")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Leisure Attitude, Self-Rated Health, and Psychological Well-Being in Older Adults: A Moderated Mediation Model
Authors Rodríguez-Cifuentes F , López-Gonzalez MA , Rubio-Garay F, Topa G , Belo P , Pocinho R, Silva S, Fernández-Muñoz JJ
Received 5 December 2023
Accepted for publication 22 March 2024
Published 29 March 2024 Volume 2024:17 Pages 1417—1431
DOI https://doi.org/10.2147/PRBM.S453396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Francisco Rodríguez-Cifuentes,1,* M Angeles López-Gonzalez,1,* Fernando Rubio-Garay,2,* Gabriela Topa,3,* Pedro Belo,4,* Ricardo Pocinho,5,* Silvia Silva,6,* Juan José Fernández-Muñoz1,*
1Psychology Department, Faculty of Health Sciences, Universidad Rey Juan Carlos, Alcorcón, Madrid, Spain; 2Associated Center in Albacete, Universidad Nacional de Educación a Distancia, Albacete, Spain; 3Department of Social and Organizational Psychology, Faculty of Psychology, Universidad Nacional de Educación a Distancia, Madrid, Spain; 4Instituto Politécnico de Setúbal, Setúbal, Portugal; 5Instituto Politécnico de Leira- CICS NOVA, Leira, Portugal; 6Escola Superior de Educação e Ciências Sociais Instituto Politécnico de Leiria, Leiria, Portugal
*These authors contributed equally to this work
Correspondence: M Angeles López-Gonzalez, Psychology Department, Faculty of Health Sciences, Universidad Rey Juan Carlos, Av. de Atenas, s/n, Alcorcón, Madrid, 28922, Spain, Email [email protected]
Purpose: A positive leisure attitude among older adults may have a beneficial effect on psychological well-being, both directly and indirectly by fostering a more positive perception of one’s health. This paper presents a correlational design that explores associations among leisure attitude, self-rated health, and psychological well-being, and analyzes the potential moderating role of gender in these relationships.
Patients and Methods: The sample was selected using simple random probability sampling (N= 409; 61.9% female; Mean age = 72.9; SD = 8.43¸ Range of age 53 to 93 years). Diverse sociodemographic information was collected, and leisure attitudes, self-perceived health, and psychological well-being (positive affect and emotional ties) were assessed.
Results: The results revealed a positive effect of leisure attitude on self-rated health and psychological well-being, with self-rated health fully mediating the association between the behavioral component of leisure attitude and psychological well-being. Furthermore, the moderating effect of gender on the relationship between self-rated health and psychological well-being was stronger among men.
Conclusion: Positive cognitive and emotional perceptions of leisure among older adults seem to benefit psychological well-being and improve self-rated health, thereby contributing to healthy ageing.
Keywords: ageing, older adults, gender, attitudes to leisure, psychological well-being, emotional ties
Introduction
As a result of increased life expectancy and lower birth rates, the number of Older Adult People (OAPs) in the world has risen significantly in recent years.1 So much so, in fact, that by 2030, the number of people aged 60 years and over is expected to reach 1.4 billion (400 million more than in 2020), and by 2050, this figure is expected to rise to 2.1 billion.2 These estimates about the elderly may vary depending on the age taken as a reference. Although 65 years of age has traditionally been considered the threshold for older age, some academic works include people over 50 in this group (e.g).3,4 This type of categorization is consistent with initiatives such as SAGE,5 promoted by the WHO, or COURAGE,6 carried out by the EU. These projects are large-scale aging research; SAGE collects representative samples from China, Ghana, India, Mexico, Russian Federation and South Africa. COURAGE tries to replicate the work but at a European level.
Thanks to this type of work, it is possible to affirm that ageing is a natural, gradual, continuous process inherent to all human beings, although individual characteristics and the environment both play a key role in its evolution. In addition to the biological changes associated with the passage of time, many other changes occur also in the field of social relationships. It is therefore essential for OAPs to be able to maintain their functional capacities. In this framework, society should adopt a view of ageing that moves away from stereotypical representations of disease and the negative perceptions commonly associated with older people. In this regard, the WHO7 understands active ageing as “the process of optimizing opportunities for health, participation and security in order to improve the quality of life of people as they age” (p. 5). It conceives healthy ageing as “the process of promoting and maintaining the functional capacity that enables well-being in old age” (p. 30). Promoting quality of life and maintaining functional capacity are therefore crucial elements in active and healthy ageing.8
Active ageing is a current paradigm that aims to foster an alternative approach to old age. According to this perspective, actions that promote people’s autonomy, creativity, freedom and good ageing practices are of particular importance.9 In this sense, active and healthy ageing is much more than the absence of disease since the focus is on maintaining functional capacities. Moreover, this understanding of the ageing process is based on three primary pillars: active participation, health, and safety.10 Thus, the aim is for older people to be able to continue engaging in and experiencing the activities they value most, including leisure and free time activities.
Leisure and a Positive Leisure Attitude
OAPs’ acceptance of ageing has changed in recent years. It is now generally accepted that individuals should deal with the process of growing older in a participatory and proactive way, avoiding disconnection or isolation from society. There are many ways in which OAPs can participate, although programs for the elderly tend to focus primarily on engagement in actions in which they play an active role. These activities include social participation (such as involvement in charitable associations or thematic interest groups), animal-assisted interventions, enrollment in friendship clubs, leisure activities and skills development, among others (see Gardiner et al).11 In this sense, Ragheb and Beard12 argue that attitude towards leisure activities may be one of the fundamental elements determining individuals’ willingness to participate in such pursuits, with a positive leisure attitude reflecting OAPs’ ability to maintain an active lifestyle.13
The role of leisure varies from person to person, depending on the beliefs and strategies associated with it. According to Iwasaki et al14 these may include empowerment (leisure as a means of developing resources for coping with life’s challenges), mood enhancement (increasing positive and decreasing negative affect) and palliative coping (a respite from stress which enables the individual to cope better with said stress). Regardless of its intended purpose, however, leisure appears to have potential effects on both short-term well-being (eg, stress reduction) and long-term health. Thus, leisure activities can help individuals strike a positive balance in different aspects of their lives.15
To achieve a good balance between different areas of life, attention must be paid to personal, interpersonal, and collective needs. The way in which OAPs experience and approach leisure will determine whether these needs are met.16 For example, a lifestyle in which leisure time involves some kind of physical activity will help promote health and have a positive impact on quality of life.17,18 Moreover, its consequences are particularly relevant among retired people, who have more leisure time available than other groups, such as working parents, for example.16 However, the development of leisure attitude is influenced by both context and previous individual experience, through which people acquire affective feelings and beliefs associated with leisure.19 It is not, therefore, a static attitude, but rather a dynamic one that may change over the years, in accordance with the individual’s knowledge, health, thoughts and concept of life.20,21
Relationship Between Leisure, Health, and Gender
Previous research (e.g)22 has shown that leisure may play a key role in improving long-term psychological well-being. In general, greater participation in leisure activities during old age is associated with better health status.22–25 In this regard, a study with a large sample of older Chinese adults (N = 7689), Zhao et al26 showed that older individuals who engage more frequently and in a greater number of leisure activities are more likely to experience successful aging. However, OAPs’ health impairments may influence their leisure activity choices and attitudes toward leisure.27 In addition to health impairment-related constraints, leisure opportunities may also be impacted by other variables, such as the environment in which the individual lives, particularly in the case of dependent people in rural areas.28 Participation in leisure activities has been found to be effective in improving depressed mood and increasing psychological well-being,16 and it has also been shown that general life satisfaction is related to life outlook and health status, which in turn determine participation in activities.29
However, the relationship between leisure and health may be even more complex since gender may act as a moderating factor between different health-related variables. For example, Gouveia et al30 found that gender moderated the relationship between physical activity and health, with engagement in leisure-time physical activity being a good predictor of quality of life among men who enjoyed better health. Moreover, higher levels of health among men were found also when subjective measures were used. Indeed, among older age groups, being male has been related to higher levels of happiness,31 life satisfaction,32 and subjective health.33 Moreover, this poorer perception of physical and psychological health among women does not seem to depend on any other relevant variables, such as the number of chronic pathologies or the number of prescription drugs taken.34
In addition to influencing aspects linked to OAPs’ health, gender also seems to influence their participation in leisure activities. Paillard-Borg et al35 identified a series of factors associated with lower involvement, which included having a mental disorder, having some kind of physical limitation, being a woman or having a restricted social network. In this sense, differences have been observed between men and women in terms of the type and form of their involvement in leisure activities.36,37 Numerous studies have reported that women spend less time on leisure and only spend more time than men on activities related to caregiving and unpaid work in the home.38–41 These gender differences become more apparent as age increases in cultural conditions in which the gender gap is more evident, such as in southern European countries (see,42,43 for example). The greater responsibilities socially assigned to women in these countries result in a lack of time for personal care and a greater risk of loneliness, which can lead to social exclusion. According to data from the Organization for Economic Cooperation and Development,44 Portugal is one of the countries with the largest gender gaps in terms of leisure time (289 hours enjoyed per year by men, compared to 200 hours for women) and unpaid work (96 hours spent on these tasks by men, compared to 328 hours by women), which includes caregiving.
Psychological Well-Being
Traditionally, psychology has viewed mental health from the perspective of the biomedical model, focusing on pathology and impairment levels as fundamental elements in OAPs.45,46 This has resulted in the positive aspects of mental health, such as satisfaction, joy, happiness, pleasure in living, optimism, and psychological well-being, being neglected. However, psychological well-being is a key aspect in OAPs’ personal development.47 It can contribute greatly to the accuracy of mental health measures, beyond symptoms of psychological distress.48 It is widely accepted that mental health in OAPs seems to pivot on two principal dimensions: psychological distress and psychological well-being.45,48 The positive dimension of mental health, ie, psychological well-being, has been conceptualized in different ways. According to Ryff,49,50 it is a multidimensional construct associated with self-acceptance and autonomy, positive relationships with others, mastery of the environment, personal growth and having a purpose in life. For their part, Veit and Ware48 conceive psychological well-being in terms of two dimensions: positive affect and emotional ties. Positive affect comprises positive emotions and moods, such as feeling happy, satisfied, relaxed, in a good mood, cheerful, optimistic, at peace or hopeful about the future. The emotional ties dimension refers to emotional bonding with other people, or in other words, feeling loved and wanted, having good affective relationships, and not feeling lonely or isolated.
The relationship between psychological well-being and various psychosocial variables in the ageing process has been a key issue in the scientific literature in recent years. Psychological well-being has been associated with intrapersonal variables (eg, self-esteem, self-efficacy, autonomy, self-rated health, attachment style, life satisfaction, etc.), situational variables (eg, perceived social or family support, participation in social activities, attitudes, etc.), and sociodemographic factors such as age, gender, marital status, education level, place of origin, and place of residence, among others.22,46,47,50–55
Justification, Hypotheses, and Objectives
As we have seen, the extant scientific literature has demonstrated the relationship that exists between OAPs’ participation in leisure activities and better health. However, research in this field is much more limited when we talk about the relationship between attitudes towards leisure in the elderly in their cognitive and affective dimensions and better health and well-being, as studies have typically focused more on participation in leisure activities (ie, the behavioral dimension of attitude). Moreover, a positive leisure attitude does not always translate into associated behaviors (ie, participation in leisure activities). For example, institutionalized individuals may have a positive attitude towards this type of activity, but if they are constrained by some kind of physical limitation, they will not be able to benefit from its effects. Furthermore, previous studies have shown that gender is a factor that should be taken into consideration when analyzing participation in leisure activities and the perception of subjective health, life satisfaction and psychological well-being. Likewise, the potential moderating effect of gender on the relationships between all these variables, and particularly between participation and involvement in leisure activities and psychological well-being, should not be overlooked. Moreover, this gender effect may be linked to or influenced by other sociocultural factors, such as the distribution of responsibilities in the care of family members and other issues related to the performance of roles. Considering the above, the present study has two main aims: (a) to analyze the relationships between Leisure Attitude, Gender, subjective perception of general health status (Self-rated Health) and Psychological Well-being; and (b) to explore whether Self-rated Health mediates between Leisure Attitude and Psychological Well-being. Based on these two aims, the following hypotheses are proposed:
H1: Leisure Attitude will have a positive effect on Psychological Well-being. H2: The relationship between Leisure Attitude and Psychological Well-being will be mediated by Self-rated Health.
Specifically, we expect to find positive associations between these variables; in other words, we expect a more positive Leisure Attitude to be linked to better Self-rated Health, which in turn will be associated with higher levels of Psychological Well-being.
H3: Gender will moderate these relationships; specifically: H3A: Gender will moderate the effect of Leisure Attitude on Psychological Well-being. H3B: Gender will moderate the effect of Self-rated Health on Psychological Well-being.
Moreover, we expect the magnitude of the associations hypothesized in H1 and H2 to differ in accordance with gender, being greater among men than among women.
Material and Methods
Participants
The sample comprised 409 Portuguese adults, 253 women (61.9%) and 156 men (38.1%), aged between 53 and 93 years, with a mean age of 72.9 years (SD = 8.43). In terms of marital status, most were married (n = 191; 46.7%) or widowed (n = 144; 35.2%), and in relation to place of origin, 52.6% lived in rural areas and the remaining 47.4% lived in urban areas. Most lived in their own homes (88.6%), and only 11.4% lived in institutionalized facilities. Concerning education level, 164 (40.1%) participants had primary school qualifications, 66 (16.1%) had not completed any educational level, and 70 (17.1%) had higher-level qualifications.
Instruments
Sociodemographic Questionnaire
An ad hoc questionnaire was constructed to collect sociodemographic information about age, gender, education level, marital status, area of residence (urban/rural) and whether participants were in a situation of dependency (yes/no).
Leisure Attitude
Leisure attitude was assessed using the Portuguese adaptation56 of the Leisure Attitude Scale (LAS).12 This instrument is a self-report scale comprising 36 items divided into three 12-item subscales, which evaluate attitude in accordance with three dimensions: cognitive, affective, and behavioral. The cognitive component assesses general knowledge about leisure and beliefs about the relationship between leisure and health, happiness, and the personal benefits of engaging in leisure activities (eg, “Engaging in leisure activities is a wise use of time”). The affective component assesses respondents’ experiences, feelings, and pleasure with respect to leisure (eg, “My leisure activities give me pleasure”). Finally, the behavioral component assesses intention to participate in leisure activities, ie, planning and actions, and past, present, and future experiences with leisure (eg, “I do leisure activities frequently”).
In the present study, the overall reliability of the scale (α = 0.98) and the individual values obtained for the cognitive (α = 0.97), affective (α = 0.98) and behavioral (α = 0.94) subscales exceeded both the overall internal consistency values obtained for the Portuguese adaptation of the instrument (α = 0.91), and the individual values obtained for each of its subscales: cognitive (α = 0.86), affective (α = 0.86) and behavioral (α = 0.79).
Self-Rated Health
Self-rated health was assessed using the Self-rated Health Scale57 a simple measure of General Health in older adults. Maddox found 65% congruence between instrument scores and medical health assessments. The instrument assesses respondents’ subjective perception of their general health status through a single question. A subsequent adaptation was carried out by the WHO58 to homogenize data collection and health objectives across Europe. The new version accepts five response options: 1: “excellent”, 2: “good”, 3: “neither good nor bad”, 4: “bad”, and 5: “very bad”. In the present study, the measures were inverted to facilitate interpretation, with a score of 1 indicating “very bad” and a score of 5 indicating “excellent”. The instrument has been shown to be a sensitive predictor of mortality, with those reporting “bad” or ‘very bad’ health being twice as likely to die (from any cause) than those reporting “excellent” health.59
Psychological Well-Being
Psychological Well-being was assessed using the Mental Health Inventory (MHI-38),48 an instrument that evaluates Mental Health, of which there is a Portuguese adaptation validated by Ribeiro.45 The inventory comprises 38 items rated on a 5- or 6-point Likert-type scale and assesses Psychological Distress and Psychological Well-being. In the present study, only the two subscales that evaluate participants’ Psychological Well-being were considered: Positive Affect (11 items, eg, “future hopeful”) and Emotional Ties (3 items, eg, “felt loved and wanted”). The overall Psychological Well-being score is calculated by summing the raw values of each subscale (after converting the scores corresponding to the reverse-scored items), with higher values indicating greater psychological well-being. The Portuguese adaptation of the instrument was found to have good reliability values: overall inventory α = 0.96; Psychological Well-being α = 0.91 [Positive Affect α = 0.91; Emotional Ties α = 0.72].45 Similar reliability values were obtained in the present study (Psychological Well-being α = 0.92; [Positive Affect α = 0.92; Emotional Ties α = 0.69]).
Procedure
After approval of the research proposal by the Bioethics Committee of the National University of Distance Education, several institutions in the Northern and Central Regions of Portugal were contacted by the research team to evaluate their interest in the present study. Their pertinent boards analyzed the ethical implications of the study and the possibility of participating in it. In this sense, directors of the institutions granted permission for data collection, however, they refused to allow their names to be published in the manuscript, citing confidentiality and anonymity concerns. In any case, those who approved their collaboration compromised to administer the questionnaire to their volunteer users and help with the data collection process. Those willing to participate signed a consent form. All participants were informed of the research aims before answering the questionnaire, and all were reminded that they could withdraw from the study at any time. The data were processed anonymously and were kept strictly confidential. The study complied with the ethical principles governing research involving humans, as enshrined in the Declaration of Helsinki (2013), regarding informed consent, confidentiality, and procedures.
The data were collected by two members of the research group, trained on psychological assessment in elderly to generate an adequate relationship of trust that would favor communication and create the initial rapport. In addition, a briefing was agreed with the rules about the questions and how to fill in the questionnaires according to the participants’ answers.
Questionnaires were administered in 25-minute face-to-face interviews. Members of the research team gave participants the instructions required to answer the questions and were available during interviews to resolve any doubts. Participants were told that there were no right or wrong answers and that we simply wanted to understand how they perceived things. As such, they were instructed to choose the most suitable response option for each item.
Design
The study followed an ex post facto prospective correlational design. The sample was selected using simple random probability sampling, with everyone having the same probability of being chosen.60
Data Analysis
Data were processed using the Statistical Package for Social Sciences software (IBM Corp., 2016), version 24. Statistical models were formulated using the PROCESS 4.2 macro, a computational tool developed by Hayes61 for analyzing mediation and moderation processes. This tool overcomes the limitations of the stepwise model developed by Baron and Kenny.62 A Bootstrap procedure (PROCESS assumes 5000 “resamples”) with a confidence level of 0.05 was used to assess unconditional indirect effects.61,63,64 In estimating the models, the variables used in the plot were mean centered to enable the regression coefficients to be easily perceived. First, the direction and magnitude of the relationships between the different variables were examined using Pearson’s R statistic. Second, a moderated mediation model was tested. Self-rated Health was considered the mediating variable in the relationship between Leisure Attitude (independent variable) and Psychological Well-being (dependent variable), with Gender as the moderating variable (see Figure 1). Finally, the same model was broken down into the different components of Leisure Attitudes and Psychological Well-being.
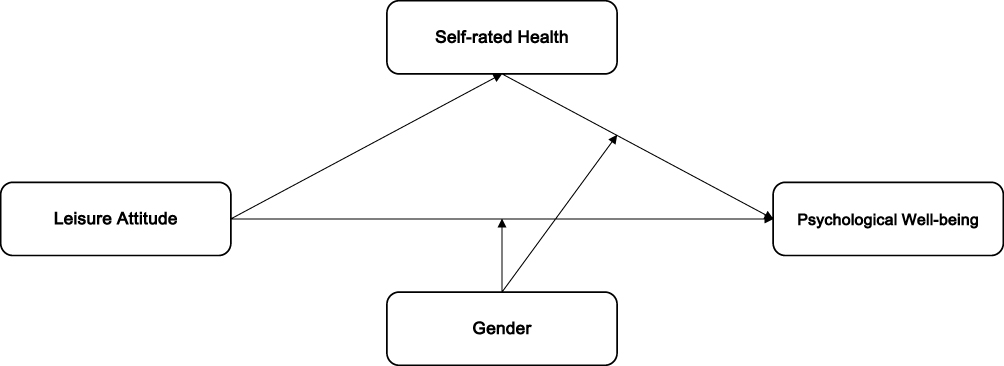 |
Figure 1 Conceptual diagram of the moderated mediation model under study. |
Results
The correlation analyses revealed positive and significant correlations between all the study variables. As shown in Table 1, the strongest correlations were observed between the internal scales of the different instruments; in other words, between the two subscales (Positive Affect and Emotional Ties) of the Psychological Well-being questionnaire and between the three components of the Leisure Attitudes Scale.
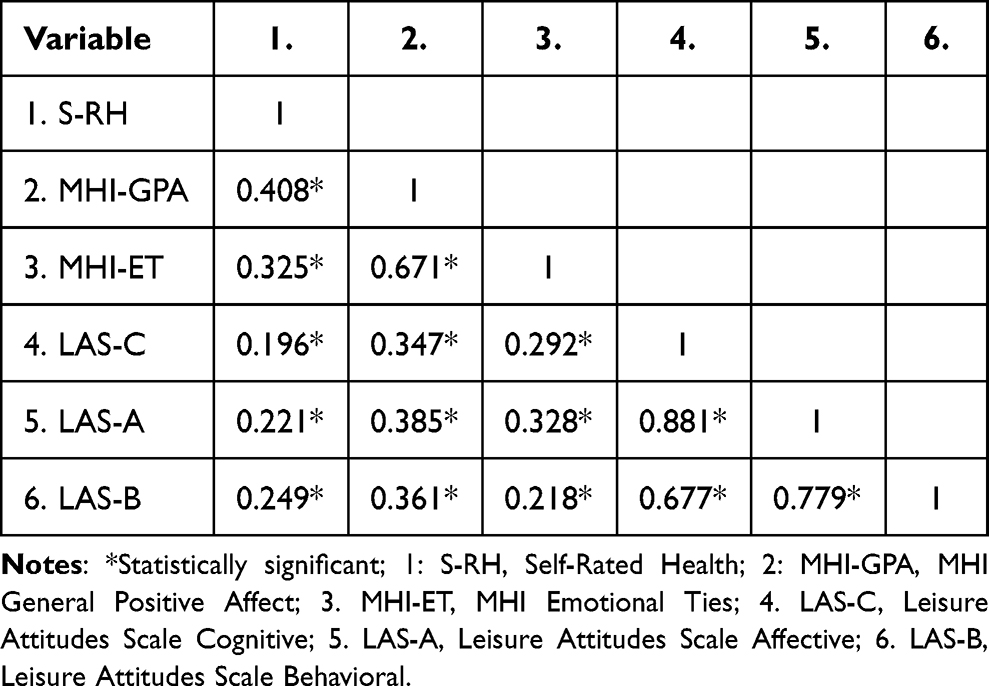 |
Table 1 Pearson’s Correlation Coefficients Between the Variables Under Study |
Table 2 presents the descriptive statistics for the independent (Leisure Attitude) and dependent (Psychological Well-being) variables included in the moderated mediation model. Regarding the mediating variable (Self-rated Health), when participants were asked how they would rate their health status, 43.8% (n = 179) answered “neither good nor bad”, and 40.3% (n = 165) answered “good”.
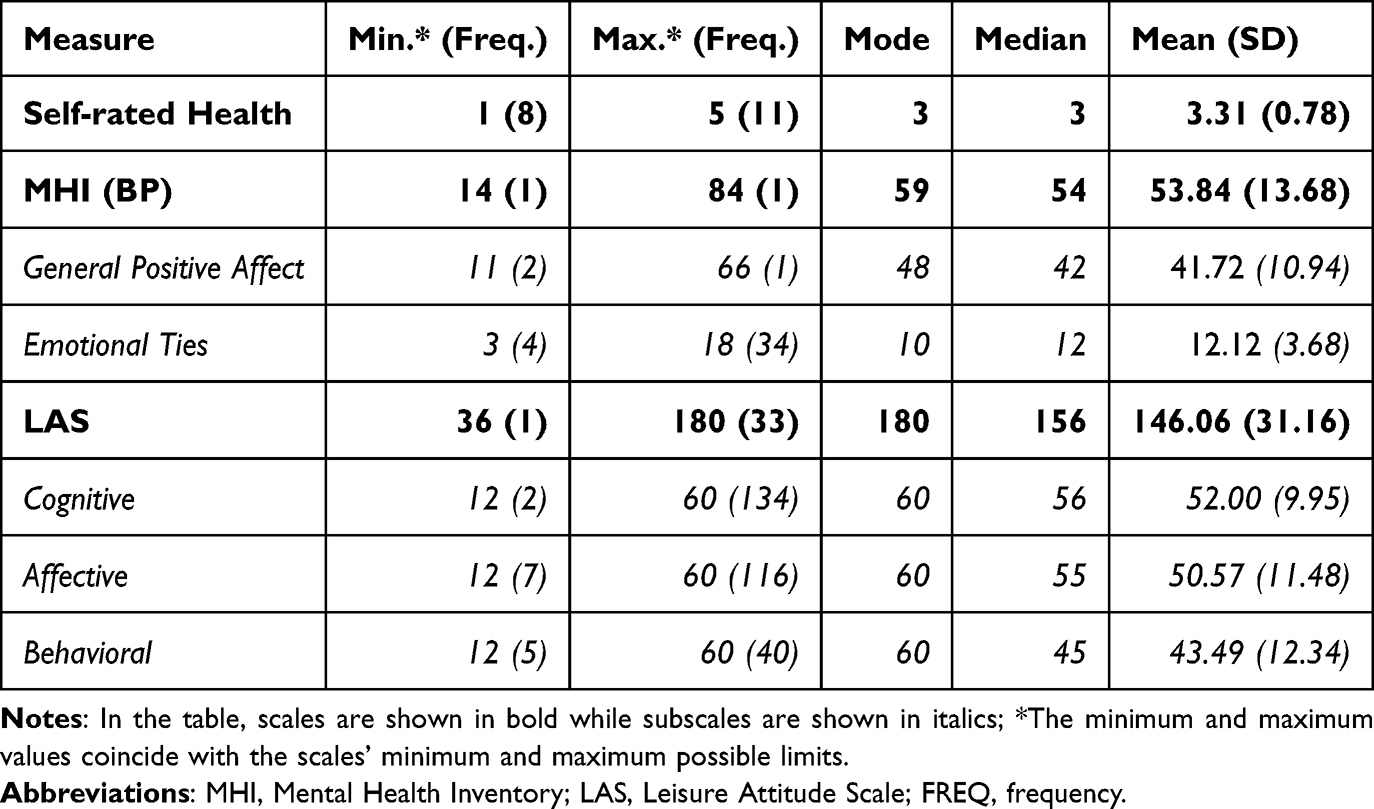 |
Table 2 Descriptive Statistics for Self-Rated Health, Psychological Well-Being, and Leisure Attitudes |
As shown in Table 2, the mean scores for the Leisure Attitude and Psychological Well-being variables were higher than the neutral points of the corresponding scales and subscales. The results obtained for Leisure Attitude were particularly noteworthy, since the maximum score was the most frequent response in all subscales. This finding suggests that, even though some of the older adults chose the lowest-scoring responses, most reported a positive Leisure Attitude and claimed to feel psychologically well.
Moderated Mediation Models
To analyze whether Self-rated Health explained the association between Leisure Attitude and Psychological Well-being, a moderated mediation model was tested using the PROCESS macro for SPSS,65 specifically model 15. This is a mediation model in which one variable moderates the relationship between the independent and dependent variables, as well as between the dependent and mediating variables. Leisure Attitude was found to explain 6% of the variance observed in Self-rated Health [F (1401) = 24.919, p < 0.001]. The global model with all variables explained 27.23% of the variance observed in Psychological Well-being [F (5397) = 29.708, p < 0.001].
The results of the model analyzed confirmed our second hypothesis (regarding mediation), revealing significant indirect effects in the case of both men = 0.0436, [0.022; 0.069] and women = 0.032, [0.015; 0.053]. However, they do not allow us to accept the third hypothesis regarding moderated mediation, in which gender was expected to play a moderating role (Moderated Mediation Index = −0.0121, [−0.034; 0.008]). The direct relationship observed between Leisure Attitudes and Psychological Well-being (0.144, [0.105; 0.183]) enables us to affirm that Self-rated Health only partially mediates this relationship (see Figure 2).
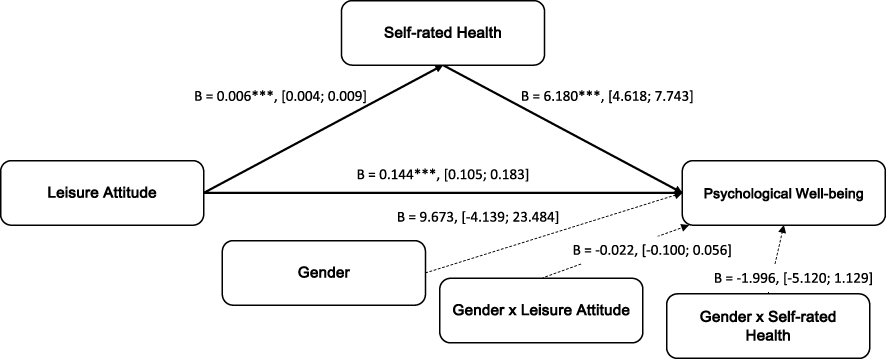 |
Figure 2 Moderated mediation analysis model: leisure attitude (independent variable), self-rated health (mediating variable), gender (moderating variable) and psychological well-being (dependent variable). Note: Statistically significant relationships are indicated with thicker lines. Significance levels: ***p < 0.001. |
Since the moderated mediation model analyzed failed to reveal any moderating effect of gender, we decided to explore other possible models, considering the potential interactions between gender and other variables. We therefore contemplated the three components of the Leisure Attitude Scale (cognitive, affective, and behavioral) and the Positive Affect and Emotional Ties subscales of Psychological Well-being separately; in total, six additional models were tested.
As shown in the Figure 3, not all the associations were significant, and differences were found in relation to the initial model. Two results were of relevance: (a) the lack of any direct relationship between the behavioral component of Leisure Attitude (ie, intention to engage in leisure activities) and Psychological Well-being measures; and (b) the moderating influence of Gender on elements linked to the Emotional Ties subscale.
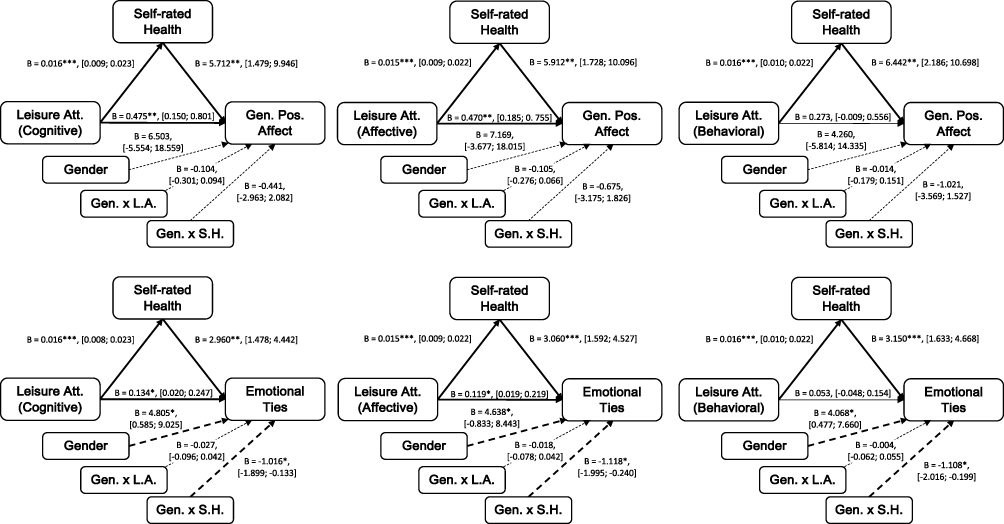 |
Figure 3 Moderated mediation analysis models with the different components of Leisure Attitude and the two Psychological Well-being subscales. Note: Statistically significant relationships are indicated with thicker lines. Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001. |
In relation to the first of these two findings, and as shown in Table 3, the behavioral component of Leisure Attitude was found to affect Psychological Well-being through Self-rated Health. It is important to note that the mediation in this case was full, whereas in the case of the other two components (cognitive and affective), the mediation was partial, since they were both found to have a direct effect also on the Psychological Well-being of older adults.
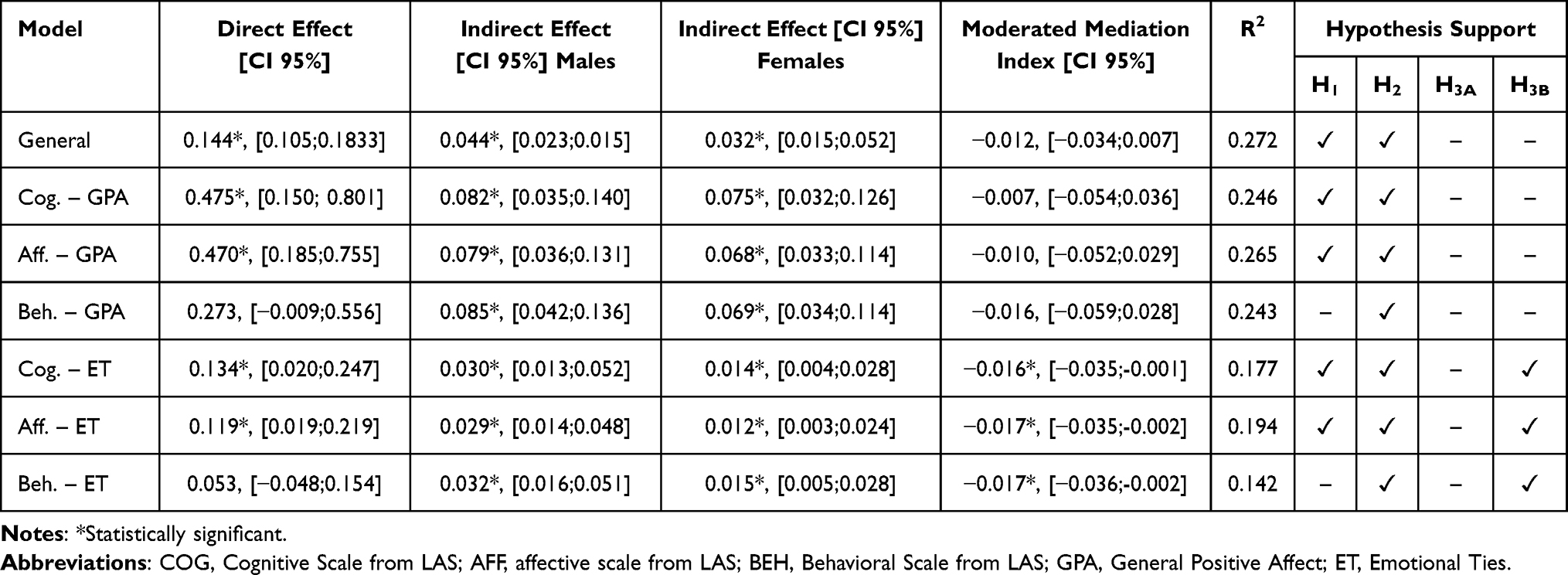 |
Table 3 Variation Explained by the Mediation and Moderated Mediation Effects in Each Model, and Support for Hypotheses |
Regarding the second differential aspect of these models, Gender was found to influence Psychological Well-being on a more social level. This enables us to accept the hypothesis of moderated mediation in those models in which Emotional Ties was taken as the dependent variable. Moreover, when the Positive Affect subscale was taken as the dependent variable, the relationship between the independent and mediating variables was stronger than in the case of the Emotional Ties subscale. These higher scores are reflected in the fact that, as shown in Table 3, the percentage of variance explained was greater in both the general model, which took Psychological Well-being as the dependent variable, and those that took Positive Affect as the dependent variable.
Considering the negative nature of the moderated mediation indices and the Gender values reported, we can affirm that the positive relationship between Self-rated Health and the Emotional Ties dimension of Psychological Well-being was stronger in the case of men.
By way of example, Figure 4 shows the influence of Gender on the values of the independent variable and the mediator in the model that took the cognitive component of Leisure Attitude as the dependent variable.
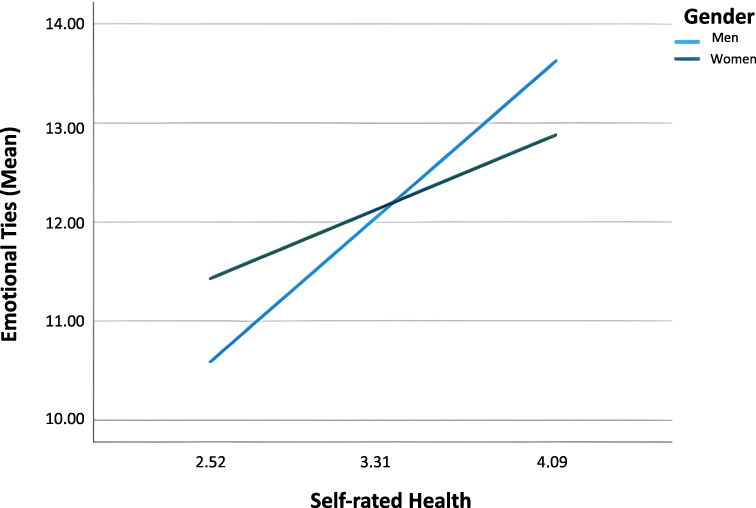 |
Figure 4 Moderating effect of gender on the relationship between Emotional Ties and Self-rated Health. |
As shown in Figure 4, women had higher baseline scores than men in the socio-affective dimension of Psychological Well-being. However, the magnitude of the mediating effect of Self-rated Health was lower.
Discussion
The present study aimed to explore the relationship between older adults’ attitude to leisure and their psychological well-being. To this end, we conceived leisure attitude as a three-dimensional structure (cognitive, affective, and behavioral), analyzing all three components in a differentiated manner.
Concerning the first hypothesis, the results confirm a positive relationship between leisure attitude and psychological well-being in OAPs. This is consistent with that reported extensively in the literature, within the framework of social psychology, and highlights the key role played by attitudes in many aspects of life. Specifically, the role of attitudes has been explored in terms of beliefs and opinions (cognitive component) and feelings of liking or disliking (affective component) towards the attitudinal object (e.g).66,67 However, the relationship between the behavioral component of attitude and the attitudinal object (in this case leisure) is not always significant. For example, in study with 80-year-old nursing home residents, the authors found a positive leisure attitude, except for the behavioral subscale measure.68 These same authors reported that, despite having a positive attitude to leisure, older people do not always engage in leisure activities because their physical limitations make it more difficult for them to acquire new routines. However, cognitive, and emotional perceptions seem to be of vital importance in OAPs’ leisure attitude. Indeed, remaining mentally active may be enough to ensure greater psychological well-being. However, although this interpretation would explain the relationship observed between the cognitive and emotional components of leisure attitude and psychological well-being, it does not explain the lack of a direct relationship between the behavioral component and this same outcome variable. It is therefore possible that other factors not contemplated in our study, such as physical or psychosocial limitations, may have influenced participants’ intention to engage in leisure activities. In sum, it seems likely that although many older adults have positive beliefs, opinions and thoughts regarding leisure, and leisure activities arouse feelings of pleasure and enjoyment, self-perceptions of functional and even financial limitations may diminish their tendency or intention to engage in these activities. It is also possible that other intrapersonal variables, such as self-efficacy expectations or personal beliefs in one’s abilities and skills,69,70 play an important role in leisure activities. In this regard, self-efficacy expectations are essential to the positive dimension of life and personal development.71 Indeed, self-efficacy to perform social activities has been found to have an impact on OAPs’ quality of life, with older adults who are more confident in their own abilities reporting a higher quality of life than those who manifest lower self-efficacy.72 Moreover, self-efficacy and other variables, such as self-esteem, for example, seem to function as promoters of physical, psychological, and social well-being in OAPs. Consequently, psychological well-being, rather than being associated with age, is more closely related to one’s perception of one’s health and autonomy, the practice of physical-sporting activities, self-esteem, and self-efficacy for ageing.47
Our second hypothesis, which concerns the mediating role of self-rated health in the relationship between leisure attitude and psychological well-being, was confirmed in all the models analyzed. This mediating role of health is not a novel result in the literature. The importance of self-rated health can be observed mainly in models that consider the behavioral component of leisure attitude, in which this variable fully mediates the relationship between attitude and psychological well-being.73,74 People’s subjective evaluation of their health status is a factor to which great importance has been attached in relation to well-being,75–78 with an older person’s self-assessment of their health being considered an important predictor of survival (e.g).79–81 Moreover, self-rated health constitutes one of the recommended health indicators for health monitoring.82 In this sense, Falk et al83 highlight the importance of using self-rated health as a simple measure to identify vulnerable populations worldwide, since the self-perception of poor health also increases the risk of suffering from mental illness.
Several studies (e.g)84–86 have shown that participation in leisure and free time activities contributes to a positive self-assessment of health. Older people who engage in leisure activities (eg, cultural, recreational, personal growth, physical exercise, etc.) perceive a better quality of life and greater mental well-being, thereby compensating for some of the physical and social deficits associated with their age.87,88
Third, we set out to analyze the potential moderating role of gender in the associations between leisure attitude, self-rated health, and psychological well-being. Our results reveal that, although gender does not seem to influence the relationship between leisure attitude and psychological well-being, it does moderate the relationship between self-rated health and this second variable. Specifically, the moderating effect was observed when the socio-affective dimension of psychological well-being (ie, emotional ties) was taken as the dependent variable; or in other words, when the outcome measured was whether the individual felt loved, was in a fulfilling romantic relationship or did not feel lonely. Our findings indicated that women had higher baseline scores on the emotional ties subscale than men. This may seem inconsistent with that reported by other studies, which have found that men generally have better levels of psychological well-being than women (e.g).89,90 However, our data do not actually contradict this idea, since men were observed to have higher levels of well-being, but only when they perceived themselves as healthy. In this sense, it is possible that men who report a better state of health feel more loved or express fewer feelings of loneliness than women, for whom “feeling loved” (or being emotionally attached to other people) is independent of their perceived state of health. The fact that men feel loved when their perception of health is high may to some extent be explained by traditional gender stereotypes and roles related to personal worth. Consequently, it is possible that men who perceive themselves as strong and healthy feel more loved and fear loneliness less. In contrast, when their health is compromised, men may undervalue themselves, no longer feel loved by their partner or close associates, and express greater emotional loneliness, which in turn generates psychological distress. In other words, men may experience increased feelings of vulnerability and hypervigilance in the face of environmental threats and eventually enter a loop in which their physiological functioning is also altered, and their risk of morbidity and mortality increases.52 Furthermore, these differences between men and women may also depend on other variables not contemplated in this study, such as emotional intelligence, in which construct much of the extant literature reports significantly higher scores among women.91 The higher scores obtained by women in terms of managing and understanding emotions92 may enable them to carry out a more realistic assessment of the emotional ties that bind them to their significant others. As a result, women may be better able to separate feelings of being supported and loved (ie, psychological well-being) from their subjective perception of health (ie, self-rated health). In contrast, men may have greater difficulty differentiating between the two: ”if I feel well, I feel that everything else is going well; if I feel bad, everything around me seems to be in a bad situation as well”.
The main limitation of the present study is linked to its design since it uses a correlational research methodology. Another important limitation derives from the limitations inherent to self-report measures in data collection. Future research would therefore do well to consider the importance of collecting data through in-depth interviews, since this would serve to strengthen the validity of the models proposed.
The literature provides us with a heterogeneous set of interrelated factors between attitudes towards leisure, self-rated health, and psychological well-being in OAPs. Future studies should therefore consider more complex models including personal variables and (eg, quality of life, autonomy, self-esteem, and self-efficacy), sociodemographic factors (eg, gender, education level, marital status, and support networks), which help to better understand the complex interrelationships that exist between all these elements. Moreover, we consider attachment style to be an underexplored aspect that should be taken into account in research on health, emotion regulation, and psychological well-being of OAPs. In this regard, previous studies have reported an association between insecure attachment, health problems and emotional distress. In contrast, secure attachment seems to be one of the most characteristic elements of well-being, so much so, that it can be considered an essential resource for resilience and social adjustment in old age.53
Conclusion
This study allows us to draw some conclusions. First, positive beliefs and opinions and feelings of pleasure towards leisure are related to greater psychological well-being in older people, furthermore, the importance of the mediating role of self-perceived health in this relationship is confirmed. Second, it is important to take how traditional gender roles can affect older people´s attitudes to leisure, so failing to take into account their personal needs and desires can contribute to perpetuating these gender roles. Third, the loss of social networks and loneliness, especially in the case of institutionalized individuals, are elements that can be very relevant in the attitudes towards leisure in OAPs. Finally, OAPs are agents in their own ageing; therefore, all programs and interventions should strive to provide them with training and to take advantage of the leadership that already exists in this population.93
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Organisation for Economic Cooperation and Development. Health at a Glance 2013: OECD Indicators. OECD Publishing; 2013.
2. World Health Organization. Ageing and Health. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
3. Mugisha JO, Edwards A, Naidoo N, Chatterji S, Seeley J, Kowal P. Longitudinal data resource from the Wellbeing of Older People cohort of people aged >50 years in Uganda and South Africa from 2009 to 2019. S Afr Med J. 2023;113(9):36–41. doi:10.7196/SAMJ.2023.v113i8.16706
4. Hermans H, Beekman AT, Evenhuis HM. Prevalence of depression and anxiety in older users of formal Dutch intellectual disability services. J Affect Disord. 2013;144(1–2):94–100. doi:10.1016/j.jad.2012.06.011
5. Organization WH. World Health Organization. WHO Study on global AGEing and adult health (SAGE). Available from: https://www.who.int/data/data-collection-tools/study-on-global-ageing-and-adult-health.
6. Service CRa DI. COURAGE in Europe - COllaborative Research on AGEing in Europe. COllaborative Research on AGEing in Europe. Available from: https://cordis.europa.eu/project/id/223071.
7. World Health Organization. World Report on Ageing and Health. World Health Organization; 2015.
8. Costa A, Câmara G, Arriaga MT, Nogueira P, Miguel JP. Active and healthy aging after COVID-19 pandemic in Portugal and other European countries: time to rethink strategies and foster action. Policy Brief Front Public Health. 2021;9:700279. doi:10.3389/fpubh.2021.700279
9. Cuenca-Amigo M, Del Valle Doistua RSS. La importancia del ocio como base para un envejecimiento activo y satisfactorio [The Importance of Leisure as a Basis for Active and Successful Ageing]. Rev Psicol Deporte. 2016;25(2):79–84.
10. López-Pulido A. La vejez como enfermedad: un tópico acuñado en la Antigüedad clásica [Old Age as a Disease: a Topic Closed in Classical Antiquity]. Gerokomos. 2018;29:156–159.
11. Gardiner C, Geldenhuys G, Gott M. Interventions to reduce social isolation and loneliness among older people: an integrative review. Health Soc Care Community. 2018;26(2):147–157. doi:10.1111/hsc.12367
12. Ragheb MG, Beard JG. Measuring Leisure Attitude. J Leisure Res. 1982;14(2):155–167. doi:10.1080/00222216.1982.11969512
13. Harahousou Y. Leisure and Aging. In: Rojek C, Shaw S, Veal A, editors. A Handbook of Leisure Studies. Palgrave McMillan; 2006.
14. Iwasaki Y, Mannell RC, Smale BJA, Butcher J. A short-term longitudinal analysis of leisure coping used by police and emergency response service workers. J Leisure Res. 2002;34(3):311–339. doi:10.1080/00222216.2002.11949974
15. Iwasaki Y, MacTavish J, MacKay K. Building on strengths and resilience: leisure as a stress survival strategy. Br J Guid Couns. 2005;33(1):81–100. doi:10.1080/03069880412331335894
16. Haworth J, Lewis S. Work, leisure and well-being. Br J Guid Couns. 2005;33(1):67–79. doi:10.1080/03069880412331335902
17. Lambrini K, Konstantinos K, Christos I, Areti T. Leisure activity in the third age. J Healthc Commun. 2018;3(1):1–3. doi:10.4172/2472-1654.100123
18. Winterbotham S, du Preez J. Psychosocial well-being in active older adults: a systematic review of qualitative literature. Int Rev Sport Exerc Psychol. 2015;9(1):96–115. doi:10.1080/1750984X.2015.1122075
19. Castro V, Carreira L. Leisure activities and attitude of institutionalized elderly people: a basis for nursing practice. Rev Latino-Am Enferm. 2015;23(2):307–314. doi:10.1590/0104-1169.3650.2556
20. Rodrigues A, Assmar E, Jablonski B. Atitudes: conceito, formação e mudança [Attitudes: concept, formation and change]. In: Rodrigues A, Assmar E, Jablonski B, editors. Psicol Soc. UNICAMP; 2007:97–146.
21. Silva L, Farias L, Oliveira T, Rabelo D. Atitude de idosos em relação à velhice e bem-estar psicológico [Attitude toward aging seniors and psychological well-being]. Rev Kairós Gerontol. 2012;15(2):119–140.
22. Chang PW, Lin L, Lin Y. Social relationships, leisure activity and health in older adults. Health Psychol. 2014;33(6):516–523. doi:10.1037/hea0000051
23. Carruthers C. The power of positive: leisure and well-being. Ther Recreat J. 2004;38(2):225–245.
24. Fave A, Bassi M, Boccaletti ES, Roncaglione C, Bernardelli G, Mari D. Promoting well-being in old age: the psychological benefits of two training programs of adapted physical activity. Frontiers in Psychology. 2018;9:828. doi:10.3389/fpsyg.2018.00828
25. Han NS, Won MH. Association between social support and physical activity in patients with coronary artery disease: multiple mediating roles of self-efficacy and autonomous motivation. Healthc. 2022;10(3):425. doi:10.3390/healthcare10030425
26. Zhao X, Yu J, Liu N. Relationship between specific leisure activities and successful aging among older adults. J Exerc Sci Fit. 2023;21(1):111–118. doi:10.1016/j.jesf.2022.11.006
27. Gagliardi C, Spazzafumo L, Papa R, Marcellini F. Changes in leisure styles and satisfaction of older people: a five years follow-up. Int J Aging Hum Dev. 2012;75(3):185–215. doi:10.2190/AG.75.3.a
28. Prieto-Bueno JM, Cantero-Garlito PA. Situación ocupacional y recursos sociales de las mujeres mayores en situación de dependencia atendidas por un servicio de ayuda a domicilio en el ámbito rural [Occupational situation and social resources of older women in a situation of dependency assisted by a home help service in rural areas]. Cad Bras Ter Ocup. 2020;28:950–966. doi:10.4322/2526-8910.ctoAO1974
29. Stolar GE, Macentee MI, Hill P. Seniors’ assessment of their health and life satisfaction: the case for contextual evaluation. Int J Aging Hum Dev. 1992;35(4):305–317. doi:10.2190/NEK7-5WGN-YEQU-N2CN
30. Gouveia BR, Ihle A, Kliegel M, Freitas DL, Gouveia ÉR. Sex differences in relation patterns between health-related quality of life of older adults and its correlates: a population-based cross-sectional study in Madeira, Portugal. Prim Health Care Res Dev. 2019;20e54. doi:10.1017/S1463423618000233
31. Martínez-Martínez AL, Bote Díaz M, Clemente Soler JA. Una aproximación a las emociones positivas generadas en las relaciones intergeneracionales: principales determinantes que inciden en la felicidad y bienestar de los mayores [An Approach to the Positive Emotions Generated in Intergenerational Relationships: main determinants that affect the happiness and well-being of the elderly]. Debates en Sociología. 2019;49:35–53.
32. Batz-Barbarich C, Tay L, Kuykendall L, Cheung HK. A meta-analysis of gender differences in subjective well-being: estimating effect sizes and associations with gender inequality. Psychol Sci. 2018;29(9):1491–1503. doi:10.1177/0956797618774796
33. Pérez-Fuentes MC, Molero MM, Mercader I, et al. Salud percibida y salud real: prevalencia en las personas mayores de 60 años [Perceived Health and Real Health: prevalence among Persons Aged 60 and Older]. Enferm Univ. 2015;12(2):56–62. doi:10.1016/j.reu.2015.03.002
34. Moreno L, Espildora E, Arriola M, Alonso J, Orueta R. Calidad de vida subjetiva en personas de 65 a 74 años y la influencia del género [Subjective quality of life in people aged 65–74 and the influence of gender]. Rev Clín Med Fam. 2019;12:119–124.
35. Paillard-Borg S, Wang H-X, Winblad B, Fratiglioni L. Pattern of participation in leisure activities among older people in relation to their health conditions and contextual factors: a survey in a Swedish urban area. Age Ageing. 2009;29(5):803–821. doi:10.1017/S0144686X08008337
36. Avital D. Gender differences in leisure patterns at age 50 and above: micro and macro aspects. Ageing Soc. 2017;37(1):139–166. doi:10.1017/S0144686X15001038
37. Jaumot-Pascual N, Monteagudo MJ, Kleiber DA, Cuenca J. Gender differences in meaningful leisure following major later life events. J Leisure Res. 2016;48(1):83–103. doi:10.18666/jlr-2016-v48-i1-6244
38. Agulló-Tomás MS, Zorrilla- Muñoz V, Gómez-García MV. Aproximación socio-espacial al envejecimiento y a los programas para cuidadoras/es de mayores [Socio-spatial approach to Aging and to the Programs for Carers of Older Persons]. Rev INFAD Psicol Int J Dev Educ Psychol. 2019;2(1):211–228. doi:10.17060/ijodaep.2019.n1.v2.1433
39. Kan M-Y, Zhou M, Negraia DV, et al. How do older adults spend their time? Gender gaps and educational gradients in time use in East Asian And Western countries. J Popul Ageing. 2021;14(4):537–562. doi:10.1007/s12062-021-09345-3
40. Perry-Jenkins M, Gerstel N. Work and family in the second decade of the 21st century. J Marriage Fam. 2020;82(1):420–453. doi:10.1111/jomf.12636
41. Sayer LC, Gornick J. Cross-national variation in older adult’s housework, active pursuits, and passive leisure. Soc Indic Res. 2009;93(1):215–218. doi:10.1007/s11205-008-9376-7
42. García Román J, Gracia P, Bikbov B. Gender differences in time use across age groups: a study of ten industrialized countries, 2005–2015. PLoS One. 2022;17(3):e0264411. doi:10.1371/journal.pone.0264411
43. Giménez-Nadal JI, Molina Chueca JA The Gender Gap in Time Allocation in Europe. presented at: IZA Discussion Paper No 13461; 2020. Available from: https://ssrn.com/abstract=3648801.
44. OCDE. Time Use. Available from: https://stats.oecd.org/Index.aspx?datasetcode=TIME_USE.
45. Ribeiro JP. Mental Health Inventory: um Estudo de Adaptação à População Portuguesa. Psicologia, saúde doenças. 2001;2(1):77–99.
46. Satorres Pons E Bienestar psicológico en la vejez y su relación con la capacidad funcional y la satisfacción vital [Psychological well-being in old age and its relationship with functional capacity and life satisfaction]. Universitat de València; 2013.
47. Mesa-Fernández M, Pérez-Padilla J, Nunes C, Menéndez S. Bienestar psicológico en las personas mayores no dependientes y su relación con la autoestima y la autoeficacia [Psychological well-being in non-dependent active elderly individuals and its relationship with self-esteem and self-efficacy]. Ciênc Saúde Colet. 2019;24(1):115–124. doi:10.1590/1413-81232018241.35302016
48. Veit CT, Ware JE Jr. The structure of psychological distress and well-being in general populations. J Consult Clin Psychol. 1983;51(5):730–742. doi:10.1037//0022-006x.51.5.730
49. Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Pers Soc Psychol. 1989;57(6):1069–1081. doi:10.1037/0022-3514.57.6.1069
50. Ryff CD. Psychological Well-Being in Adult Life. Curr Dir Psychol Sci. 1995;4(4):99–104. doi:10.1111/1467-8721.ep10772395
51. Topa G, García-Ael C. Desarrollo de carrera laboral y género. In: Holgueras-González AI, editor. Construcción sociocultural de género. Sanz y Torres; 2022:45–88.
52. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–827. doi:10.1007/s12160-010-9210-8
53. Quiroga-Méndez P. El apego en la vejez, una dimensión a tener en cuenta [Attachment in Old Age, a Dimension to Take into Account]. Acción Psicol. 2020;17(2):13–24. doi:10.5944/ap.17.2.29838
54. Vivaldi F, Barra E. Bienestar Psicológico, Apoyo Social Percibido y Percepción de Salud en Adultos Mayores [Psychological Well-Being, Perceived Social Support and Health Perception Among Older Adults]. Ter Psicol. 2012;30(2):23–29. doi:10.4067/S0718-48082012000200002
55. Zhou J, Yang C, Yu J, et al. The influence of social support on leisure-time physical activity of the elderly in the Chinese Village of Fuwen. Healthc. 2023;11(15):2193. doi:10.3390/healthcare11152193
56. Freire T, Fonte C. Escala de atitudes face ao lazer [Leisure attitude scale in adolescents and young adults]. Cad Psicol Educ. 2007;17(36):79–87. doi:10.1590/S0103-863X2007000100008
57. Maddox GL. Some correlates of differences in self-assessment of health status among the elderly. J Gerontol. 1962;17(2):180–185. doi:10.1093/geronj/17.2.180
58. World Health Organization. Statistics Netherlands. Health Interview Surveys: Towards International Harmonization of Methods and Instruments. Vol. 58. European: WHO Regional Office for Europe, WHO Regional Publications; 1996.
59. DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. A meta-analysis. J Gen Intern Med. 2006;21(3):267–275. doi:10.1111/j.1525-1497.2005.00291.x
60. Gravetter F, Forzano L. Research Methods for the Behavioural Sciences. Wadsworth Cengage Learning; 2011.
61. Hayes AF PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling; 2012.
62. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037/0022-3514.51.6.1173
63. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Erlbaum; 1988.
64. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
65. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
66. Katz D. The functional approach of the study of attitudes. Public Opin Q. 1960;24(2):163–204. doi:10.1086/266945
67. Smith MB. The personal setting of public opinions: a study of attitudes Toward Russia. Public Opin Q. 1947;11(4):507–523. doi:10.1086/265884
68. de Castro VC, Carreira L. Las actividades de ocio y la actitud de ancianos institucionalizados: informaciones para la práctica de enfermería [Leisure activities and attitude of institutionalized elderly people: a basis for nursing practice]. Rev Latino-Am Enferm. 2015;23(2):307–314. doi:10.1590/0104-1169.3650.2556
69. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall; 1986.
70. Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. 1993;28(2):117–148. doi:10.1207/s15326985ep2802_3
71. Merino Tejedor E. La expectativa de autoeficacia: su influencia y relevancia en el desarrollo personal [Self-Efficacy beliefs: its influence and relevance on Personal Development]. Int J Dev Educ Psychol. 2010;3(1):371–377.
72. González-Celis Rangel AL, Lima Ortiz L. Autoeficacia, percepción de salud y soledad, sobre la calidad de vida en adultos mayores [Self-Efficacy, Health Perception and Loneliness, on the Quality of Life in Older Adults]. Entreciencias: Diálogos en la Sociedad del Conocimiento. 2017;5(15):3–18. doi:10.22201/enesl.20078064e.2017.15.62571
73. Belo P Effects of educational level and leisure on elderly mental health in Portugal. Doctoral Thesis. Universitat de Valencia; 2021.
74. Belo P, Pocinho R, Navarro-Pardo E. Study of the leisure influence on attitude for leisure and mental health in a sample of Portuguese seniors. Rev Lusof Educ. 2017;38:119–130. doi:10.24140/issn.1645-7250.rle38.08
75. Borim F, Neri A, Francisco P, Barros MBDA. Dimensions of self-rated health in older adults. Rev Saúde Púb. 2014;48(5):714–722. doi:10.1590/S0034-8910.2014048005243
76. Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: three decades of progress. Psychol Bull. 1999;125(2):276–302. doi:10.1037/0033-2909.125.2.276
77. Galenkamp H, Deeg D, Huisman M, Hervonen A, Braam A, Jylha M. Is self-rated health still sensitive for changes in disease and functioning among nonagenarians? J Gerontol Ser B. 2013;68(5):848–858. doi:10.1093/geronb/gbt066
78. Leinonen R, Heikkinen E, Jylha M. Predictors of decline in self-assessments of health among older people – a 5-year longitudinal study. Soc Sci Med. 2001;52(9):1329–1341. doi:10.1016/S0277-9536(00)00249-5
79. Ocampo J. Self-rated health: importance of use in elderly adults. Colomb Med. 2010;41(3):275–289.
80. Rohrer J, Arif A, Denison A, Young R, Adamson S. Overall Self-rated health as an outcome indicator in primary care. J Eval Clin Pract. 2006;13(6):882–888. doi:10.1111/j.1365-2753.2006.00766.x
81. Vuorisalmi M Examining Self-Rated Health in Old Age: A methodological study of survey questions. Doctoral Thesis. University of Tampere; 2007.
82. de Bruin A, Picavet H, Nossikov A. Health Interview Surveys: Towards International Harmonization of Methods and Instruments. Vol. 58. WHO Regional Publications European Series. World Health Organization. Regional Office for Europe; 1996.
83. Falk H, Skoog I, Johansson L, et al. Self-rated health and its association with mortality in older adults in China, India and Latin America-A 10/66 Dementia Research Group study. Age Ageing. 2017;46(6):932–939. doi:10.1093/ageing/afx126
84. Confortin S, Giehl M, Antes D, Schneider I, d’Orsi E. Positive self-rated health in the elderly: a population-based study in the south of Brazil. Cad Saúde Púb. 2015;31(5):1049–1060. doi:10.1590/0102-311X00132014
85. Lima-Costa M, Firmo J, Uchôa E. Differences in self-rated health among older adults according to socio-economic circumstances. Cad Saúde Púb. 2005;21(3):830–839. doi:10.1590/S0102-311X2005000300017
86. Lucumi D, Grogan-Kaylor A, Espinosa-Garcia G. Asociación de la posición socioeconómica y la percepción del ambiente con la autopercepción del estado de salud en mujeres de Bogotá-Colombia [Socioeconomic status, perception of environment, and their association with self rated health status among women in Bogotá, Colombia]. Rev Panam Salud Pública. 2013;34(1):14–20.
87. Silverstein M, Parker MG. Leisure activities and quality of life among the oldest old in Sweden. Res Aging. 2002;24(5):528–547. doi:10.1177/0164027502245003
88. Windle G, Hughes D, Linck PG, Russell IT, Woods RT. Is exercise effective in promoting mental well-being in older age? A systematic review. Aging Mental Health. 2010;14(6):652–669. doi:10.1080/1360786100371323
89. Simons M, Reijnders J, Janssens M, Lataster J, Jacobs N. Staying connected in old age: associations between bonding social capital, loneliness and well-being and the value of digital media. Aging Mental Health. 2023;27(1):147–155. doi:10.1080/13607863.2022.2036947
90. Swami V, Weis L, Barron D, Furnham A. Positive body image is positively associated with hedonic (emotional) and eudaimonic (psychological and social) well-being in British adults. J Soc Psychol. 2018;158(5):541–552. doi:10.1080/00224545.2017.1392278
91. Joseph DL, Newman DA. Emotional intelligence: an integrative meta-analysis and cascading model. J Appl Psychol. 2010;95(1):54–78. doi:10.1037/a0017286
92. Gartzia L, Aritzeta A, Balluerka N, Barbera Heredia E. Inteligencia emocional y género: más allá de las diferencias sexuales [Emotional intelligence and gender: beyond sex differences]. Ann Psychol. 2012;28(2):567–575. doi:10.6018/analesps.28.2.124111
93. Murillo-Campos E, Ureña-Bonilla P. Personas adultas mayores como líderes transformadoras de la subcultura del centro diurno por medio de la actividad física [Senior Citizens Leaders Transforming the Subculture of the Day Care Center through Physical Activity]. Rev Electr Educare. 2016;20(1):1–15. doi:10.15359/ree.20-1.16
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.