")
Back to Journals » International Medical Case Reports Journal » Volume 17
Lethal Immune Myocarditis and Myasthenia Gravis Due to Anti-PD-1 Treatment for a Bladder Cancer Patient: A Case Report and Possible Treatment Inspiration
Authors Gao P , Li X, He Z, Zhang H, Zhang Z, Liu Z
Received 5 December 2023
Accepted for publication 4 April 2024
Published 18 April 2024 Volume 2024:17 Pages 359—365
DOI https://doi.org/10.2147/IMCRJ.S449525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Pan Gao,1,2 Xinyu Li,1,2 Ziqiu He,1,2 Hongbo Zhang,1,2 Zhi Zhang,1,2 Zonglai Liu1,2
1Department of Urology, Second People’s Hospital of Yichang, Yichang, Hubei Province, People’s Republic of China; 2Department of Urology, Second People’s Hospital of China Three Gorges University, Yichang, Hubei Province, People’s Republic of China
Correspondence: Zonglai Liu, Department of Urology, Second People’s Hospital of Yichang, Second People’s Hospital of China Three Gorges University, 21 Xiling One Road, Yichang, 443000, Hubei Province, People’s Republic of China, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICI) have become a new hope for many patients with advanced cancer by blocking tumor immune escape. Bladder cancer is a common malignant tumor of the urinary tract epithelium that often relapses and metastasizes after surgery, chemotherapy, and radiotherapy. Immunotherapy has dramatically improved patient survival rates and clinical benefits as a new, potentially effective therapy. However, avoidance of various immune-related adverse events (irAEs) remains an implausible idea. ICI-induced myocarditis is different from viral myocarditis, and mortality is still high with the current treatment. We report the case of an 82-year-old female patient with ICI-induced fulminant myocarditis and myasthenia gravis. Although she actively accepted the current mainstream treatment for immune-related myocarditis and myasthenia, she died of heart and respiratory failure. Analyzing and reporting the patient’s disease development process and the changes in related indicators may help peers gain a deeper understanding of immune-related adverse events and reduce the mortality of immune-related myocarditis.
Keywords: immune checkpoint inhibitors, immunotherapy, heart failure, multiple organs failure
Introduction
Urothelial carcinomas (UCs) rank as one of the most prevalent tumors globally and can be found in various locations, including the bladder, urethra, pyelocaliceal cavities, and ureter.1 Notably, bladder cancer (BC) tumors constitute the majority of UCs, accounting for 90–95% of cases, whereas upper tract UCs (UTUCs) are relatively rare, comprising only 5–10% of the total UCs.2 Over 200,000 deaths attributed to Urothelial carcinoma each year.3 Many clinical trials have evaluated the efficacy and toxicity of checkpoint inhibitors in treating urothelial cancer in metastatic, local muscle-invasive, upper urothelial, and non-muscle invasive bladder cancer.4
Immune checkpoint inhibitors (ICIs) play an established role in modern medical institutions and may expand their applications. Based on self-immune tolerance under normal conditions, the PD-1/PD-L1 immune checkpoint can maintain a balance between T cell activation, tolerance, and immune-mediated tissue damage by negatively regulating T cell function. In the tumor microenvironment, PD-1 is highly expressed on tumor-specific T cells and PD-L1 can also be expressed on tumor cells. The combination of PD-1/PD-L1 can activate tumor-specific T cells, thus causing adaptive immunity and maintaining immune tolerance in the microenvironment.5 Cells can use immune homeostasis to evade immune surveillance and promote the growth of malignant tumors. Combining immune checkpoint inhibitors (ICI) with PD-1 or PD-L1 can block the combination of tumor cells with T cells, so that T cells can continue to play their immune role normally, thus eliminating tumor cells. However, although T cells kill tumor cells, they may also damage normal tissues, leading to immune-related adverse events (irAEs).6 We report a case of fatal myocarditis and myasthenia gravis caused by ICIs and provide possible treatment enlightenment.
Case Presentation
In June 2022, an 82-year-old female patient underwent laparoscopic radical resection of the right kidney, right ureter, and partial cystectomy at our hospital due to ureteral and bladder tumors. Post-surgical pathology confirmed a high-grade invasive urothelial carcinoma (T2N0M0). Following the procedure, the patient received regular bladder infusions of gemcitabine chemotherapy and was administered Tislelizumab, a domestically produced anti-PD-1 mAb (administered as 200 mg intravenous infusions every 3 weeks). Prior to commencing treatment, her electrocardiogram (ECG) and transthoracic echocardiography (TTE) were within normal limits (her electrocardiogram (ECG) and transthoracic echocardiography (TTE) were within normal limits (Figure 1), and her myocardial enzyme levels, myocardial infarction markers, and N-terminal B-type natriuretic peptide precursor were all within the normal range. However, after 7 weeks of immunotherapy, the patient presented with symptoms including dizziness, chest tightness, fatigue, and drooping eyelids, leading to her readmission to our hospital on July 20, 2022.
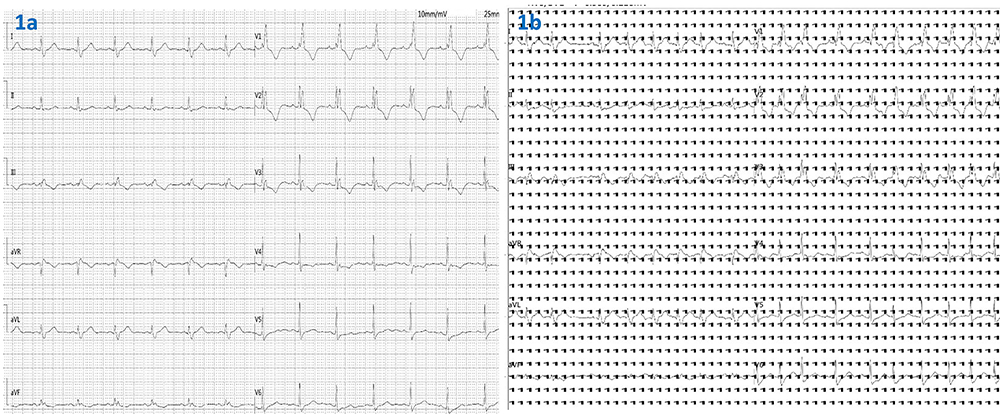 |
Figure 1 Electrocardiogram images showed changes in electrocardiogram during the course of the disease. (a) Electrocardiogram of the patient before immunotherapy. (b) Electrocardiogram of the patient after seven weeks of immunotherapy: Appeared tachycardia, complete right bundle branch block, and abnormal ST-T segment. |
Upon admission, the patient presented with vital signs including a body temperature of 36.2°C, a pulse of 75 beats per minute, and a blood pressure of 145/90 mmHg. Given her condition, we promptly conducted relevant laboratory tests, electrocardiogram (ECG), and transthoracic echocardiography (TTE). The ECG revealed tachycardia, complete right bundle branch block, and an abnormal ST-T segment (Figure 1). TTE showed decreased diastolic function of the left ventricle (LV) with an ejection fraction (LVEF) of 65%. COVID-19 testing was negative. However, there were significant elevations in several markers, including glutamic pyruvic transaminase (403 U/L), glutamic oxaloacetic transaminase (787 U/L), lactate dehydrogenase (1518 U/L), α-hydroxybutyrate (1310 U/L), creatine kinase (5718 U/L), creatine kinase isoenzyme (mass) (167.10 ng/mL), creatinine (109 umol/L), myoglobin (>4104.00 ng/mL), and cardiac troponin T (5.16 ng/mL). We reviewed her medical history and consulted with the Cardiology Department, leading to a diagnosis of immune checkpoint inhibitor (ICI)-mediated myocarditis and myasthenia gravis (MG).
Treatment was initiated with immunosuppressive therapy using corticosteroids (intravenous methylprednisolone 1g/day). The patient also received continuous ECG monitoring, oxygen therapy, gastric and liver protection, diuretics, and fluid replacement. Adenosine Cyclophosphate was administered intravenously to address myocardial hypoxia and liver damage. After three days, there were improvements in laboratory markers, but the patient’s condition suddenly worsened with delirium, hypoxemia, irregular heartbeat, and hypotension. She was transferred to the intensive care unit (ICU) for endotracheal intubation and mechanical ventilation.
Further testing in the ICU revealed negative results for acetylcholine, acetylacetic acid, acetyltriamine, acetyl striated muscle, and gamma globulin antibodies. However, the anti-titin antibody was positive (1:300), and the myositis spectrum test showed a positive cN1A antibody (1:30). Respiratory pathway antibody testing was negative for various pathogens. Autoimmune antibody testing was also negative, except for a slightly elevated anti-nuclear antibody level (13.40 AU/mL). Based on these findings, we confirmed the diagnosis of ICI-mediated myocarditis and MG, ruling out other potential causes.
Treatment in the ICU continued with methylprednisolone and cholinesterase inhibitor neostigmine. Peripheral blood T lymphocyte subpopulations showed abnormalities, leading to the addition of tacrolimus as an immunosuppressant. After four weeks of hormone therapy, we attempted to wean the patient off the ventilator. However, she suddenly lost consciousness, developed respiratory failure, and experienced cardiac arrest. Despite immediate cardiopulmonary resuscitation and reintubation, multiple attempts to wean her off the ventilator failed. One month following tracheal intubation and the utilization of ventilator-assisted breathing, the patient developed severe lung infections due to fungal and multidrug-resistant bacterial invasion, as confirmed by general bacterial smears, acid-fast smears, fungal smears, as well as sputum and urine culture tests. Vital indicators were consistently monitored throughout the entirety of the treatment process (Figures 2–4). Despite receiving 43 days of aggressive medical intervention, the patient ultimately succumbed to myasthenia gravis and multiple organ failure on September 3, 2022.
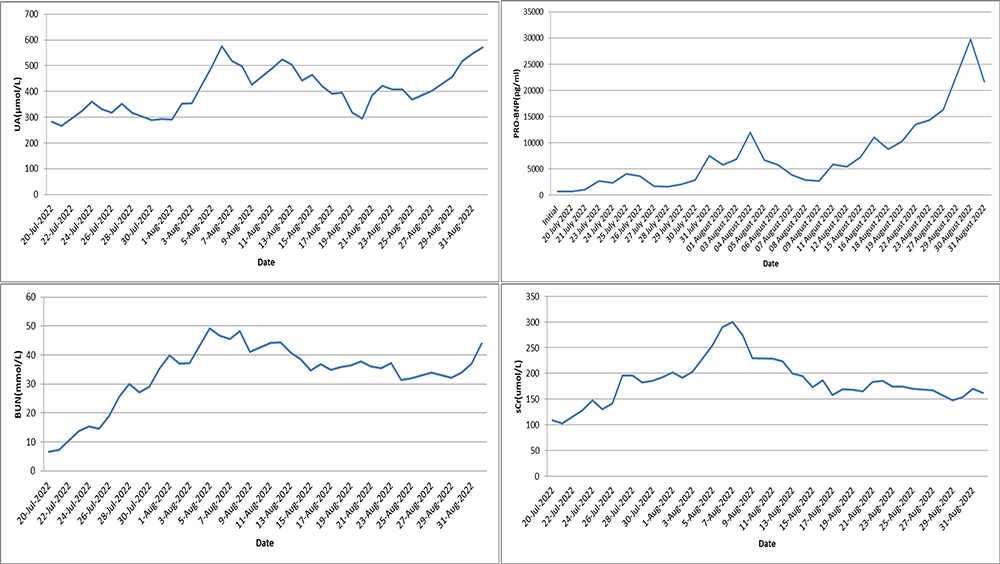 |
Figure 2 Changes in urea nitrogen, creatinine, uric acid, and the amino-terminal precursor of brain natriuretic peptide (NT proBNP) during the course of the disease. The figure shows a progressive increase in urea nitrogen, creativity, uric acid, and the amino terminal precursor of brain natural peptide (NT proBNP) of the patient over time. |
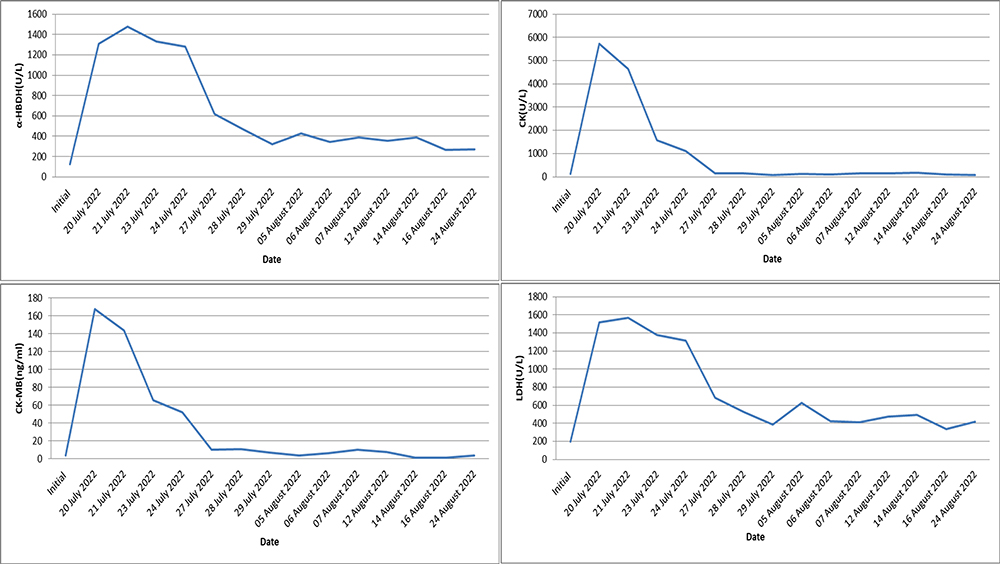 |
Figure 3 Changes in Creatine kinase (CK), creatine Isozyme (CK mb), Lactate dehydrogenase (LDH), lactate dehydrogenase Isozyme (LDH1, LDH2), a-hydroxybutyrate dehydrogenase (a-hbdh). The figure shows a significant increase in relevant indicators in the early stages of the patient’s onset. After 3 days of high-dose corticosteroids therapy, it quickly decreased and maintained at a lower level. |
 |
Figure 4 Changes in Glutamic pyruvic transaminase (ALT), glutamic oxaloacetic transaminase (AST), Myoglobin (Myo), cardiac troponin T (cTnT). The figure shows a significant increase in relevant indicators in the early stages of the patient’s onset. After 3 days of high-dose corticosteroids therapy, it quickly decreased and maintained at a lower level. |
Discussion
Since the FDA-approved PD-1/PD-L1 antibody drugs for urothelial carcinoma in 2016, an increasing number of PD-1/PD-L1 antibody drugs have been approved for urothelial carcinoma indications. Immune checkpoint inhibitors (ICIs) have drastically altered the treatment landscape and prognosis of many cancers.7 However, Immune-related adverse events, particularly severe toxicities such as myocarditis, are major challenges to the use of immune checkpoint inhibitors (ICI) in anticancer therapy. The pathogenesis of ICI myocarditis is poorly understood.8 PD-1/PD-L1 inhibitors associated with myocarditis are rare and fatal. Multiple clinical studies have shown that PD-1/PD-L1 inhibitor-related myocarditis is relatively rare.9 The incidence of anti PD-1/PDL1 treatment-related myocarditis was only 0.41%. However, after combined use of a CTLA4 inhibitor, the incidence of myocarditis doubled to 1.33%.10 Biomarkers such as BNP or troponin T/I, electrocardiograms, and MCR can help diagnose immune myocarditis. The infiltration of T lymphocytes was found to be the foundation of the myocarditis phenotype via the exploration of possible pathogenesis at the histological, cellular, and molecular transcriptional levels. The macrophage-mediated immune response and the synergistic effect of PD-1/CTLA4 may act as a catalyst in this process. The core treatment method for PD-1/PD-L1 inhibitor-associated myocarditis is to inhibit overactivated T lymphocytes, and corticosteroids are the first-line immunosuppressants.11
The case reported in this article is that of an elderly female patient with bladder cancer. The patient could not tolerate systemic chemotherapy. In the absence of better treatment options, patients and their families urgently require immunotherapy to control tumor progression. The patient had no clear history of immune-related diseases, regardless of personal or family history. After approximately seven weeks of treatment with the PD-1 antibody tislelizumab, she experienced significant dizziness, chest tightness, fatigue, and blurred vision. ECG showed tachycardia, a complete right bundle branch block, and an abnormal ST-T segment (Figure 1). Laboratory test results showed glutamate pyruvate transaminase 403 (U/L), glutamate oxaloacetate transaminase 787 (U/L), lactate dehydrogenase 1518 (U/L), α-hydroxybutyrate 1310 (U/L), creatinine 109 (µmol/L), Myoglobin>4104.00 (ng/mL), cardiac troponin T 5.16 (ng/mL), and N-terminal B-type natriuretic peptide precursor 712.30 (pg/mL). Myocardial magnetic resonance (CMR) is a noninvasive gold standard for diagnosing myocarditis, using techniques such as tissue features T1 weighted imaging and T2 weighted imaging, along with gadolinium-enhanced imaging, to detect myocardial edema, inflammation, and fibrosis. The criteria used in CMR for the diagnosis of myocarditis are myocardial edema, hyperemia or capillary leak (early gadolinium enhancement), irreversible injury (necrosis, scar, late gadolinium enhancement), regional or global systolic or diastolic dysfunction, with or without LV dilatation, increased wall thickness, pericardial effusion, intracavitary thrombi.12 However, its sensitivity for diagnosing ICI-related myocarditis is low.13 Endocardial biopsy (EMB) remains the gold standard for diagnosing myocarditis.14 Unfortunately, considering the patient’s critical condition, they cannot complete CMR and cannot tolerate EMB. However, based on her clinical data, we diagnosed with ICI-related myocarditis.
Patients with ICI-related myocarditis have high mortality rates. Therefore, early detection is crucial before severe cardiotoxic effects and life-threatening complications are induced by ICIs. Currently recognized monitoring indicators include baseline cardiac function, clinical history, risk factors, electrocardiogram, troponin, NT proBNP, and echocardiography.15 For early treatment, the Society for Cancer Immunotherapy (SITC) has issued the latest clinical practice guidelines for management. The incidence rate of ICI-related myocarditis shows that high doses of corticosteroids (intravenous injection of methylprednisolone 1 g/day or the same dose, lasting for 3–5 days, steroids should be used until the symptoms improve and biomarker normalized) should be administered to patients with suspected ICIs induced myocarditis. Once the diagnosis results are taken into consideration, myocarditis should be treated as soon as possible, and for the following 4–6 weeks, 1–2 mg/kg prednisone was reduced in dosage.16 Figures 3–4 shows the changes in serum myocardial markers of the patients during hospitalization. After three days of high-dose methylprednisolone pulse therapy, myocardial injury markers, such as creatine kinase (CK), creatine isozyme (CK mb), lactate dehydrogenase (LDH), lactate dehydrogenase isozyme (LDH1, LDH2), α-hydroxybutyrate dehydrogenase (a-hbdh), and myocardial Troponin T (cTnT), were significantly decreased (Figures 3 and 4).
Despite the rapid decline in patient-related monitoring indicators after active early treatment, our patient still had poor prognosis. From the graph, we can see that the series of myocardial enzyme spectrum indicators was maintained at a low level after decreasing. However, urea nitrogen, creatinine, uric acid, and the amino-terminal precursor of brain natriuretic peptide (NT-proBNP) levels continued to increase. Previous studies have shown that sacubitril/valsartan (an angiotensin receptor neoplasia inhibitor) improves cardiovascular risk, sudden death, or reduced ejection fraction (HFrEF) in heart failure.17 Therefore, we simultaneously administered sacubitril/valsartan. Unfortunately, the patient’s condition did not improve. The European Society of Oncologists (ESMO) recommends adding another immunosuppressive drug (mycophenolate mofetil or tacrolimus) when the condition worsens further.18 A multicenter registration report found that early high-dose hormone therapy was more effective in patients. A combination of mycophenolate mofetil, tacrolimus, infliximab, and anti-thymocyte globulin with steroids can alleviate these symptoms. After the addition of tacrolimus, the patient’s condition seemed to have improved to some extent (from August 5th to August 7th in Figure 4), but soon returned to a deteriorating trend. Accompanied by severe myasthenia gravis and multiple drug-resistant bacterial infections in both lungs, tracheal intubation and mechanical ventilation should be maintained. Multiple attempts to detach the patient from the ventilator failed, and the patient ultimately died of immune checkpoint inhibitor-associated myasthenia gravis, immune checkpoint inhibitor-associated myocarditis, and multiple organ failure.
Conclusion
The emergence of immune checkpoint inhibitor therapy offers renewed hope for patients suffering from urothelial carcinoma, particularly those whose tumors have progressed to advanced stages. However, clinicians must be mindful of the immune-related side effects that immune checkpoint inhibitors may induce when administering immunotherapy, including the rare but life-threatening conditions of myocarditis and myasthenia gravis. Although the mechanism of ICI-related cardiac toxicity has not yet been fully elucidated, physicians treating patients with ICIs should be vigilant of potential fatal cardiac toxicity effects. Considering that ICI-related myocarditis does not have specific clinical manifestations, myocardial biopsy and cardiac magnetic resonance imaging are difficult to perform in critically ill patients. Therefore, early diagnosis, appropriate prevention, and treatment based on clinical data are crucial. The pulse dose of methylprednisolone (1 g/day, lasting 3–5 days) is helpful for early control of the condition. When the condition worsened further, adding another immunosuppressive drug (mycophenolate mofetil or tacrolimus) improved the condition. Currently, there is no guiding treatment for myasthenia gravis caused by PD-1 treatment. Thus, clinicians should pay attention to myasthenia gravis caused by ICIs while also paying attention to immune-related myocarditis. We look forward to more research and treatment of fatal immune myocarditis and myasthenia gravis caused by anti-PD-1 treatment.
Ethical Statement and Consent to Participate
The publication of this case report obtained the verbal informed consent of the patient’s daughter, which was witnessed by a member of the research team and documented accordingly. The report excludes potential identifiers for patients. The institutional approval was not required to publish the case details.
Acknowledgments
We are incredibly appreciative to the patient’s daughter for enabling us to present the case.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
2. Soria F, Shariat SF, Lerner SP, et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J Urol. 2017;35(3):379–387. doi:10.1007/s00345-016-1928-x
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. Meeks J, Black P, Galsky M, et al. Checkpoint inhibitors in urothelial carcinoma-future directions and biomarker selection. Europ Urol. 2023;84(5):473–483. doi:10.1016/j.eururo.2023.05.011
5. Moslehi J, Salem J, Sosman J, et al. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet. 2018;391(10124):933. doi:10.1016/S0140-6736(18)30533-6
6. Bonaca M, Olenchock B, Salem J, et al. Myocarditis in the setting of cancer therapeutics: proposed case definitions for emerging clinical syndromes in cardio-oncology. Circulation. 2019;140(1):80–91. doi:10.1161/CIRCULATIONAHA.118.034497
7. Wang D, Salem J, Cohen J, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4(12):1721–1728. doi:10.1001/jamaoncol.2018.3923
8. Axelrod M, Meijers W, Screever E, et al. T cells specific for α-myosin drive immunotherapy-related myocarditis. Nature. 2022;611(7937):818–826. doi:10.1038/s41586-022-05432-3
9. Dong H, Qi Y, Kong X, et al. PD-1/PD-L1 inhibitor-associated myocarditis: epidemiology, characteristics, diagnosis, treatment, and potential mechanism. Front Pharmacol. 2022;13:835510. doi:10.3389/fphar.2022.835510
10. Salem J, Manouchehri A, Moey M, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018;19(12):1579–1589. doi:10.1016/S1470-2045(18)30608-9
11. Liang S, Yang J, Lin Y, et al. Immune myocarditis overlapping with myasthenia gravis due to anti-PD-1 treatment for a chordoma patient: a case report and literature review. Front Immunol. 2021;12:682262. doi:10.3389/fimmu.2021.682262
12. Ferreira V, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol. 2018;72(24):3158–3176. doi:10.1016/j.jacc.2018.09.072
13. Zhang L, Awadalla M, Mahmood S, et al. Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis. Eur Heart J. 2020;41(18):1733–1743. doi:10.1093/eurheartj/ehaa051
14. Ji C, Roy M, Golas J, et al. Myocarditis in cynomolgus monkeys following treatment with immune checkpoint inhibitors. Clin Cancer Res. 2019;25(15):4735–4748. doi:10.1158/1078-0432.CCR-18-4083
15. Ganatra S, Neilan T. Immune checkpoint inhibitor-associated myocarditis. Oncologist. 2018;23(8):879–886. doi:10.1634/theoncologist.2018-0130
16. Thompson J, Schneider B, Brahmer J, et al. Management of immunotherapy-related toxicities, version 1.2022, NCCN clinical practice guidelines in oncology. J National Compr Cancer Network. 2022;20(4):387–405. doi:10.6004/jnccn.2022.0020
17. Liu Z, Fan Y, Guo J, et al. Fulminant myocarditis caused by immune checkpoint inhibitor: a case report and possible treatment inspiration. ESC Heart Fail. 2022;9(3):2020–2026. doi:10.1002/ehf2.13912
18. Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann Oncol. 2020;31(2):171–190. doi:10.1016/j.annonc.2019.10.023
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.