).48–51 Nonetheless, numerous studies revealed lower rates (37.7–64.0%) of adherence compared to our study.52–59 Intriguingly, the rates of adherence from this study are remarkably higher than those from an earlier study conducted in the same setting that involved heart failure patients (ie 25.3% had good adherence).60 Nonetheless, we have observed an extraordinary increase in health insurance possession among patients between the two studies (ie 22.2% vs 74.1%) and we hypothesize this as the main contributor to the adherence discrepancy.60
Numerous barriers to adherence among hypertensive patients have been documented in different communities across the globe. Despite the relatively high adherence rate from this study, a large majority of participants (ie 96.3%) acknowledged facing at least one barrier to their adherence. This observation potentially suggests that the current recorded rates could go down at any time if concerted efforts to deal particularly with modifiable barriers are not made in a timely manner. Largely, the reported barriers from this present study ie disease fatigue, “stop medications when symptom-free”, “unawareness of treatment length”, treatment fatigue, “medications not helpful belief”, and “healed through prayers belief” could be mitigated by improving providers communication (including education and counseling) to patients. Moreover, some barriers ie “run out of medication before next appointment” and unavailability of drugs are health-system related and could be improved by simply refining the appointment system to run parallel with quantity of prescribed drugs as well as strengthening of the inventory management system to almost always ensure a positive stock-balance particularly of commonly prescribed antihypertensives. Additionally, cost remains a huge obstacle in most communities particularly in resource-limited settings like this one. However, in such unprivileged societies (as witnessed in this study) possession of a health insurance is a game changer. In view of this, deliberate yet collaborative efforts to increase its acquisition so as to attain a universal status will be a rewarding endeavor. Nevertheless, the barriers observed in this study have been documented at variable rates by previous research from different settings worldwide.26,47,48,50,56,59,61–70
Patients’ familiarity with their management plan is a critical success factor to favorable clinical outcomes. Furthermore, patient knowledge of BP goal has been shown to be an independent predictor of BP control.71 Unfortunately, major deficiencies in communications is characteristic of patient-provider interactions in SSA.72 Barely 3% of hypertensives in this study were aware of their target BP. Generally, unsatisfactory rates of awareness of target BP is reported in the body of literature, however, our proportion is very low compared to preceding scholarly works (18.2–68.0%).71,73–79 A quality (clear and comprehensible) and empathic physician-patient communication has been shown to aid adherence to prescribed treatments and to recommended preventive activities.80–83 For instance, the rates of nonadherence are nearly 20% higher among patients whose healthcare provider communicates poorly versus their counterparts receiving a sound communication.84 Through collaborative communication and decision making, patients are empowered to understand all essential aspects of their treatment plans which has been correlated with successful reaching of treatment goals. Moreover, as one’s understanding correlates with the level of education, it is pivotal that physicians take enough time clarifying the treatment plans and goals particularly to patients with lower levels of education which is a predominant group in the developing world.
Lifestyle measures (ie alcohol reduction, smoking cessation, salt intake reduction, increased physical activity and weight reduction) have been shown to be an effective adjuvant to pharmacotherapy in achieving BP control.85–90 Likewise, nonadherence to lifestyle modifications is associated with inadequate BP control.86,91–93 Furthermore, incorporation of lifestyle interventions to antihypertensive medications is associated with a drug step-down.94,95 Awareness of lifestyle modifiable risks for hypertension was quite low in this present study. Consequently, unhealthy lifestyle behaviors particularly physical inactivity and excess body weight were evident in about three-quarters and four-fifths of participants respectively. Compared to an earlier study in the same setting that involved caretakers of CVD patients, participants of this present study displayed inferior awareness across all risk factors ie excess salt intake 38.2% vs 85.9%, overweight 16.8% vs 90.1%, physical inactivity 12.7% vs 95.6%, smoking 3.9% vs 77.0%, excess alcohol intake 10.3% vs 90.1% and positive family history by 3.2% vs 65.6%.97 As the awareness assessment used a close-ended method in the previous study while the present study utilized an open-ended way, this might be the possible explanation towards the rate discrepancy. Nevertheless, the unsatisfactory low awareness and practices to lifestyle modification irrespective of the modest medication adherence suggests a potential over-reliance on drugs in lieu of commitment to a healthy lifestyle. These findings however echo Ethiopian, Jordanian, and Iranian studies which revealed that barely a quarter (ie 24.8%, 23.0%, and 27.8% respectively) of its participants were compliant with healthy lifestyle behaviors.57,96,97 Moreover, quite worrying rates of modifiable lifestyle risks documented by recent community and hospital-based studies from Tanzania calls for a resilient multisectoral approach and urgent evaluation of policies implemented to combat hypertension and other NCDs.95,98–103
Improved and sustained BP control is pivotal in reduction of CVD morbidity and mortality. Regardless of the modest adherence rates witnessed in this study, less than a half of participants had achieved BP control. Ranging between 9.4% and 49.9%, a similar pattern (ie less than a half of participants having controlled BPs) is observed from the majority of studies in the body of literature irrespective of the geographical location.46,76,104–125 However, relatively fewer studies have reported a slightly higher proportion (51.7–63.0%) of participants with desirable BP range.26,79,126–128 Globally, BP control remains far from adequate regardless of the presence of effective medications and proven healthy lifestyle changes. Nonetheless, as hypertension control requires a multimethod approach, it is fundamental for healthcare providers to improve not only on the aforementioned communication but should also incorporate assessment of adherence to both pharmacological agents and lifestyle modification in routine clinical practice.
Strengths and Limitations
Numerous strengths can be drawn from this study including; (i) the utilization of a pill count method in assessing adherence mitigated reporting bias, (ii) assessment of various comorbidities that may influence adherence and BP control including chronic kidney disease, heart failure, and diabetes mellitus, (iii) as this study utilized a probability sampling method (ie simple random sampling), this mitigated bias as well as increasing the likelihood of our findings to be generalizable to hypertensive patients attending tertiary care level hospital in SSA and similar resource limited settings. However, we recognize some limitations including; (i) limitation of temporal association exploration due to the cross-sectional nature and (ii) as our assessment of health knowledge and self-care largely based on self-reports, we cannot rule out the possibility of response bias and/or recall bias.
Conclusion
A substantial proportion of hypertensive outpatients in this tertiary-level setting had a good adherence to prescribed antihypertensive medications. Nonetheless, observed suboptimal blood pressure control regardless of a fairly satisfactory adherence rate suggests that lifestyle modification plays a central role in hypertension management. As literally all recognized barriers for adherence in this study are modifiable, this calls for deliberate yet targeted efforts to strengthen the communication of healthcare providers with patients. Furthermore, considering the high prevalence of modifiable lifestyle risk factors (particularly overweight and physical inactivity) and the low awareness of such, it is pivotal for the routine clinical practice and health promotion programs to address lifestyle modification. Lastly, irrespective of the satisfactory adherence rate observed in this study, nonadherence continues to be a significant obstacle in hypertension management thus regular assessment of adherence to medication is fundamental.
Abbreviations
95% CI, 95% Confidence Interval; β-blocker, beta-blocker; ACE inhibitor, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BP, blood pressure; CCB, calcium channel blocker; CVD, cardiovascular disease; DALYs, disability-adjusted life years; DBP, diastolic blood pressure; ECHO, echocardiography; EF, ejection fraction; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; Hb, hemoglobin; HbA1c, glycated hemoglobin; HMIS, health management information system; JKCI, Jakaya Kikwete Cardiac Institute; LDL, low-density lipoprotein; MDRD, Modification of Diet in Renal Disease; NCDs, non-communicable diseases; OR, odds ratio; PAVS, physical activity vital sign; PCAR, pill count adherence ratio; SSA, sub-Saharan Africa; SBP, systolic blood pressure; SD, standard deviation; USA, United States of America; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Participants gave written informed consent to participate in the study. The study protocol was approved by the local ethics committees (Jakaya Kikwete Cardiac Institute) and was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We extend our appreciation to all the study participants for their willingness, tolerance and cooperation offered during this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by PedPal Research Initiative. The funder had no role in the design of this study, collection of data, data analysis, interpretation of results or writing of this manuscript.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi:10.1016/S0140-6736(12)61766-8
2. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–450. doi:10.1161/CIRCULATIONAHA.115.018912
3. WHO. A global brief on hypertension. Available from: http://www.who.int/cardiovascular_diseases/publications/global_brief_hypertension/en/.
4. Ferdinand KC. Uncontrolled hypertension in sub-Saharan Africa: now is the time to address a looming crisis. J Clin Hypertens. 2020;22(11):2111–2113. doi:10.1111/jch.14046
5. WHO. Global brief on hypertension; 2017. Available from: http://ish-world.com/downloads/pdf/global_brief_hypertension.Pdf.
6. Adeloye D, Kiechl S. An estimate of the incidence and prevalence of stroke in Africa: a systematic review and meta-analysis. PLoS One. 2014;9:e100724. doi:10.1371/journal.pone.0100724
7. Ataklte F, Erqou S, Kaptoge S, et al. Burden of undiagnosed hypertension in sub-saharan Africa: a systematic review and metaanalysis. Hypertension. 2015;65:291–298. doi:10.1161/HYPERTENSIONAHA.114.04394
8. Mayige M, Kagaruki G. Tanzania steps survey report. 2013.
9. Muhamedhussein MS, Nagri ZI, Manji KP. Prevalence, risk factors, awareness, and treatment and control of hypertension in Mafia Island, Tanzania. Int J Hypertens. 2016;2016:1281384. doi:10.1155/2016/1281384
10. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009;338:b1665. doi:10.1136/bmj.b1665
11. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913.
12. Corrao G, Parodi A, Nicotra F, et al. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011;29:610–618. doi:10.1097/HJH.0b013e328342ca97
13. Böhm M, Schumacher H, Laufs U, et al. Effects of nonpersistence with medication on outcomes in high-risk patients with cardiovascular disease. Am Heart J. 2013;166(2):306–314. doi:10.1016/j.ahj.2013.04.016
14. Akintunde AA, Akintunde TS. Antihypertensive medications adherence among Nigerian hypertensive subjects in a specialist clinic compared to a general outpatient clinic. Ann Med Health Sci Res. 2015;5:173–178. doi:10.4103/2141-9248.157492
15. Peacock E, Krousel-Wood M. Adherence to antihypertensive therapy. Med Clin North Am. 2017;101(1):229–245. doi:10.1016/j.mcna.2016.08.005
16. van Dulmen S, Sluijs E, van Dijk L, et al. Patient adherence to medical treatment: a review of reviews. BMC Health Serv Res. 2007;7:55. doi:10.1186/1472-6963-7-55
17. World Health Organization. Adherence to Long Term Therapy: Evidences for Action. Switzerland: World Health Organization; 2003:107–112.
18. Mant J, McManus RJ. Does it matter whether patients take their antihypertensive medication as prescribed? The complex relationship between adherence and blood pressure control. J Hum Hypertens. 2006;20:551–553. doi:10.1038/sj.jhh.1002046
19. Jung O, Gechter JL, Wunder C, et al. Resistant hypertension? Assessment of adherence by toxicological urine analysis. J Hypertens. 2013;31:766–774. doi:10.1097/HJH.0b013e32835e2286
20. Mazzaglia G, Ambrosioni E, Alacqua M, et al. Adherence to antihypertensive medications and cardiovascular morbidity among newly diagnosed hypertensive patients. Circulation. 2009;120:1598–1605. doi:10.1161/CIRCULATIONAHA.108.830299
21. Mensah GA. Epidemiology of stroke and high blood pressure in Africa. Heart. 2008;94:697–705. doi:10.1136/hrt.2007.127753
22. Ogden LG, He J, Lydick E, Whelton PK. Long-term absolute benefit of lowering blood pressure in hypertensive patients according to the JNC VI risk stratification. Hypertension. 2000;35:539–543. doi:10.1161/01.HYP.35.2.539
23. Osterberg L, Blaschke T. Drug therapy: adherence to medication. N Engl J Med. 2005;353:487–497. doi:10.1056/NEJMra050100
24. The benefits of responsible use of medicines - Setting policies for better and cost-effective healthcare. Ministers Summit3October 2012, Amsterdam, The Netherlands; 2012. Available from: http://www.imshealth.com/en/thoughtleadership/ims-institute/reports/responsible-useofmedicines-report#ims-form.
25. Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50:105–116. doi:10.1016/S0895-4356(96)00268-5
26. Al Ghobain M, Alhashemi H, Aljama A. Nonadherence to antihypertensive medications and associated factors in general medicine clinics. Patient Prefer Adherence. 2016;10:1415–1419. doi:10.2147/PPA.S100735
27. Rudnick KV, Sackett DL, Hirst S, Holmes C. Hypertension in a family practice. Can Med Assoc J. 1977;117(5):492–497.
28. Haynes RB, Taylor DW, Sackett DL, et al. Can simple clinical measurements detect patient noncompliance? Hypertension. 1980;2:757–764. doi:10.1161/01.HYP.2.6.757
29. Karve S, Cleves MA, Helm M, et al. Good and poor adherence: optimal cut-point for adherence measures using administrative claims data. Curr Med Res Opin. 2009;25:2303–2310. doi:10.1185/03007990903126833
30. Golightly YM, Allen KD, Ambrose KR, et al. Physical activity as a vital sign: a systematic review. physical activity as a vital sign: a systematic review. Prev Chronic Dis. 2017;14:170030. doi:10.5888/pcd14.170030
31. Centers for Disease Control and Prevention. Division of nutrition, physical activity, and obesity. about adult BMI. Available from: http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/.
32. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
33. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. doi:10.1093/eurheartj/ehy339
34. American Diabetes Association. Classification and diagnosis of diabetes. Sec. 2. in standards of medical care in diabetes—2015. Diabetes Care. 2015;38(Suppl. 1):S8–S16. doi:10.2337/dc15-S005
35. Murphy SP, Ibrahim NE, Januzzi JL. Heart failure with reduced ejection fraction: a review. JAMA. 2020;324(5):488–504. doi:10.1001/jama.2020.10262
36. Fenton A, Montgomery E, Nightingale P, et al. Glomerular filtration rate: new age- and gender- specific reference ranges and thresholds for living kidney donation. BMC Nephrol. 2018;19:336. doi:10.1186/s12882-018-1126-8
37. Khusun H, Yip R, Schultink W, Dillon DHS. World Health Organization hemoglobin cut-off points for the detection of anemia are valid for an Indonesian population. J Nutr. 1999;129(9):1669–1674. doi:10.1093/jn/129.9.1669
38. Nantsupawat N, Booncharoen A, Wisetborisut A, et al. Appropriate total cholesterol cut-offs for detection of abnormal LDL cholesterol and non-HDL cholesterol among low cardiovascular risk population. Lipids Health Dis. 2019;18(1):28. doi:10.1186/s12944-019-0975-x
39. Zhou B, Perel P, Mensah GA, et al. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol. 2021;18:785–802. doi:10.1038/s41569-021-00559-8
40. Chow CK, Gupta R. Blood pressure control: a challenge to global health systems. Lancet. 2019;394(10199):613–615. doi:10.1016/S0140-6736(19)31293-0
41. Fisher NDL, Curfman G. Hypertension-a public health challenge of global proportions. JAMA. 2018;320(17):1757–1759. doi:10.1001/jama.2018.16760
42. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
43. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
44. Sabaté E. Project WA to LTT, Network GAI, Diseases WHOD of M of N. Adherence to long-term therapies: evidence for action; 2003 Available from: http://www.who.int/iris/handle/10665/42682.
45. Ritchey M, Chang A, Powers C, et al. Vital signs: disparities in antihypertensive medication nonadherence among medicare part D beneficiaries — United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65:967–976. doi:10.15585/mmwr.mm6536e1
46. Bramley TJ, Gerbino PP, Nightengale BS, et al. Relationship of blood pressure control to adherence with antihypertensive monotherapy in 13 managed care organizations. J Manag Care Pharm. 2006;12(3):239–245. doi:10.18553/jmcp.2006.12.3.239
47. Hashmi SK, Afridi MB, Abbas K, et al. Factors associated with adherence to anti-hypertensive treatment in Pakistan. PLoS One. 2007;2(3):e280. doi:10.1371/journal.pone.0000280
48. Chelkeba L, Dessie S. Antihypertension medication adherence and associated factors at Dessie hospital, north East Ethiopia, Ethiopia. Int J Res Med Sci. 2013;1(3):191–197. doi:10.5455/2320-6012.ijrms20130802
49. Inkster ME, Donnan PT, MacDonald TM, et al. Adherence to antihypertensive medication and association with patient and practice factors. J Hum Hypertens. 2006;20(4):295–297. doi:10.1038/sj.jhh.1001981
50. Nakwafila O, Mashamba-Thompson T, Godi A, et al. A cross-sectional study on hypertension medication adherence in a high-burden region in Namibia: exploring hypertension interventions and validation of the Namibia Hill-bone compliance scale. Int J Environ Res Public Health. 2022;19:4416. doi:10.3390/ijerph19074416
51. de Souza AO, Ramos RN, de Oliveira T, et al. Adhesion to antihypertensive drug therapy in primary health care in a medium-sized Brazilian city. O Mundo da Saúde São Paulo. 2019;43(1):025–044.
52. Liu Q, Quan H, Chen G, et al. Antihypertensive medication adherence and mortality according to ethnicity: a cohort study. Can J Cardiol. 2014;30(8):925–931. doi:10.1016/j.cjca.2014.04.017
53. Tajeu GS, Kent ST, Huang L, et al. Antihypertensive medication nonpersistence and low adherence for adults <65 years initiating treatment in 2007–2014. Hypertension. 2019;74(1):35–46. doi:10.1161/HYPERTENSIONAHA.118.12495
54. Nguyen TPL, Schuiling-Veninga CCM, Nguyen TBY, et al. Adherence to hypertension medication: quantitative and qualitative investigations in a rural Northern Vietnamese community. PLoS One. 2017;12(2):e0171203. doi:10.1371/journal.pone.0171203
55. Shin S, Song H, Oh SK, et al. Effect of antihypertensive medication adherence on hospitalization for cardiovascular disease and mortality in hypertensive patients. Hypertens Res. 2013;36(11):1000–1005. doi:10.1038/hr.2013.85
56. Nashilongo MM, Singu B, Kalemeera F, et al. Assessing adherence to antihypertensive therapy in primary health care in Namibia: findings and implications. Cardiovasc Drugs Ther. 2017;31:565–578. doi:10.1007/s10557-017-6756-8
57. Girma F, Emishaw S, Alemseged F, et al. Compliance with anti-hypertensive treatment and associated factors among hypertensive patients on follow-up in Jimma University specialized hospital, Jimma, south west Ethiopia: a quantitative cross-sectional study. J Hypertens. 2014;3(5):1–6.
58. Gebreyohannes EA, Bhagavathula AS, Abebe TB, et al. Adverse effects and non-adherence to antihypertensive medications in University of Gondar Comprehensive Specialized Hospital. Clin Hypertens. 2019;25:1. doi:10.1186/s40885-018-0104-6
59. Pallangyo P, Millinga J, Bhalia S, et al. Medication adherence and survival among hospitalized heart failure patients in a tertiary hospital in Tanzania: a prospective cohort study. BMC Res Notes. 2020;13(1):89. doi:10.1186/s13104-020-04959-w
60. Gikunda GN, Gitonga L. Patients related factors associated with non-adherence to antihypertensive medication among patients at Chuka Referral Hospital, Kenya. Open J Clin Diagnostics. 2019;9:90–113. doi:10.4236/ojcd.2019.93007
61. Gikunda C, Gitonga L, Kamweru P. Patient and health system related factors associated with non-adherence to antihypertensive medication among patients at Chuka Referral Hospital, Kenya. Open J Clin Diagnostics. 2021;11:19–46. doi:10.4236/ojcd.2021.112002
62. Mweene MD, Banda J, Andrews B, et al. Factors associated with poor medication adherence in hypertensive patients in Lusaka, Zambia. Med J Zambia. 2010;37:3.
63. Osman FAA, Mohamed HH, Alhaj NA. Non-adherence to antihypertensive medication and its associated factors among cardiac patients at alshaab referred clinic, November 2017. Sudan J Med Sci. 2019;14(2):24–37.
64. Moss JT, Kimani H, Mwanzo I. Compliance to antihypertensive therapy and associated factors among adults’ hypertensive patients attending medical clinics in Kilifi County Kenya. Int J Commun Med Public Health. 2021;8(10):4655–4665. doi:10.18203/2394-6040.ijcmph20213758
65. Rana I, Shrestha P, Pokharel AS. Associated factors of treatment compliance among hypertensive patients of selected Hospital of Rupendehi. J Univ Coll Med Sci. 2020;8(1):70–73. doi:10.3126/jucms.v8i1.29788
66. Thomas D, Meera NK, Binny K, et al. Medication adherence and associated barriers in hypertension management in India. Glob Heart. 2011;6(1):9–13. doi:10.1016/j.cvdpc.2010.11.001
67. Kretchy I, Owusu-Daaku F, Danquah S. Spiritual and religious beliefs: do they matter in the medication adherence behaviour of hypertensive patients? Biopsychosoc Med. 2013;7(1):15. doi:10.1186/1751-0759-7-15
68. Abdul Wahab NA, Makmor Bakry M, Ahmad M, et al. Exploring culture, religiosity and spirituality influence on antihypertensive medication adherence among specialised population: a qualitative ethnographic approach. Patient Prefer Adherence. 2021;15:2249–2265. doi:10.2147/PPA.S319469
69. Atinga RA, Yarney L, Gavu NM. Factors influencing long-term medication non-adherence among diabetes and hypertensive patients in Ghana: a qualitative investigation. PLoS One. 2018;13(3):e0193995. doi:10.1371/journal.pone.0193995
70. Pirasath S, Sundaresan T. Descriptive cross-sectional study on knowledge, awareness and adherence to medication among hypertensive patients in a tertiary care center, Eastern Sri Lanka. SAGE Open Med. 2021;9:20503121211012497. doi:10.1177/20503121211012497
71. Wright-Nunes JA, Luther JM, Ikizler TA, Cavanaugh KL. Patient knowledge of blood pressure target is associated with improved blood pressure control in chronic kidney disease. Patient Educ Couns. 2012;88(2):184–188. doi:10.1016/j.pec.2012.02.015
72. Camara BS, Belaid L, Manet H, et al. What do we know about patient-provider interactions in sub-Saharan Africa? A scoping review. Pan Afr Med J. 2020;37:88. doi:10.11604/pamj.2020.37.88.24009
73. Mc Namara KP, Versace VL, Marriott JL, Dunbar JA. Patient engagement strategies used for hypertension and their influence on self-management attributes. Fam Pract. 2014;31(4):437–444. doi:10.1093/fampra/cmu026
74. Pirasath S, Sugathapala AGH, Wanigasuriya K. Descriptive cross-sectional study on knowledge, awareness, and adherence to medication among hypertensive patients at a tertiary care centre in Colombo District, Sri Lanka. Int J Hypertens. 2020;2020(2020):1320109. doi:10.1155/2020/1320109
75. Jo SH, Kim HS, Park KH, et al. GW29-e0714 self blood pressure monitoring improves awareness and attainment of target blood pressure goal: prospective observational study of 7751 patients. J Am Coll Cardiol. 2018;72(16_Supplement):C154. doi:10.1016/j.jacc.2018.08.705
76. Alexander M, Gordon NP, Davis CC, Chen RS. Patient knowledge and awareness of hypertension is suboptimal: results from a large health maintenance organization. J Clin Hypertens. 2003;5(4):254–260. doi:10.1111/j.1524-6175.2003.01963.x
77. Algabbani FM, Algabbani AM. Treatment adherence among patients with hypertension: findings from a cross-sectional study. Clin Hypertens. 2020;26:18. doi:10.1186/s40885-020-00151-1
78. Tesema S, Disasa B, Kebamo S, Kadi E. Knowledge, attitude and practice regarding lifestyle modification of hypertensive patients at Jimma University Specialized Hospital, Ethiopia. Prim Health Care. 2016;6(1):218.
79. Bakhsh LA, Adas AA, Murad MA, et al. Awareness and knowledge on hypertension and its self- care practices among hypertensive patients in Saudi. Ann Int Med Dent Res. 2017;2:5. doi:10.21276/aimdr.2017.3.5.ME13
80. Toole J, Kohansieh M, Khan U, et al. Does your patient understand their treatment plan? Factors affecting patient understanding of their medical care treatment plan in the inpatient setting. J Patient Exp. 2020;7(6):1151–1157. doi:10.1177/2374373520948400
81. Street RL; Street RL. How clinician-patient communication contributes to health improvement: modeling pathways from talk to outcome. Patient Educ Couns. 2013;92:286–291. doi:10.1016/j.pec.2013.05.004
82. Cubaka VK, Schriver M, Kayitare JB, et al. ‘He should feel your pain’: patient insights on patient-provider communication in Rwanda. Afr J Prim Health Care Fam Med. 2018;10(1):e1–e11. doi:10.4102/phcfm.v10i1.1514
83. Świątoniowska-Lonc N, Polański J, Tański W, et al. Impact of satisfaction with physician–patient communication on self-care and adherence in patients with hypertension: cross-sectional study. BMC Health Serv Res. 2020;20:1046. doi:10.1186/s12913-020-05912-0
84. Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. doi:10.1097/MLR.0b013e31819a5acc
85. Amoah EM, Okai DE, Manu A, et al. The role of lifestyle factors in controlling blood pressure among hypertensive patients in two health facilities in Urban Ghana: a cross-sectional study. Int J Hypertens. 2020;2020:9379128. doi:10.1155/2020/9379128
86. Bruno CM, Amaradio MD, Pricoco G, Marino E, Bruno F. Lifestyle and hypertension: an evidence-based review. J Hypertens Manag. 2018;4:30.
87. Organia EG, Pangandaman HK, Adap DM, et al. A systematic review on the effectiveness of lifestyle modifications in the management of hypertension. Int J Health Med Curr Res. 2019;4(04):1550–1564.
88. Blumenthal JA, Hinderliter AL, Smith PJ, et al. Effects of lifestyle modification on patients with resistant hypertension: results of the TRIUMPH randomized clinical trial. Circulation. 2021;144(15):1212–1226. doi:10.1161/CIRCULATIONAHA.121.055329
89. Xiao J, Ren WL, Liang YY, et al. Effectiveness of lifestyle and drug intervention on hypertensive patients: a randomized community intervention trial in rural China. J Gen Intern Med. 2020;35:3449–3457. doi:10.1007/s11606-019-05601-7
90. Nicoll R, Henein MY. Hypertension and lifestyle modification: how useful are the guidelines? Br J Gen Pract. 2010;60(581):879–880. doi:10.3399/bjgp10X544014
91. Yang MH, Kang SY, Lee JA, et al. The effect of lifestyle changes on blood pressure control among hypertensive patients [published correction appears in Korean J Fam Med. 2017 Sep; 38(5):311–312]. Korean J Fam Med. 2017;38(4):173–180. doi:10.4082/kjfm.2017.38.4.173
92. Babiker FA, Elkhalifa LA, Moukhyer ME. Awareness of hypertension and factors associated with uncontrolled hypertension in Sudanese adults. Cardiovasc J Afr. 2013;24(6):208–212. doi:10.5830/CVJA-2013-035
93. Fargally M, Elsadek A, Abdelhady AS, et al. Effect of lifestyle modification in hypertensive patients in Greater Cairo. Egypt J Hosp Med. 2013;53:991–1006. doi:10.12816/0001662
94. Appel LJ. Lifestyle modification as a means to prevent and treat high blood pressure. J Am Soc Nephrol. 2003;14(7 Suppl 2):S99–S102. doi:10.1097/01.ASN.0000070141.69483.5A
95. Pallangyo P, Misidai N, Komba M, et al. Knowledge of cardiovascular risk factors among caretakers of outpatients attending a tertiary cardiovascular center in Tanzania: a cross-sectional survey. BMC Cardiovasc Disord. 2020;20:364. doi:10.1186/s12872-020-01648-1
96. Alefan Q, Huwari D, Alshogran OY, Jarrah MI. Factors affecting hypertensive patients’ compliance with healthy lifestyle. Patient Prefer Adherence. 2019;13:577–585. doi:10.2147/PPA.S198446
97. Akbarpour S, Khalili D, Zeraati H, Mansournia MA, Ramezankhani A, Fotouhi A. Healthy lifestyle behaviors and control of hypertension among adult hypertensive patients. Sci Rep. 2018;8(1):8508. doi:10.1038/s41598-018-26823-5
98. Pallangyo P, Komba M, Mkojera ZS, et al. Non-communicable disease risk factors among caregivers of patients attending a tertiary cardiovascular hospital in Tanzania. Int J Gen Med. 2022;15:4685–4696. doi:10.2147/IJGM.S364392
99. Pallangyo P, Mkojera ZS, Hemed NR, et al. Obesity epidemic in urban Tanzania: a public health calamity in an already overwhelmed and fragmented health system. BMC Endocr Disord. 2020;20:147. doi:10.1186/s12902-020-00631-3
100. Pallangyo P, Mgopa LR, Mkojera Z, et al. Obstructive sleep apnea and associated factors among hypertensive patients attending a tertiary cardiac center in Tanzania: a comparative cross-sectional study. Sleep Sci Pract. 2021;5:17. doi:10.1186/s41606-021-00069-z
101. Pallangyo P, Mkojera ZS, Komba M, et al. Burden and correlates of cognitive impairment among hypertensive patients in Tanzania: a cross-sectional study. BMC Neurol. 2021;21(1):433. doi:10.1186/s12883-021-02467-3
102. Pallangyo P, Nicholaus P, Kisenge P, et al. A community-based study on prevalence and correlates of erectile dysfunction among Kinondoni District Residents, Dar es Salaam, Tanzania. Reprod Health. 2016;13:140. doi:10.1186/s12978-016-0249-2
103. Pallangyo P, Nicholaus P, Kisenge P, et al. High blood pressure, an epidemic inadequately diagnosed and poorly controlled: a community-based survey in Kinondoni District, Dar es Salaam Tanzania. GJMR-I. 2016;16:3.
104. Tapela NM, Clifton L, Tshisimogo G, et al. Prevalence and determinants of hypertension awareness, treatment, and control in Botswana: a nationally representative population-based survey. Int J Hypertens. 2020;2020:8082341. doi:10.1155/2020/8082341
105. Ojo OS, Malomo SO, Sogunle PT, Ige AM. An appraisal of blood pressure control and its determinants among patients with primary hypertension seen in a primary care setting in Western Nigeria. South African Fam Pract. 2016;58(6):1–10. doi:10.4102/safp.v58i6.4442
106. Devkota S, Dhungana RR, Pandey AR, et al. Barriers to Treatment and Control of Hypertension among Hypertensive Participants: a Community-Based Cross-sectional Mixed Method Study in Municipalities of Kathmandu, Nepal. Front Cardiovasc Med. 2016;3:26. doi:10.3389/fcvm.2016.00026
107. Sorato MM, Davari M, Kebriaeezadeh A, et al. Reasons for poor blood pressure control in Eastern Sub-Saharan Africa: looking into 4P’s (primary care, professional, patient, and public health policy) for improving blood pressure control: a scoping review. BMC Cardiovasc Disord. 2021;21:123. doi:10.1186/s12872-021-01934-6
108. Turé R, Damasceno A, Djicó M, Lunet N. Prevalence, awareness, treatment, and control of hypertension in Bissau, Western Africa. J Clin Hypertens. 2022;24(3):358–361. doi:10.1111/jch.14443
109. Masilela C, Pearce B, Ongole JJ, et al. Cross-sectional study of prevalence and determinants of uncontrolled hypertension among South African adult residents of Mkhondo municipality. BMC Public Health. 2020;20:1069. doi:10.1186/s12889-020-09174-7
110. Musinguzi G, Nuwaha F, Ashton N. Prevalence, awareness and control of hypertension in Uganda. PLoS One. 2013;8(4):e62236. doi:10.1371/journal.pone.0062236
111. Yazdanpanah L, Shahbazian H, Shahbazian H, Latifi SM. Prevalence, awareness and risk factors of hypertension in southwest of Iran. J Renal Inj Prev. 2015;4(2):51–56. doi:10.12861/jrip.2015.11
112. Mbouemboue OP, Ngoufack TJO. High blood pressure prevalence, awareness, control, and associated factors in a low-resource African setting. Front Cardiovasc Med. 2019;6:119. doi:10.3389/fcvm.2019.00119
113. Hien HA, Tam NM, Tam V, Derese A, Devroey D. Prevalence, awareness, treatment, and control of hypertension and its risk factors in (Central) Vietnam. Int J Hypertens. 2018;2018:6326984. doi:10.1155/2018/6326984
114. Lv X, Niu H, Qu Y, et al. Awareness, treatment and control of hypertension among hypertensive patients aged 18 to 59 years old in the northeast of China. Sci Rep. 2018;8:17019. doi:10.1038/s41598-018-34923-5
115. Wu Y, Tai ES, Heng D, et al. Risk factors associated with hypertension awareness, treatment, and control in a multi-ethnic Asian population. J Hypertens. 2009;27(1):190–197. doi:10.1097/HJH.0b013e328317c8c3
116. Calas L, Subiros M, Ruello M, et al. Hypertension prevalence, awareness, treatment and control in 2019 in the adult population of Mayotte. Eur J Public Health. 2022;2022:ckac015.
117. Gebrihet TA, Mesgna KH, Gebregiorgis YS, et al. Awareness, treatment, and control of hypertension is low among adults in Aksum town, northern Ethiopia: a sequential quantitative-qualitative study. PLoS One. 2017;12(5):e0176904. doi:10.1371/journal.pone.0176904
118. Pengpid S, Peltzer K. Prevalence, awareness, treatment and control of hypertension among adults in Kenya: cross-sectional national population-based survey. East Mediterr Health J. 2020;26(8):923–932. doi:10.26719/emhj.20.063
119. Damasceno A, Azevedo A, Silva-Matos C, et al. Hypertension prevalence, awareness, treatment, and control in Mozambique: urban/rural gap during epidemiological transition. Hypertension. 2009;54(1):77–83. doi:10.1161/HYPERTENSIONAHA.109.132423
120. Dhungana RR, Pandey AR, Shrestha N. Trends in the prevalence, awareness, treatment, and control of hypertension in Nepal between 2000 and 2025: a systematic review and meta-analysis. Int J Hypertens. 2021;2021:6610649. doi:10.1155/2021/6610649
121. Okello S, Muhihi A, Mohamed SF, et al. Hypertension prevalence, awareness, treatment, and control and predicted 10-year CVD risk: a cross-sectional study of seven communities in East and West Africa (SevenCEWA). BMC Public Health. 2020;20:1706. doi:10.1186/s12889-020-09829-5
122. Dzudie A, Kengne AP, Muna WFT, et al. Prevalence, awareness, treatment and control of hypertension in a self-selected sub-Saharan African urban population: a cross-sectional study. BMJ Open. 2012;2:e001217. doi:10.1136/bmjopen-2012-001217
123. Costa Filho FF, Timerman A, Saraiva JFK, et al. Independent predictors of effective blood pressure control in patients with hypertension on drug treatment in Brazil. J Clin Hypertens. 2018;20(1):125–132. doi:10.1111/jch.13139
124. Horsa BA, Tadesse Y, Engidawork E. Assessment of hypertension control and factors associated with the control among hypertensive patients attending at Zewditu Memorial Hospital: a cross sectional study. BMC Res Notes. 2019;12:152. doi:10.1186/s13104-019-4173-8
125. Menanga A, Edie S, Nkoke C, et al. Factors associated with blood pressure control amongst adults with hypertension in Yaounde, Cameroon: a cross-sectional study. Cardiovasc Diagn Ther. 2016;6(5):439–445. doi:10.21037/cdt.2016.04.03
126. Eghbali M, Khosravi A, Feizi A, et al. Prevalence, awareness, treatment, control, and risk factors of hypertension among adults: a cross-sectional study in Iran. Epidemiol Health. 2018;40:e2018020. doi:10.4178/epih.e2018020
127. Mohamed SF, Mutua MK, Wamai R, et al. Prevalence, awareness, treatment and control of hypertension and their determinants: results from a national survey in Kenya. BMC Public Health. 2018;18(Suppl 3):1219. doi:10.1186/s12889-018-6052-y
128. Beaney T, Schutte AE, Tomaszewski M, et al.; MMM Investigators. May measurement month 2017: an analysis of blood pressure screening results worldwide. Lancet Glob Health. 2018;6(7):e736–e743. doi:10.1016/S2214-109X(18)30259-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.