")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Medical Interns’ Knowledge, Attitude, and Practice Toward People Living with HIV: Multicenter Experience from Saudi Arabia
Authors Malli IA , Hamdan D, Aljahdali A, Almutairi A, Jar R, Alzahrani R, Khan MA
Received 26 April 2023
Accepted for publication 7 September 2023
Published 18 September 2023 Volume 2023:15 Pages 571—582
DOI https://doi.org/10.2147/HIV.S418948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Israa Abdullah Malli,1– 3 Dalia Hamdan,1,2 Alhanoof Aljahdali,1,2 Amal Almutairi,1,2 Raghad Jar,1,2 Reham Alzahrani,1,2 Muhammad Anwar Khan1,2
1Department of Basic Medical Sciences, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, 21423, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, 22384, Saudi Arabia; 3Ministry of the National Guard - Health Affairs, Jeddah, 22384, Saudi Arabia
Correspondence: Israa Abdullah Malli, Email [email protected]
Background: Discrimination by some healthcare providers toward people living with HIV/AIDS has been documented. Differences in cultural backgrounds make it harder for future doctors, who need a lot of knowledge and a positive attitude to treat patients. In conservative countries like Saudi Arabia, not enough is known about how much medical interns know about HIV and how they feel about people living with HIV/AIDS.
Methods: From April to September 2021, this cross-sectional study use non-probability random sampling and utilized a self-administered questionnaire to collected the data from 346 medical interns who had graduated from five different medical schools.
Results: Most of the subjects correctly identified the main transmission routes, such as unprotected sex (94.57%), blood and body fluid exchange (94.19%), and sharing needles or syringes (91.47%). But they did not know what the most common co-infections were for HIV patients or how to protect themselves after exposure. This paper showed that medical interns have some stigmatizing behaviors toward patients living with HIV, as 31.1% and 22.9% agreed, respectively, that they would feel more sympathetic toward people who get AIDS from blood transfusions compared to IV drug users (IDU).
Conclusion: Medical interns also showed some positive attitudes, as more than half of the sample (56.2%) would not isolate beds for people living with HIV/AIDS. The study’s conclusion is that HIV education and training programs should be added for medical interns, which might have a significant positive impact on their attitude.
Keywords: people living with HIV/AIDS, AIDS, medical, interns, knowledge, attitude, HIV, PLWHA
Introduction
Human immunodeficiency virus (HIV) is a member of the Retroviridae, a part of the Lentivirus family, based on its physical, biological, and genetic traits that cause HIV infection and acquired immune deficiency syndrome (AIDS).1,2 In HIV infection, the pathological condition is started by attacking and destroying the host immune cells, such as T-helper, dendritic, and macrophage.3–5 Acute HIV infection has a broad spectrum, ranging from hyperthermia to severe diseases. Thus, fever, fatigue, and myalgia are the most common symptoms of acute HIV infections.6 The major complication of HIV infection is its progression to AIDS if left untreated, which appears if the HIV-positive patient gets a low CD4 count and becomes prone to opportunistic infections.7,8 The most common ways to get HIV infection are through unprotected sexual contact and drug injection.9–11 Also, blood transfusion can transmit HIV, but it has been eliminated in countries that apply the HIV screening system for donated blood.12–15 Due to the availability of antiretroviral therapy (ART), which focuses on reducing the HIV viral load and maintaining the T-helper cells. Thus, normal life expectancy will be increased and progression to AIDS will be decreased by eliminating opportunistic infections.16–18
HIV remains a prominent cause of mortality and disease burden in many countries, despite substantial advances in prevention, treatment, and care.12,19 Globally, it was predicted that roughly 38 million individuals worldwide were infected with HIV.20 This startling figure demonstrates the scope of the pandemic and its consequences for public health institutions and impacted communities.12,20 The global HIV load is not uniformly distributed, with some places having a greater frequency of the virus than others. Sub-Saharan Africa, for example, has been disproportionately impacted by HIV, accounting for almost two-thirds of all people living with HIV worldwide.21 In the European Region, HIV infection continues to harm the health and welfare of millions of individuals. In 2021, more than 100 thousand people will be newly diagnosed with HIV.9,10 Saudi Arabia, with a population of more than 30 million, has been affected by the worldwide HIV pandemic. However, compared to other locations, the prevalence of HIV in Saudi Arabia has been reported to be lower than the worldwide norm.14,22
Different countries with high HIV prevalence rates may face diverse challenges in controlling the spread of HIV, influenced by cultural norms, government policies, and community engagement in prevention and awareness efforts.9,23 Sub-Saharan Africa, for instance, has encountered enormous obstacles in managing the pandemic due to economic restraints, limited access to free healthcare, and societal stigmas.12,21 To curb the spread of the virus, the Saudi government, in the form of the Ministry of Health, implemented extensive preventative and control initiatives such as rigorous screening procedures for immigrants, workers, pilgrims, and visitors, as well as mandatory premarital screening program.19,22,24 Also, as part of its HIV-fighting efforts, the Saudi government offers a proactive strategy and strives to guarantee that people living with HIV/AIDS (PLWHA) get free access to ART and equal medical services to manage the infection properly.22,24
Despite progress in understanding the virus and advancements in treatment choices, stigmatizing views against PLWHA have persisted since the epidemic’s inception.25 HIV-associated stigma can be defined as negative attitudes, beliefs, and actions directed toward PLWHA; it continues to be a serious issue in many areas of the globe. It stems from a lack of understanding, fear, prejudice, and societal norms.26 The extent and character of stigmatizing views might differ among areas and populations. Some communities saw a drop in stigmatizing attitudes because of educational initiatives and advocacy work targeted at debunking myths and misunderstandings regarding HIV.27,28 Stigma might have a serious impact on people living with HIV’s quality of life; some affected subjects might get discouraged from obtaining HIV testing and treatment or not disclosing their status; therefore, social stigma may stymie attempts to manage the pandemic by deteriorating their health status, increasing the number of incidences, and increasing the mortality rate.27,29
Medical practitioners are often the initial point of contact for people newly diagnosed with HIV; thus, they play a critical role in breaking the bad news and delivering effective care and support. However, researchers have reported that some medical practitioners might express hidden stigma toward people living with HIV.29–32 In the Lao People’s Democratic Republic, a study measured healthcare workers’ discrimination toward PLWHA. Of 558 participants, 49.7% of healthcare professionals showed discriminating attitudes towards HIV/AIDS patients, while low levels of prejudice were associated with professionals having proper knowledge and experience in treating HIV subjects.31 Also, a qualitative survey conducted in northwest England to investigate negative attitudes among dental practitioners found that one-third thought they were in jeopardy of acquiring the infection by treating patients. At the same time, one-fifth thought it was not their ethical responsibility to treat this high-risk group.33 In the same aspect, a study done in Puerto Rico showed that most participants showed judgmental attitudes toward those patients due to the stigma that living a dissolute lifestyle is the cause of acquiring HIV infection.29
The connection between medical professionals and PLWHA is based on trust, empathy, and efficient communication. In some conservative communities, they might be facing heavier duties to provide a safe and non-judgmental environment that helps to reduce the HIV stigma.25 In a study done in Iran, 42.42% of the 575 healthcare providers were asked how they felt about HIV/AIDS patients. They claimed that prejudice against PLWHA was primarily a result of social stigma, religion, and ignorance of the disease’s transmission.32 Saudi Arabian society is classified as one of the largest conservative communities, where Islamic religion and cultural norms might highly affect people living with HIV.22 Farahat et al demonstrated that higher multi-morbidity frequency is associated with increased age among PLWHA in Jeddah, western Saudi Arabia.19 Since medical care is available for free, it is unclear whether social stigma is contributing to this increase in the rate. Medical students are the future doctors who treat HIV patients, whose treatment requires much knowledge and a positive attitude. Medical interns’ stigma is underreported; thus, this study evaluates their knowledge and attitude toward people living with HIV in Jeddah, Saudi Arabia.
Materials and Methods
Study Design, Setting, and Study Period
This cross-sectional study was conducted using a structured questionnaire to assess medical interns’ knowledge and behavior toward PLWHA in Jeddah, Saudi Arabia, between January 2021 and March 2021. Graduates of five medical colleges were included in this study: College of Medicine at King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), the College of Medicine at King Abdul-Aziz University (KAU), the College of Medicine at Batterjee Medical College (BMC), the Ibn Sina National College for Medical Studies (ISNC), and the College of Medicine-Jeddah University (JU-COM). Three of the selected colleges are public, and two are private universities; all specialize in health sciences and are accredited by the Ministry of Education for various undergraduate degrees.
Sample Size and Sampling Method
This study was open to both male and female medical interns who had graduated from the schools listed and worked at hospitals in Jeddah for at least one month during the study period. So, it was decided that there are about 713 medical interns in Jeddah from five different colleges. The single proportion method will be used to figure out how many medical interns will be needed, with a figure of 50% of the population from previous research in Saudi Arabia. Cross-sectional research was used to figure out the sample size (n = the needed sample size, n = Z (/2) 2 pq / d2), and Raosoft, Inc. http://www.raosoft.com/samplesize.html was used to do the math. At the 95% confidence level (CI), the number of people who should know about HIV was estimated to be 50%, and the margin of error was set at 5%. The minimum sample size was determined to be 250.
Instruments of the Study
A structured questionnaire was developed and validated based on previously published surveys. The questionnaire has a demographics section and three themes: knowledge, attitude, and practice. It consisted of two sections: the first section included questions regarding the demographic profile; the second section had three multiple-choice questions intended to assess participants’ knowledge; and the third section had two practice questions. The primary outcome variable was the knowledge score, which was taken as the total score and ranged from 0 to 16 points. In the first version of the third section, 12 (5-point Likert scale questions) were intended to measure medical interns’ attitudes; three were positive, while the remaining were negative.
For validation purposes, a pilot study was conducted using 89 college students. The questionnaire was validated by calculating the internal consistency and reliability test using Cronbach’s alpha. In the first version, reliability testing was reported to be 0.333, considered low. After removing four negative questions, the internal reliability improved to 0.6842, which was acceptable A total of eight attitude questions related to HIV practice were represented and rated on a three-point categorical scale as negative (8–13), neutral (14–26), and positive (27–40). The questionnaire was distributed among the intern’s population using official email and was completed anonymously using the Google Forms platform. It was mandatory to complete all primary data variables to avoid missing or incomplete data in the analysis.34
Statistical Analysis
Qualitative data were reported as frequency and percentage, whereas continuous variables were presented as mean, standard deviation (SD), median, minimum, and maximum as appropriate. This cross-sectional study used the measure of association to identify the relationship between two or more variables. The Chi-square test of independence was performed to compare categorical data and assess the relationship between HIV knowledge and attitude scores and study variables. The Kruskal–Wallis test, a nonparametric test, was used to compare categorical or numerical variables. The significance level was set at <0.05. Collected data were tabulated and statistically analyzed using JMP software (John’s Macintosh Project), version 10.0 (SAS Institute Inc., Cary, NC, USA) for Windows, version 15.
Results
Participants’ Demographic Characteristics
A total of three hundred forty-six participants responded positively to the dispensed survey and were enrolled in this study. 186 (53.76%) were females, and 160 (46.24%) were males from five medical colleges in Jeddah city. Most subjects, 314 (90.75%), were Saudi nationals. Regarding marital status, 331 (95.66%) were singles. More than half of the 197 (56.94%) medical interns graduated from King Saud bin Abdul-Aziz University for Health Sciences, and the lowest number of participants, 12 (3.47%), were from Jeddah University (JU). 157 (45.38%) medical interns had 1–3 months of training, and 86 (24.86%) were medical interns for 7–9 months. Others, 66 (19.08%), were medical interns for 4–6 months, as shown in Table 1.
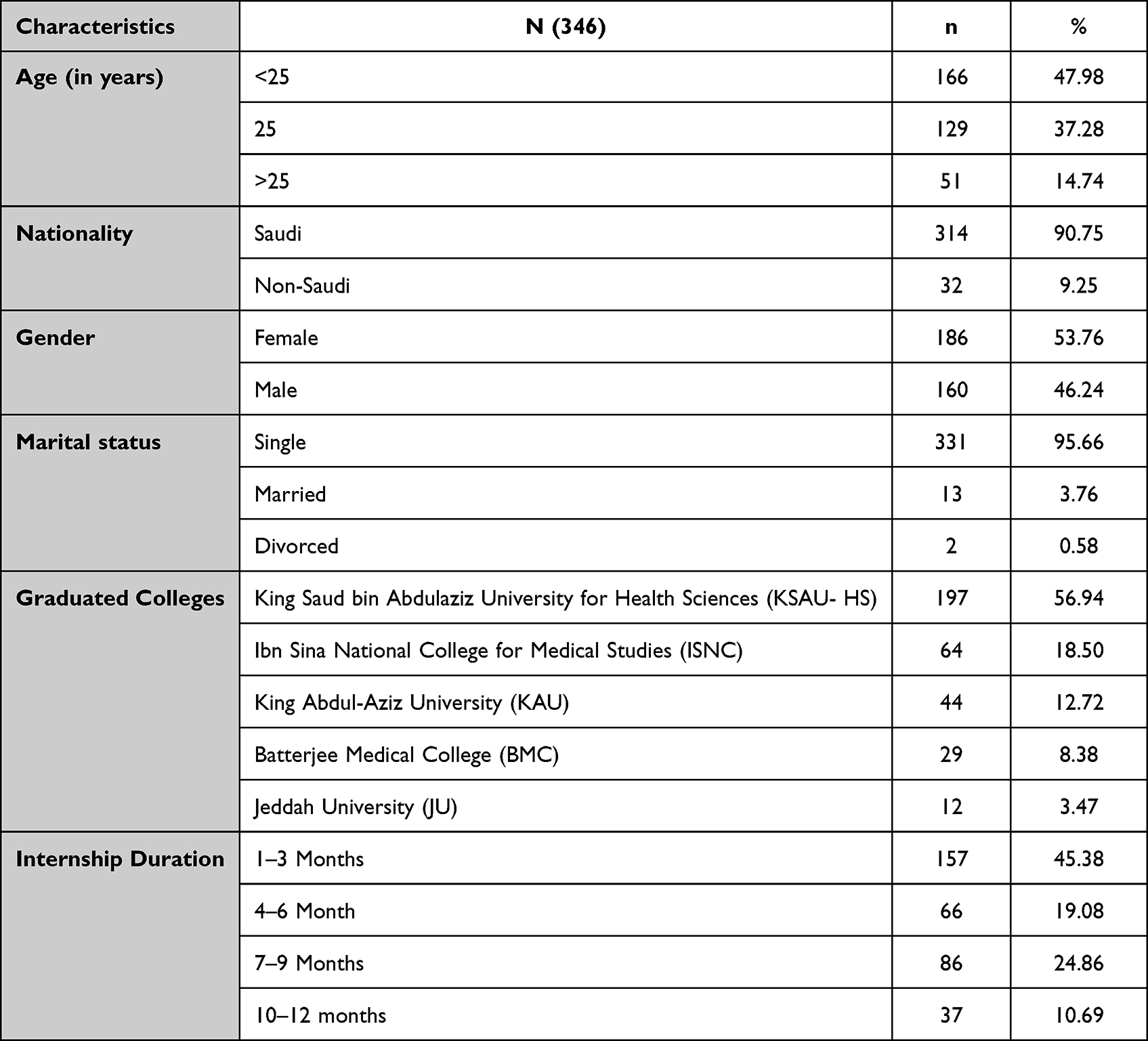 |
Table 1 Essential Medical Interns Demographic Characteristics |
Participants’ Knowledge of HIV Infection
When asked how much they knew about the different body fluids that could spread HIV, they could choose more than one answer. Out of 1257 selections, more than half of the medical interns selected the correct answers. The most common fluids selected by participants were blood (328, 26.09%), semen (312, 24.82%), and vaginal secretions (302, 24.03%), but breast milk was only selected 213 (16.95%) times by medical interns, those who believed it could transmit HIV. Saliva, sweat, and tears were the least likely to be selected, as shown in Figures 1 and 2. Also, the participants were asked to pick the correct answer among three statements regarding HIV transmission to evaluate their knowledge, which revealed that more than half of the medical interns, 216 (62.43%), agreed that “splashes with body fluids have a high risk for HIV transmission“. However, for the last statement, “Fluid splashes to intact skin or mucous membrane”, most participants (254, or 73.4%) did not agree. Also, 186 (53.76) of the medical interns agreed with the statement, “Percutaneous (needle-stick) injury has a risk of less than 1%”, as shown in Table 2.
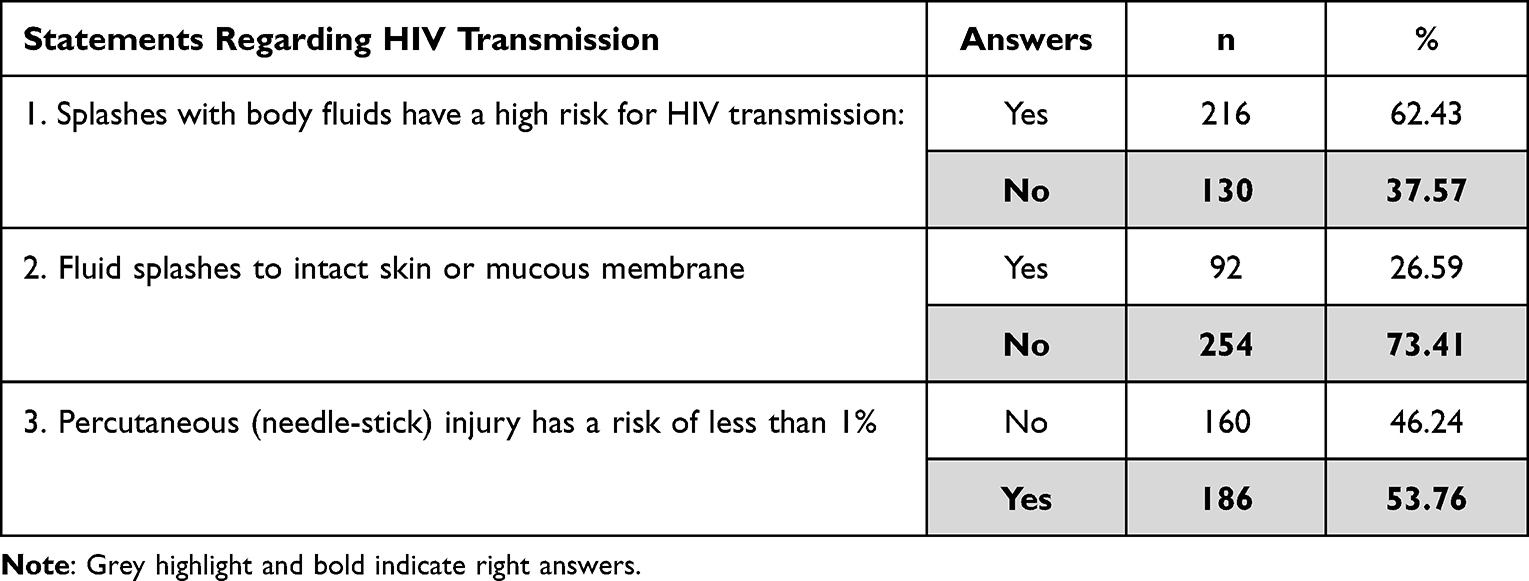 |
Table 2 HIV Transmission Knowledge Assessment |
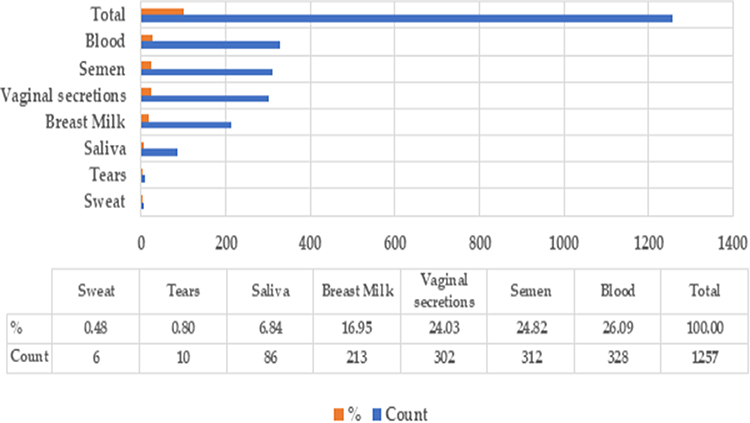 |
Figure 1 Participants’ knowledge of Body Fluids and HIV Transmission. |
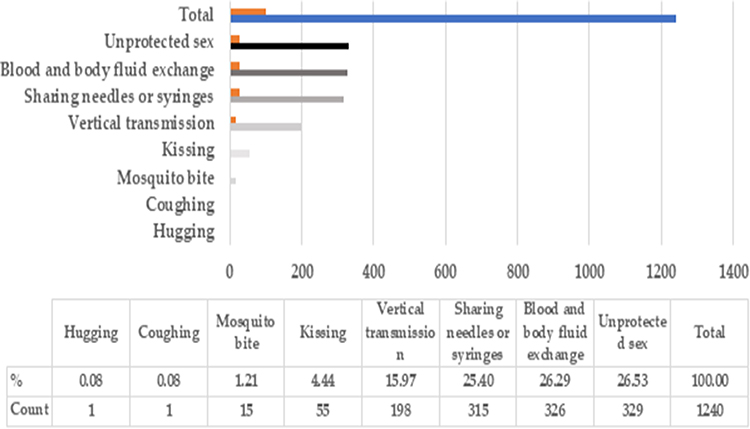 |
Figure 2 Mode of transmission of HIV infection. |
Also, the participants were asked about the correct statements regarding what they would do if they experienced a needle-stick injury from a patient with unknown HIV status. 228 of the medical professionals will check the patients’ HIV status, and 220 will use post-exposure prophylaxis (PEP). In addition, the majority had selected to report the exposure to infection control, while 132 would assess the patient’s HIV exposure risk. Furthermore, on-The-spot treatment for the injury and squeezing of the wound was the least to be selected, as shown in Figure 3. Hepatitis 278 was chosen by 80.35% of the people who took part in the study as the most common co-infection among people with HIV. The second one selected was tuberculosis (TB) at 45 (13.01%). The least common co-infections were Chlamydia 14 (4.05%) and Gonorrhea 4 (1.16%), as illustrated in Table 3.
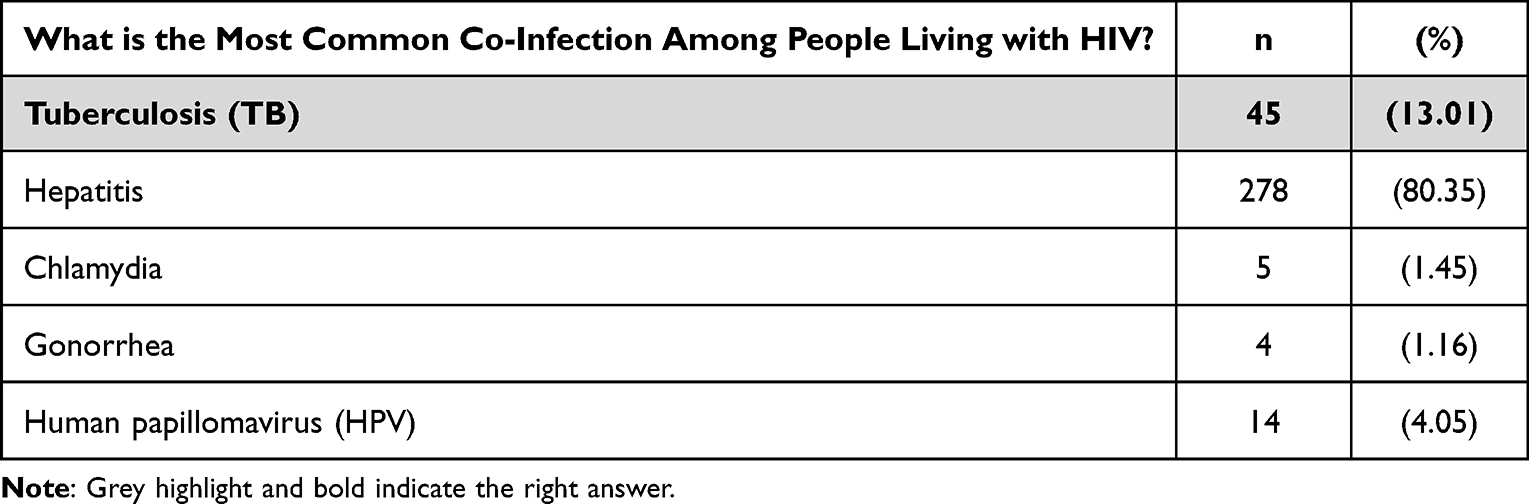 |
Table 3 The Most Common Co-Infection Among People Living with HIV |
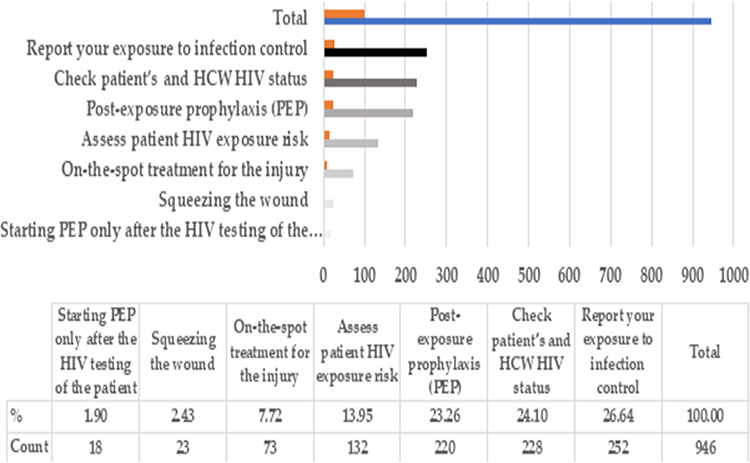 |
Figure 3 Management of needle-stick injury from an unknown HIV status. |
Participants’ Attitude Score
The attitude section of the survey was measured using a Likert scale ranging from strongly disagree to agree, as shown in Table 4. When participants were asked whether relatives or spouses should be notified regardless of the patient’s consent, 157 (45.38%) of the participants strongly disagreed, while 51 (14.74%) strongly agreed. Of the 346 participants, 138 (39.88%) refused to share their utensils and toilet with HIV-positive subjects. Moreover, 176 (50.87%) said they would keep the information about HIV-positive colleagues confidential. However, more than half of the participants (58.09%) believed an PLWHA should be denied a leadership position and banned from receiving some benefits. In comparison, 66 (19.08) would not mind PLWHA having leading positions. Additionally, 244 (70.52%) did consider treating HIV-infected patients a waste of resources.
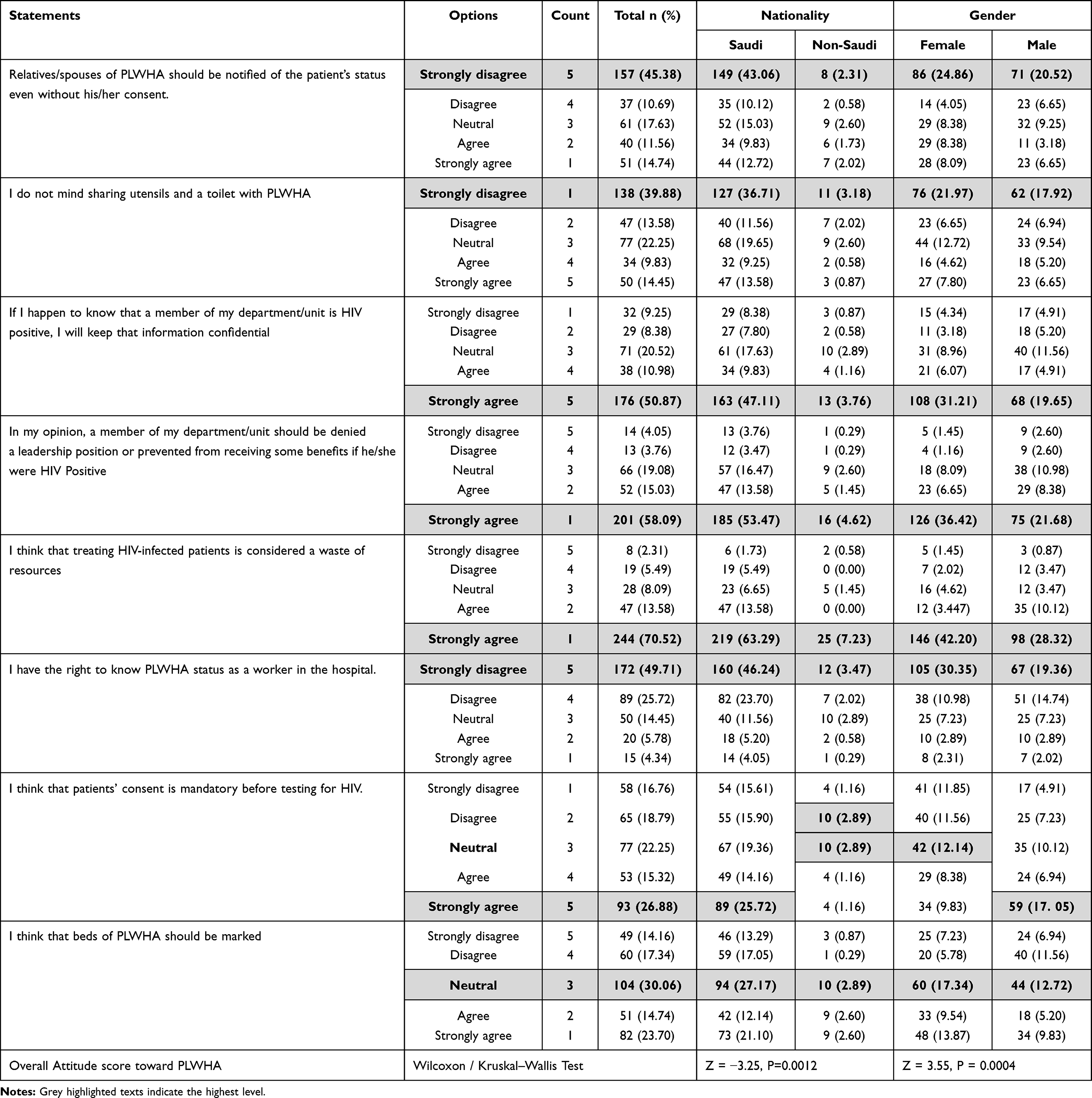 |
Table 4 Participants’ Attitude Toward HIV-Positive Subjects |
Moreover, more than half of the participants, 172 (49.71%), strongly disagreed that they had the right to know the PLWHA status as a health worker. Also, 93 (26.88%) of the participants strongly agreed with the requirement of the patient’s consent before testing for HIV infection. At the same time, the proportions of the strongly agreeing participants and those who were neutral about labeling the beds of PLWHA were close, at 82 (23.7%) and 104 (30.06%), respectively. The chi-square test of independence and fisher exact were used to find out if there was a link between gender and level of attitude. As outlined in Table 5, there was a statistically significant association between gender and attitude level (X2 (2) = 8.553, p = 0.0139*). The association was strong, and we can reject the null hypothesis and accept the alternative hypothesis, women have had more negative attitude than men, as shown in Table 5.
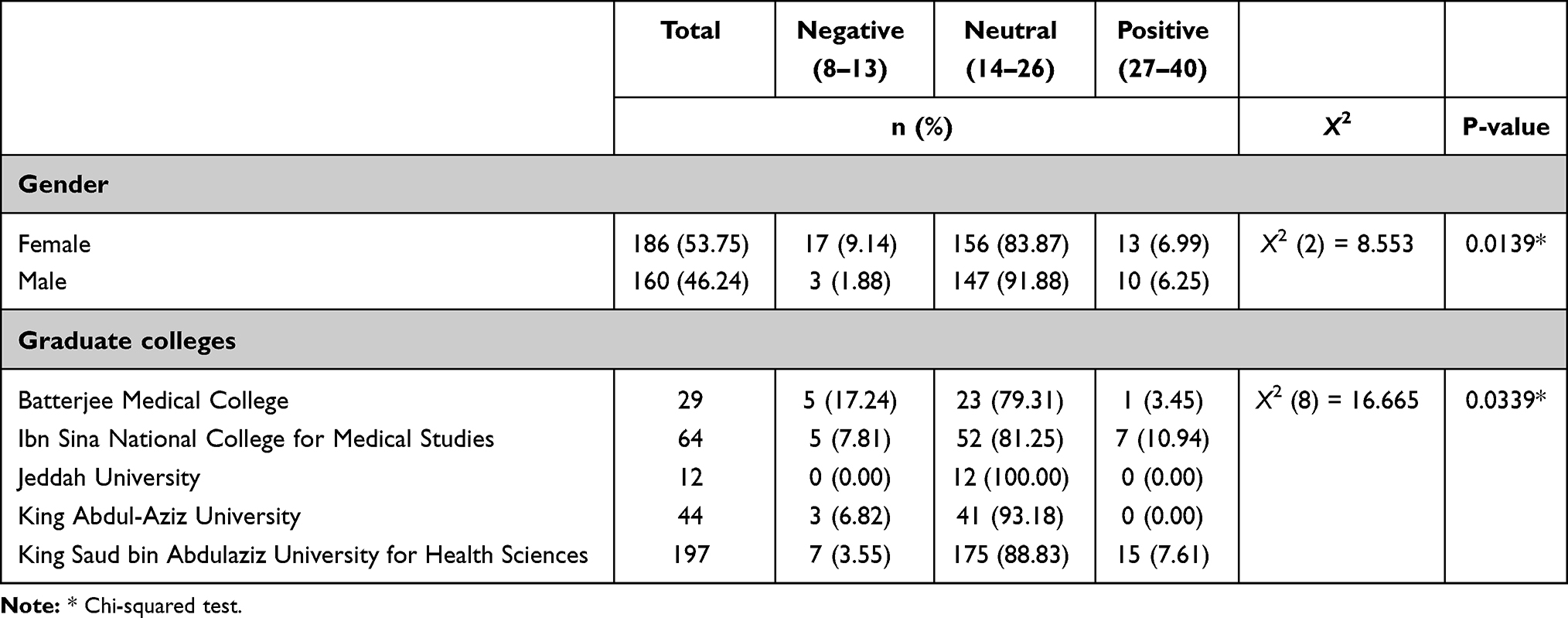 |
Table 5 The Association Between Attitude, Gender, and Graduate College |
Discussion
Despite advances in increasing awareness and lowering stigma, many areas and groups continue to face stigmatizing views concerning PLWHA.25 Medical professionals have an important role in providing medical treatment and emotional support to help people achieve optimum health outcomes and respect their dignity and autonomy.32,33 This study assessed medical interns’ knowledge and attitudes concerning PLWHA in Jeddah, Saudi Arabia. Our findings suggest that medical interns who had relatively poor knowledge about HIV prevalence, transmission, and treatment had a lower attitude than those with better knowledge who did not show any negative attitude.
Even though healthcare systems are different around the world, it has been shown that both society and healthcare providers care about PLWHA in the same way.30 There are several variables that contribute to HIV-related stigma, including medical interns’ misconceptions about how HIV is spread.26 The study showed that the issue of transmission routes was one of the areas in which interns had relatively common knowledge. Most of the subjects correctly identified the main transmission routes, such as unprotected sex (94.57%), blood and body fluid exchange (94.19%), and sharing needles or syringes (91.47%). However, there was a clear misconception and overestimation about the role of other transmission routes. For example, they selected kissing (14.73%), mosquito bites (3.88%), coughing (0.78%), and hugging (0.78%) as routes of transmission. This can cause concern, as this lack of knowledge might lead to undue apprehension during clinical practice.
Most participants were aware of which bodily fluids may transmit HIV. For instance, 94.96% of the interns knew that blood might transmit HIV, which is comparable to that reported in 2018 by Neerajaa et al, where 94% of participants believed HIV was avoidable, 89% recognized the transmission mechanism, 90% understood transmission control, and 84% had a positive attitude.35 However, our results are less than those of Platten et al in final-year medical students (100%).36 Aside from blood exposure, which poses the greatest risk of HIV transmission, other bodily fluids are also considered infectious, such as breast milk. Only 61.63% of the participants were aware that breast milk could transmit HIV. These results were less than those reported by Neerajaa et al in a medical intern. Saliva, tears, and sweat are not contagious unless bloody.35 Only a few of the participants were unaware of this fact, as only 25.58%, 3.49%, and 1.94% of the interns gave incorrect answers, respectively. Upon asking about the most common co-infection among HIV patients, the results were not promising. Only 13.01% of the medical interns identified TB as the most common co-infection with HIV. On the other hand, a study done in Vietnam on final-year medical students revealed better results. (90%) subjects identified TB as the most common co-infection with HIV.36
In our study, upon being asked what they should do if they got a needle-stick injury at work from a patient with unknown HIV status, 67.44% of interns said they would use post-exposure prophylaxis, which is comparable to the results revealed by Kasat et al in interns (68.8%).33 Also, 43.41% of our interns said they would assess patient’s HIV exposure risk, while 56.59% said they would not. This relatively low awareness regarding the proper management of HIV exposure was found among participants in this study. Other studies may be attributable to multiple reasons, such as low clinical experience, HIV prevalence in the era, and an emphasis on HIV in the curriculum. Screening for co-infection among HIV patients must be done earlier, as the CDC recommends. Hence, a lack of knowledge will compromise the patient’s quality of care and lead to many complications.37
Saudi Arabia faces a significant struggle to tolerate PLWHA. The causes have been linked to highly traditional Islamic beliefs and a high level of moral instruction, to the point where open discussion about sex is rare.38 As a result, the assumption that positive cases of HIV/AIDS are thought to have been acquired due to sexual misconduct is unacceptable in Islamic society.24 This study shows that medical interns stigmatize PLWHA. This result supports a similar study to evaluate the knowledge and attitude of healthcare providers in Saudi Arabia.24,38 The stigmatizing attitude could be attributed to the social stigma and the religious and conservative nature of the Saudi community, as HIV is associated with drug abuse and promiscuity. This appears as (31.1%) and (22.9%) strongly agree and agree, respectively, that they would feel more sympathetic toward people who get AIDS from blood transfusions compared to IV drug users (IDU).37 This manifested well in another study, where physicians showed less sympathy toward IDU and extramarital sex.38
The interns also showed some positive attitudes, as more than half of the sample (56.2%) would not isolate the beds of PLWHA. In contrast to another study, 78.42% of the sample asked for a different ward for HIV patients.38 This difference could result from a lack of knowledge or from the different samples, as this study targeted medical interns and postgraduates. Lack of knowledge of transmission routes could be a reason for the stigmatizing attitudes. This manifested itself in this study in that a lot of people, collectively, would not share utensils or toilets with the PLWHA. However, the link between stigmatizing attitudes and a lack of knowledge contradicts one study while being supported by another.39,40 It is believed that the conservative community and the association of HIV with promiscuity and IDU play major roles in the stigmatization of PLWHA. This is consistent with the findings of another study.41
Conclusions
Stigma continues to be a significant impediment to successful HIV prevention, treatment, and care. This study showed that medical interns have insufficient knowledge regarding the HIV mode of transmutation, the most common co-HIV infection, and the proper post-exposure prophylaxis. Moreover, the study showed that interns in Jeddah have stigmatizing behavior toward PLWHA, and a lack of knowledge about HIV can explain the stigmatizing behavior toward HIV patients. To tackle HIV-related stigma, a multimodal strategy is required, such as extensive and accurate education programs to debunk myths and misunderstandings regarding HIV transmission, treatment, and prevention. To establish a more inclusive and compassionate society for PLWHA, governments, healthcare institutions, civil society groups, and individuals must work together to address workplace stigma. Enacting and implementing legislation that safeguards the rights of PLWHA may also assist in avoiding discrimination from medical practitioners and providing equitable access to healthcare, employment, and other medical services. Based on the results, more education and training programs for medical interns are necessary to fill the knowledge gap, which should significantly impact their attitude.
Institutional Review Board Statement
The Institutional Review Board (IRB) and the Research Board of King Abdullah International Medical Research Center (KAIMRC) approved this study design following the Helsinki Declaration’s ethical criteria. Study Number: SP20/150/J, approval memo number: IRBC/0825/20, and the approval date is the 8th of June 2020. Before completing the anonymous survey, participants provided their informed written consent, no identifiable personal data was retained no biological specimens were collected.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Sharing Statement
The data used to support the findings of this study have been deposited in the 4TU.ResearchData repository [10.4121/22225849].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Ghosn J, Taiwo B, Seedat S, Autran B, Katlama C. HIV. Lancet. 2018;392:685–697. doi:10.1016/s0140-6736(18)31311-4
2. Coffin J, Blomberg J, Fan H, et al. ICTV virus taxonomy profile: Retroviridae 2021. J Gen Virol. 2021;102. doi:10.1099/jgv.0.001712
3. Del Rio C. The global HIV epidemic: what the pathologist needs to know. Semin Diagn Pathol. 2017;34:314–317. doi:10.1053/j.semdp.2017.05.001
4. Visseaux B, Le Hingrat Q, Damond F, Charpentier C, Descamps D. Physiopathology of HIV-2 Infection. Virologie. 2019;23:277–291. doi:10.1684/vir.2019.0789
5. Macatangay BJ, Rinaldo CR. Regulatory T Cells in HIV Immunotherapy. HIV Ther. 2010;4:639–647. doi:10.2217/hiv.10.51
6. Lin T-Y, Yang C-J, Liu C-E, et al. Clinical features of acute human immunodeficiency virus infection in Taiwan: a multicenter study. J Microbiol Immunol Infect. 2019;52:700–709. doi:10.1016/j.jmii.2018.01.005
7. Kaushic C. HIV-1 infection in the female reproductive tract: role of interactions between HIV-1 and genital epithelial cells. Am J Reprod Immunol. 2011;65:253–260. doi:10.1111/j.1600-0897.2010.00965.x
8. Xiao T, Cai Y, Chen B. HIV-1 entry and membrane fusion inhibitors. Viruses. 2021;13:735. doi:10.3390/v13050735
9. McCann NC, Stanic T, Penazzato M, et al. The expanding epidemic of HIV-1 in the Russian Federation. PLoS Med. 2017;14:e1002462. doi:10.1371/journal.pmed.1002462
10. Okano JT, Sharp K, Valdano E, Palk L, Blower S. HIV transmission and source–sink dynamics in sub-Saharan Africa. Lancet HIV. 2020;7:e209–e214. doi:10.1016/s2352-3018(19)30407-2
11. Kostaki E-G, Karamitros T, Bobkova M, et al. Spatiotemporal Characteristics of the HIV-1 CRF02_AG/CRF63_02A1 Epidemic in Russia and Central Asia. AIDS Res Hum Retroviruses. 2018;34:415–420. doi:10.1089/aid.2017.0233
12. Zakeyo K, Nyashanu M. Exploring the potential causes of HIV prevalence among young women in South Africa: a critical literature review. Int J Hum Rights Healthc. 2021. doi:10.1108/ijhrh-12-2020-0106
13. CDC. Fact sheets, testing & diagnosis, recommendations for human immunodeficiency virus (HIV) screening in tuberculosis (TB) clinics. Available from: https://www.cdc.gov/tb/publications/factsheets/testing/hivscreening.htm.
14. Alsughayyir J, Almalki Y, Alburayk I, et al. Prevalence of transfusion-transmitted infections in Saudi Arabia Blood Donors. Saudi Med J. 2022;43:1363–1372. doi:10.15537/smj.2022.43.12.20220634
15. Zulfiqar HF, Javed A, Afroze B, et al. HIV diagnosis and treatment through advanced technologies. Front Public Health. 2017;5:5. doi:10.3389/fpubh.2017.00032
16. Kammers K, Chen A, Monaco DR, et al. HIV antibody profiles in HIV controllers and persons with treatment-induced viral suppression. Front Immunol. 2021:12. doi:10.3389/fimmu.2021.740395
17. Genovese L, Nebuloni M, Alfano M. Cell-mediated immunity in elite controllers naturally controlling HIV viral load. Front Immunol. 2013;4:4. doi:10.3389/fimmu.2013.00086
18. Mwangi A, van Wyk B. factors associated with viral suppression among adolescents on antiretroviral therapy in Homa Bay County, Kenya: a retrospective cross-sectional study. Res Palliat Care. 2021;13:1111–1118. doi:10.2147/hiv.s345731
19. Farahat FM, Alghamdi YS, Farahat AF, et al. The prevalence of comorbidities among adult people diagnosed with HIV infection in a tertiary care hospital in Western Saudi Arabia. J Infect Public Health. 2020;13:1699–1704. doi:10.1016/j.jiph.2020.08.009
20. Gupta S, Granich R. Age-specific national HIV care continua in Sub-Saharan Africa. J Virus Erad. 2018;4:13. doi:10.1016/s2055-6640(20)30360-5
21. Moyo E, Moyo P, Murewanhema G, Mhango M, Chitungo I, Dzinamarira T. Key Populations and Sub-Saharan Africa’s HIV Response. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1079990
22. Baadani AM, Ballool S, Alhemyadi S, et al. The clinical outcome of HIV infection at a tertiary care center in Riyadh, Saudi Arabia. Saudi Med J. 2020;41:965–970. doi:10.15537/smj.2020.9.25274
23. Johnson LF, Neilan AM, Davies M, et al. Prevalence of undiagnosed HIV among Children in South Africa, Côte d’Ivoire and Zimbabwe: a model‐based analysis to inform paediatric HIV screening programmes. J Int AIDS Soc. 2022:25. doi:10.1002/jia2.26045
24. Al-Mozaini M, Alrahbeni T, Dirar Q, Alotibi J, Alrajhi A. HIV in the Kingdom of Saudi Arabia: can we change the way we deal with co-infections. Infect Drug Resist. 2021;14:111–117. doi:10.2147/idr.s270355
25. Grossman CI, Stangl AL. Global Action to Reduce HIV Stigma and Discrimination. J Int AIDS Soc. 2013;16:18881. doi:10.7448/ias.16.3.18881
26. Kane JC, Elafros MA, Murray SM, et al. A scoping review of health-related stigma outcomes for high-burden diseases in low- and middle-income countries. BMC Med. 2019;17. doi:10.1186/s12916-019-1250-8
27. Watt MH, Knippler ET, Minja L, et al. A counseling intervention to address HIV stigma at entry into antenatal care in Tanzania (Maisha): study protocol for a pilot randomized controlled trial. Trials. 2019;20. doi:10.1186/s13063-019-3933-z
28. Watt MH, Minja L, Knettel BA, et al. Pilot outcomes of maisha: an HIV stigma reduction intervention developed for antenatal care in Tanzania. AIDS Behav. 2020;25:1171–1184. doi:10.1007/s10461-020-03093-9
29. Ruiz-Torres Y, Cintrón-Bou FN, Varas-Díaz N. AIDS-related stigma and health professionals in Puerto Rico. Rev Interam De Psicol. 2007;41(1):49–56.
30. Katz IT, Ryu AE, Onuegbu AG, et al. Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis. J Int AIDS Soc. 2013;16:18640. doi:10.7448/ias.16.3.18640
31. Vorasane S, Jimba M, Kikuchi K, et al. An investigation of stigmatizing attitudes towards people living with HIV/AIDS by doctors and nurses in Vientiane, Lao PDR. BMC Health Serv Res. 2017;17:17. doi:10.1186/s12913-017-2068-8
32. Zarei N, Joulaei H, Darabi E, Fararouei M. Stigmatized attitude of healthcare providers: a barrier for delivering health services to HIV positive patients. Int J Community Based Nurs Midwifer. 2015;3(4):292–300.
33. Kasat V, Saluja H, Ladda R, Sachdeva S, Somasundaram K, Gupta A. Knowledge, attitude and practices toward post exposure prophylaxis for human immunodeficiency virus among dental students in India. Ann Med Health Sci Res. 2014;4:543. doi:10.4103/2141-9248.139308
34. Sullivan GM, Artino AR. Analyzing and interpreting data from likert-type scales. J Grad Med Educ. 2013;5:541–542. doi:10.4300/jgme-5-4-18
35. Neerajaa L, Vijayakarthikeyan M, Umadevi R. A study on awareness regarding HIV/AIDS among medical students in Kancheepuram District, Tamil Nadu. Int J Community Med Public Health. 2018;5:4242. doi:10.18203/2394-6040.ijcmph20183885
36. Platten M, Pham HN, Nguyen HV. Knowledge of HIV and factors associated with attitudes towards HIV among final-year medical students at Hanoi medical university in Vietnam. BMC Public Health. 2014;14:14. doi:10.1186/1471-2458-14-265
37. Rossato Silva D, Müller AM, de Tarso Roth Dalcin P. Factors associated with delayed diagnosis of tuberculosis in hospitalized patients in a high TB and HIV burden setting: a cross-sectional study. BMC Infect Dis. 2012;12:12. doi:10.1186/1471-2334-12-57
38. Aldhaleei WA, Bhagavathula AS. HIV/AIDS-knowledge and attitudes in the Arabian peninsula: a systematic review and meta-analysis. J Infect Public Health. 2020;13:939–948. doi:10.1016/j.jiph.2020.04.002
39. Zuber J, Werner J. Analyse von Vorurteilsstrukturen bei medizinischem Personal gegenüber HIV-Positiven und AIDS-Kranken. [Analysis of preconceived attitudes of medical personnel toward HIV positive and AIDS patients]. Psychother Psychosom Med Psychol. 1996;46(2):52–60. German.
40. Krasnik A, Fouchard JR, Bayer T, et al. Health workers and AIDS: knowledge, attitudes and experiences as determinants of anxiety. Scand J Soc Med. 1990;18(2):103–113. doi:10.1177/14034948900180020Bibliography
41. Memish ZA, Filemban SM, Bamgboyel A, Al Hakeem RF, Elrashied SM, Al-Tawfiq JA. Knowledge and attitudes of doctors toward people living with HIV/AIDS in Saudi Arabia. J Acquir Immune Defic Syndr. 2015;69:61–67. doi:10.1097/qai.0000000000000550
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.