")
Back to Journals » Patient Preference and Adherence » Volume 18
Latent Profile Analysis of Medication Beliefs in Patients with Type 2 Diabetes in the Hospital-Home Transition and Comparison with Medication Adherence
Authors Jiang S , Luo T, Zhu Z , Huang Y , Liu H, Li B, Feng S, Zeng K
Received 15 November 2023
Accepted for publication 19 March 2024
Published 16 April 2024 Volume 2024:18 Pages 839—853
DOI https://doi.org/10.2147/PPA.S450107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Sifen Jiang,1,2,* Tingyu Luo,2,* Zhuoqi Zhu,3,* Yanling Huang,2 Haopeng Liu,4 Bing Li,2 Suibin Feng,5 Kun Zeng1
1Science and Education Section, Dongguan Eighth People’s Hospital (Dongguan Children’s Hospital), Dongguan, People’s Republic of China; 2School of Nursing, Guangdong Pharmaceutical University, Guangzhou, People’s Republic of China; 3School of Public Health, Guangxi Medical University, Guangxi, People’s Republic of China; 4School of Public Health, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 5Surgery Department, Dongguan Eighth People’s Hospital (Dongguan Children’s Hospital), Dongguan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Suibin Feng, Surgery Department, Dongguan Eighth People’s Hospital (Dongguan Children’s Hospital), No. 68 South West Lake 3 Road, Shilong Town, Dongguan City, Guangdong Province, 523321, People’s Republic of China, Tel +86 13430293807, Email [email protected] Kun Zeng, Science and Education Section, Dongguan Eighth People’s Hospital (Dongguan Children’s Hospital), No. 68 South West Lake 3 Road, Shilong Town, Dongguan City, Guangdong Province, 523321, People’s Republic of China, Tel +86 13790300213, Email [email protected]
Background: The treatment of Type 2 Diabetes Mellitus (T2DM) is a protracted and arduous process. Medication, being a universally crucial therapeutic measure, underscores the significance of medication adherence in managing the disease effectively. Medication beliefs have emerged as a significant predictor of adherence, attracting considerable scholarly attention in recent years. However, there remains a paucity of research utilizing individual-centered approaches to explore medication beliefs among the T2DM population during the hospital-home transition, leaving the relationship between these beliefs and medication adherence unclear.
Purpose: To investigate latent categories of medication beliefs among patients with T2DM during the transition from hospital to home, and to analyze variations in medication adherence across these categories of patients.
Patients and methods: Between August 2022 and September 2023, this study selected 304 patients with a pre-discharge diagnosis of T2DM as study subjects from a tertiary hospital in Dongguan City. The patients’ profiles were assessed comprehensively via the Sociodemographic and Clinical Characteristics Questionnaire, alongside the Chinese version of Beliefs about Medicines Questionnaire-Specific and Morisky Medication Adherence Scale-8. The present study conducted latent profile analysis using Mplus 7.4 software and analyzed the influencing factors of different medication belief categories and their differences in medication adherence using SPSS 26.0 software.
Results: The medication beliefs of 304 patients were rated at 3.36± 5.24 points, while medication adherence scored 6.23± 1.56 points. The medication beliefs were classified into four categories: moderate necessity - low to moderate concern group (40.13%), high necessity - low concern group (9.54%), moderate necessity - moderate to high concern group (19.08%), and moderate necessity - high concern group (31.25%). Age, monthly per capita household income, and place of residence emerged as influential factors for the four categories. Moreover, the disparity in medication adherence among these categories demonstrated statistical significance (P < 0.001).
Conclusion: The medication beliefs of patients were classified into four distinct categories, and variations in medication adherence were evident across these categories. The high necessity - low concern group demonstrated the highest medication adherence scores, while the moderate necessity - high concern group exhibited the lowest scores. Healthcare providers are advised to tailor personalized medication belief enhancement programs based on patients’ homogeneous beliefs, addressing specific issues encountered by each category. This approach aims to ensure optimal medication adherence across diverse medical and social environments, effectively improving patient prognosis and enhancing quality of life.
Keywords: diabetes mellitus, T2DM, medication beliefs, medication adherence, latent profile analysis, influencing factors
Introduction
Diabetes mellitus is one of the most important non-communicable diseases threatening human health today.1 Data from the International Diabetes Federation in 2021 showed about 537 million adults with diabetes worldwide, with Type 2 Diabetes Mellitus (T2DM) constituting over 90% of the total diabetes population. It is expected that the total number of people with diabetes will increase to 783 million by 2045.2 Diabetes mellitus not only poses a higher challenge and threat to the physical and mental health of patients but also puts tremendous pressure on the healthcare system.3,4 Currently, there is still no complete cure for diabetes, requiring patients to rely on medication to control blood glucose for an extended period or even for life as a way to delay the onset of complications. Medication adherence refers to the extent to which patients adhere to the medication regimen prescribed by their physicians, including timing, dosage, and frequency.5 It highlights the importance of considering patients as partners in healthcare and emphasizes that medication adherence prioritizes patients’ acceptance of the treatment plan and their active participation in their health management.6 Various factors influence patient medication adherence. It involves a mutual decision between the patient and the prescriber to select the appropriate medication to ensure adherence, and patient education also plays a role in adherence.7 Foreign studies indicate that approximately one-sixth of patients fully comply with their medication treatment plans.8 Compared to chronic disease patients abroad, Chinese patients exhibit lower overall medication adherence levels.9 Data indicates that as many as 33% to 69% of chronic disease patients experience readmissions due to adverse outcomes stemming from medication non-adherence.10 Additionally, instances of diabetes patients experiencing emergent complications as a result of low medication adherence have been observed.11 Research has shown that implementing medication-related interventions can enhance patients’ understanding of medication knowledge and improve their medication adherence, thereby enhancing patients’ adaptability during the transition period after discharge and preventing the occurrence of adverse drug events.12 Therefore, adverse events may be modified to improve treatment outcomes instead. Improving patient medication adherence is crucial for preventing adverse events.
The transition from hospital to home is a high-risk period for patients exhibiting low medication adherence behavior. Naylor defines the period of transition from hospital to home as the eight weeks that follow a patient’s discharge and return to their home.13 During the transition period, patients undergo numerous changes. Research indicates that 19% of patients experience adverse events, with 66% of these events being medication-related.14 During hospitalization, patients benefit from the care and supervision of healthcare professionals, ensuring a high level of medication adherence. Further research suggests that hospital services play a significant role in ensuring medication adherence during the transition from hospital to home.15 A clinical survey found that over 50% of patients readmitted within 30 days lacked post-discharge follow-up records, indicating inadequate follow-up management by healthcare personnel.16 Disparities between discharge medications and those used at home can complicate medication regimens, leading to decreased adherence.17 Consequently, the lack of healthcare support, supervision, and regular follow-up during this transition, combined with multiple chronic conditions and complex medication regimens, may contribute to low medication adherence behaviors. Relevant data indicates that low medication adherence behavior in patients with T2DM can reach as high as 46.7% during the transition from hospital to home.18 Therefore, ensuring proper medication management during this transition period is of paramount importance.
Horne proposed that medication beliefs, which are the most important predictor of medication adherence, are a cognitive factor that can be changed. The beliefs encompass perceptions regarding the pros and cons of adhering to prescribed medication, incorporating both the perception of benefits (necessity beliefs) and concerns about potential drawbacks (concern beliefs).19 Horne and other researchers, in their study of the impact of medication beliefs on treatment adherence in patients with chronic diseases, pointed out that the higher the belief in necessity, the greater the perceived benefits of medication and the greater the likelihood that the individual will adopt adherence behaviors. In contrast, the higher the belief of concern, the more the individual worries about problems such as adverse reactions to medications, the more barriers are perceived during medication administration, and consequently, the emergence of low adherence behaviors.19 It has been demonstrated that hospital discharge can alter medication beliefs and increase the risk of non-adherence. This is primarily due to potential changes in the patient’s medication regimen during hospitalization and inadequate transfer of information at discharge.20,21 Interventions by healthcare personnel during hospitalization, along with post-discharge follow-up management, can effectively enhance patients’ medication beliefs, leading to improved medication adherence and treatment efficacy.22 Medication beliefs are gaining increasing attention as protective factors against adverse medication behavior. However, many previous studies on medication beliefs have categorized them based on total scale scores or traditional cut-off points,23 without considering the differences in participants’ scores for each item. Additionally, the relationship between these inter-individual differences and medication adherence has not been studied, rendering the existing findings irrelevant in guiding personalized clinical practice, which can result in ineffective interventions and wasted healthcare resources. Thus, a comparison that focuses on individual medication belief category characteristics and their relationship with medication adherence may be more pertinent.
Latent Profile Analysis (LPA) is a statistical analysis method based on continuous variables, which classifies individuals with similarities into the same subgroups for group heterogeneity analysis based on their response patterns on the externally measured entries and is now widely used in psychology, medicine, and other fields.24 In addition, compared to traditional individual-centered techniques, LPA maintains stricter criteria for the number of categories, resulting in more precise classification outcomes.25 Therefore, building upon the limitations of prior research, this study aims to investigate the medication belief scores of T2DM patients during the hospital-home transition using LPA. The objective is to achieve a precise categorization of medication beliefs, explore the distribution of each latent category, and examine their association with medication adherence. Ultimately, the study seeks to provide a reference and rationale for the development of interventions aimed at improving medication adherence among T2DM patients.
Materials and Methods
Participants
T2DM patients discharged after receiving inpatient treatment at a tertiary hospital in Dongguan City from August 2022 to September 2023 were selected for the study using a convenience sampling method. The inclusion criteria were as follows: ① age ≥18 years; ② meeting the diagnostic criteria for T2DM according to the World Health Organization (WHO);26 ③ having a history of T2DM for at least three months, excluding newly diagnosed patients; ④ long-term oral administration of at least one antidiabetic medication post-discharge (lasting more than three months or continuing for several years), including patients using insulin injections; ⑤ providing informed consent and willingly participating in this study. The exclusion criteria were as follows: ① being transferred to other medical institutions for further treatment (including long-term care facilities) after discharge; ② having severe mental disorders, mental retardation, hearing impairment, or speech and communication disorders; ③ being unable to provide self-care entirely.
Sample Size Calculation
In this study, there were a total of 18 variables. Among these, the Sociodemographic and Clinical Characteristics Questionnaire encompassed 15 variables, the Chinese Version of Beliefs about Medicines Questionnaire-Specific (C-BMQ-S) comprised two dimensions, and the Chinese Version of Morisky Medication Adherence Scale-8 (C-MMAS-8) contained one dimension. The sample size was estimated using the method proposed by Castro and Kendall, which recommends a sample size of at least 10–15 times the number of variables.27 Considering a 20% potential loss-to-follow-up rate, the final sample size was between 216 and 324 cases. Out of the initial 329 selected patients, 17 could not be reached by phone, and eight refused to participate during the follow-up visit. In total, 25 cases were not visited. The successful return visit was conducted for 304 patients, resulting in an effective return rate of 92.4%.
Methods
Through a literature review and consultation with clinical care experts, the research team developed its questionnaire to collect information on the sociodemographic and clinical characteristics of the patients: gender, age, marriage, education level, place of residence, monthly per capita household income, duration of diabetes, number of discharged drugs, number of comorbid chronic diseases, and length of hospitalization, among others.
In 1999, Horne developed the Beliefs about Medicines Questionnaire (BMQ).28 This questionnaire comprises two subscales: Specific (BMQ-S) and General (BMQ-G) beliefs about medication. These subscales can be employed separately or in conjunction to evaluate patients’ medication beliefs, especially those with chronic diseases. Tang and her team adapted and revised the BMQ-S for the Chinese population, resulting in the Chinese version of Beliefs about Medicines Questionnaire-Specific (C-BMQ-S), specifically tailored for patients with T2DM.29 This scale encompasses two dimensions: necessity beliefs (items 1–2, 8–10) and concern beliefs (items 3–7), each consisting of five items, totaling ten. The scale uses a Likert 5-point scoring method, where 1 = strongly disagree, 2 = disagree, 3 = unsure, 4 = agree, and 5 = strongly agree. Higher scores in each dimension indicate stronger patient beliefs regarding the necessity of medication or their concerns. Based on the formula “medication beliefs score = total necessity beliefs score minus total concerns beliefs score”, a positive score signifies that the benefits or necessity of medication outweigh any potential drawbacks or concerns, implying that the patient holds a favorable perception toward the medication regimen. The scale demonstrated satisfactory reliability in this study, with a Cronbach’s alpha coefficient of 0.797 for necessity and 0.700 for concern beliefs.
Morisky and his team developed the Morisky Medication Adherence Scale-8 (MMAS-8) to assess patients’ medication adherence levels.30–32 The team led by Wang developed the Chinese version of the Morisky Medication Adherence Scale-8 (C-MMAS-8) through translation, back-translation, and debugging.33 They tested its reliability and validity in patients with T2DM. The Cronbach’s alpha coefficient of the C-MMAS-8 is similar to findings from studies conducted by scholars in Thailand and Malaysia, indicating good reliability.34,35 The C-MMAS-8 consists of a total of eight items. Items 1 to 7 are dichotomously scored as “yes” (recorded as 0 points) or “no” (recorded as 1 point), with item 5 reverse-scored. Item 8 employs a Likert 5-point scoring method, ranging from “never/rarely” to “all the time”, corresponding to scores of 1, 0.75, 0.5, 0.25, and 0, respectively. The total score ranges from 0 to 8. Scores below 6 indicate poor adherence, scores between 6 and less than 8 indicate moderate adherence, and a score of 8 indicates good adherence.
Data Collection
The participants were methodically chosen based on predefined inclusion and exclusion criteria using a consecutive sampling approach, continuing until the intended sample size was attained. The researchers explained the study’s objectives, significance, and participation principles to the patients. They also informed the patients that the investigation would be conducted anonymously and in adherence to confidentiality principles. A standardized set of instructions was used to clarify the necessary steps to complete the questionnaire. Patients were provided with thorough explanations for any items that caused confusion.
The entire survey took roughly 15 to 25 minutes to finish. Data collection for this study was divided into two phases. Phase 1 (day of discharge): sociodemographic and clinical characteristic information was gathered by researchers from either inpatient records or through face-to-face interaction with the patient. This phase, which also involved obtaining the hospital-provided discharge records, took approximately 5 minutes. Phase 2 (within eight weeks of discharge): during outpatient follow-up visits, the researchers conducted face-to-face surveys with the patients using the C-BMQ-S and C-MMAS-8 scales to collect data. In cases where patients did not attend follow-up visits, the researchers collected data through telephone follow-up interviews. The researchers refrained from providing any suggestive prompts while patients answered questions, and assessed the accuracy of patients’ medication information based on the collected discharge records and duly recorded them. This phase took approximately 10 to 20 minutes.
Statistical Analysis
Statistical analysis was performed using Mplus 7.4 and IBM SPSS 26.0 software. (1) The categories of medication beliefs were explored using LPA, with the C-BMQ-S item scores of T2DM patients as the model exogenous variable, setting the initial model to one category and gradually increasing the number of category models from the initial model. Based on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted BIC (aBIC), Entropy index, the Lo-Mendell-Rubin Likelihood Ratio Test (LMRT), and the Bootstrap Likelihood Ratio Test (BLRT) were used to determine the fitness of the model. Model fit assessment criteria: ① smaller values of AIC, BIC, and aBIC indicate better model fit; ② Entropy represents the accuracy of classification, ranging from 0 to 1. A value of 0.8 indicates a classification accuracy exceeding 90%, and the closer the value is to 1, the higher the probability of individuals being accurately classified;36 ③ LMRT and BLRT compare the goodness of fit between the k and k-1 models; if the two likelihood ratio tests are P < 0.05, the k models fit better than the k-1 models until the model fit data is optimal.36,37 (2) When the research data is based on patient self-reports, there may be a potential common method bias. The Harman’s single-factor test was employed to examine the presence of common method bias.38 It is generally accepted that a single factor accounting for variance should not exceed 40%.39 (3) Continuous variables were expressed as mean ± standard deviation or median with interquartile range (IQR), while proportions represented categorical variables. Chi-square tests were employed to analyze differences in sociodemographic and clinical characteristics among patients with different categories of medication beliefs. An unordered multinomial logistic regression was employed with medication belief latent categories as the dependent variable. Factors that exhibited significant differences in the univariate analysis were used as independent variables to investigate further their influence on patients’ medication belief latent categories. Differences were considered statistically significant at a threshold of P < 0.05. Unordered multinomial logistic regression automatically compares categorical data without the need for setting dummy variables. (4) A one-way ANOVA test and Chi-square test were employed to compare medication belief latent categories with medication adherence scores and levels. Differences were considered statistically significant at a threshold of P < 0.05.
Results
Common Method Bias Test
An exploratory factor analysis without rotation was conducted on all measurement items related to medication beliefs and medication adherence. Six factors were extracted with eigenvalues greater than 1. The first factor explained 19.81% of the variance, below the critical threshold of 40%, which indicates that there is no significant common method bias present in this study.
Patient Characteristics
This study included 304 patients with T2DM, ranging in age from 22 to 90 years old (63.63±13.17 years). The ratio of males to females was 43.1% to 56.9%. A significant majority of participants, 79.6%, had an education level at or below junior high school. Retired or unemployed individuals accounted for 65.5% of the sample. The average duration of diabetes was 6 (IQR 3-13) years, with an average of 2.77±1.42 types of comorbid chronic conditions. The number of prescribed medications at discharge was 7.12±2.68 types, with an average hospital stay of 9 (IQR 6-13) days. Table 1 outlines the detailed characteristics.
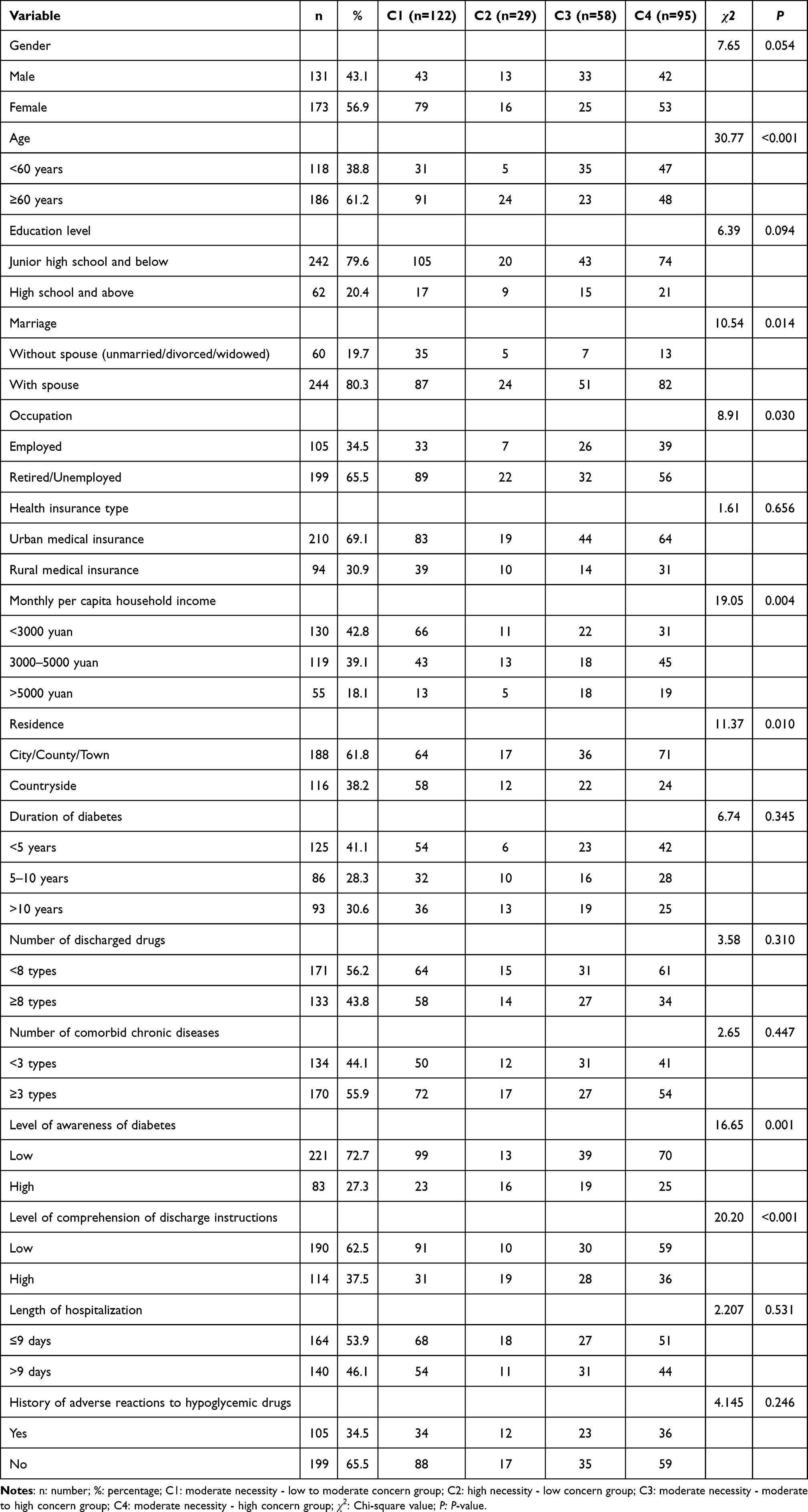 |
Table 1 T2DM Patient Characteristics and the Univariate Analysis of Medication Belief Categories (n = 304) |
Scores of C-BMQ-S and C-MMAS-8
The medication belief score for T2DM patients was 3.36±5.24, with a necessity belief score of 18.47±3.18 and a concern belief score of 15.10±3.86. Approximately 72% of the patients displayed a positive discrepancy in their beliefs regarding necessity and concern, while 21.7% exhibited a negative discrepancy, and 6.3% had no discrepancy at all. The medication adherence score was 6.23±1.56, suggesting that medication adherence among the T2DM population typically falls within the moderate range. Based on the classification criteria, 121 patients (39.8%) in this study demonstrated poor adherence, while 139 (45.7%) exhibited moderate adherence, and only 44 patients (14.5%) showed good adherence.
Latent Profiling of Medication Beliefs in Patients with T2DM
Person-centered LPA was conducted on the C-BMQ-S scores of 304 patients with T2DM, with the scores of the ten items serving as exogenous indicators. Models were fitted with 1 to 5 latent profiles, starting from the baseline model with one category, as presented in Table 2. The AIC, BIC, and aBIC values exhibited consistent decreases in this analysis. Retaining four categories resulted in an Entropy index range of 0.9 to 1. Also, both the LMRT and BLRT values achieved statistical significance (P < 0.05). The assignment probabilities for the four categories were 98%, 96.7%, 96.2%, and 99.8%, all exceeding 90%, indicating a reliable classification of the model results. While retaining five categories resulted in the minimum AIC, BIC, and aBIC values, the LMRT value did not reach significance. Therefore, considering all the results, the final decision is to choose the 4-category model as the optimal model for categorizing medication belief profiles in T2DM patients.
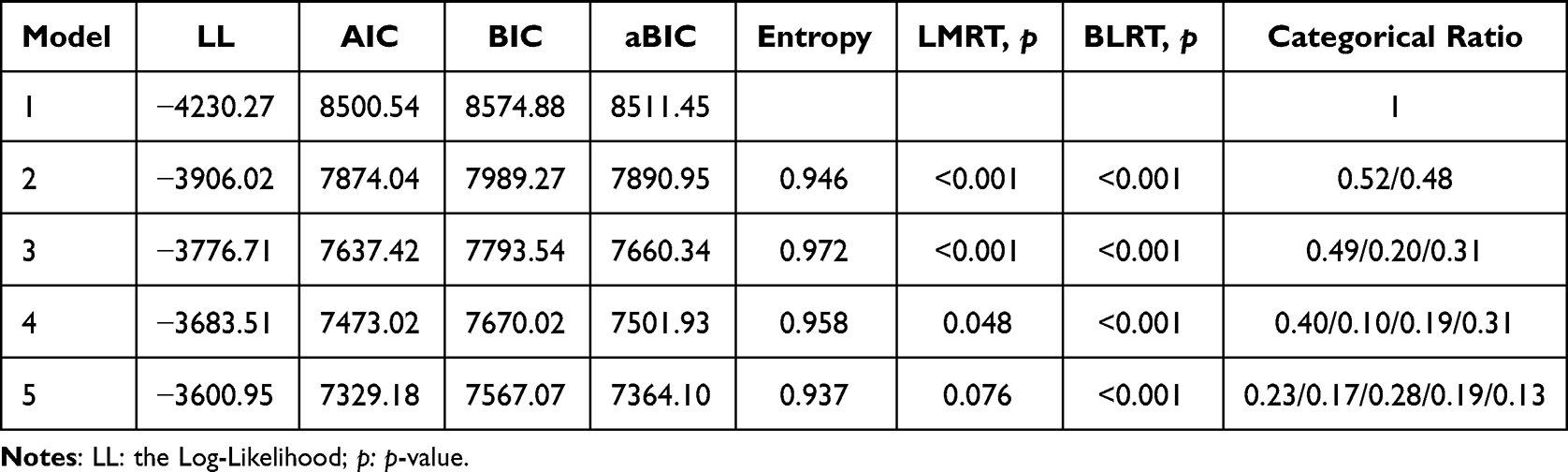 |
Table 2 Fitting Metrics for a Latent Profile Model of Medication Beliefs in Patients with T2DM |
In the C-BMQ-S scale, higher scores on items 1–2 and 8–10 indicate stronger beliefs in the necessity of medication for the patient. Conversely, higher scores on items 3–7 indicate greater concerns about medication for the patient. Based on Model 4, the mean scores of the items for each category of medication beliefs can be found in Figure 1. Subsequently, C1, C2, C3, and C4 were named based on the distribution patterns of each category. The scores for items 1–2 and 7–10 in categories C1, C3, and C4 were similar. However, C1 exhibited lower scores on items 3–6, indicating that patients in this group possess moderate necessity beliefs and lower concern beliefs. C1 was titled “moderate necessity - low to moderate concern” group. The medication belief score was 4.90±3.16 points, and C1 comprised 40.13% (122/304) of the sample. C2 exhibited a high level of necessity and low concern beliefs, representing 9.54% (29/304) of the sample. It is named “high necessity - low concern” group; the score for belief in medication was 13.00±3.26 points. C3 demonstrated higher scores on items 3–7 and was named “moderate necessity - moderate to high concern” group, comprising 19.08% (58/304) of the sample. The medication belief score was 1.62±3.35 points. In the sample, C4 represented 31.25% (95/304), and the medication belief score was −0.48±4.15 points. Patients in this category demonstrated elevated mean values in the concern dimension, indicating they view medication as necessary while harboring severe concerns about potential adverse effects and disruptions to their daily activities. Therefore, C4 was named “moderate necessity - high concern” group.
 |
Figure 1 Score distribution of latent categories for medication beliefs in T2DM patients. |
The Univariate Analysis of Medication Belief Latent Categories in T2DM Patients
The results of the univariate analysis demonstrated significant differences among the four groups in age, marriage, occupation, monthly per capita household income, place of residence, level of awareness of diabetes, and comprehension of discharge instructions (all P < 0.05), as shown in Table 1.
The Multifactorial Analysis of Latent Categories of Medication Beliefs in Patients with T2DM
The research results indicated that age, monthly per capita household income, and place of residence influenced the latent categorization of medication beliefs in T2DM patients (P < 0.05), as shown in Table 3.
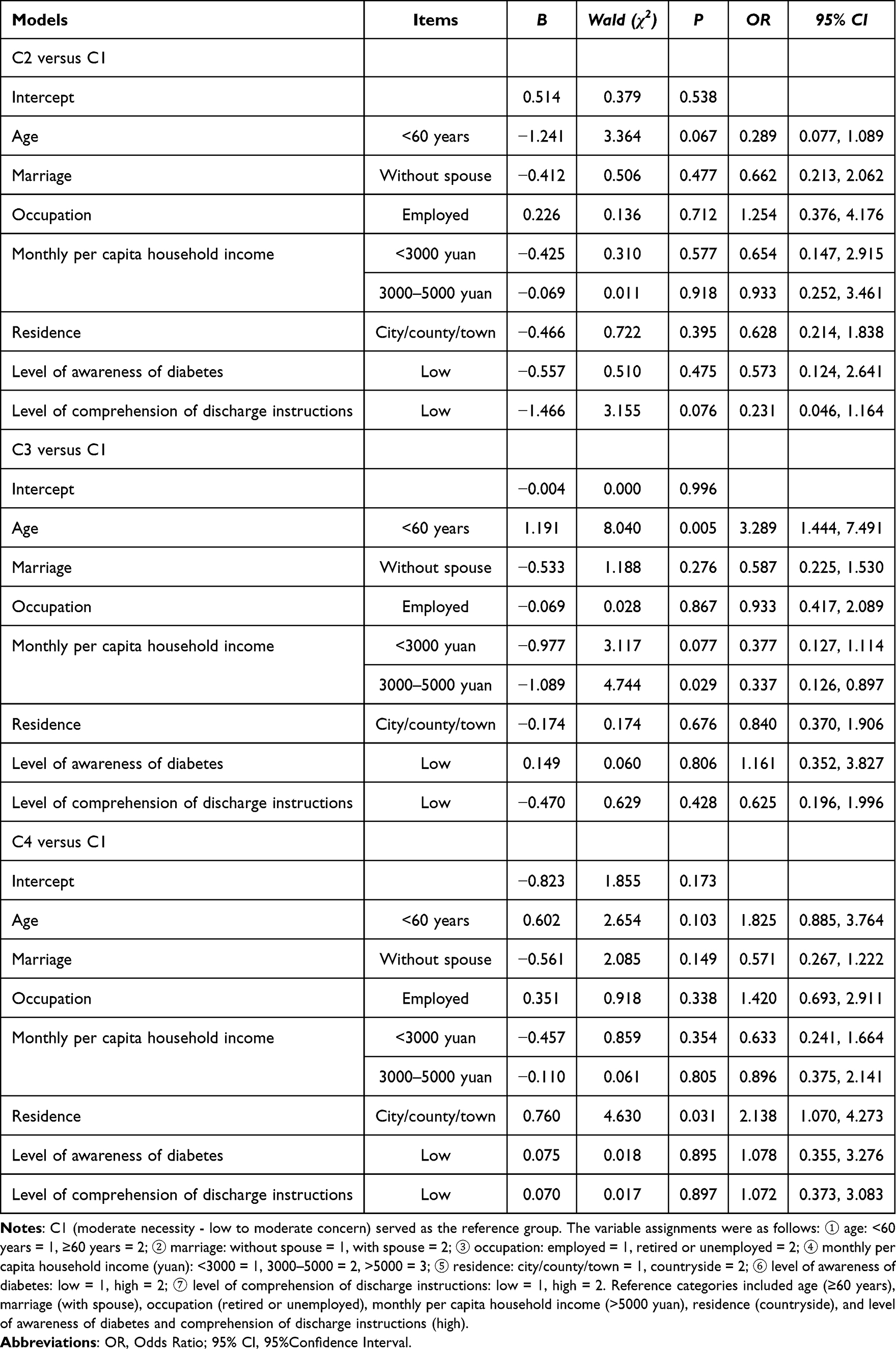 |
Table 3 Multifactorial Analysis of Latent Categories of Medication Beliefs in Patients with T2DM |
Comparison of Medication Adherence Among T2DM Patients with Different Medication Belief Categories
The latent profile analysis extracted four distinct medication belief categories, and a comparison of medication adherence scores and levels among these categories revealed statistically significant differences (P < 0.001), as shown in Table 4.
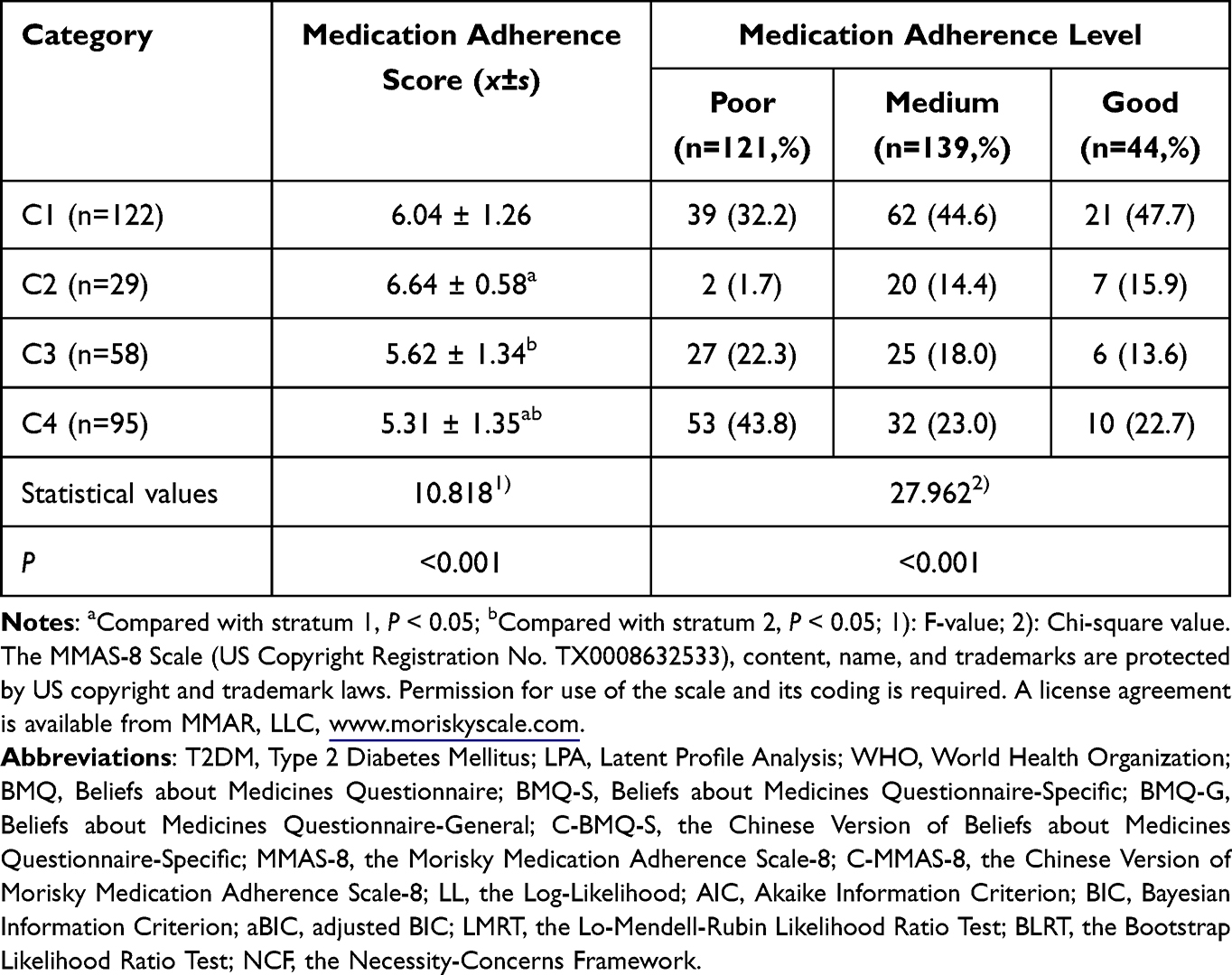 |
Table 4 Comparison of Medication Adherence Among T2DM Patients with Different Medication Belief Categories (n = 304) |
Discussion
Current Status of Medication Beliefs and Adherence in Patients with T2DM
The results indicated that T2DM patients in the hospital-home transition period had a medication belief score of 3.36±5.24, suggesting significant room for improvement in medication beliefs within this population, particularly when compared to the findings of Mortelmans.40 The study surveyed 400 elderly patients receiving polypharmacy post-discharge, revealing a medication belief score of 7.50±5.09, approximately 91.4% of patients showed a positive necessity-concern discrepancy.40 The difference could potentially be attributed to the fact that Mortelmans’s study focused on elderly patients with comorbidities, a demographic that typically relies more heavily on medication for their health. Elderly patients with comorbidities tend to hold strong beliefs regarding the necessity of current and future health maintenance, leading to firmer medication beliefs.40
In this study, T2DM patients demonstrated a medication adherence score of 6.23±1.56 during the transition period, similar to the results reported by Xue.18 The above results indicate that medication adherence among T2DM patients during the transition period is not optimistic. Given the increasing global prevalence of T2DM patients, it suggests that healthcare professionals should enhance medication education before patient discharge to comprehensively improve patients’ medication knowledge and beliefs. Conducting early post-discharge follow-ups with patients is crucial, which allows for the assessment of medication adherence and enables the prompt identification and management of any symptoms that may arise at home, ensuring the safety of medication use for patients.
The Latent Categories and Characteristics of Medication Beliefs in T2DM Patients
Patients often engage in a cost-benefit analysis of medications before administration, weighing the necessity of taking the medication against potential adverse reactions.19 This study found that medication beliefs among T2DM patients can be categorized into four groups: moderate necessity - low to moderate concern (C1), high necessity - low concern (C2), moderate necessity - moderate to high concern (C3), and moderate necessity - high concern (C4).
Patients in C1 comprised 40.13% of the sample. These patients had low concern scores compared to the overall level. However, they had the highest scores in the concern beliefs for item 7, “I do not know about my hypoglycemic medication”, reflecting that this group of patients was very uninformed about the medication they were taking. It may be related to the fact that this group of patients was older and less educated. Older individuals often experience varying degrees of decline in cognitive function and memory. Moreover, individuals with lower levels of education may face challenges in comprehending the role of medications in the diagnosis and treatment process. Consequently, their limited ability to acquire knowledge about the disease and medications may result in a lack of understanding regarding the drugs they are taking.41
The result revealed that 9.54% of patients belonged to C2, 82.8% of whom were elderly. This group exhibited a favorable attitude towards medication treatment, with minimal levels of concern. Their beliefs regarding medications were positive and affirming. Previous research indicates a strong positive relationship between age and belief in the necessity of medication. As individuals age, their belief in the necessity of medication tends to increase.42,43 Older patients may often exhibit higher trust in their physicians than younger patients. Additionally, physicians tend to emphasize the necessity of medication, which may lead older patients to more readily adopt a belief characterized by high necessity and low concern.44
Patients in C3 constituted 19.08% of the overall population. The medication belief score among this group was 1.62±3.35, similar to the results of Zhang’s study.45 While patients in this group perceive the necessity of taking antidiabetic medications to outweigh their concerns, 39.7% of them have experienced adverse drug reactions during the medication process, which has increased their concerns and apprehensions towards medication. Moreover, over 50% of patients in this group have a limited understanding of diabetes and discharge directions. This lack of understanding could lead to apprehensions about drug therapy, ultimately resulting in weaker medication adherence.
Patients in C4 had a medication belief score of −0.48±4.15. The scores for items three to five related to concern beliefs were significantly higher in this group compared to the other groups. It primarily reflects concerns about the side effects of antidiabetic drugs, long-term effects, and worries about dependence on drugs. Indicating that, although patients in this group hold a moderate level of necessity beliefs, they express significant concerns about taking medication, especially when experiencing adverse drug reactions or lacking confidence in the long-term effectiveness of the medication.
Factors Influencing Latent Categories of Medication Beliefs in Patients with T2DM
In this study, T2DM patients under 60 years of age were 3.289 times more likely to be classified in C3 than C1. Wan’s study also showed that patients under 60 years of age have higher concern beliefs.46 T2DM signifies that individuals are poised to undergo prolonged medication regimens, necessitating a substantial financial commitment. Additionally, potential work disruptions due to medication side effects may lead to a reduction in economic earnings. As a result, these factors heighten medication concerns among individuals under the age of 60.
The results of present study indicated that monthly per capita household income was a potential influencing factor for the categorization of medication beliefs. Compared to C3, patients with monthly per capita household income ranging from 3000 to 5000 yuan were more likely to be classified into C1. Related studies have also confirmed that low income has a statistically significant impact on concern beliefs.47 Patients with low income may struggle to sustain the expenses of disease treatment. The economic pressures may overwhelm patients, leading to negative beliefs about medication treatment.
This study also found that, comparison to C1, patients residing in city/county/town areas predominantly belong to C4. Rural patients may have less knowledge about medications,48 leading them to adopt a mindset of “if there is medicine, take it”, and overlook potential adverse effects, resulting in lower concerns about medication. Studies have reported a significantly higher incidence of depression and anxiety among urban residents compared to rural residents.49 Bünemann’s research indicates a significant correlation between anxiety, depression, and higher levels of concern about medication.50 Patients with depression or anxiety tend to be more apprehensive and experience a sense of insecurity, potentially leading urban patients to develop more concerns and worries about their medication.
Differences in Medication Adherence Scores and Levels in Different Categories of T2DM Patients
The Necessity-Concerns Framework (NCF) posits that medication adherence is influenced by an individual’s perceived need for the prescribed medication and concerns about potential side effects.51 A study identified positive correlation between medication beliefs and adherence.52 As the medication belief scores increased, so did the adherence scores, aligning with the findings of present study. The present study observed significant differences in medication adherence scores among the four latent categories of medication beliefs. Patients in C2 exhibited the highest medication adherence scores, followed by those in C1 and C3. Conversely, patients in C4 demonstrated the lowest scores. These findings align with the results reported by Italian scholars.53 The Italian scholars classified medication beliefs into four groups based on patients’ attitudes toward medication needs and concerns: skeptical (low necessity and high concerns), ambivalent (high necessity and high concerns), indifferent (low necessity and low concerns), and accepting (high necessity and low concerns). The findings indicated that patients in the accepting group exhibited the highest adherence to medication, while those in the skeptical group had the lowest.53
According to self-regulation theory, an individual’s beliefs influence their understanding of information, subsequently affecting their behavior. Semahegn’s study demonstrated that the primary reasons for patients’ subjective and intentional nonadherence to medication are insufficient beliefs about medication and a lack of knowledge about the disease and medication.54 The present study also indicated significant differences in the level of medication adherence among the four medication belief categories. The current study again suggest that patients with higher medication beliefs tend to exhibit better medication adherence. It may be attributed to the fact that when patients perceive the benefits of adhering to prescribed medication outweigh the drawbacks, they are more inclined to take medication voluntarily.55 Providing services such as medication reconciliation, medication education, and post-discharge telephone follow-up to discharged patients can significantly enhance their medication competence and adherence.56 Therefore, healthcare professionals should provide health education to T2DM patients to enhance their beliefs about the necessity of taking medication and eliminate their concerns about the treatment of the disease, which will help to improve their medication adherence and subsequently improve their quality of life.
Limitations
For the first time, the present study utilized LPA to classify the medication beliefs of T2DM patients during the transition from hospital to home at an individual level, and the appropriateness of the assigned names requires further exploration. Furthermore, The chosen location of the hospital in this study resulted in the predominance of residents from the hospital vicinity among the study subjects. This study was limited to a tertiary hospital in Dongguan City due to objective constraints. In the future, it would be beneficial to conduct surveys in multiple regions with larger sample sizes to further analyze the characteristics of medication beliefs among T2DM patients and validate and refine the conclusions.
Conclusion
In the present study, T2DM patients displayed low medication beliefs and medium adherence during the transition from hospital to home. The study employed LPA to explore latent categories of medication beliefs among T2DM patients, identifying four categories: moderate necessity - low to moderate concern, high necessity - low concern, moderate necessity - moderate to high concern, and moderate necessity - high concern. Secondly, the analysis unveiled significant differences in age distribution, monthly per capita household income, and residence among different categories of T2DM patients. This suggests that healthcare professionals should implement targeted interventions tailored to the medication belief characteristics of different T2DM patient categories in clinical practice. Additionally, this research confirmed a positive correlation between stronger patient medication beliefs and improved medication adherence. Among them, the group with high necessity - low concern exhibited the highest level of adherence, while the group with moderate necessity - high concern showed the lowest level of adherence. Healthcare professionals should pay special attention to the latter group and enhance their medication beliefs to improve their medication adherence.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. Approval for the study (Approval Number: LL2022053002) was granted by the Ethics Committee of Dongguan Eighth People’s Hospital. After providing a brief overview of the study’s purpose, methodology, and associated risks and benefits, participants provided informed consent willingly. During the research, we took stringent measures to ensure utmost confidentiality of all patient-related data.
Acknowledgments
We sincerely thank the investigators and patients at Dongguan Eighth People’s Hospital for their valuable contributions to our study.
The MMAS-8 Scale (US Copyright Registration No. TX0008632533), content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., www.moriskyscale.com.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heald AH, Stedman M, Davies M, et al. Estimating life years lost to diabetes: outcomes from analysis of National Diabetes Audit and Office of National Statistics data. Cardiovasc Endocrinol Metab. 2020;9(4):183–185. doi:10.1097/XCE.0000000000000210
2. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. doi:10.1038/s41598-020-71908-9
4. Kennedy-martin T, Boye KS, Peng X. Cost of medication adherence and persistence in type 2 diabetes mellitus: a literature review. Patient Prefer Adherence. 2017;11:1103–1117. doi:10.2147/PPA.S136639
5. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
6. Viktil KK, Frøyland H, Rogvin M, et al. Beliefs about medicines among Norwegian outpatients with chronic cardiovascular disease. Eur J Hosp Pharm. 2014;21(2):118–120. doi:10.1136/ejhpharm-2013-000346
7. Ayodapo AO, Elegbede OT, Omosanya OE, et al. Patient education and medication adherence among hypertensives in a tertiary hospital, South Western Nigeria. Ethiop J Health Sci. 2020;30(2):243–250. doi:10.4314/ejhs.v30i2.12
8. Urquhart J. The odds of the three nons when an aptly prescribed medicine isn’t working: non-compliance, non-absorption, non-response. Br J Clin Pharmacol. 2002;54(2):212–220. doi:10.1046/j.1365-2125.2002.01629.x
9. Wang W, Luan W, Zhang Z, et al. Association between medication literacy and medication adherence and the mediating effect of self-efficacy in older people with multimorbidity. BMC Geriatr. 2023;23(1):378. doi:10.1186/s12877-023-04072-0
10. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
11. Wolf RA, Haw JS, Paul S, et al. Hospital admissions for hyperglycemic emergencies in young adults at an inner-city hospital. Diabet Res Clin Pract. 2019;157:107869. doi:10.1016/j.diabres.2019.107869
12. Foust JB, Kilbourne GA. Improving posthospital medication management for chronically ill older adults. Am Nurse Today. 2015;10(3):26–29.
13. Naylor MD, Marcille J. Managing the transition from the hospital. Manag Care. 2014;23(6):27–30.
14. Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167. doi:10.7326/0003-4819-138-3-200302040-00007
15. Daliri S, Boujarfi S, Ei Mokaddam A, et al. Medication-related interventions delivered both in hospital and following discharge: a systematic review and meta-analysis. BMJ Qual Saf. 2021;30(2):146–156. doi:10.1136/bmjqs-2020-010927
16. Rohr R. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;361(3):311–312.
17. Pantuzza LL, Ceccato M, Silveira MR, et al. Association between medication regimen complexity and pharmacotherapy adherence: a systematic review. Eur J Clin Pharmacol. 2017;73(11):1475–1489. doi:10.1007/s00228-017-2315-2
18. Xue WJ, Niu XD, Wang YH. Research on the condition of medication discrepancy in hospital-family transitional period in elderly patients with type 2 diabetes mellitus. Chin J Nurs. 2021;56(02):225–232. doi:10.3761/j.issn.0254-1769.2021.02.011
19. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
20. Daliri S, Bekker CL, Buurman BM, et al. Barriers and facilitators with medication use during the transition from hospital to home: a qualitative study among patients. BMC Health Serv Res. 2019;19(1):204. doi:10.1186/s12913-019-4028-y
21. Cua YM, Kripalani S. Medication use in the transition from hospital to home. Ann Acad Med Singap. 2008;37(2):136.
22. Wang Q, Zhu R, Cao Y, et al. Sublingual immunotherapy adherence in patients with allergic rhinitis: effects of an intervention based on the information-motivation-behavioral skills mode. Heliyon. 2023;9(12):e22929. doi:10.1016/j.heliyon.2023.e22929
23. Wei L, Champman S, Li X, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ Open. 2017;7(10):e17293. doi:10.1136/bmjopen-2017-017293
24. Yin K, Peng J, Zhang J. The application of latent profile analysis in organizational be-havior research. Adv Psychol Sci. 2020;28(07):1056–1070. doi:10.3724/SP.J.1042.2020.01056
25. Vermunt JK, Magidson J. Factor analysis with categorical indicators: a comparison between traditional and latent class approaches. In: New Developments in Categorical Data Analysis for the Social and Behavioral Sciences. Psychology Press; 2005:41–62.
26. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(sici)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-s
27. Castro AL, Kendall MC. Sample size and the establishment of safety in perioperative medicine. Actas Urol Esp. 2018;42(9):610. doi:10.1016/j.acuro.2018.05.007
28. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
29. Tang J, Gao LL, Hu XL, et al. The reliability and validity of the Chinese version of beliefs about medicines questionnaire-specific among patients with type 2 diabetes mellitus. J Nurs Sci. 2019;34(21):25–28. doi:10.3870/j.issn.1001-4152.2019.21.025
30. Morisky DE, Ang A, Krousel-wood M, et al. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
31. Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of intensive versus standard blood-pressure control. N Engl J Med. 2017;377(8):745–755. doi:10.1056/NEJMsa1616035
32. Berlowitz DR, Foy CG, Kazis LE, et al. Impact of intensive blood pressure therapy on patient-reported outcomes: outcomes results from the SPRINT study. N Engl J Med. 2017;377:733–744. doi:10.1056/NEJMoa1611179
33. Wang J, Mo YZ, Bian RW, et al. Chinese 8-item morisky medication adherence questionnaire: reliability and validity in elderly type 2 diabetes mellitus patients. Chin J Gerontol. 2015;35(21):6242–6244. doi:10.3969/j.issn.1005-9202.2015.21.115
34. Sakthong P, Chabunthom R, Charoenvisuthiwongs R. Psychometric properties of the Thai version of the 8-item Morisky Medication Adherence Scale in patients with type 2 diabetes. Ann Pharmacother. 2009;43(5):950–957. doi:10.1345/aph.1L453
35. Al-qazaz H, Hassali MA, Shafie AA, et al. The eight-item Morisky Medication Adherence Scale MMAS: translation and validation of the Malaysian version. Diabet Res Clin Pract. 2010;90(2):216–221. doi:10.1016/j.diabres.2010.08.012
36. Lubke G, Muthén BO. Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Structl Equat Model. 2007;14(1):26–47. doi:10.1080/10705510709336735
37. Jung T, Wickrama KAS. An Introduction to latent class growth analysis and growth mixture modeling. Soc Personal Psychol Compass. 2010;2(1):302–317. doi:10.1111/j.1751-9004.2007.00054.x
38. Zhou H, Long LR. Statistical remedies for common method biases. Adv Psychol Sci. 2004;6:942–950.
39. Tang DD, Wen ZL. Common methodology bias testing: issues and recommendations. J Psychol Sci. 2020;43(01):215–223. doi:10.16719/j.cnki.1671-6981.20200130
40. Mortelmans L, Goossens E, Dilles T. Beliefs about medication after hospital discharge in geriatric patients with polypharmacy. Geriatr Nurs. 2022;43:280–287. doi:10.1016/j.gerinurse.2021.12.007
41. Plaza-zamora J, Legaz I, Osuna E, et al. Age and education as factors associated with medication literacy: a community pharmacy perspective. BMC Geriatr. 2020;20(1):501. doi:10.1186/s12877-020-01881-5
42. Aikens JE, Nease DJ, Klinkman MS. Explaining patients’ beliefs about the necessity and harmfulness of antidepressants. Ann Fam Med. 2008;6(1):23–29. doi:10.1370/afm.759
43. Vankova B, Mala-ladova K, Kubena AA, et al. Immunosuppressive therapy related adherence, beliefs and self-management in kidney transplant outpatients. Patient Prefer Adherence. 2018;12:2605–2613. doi:10.2147/PPA.S184166
44. Butterworth JE, Campbell JL. Older patients and their GPs: shared decision making in enhancing trust. Br J Gen Pract. 2014;64(628):e709–e718. doi:10.3399/bjgp14X682297
45. Zhang J, Zhang WH, Xu LY, et al. The status and influencing factors of beliefs about medicines in breast cancer patients on endocrine therapy. J Nurs Sci. 2016;31(20):18–21. doi:10.3870/j.issn.1001-4152.2016.20.018
46. Wan B, Cheung W, Ball PA, et al. Beliefs about medicines among Hong Kong hospital outpatients. Int J Pharm Pract. 2017;25(6):447–453. doi:10.1111/ijpp.12353
47. Lv Y, Li Z, Han MY, et al. The reliability and validity of the Chinese version of beliefs about medical questionnaire am on elderly patients with depressive disorder. Chin J Nurs. 2014;49(4):389–393. doi:10.3761/j.issn.0254-1769.2014.04.001
48. Levic M, Bogavac-stanojevic N, Ubavic S, et al. Pharmacotherapy literacy level and predictors of low literacy among diabetes mellitus type 2 patients in Serbia. BMC Public Health. 2023;23(1):1822. doi:10.1186/s12889-023-16639-y
49. Li R. Elder depression, anxiety and cognitive function state, influencing factors and their relationships analysis. China Health Ind. 2015;12(15):139–140. doi:10.16659/j.cnki.1672-5654.2015.15.019
50. Bünemann M, Bauer-hohmann M, Klewitz F, et al. Beliefs about immunosuppressant medication and correlates in a German kidney transplant population. J Psychosom Res. 2020;132:109989. doi:10.1016/j.jpsychores.2020.109989
51. Horne R, Chapman SC, Parham R, et al. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journa-l.pone.0080633
52. Wu J, Shen J, Tao Z, et al. Self-efficacy as moderator and mediator between medication beliefs and adherence in elderly patients with type 2 diabetes. Patient Prefer Adherence. 2023;17:217–226. doi:10.2147/PPA.S382362
53. Tibaldi G, Clatworthy J, Torchio E, et al. The utility of the Necessity-Concerns Framework in explaining treatment non-adherence in four chronic illness groups in Italy. Chronic Illn. 2009;5(2):129–133. doi:10.1177/1742395309102888
54. Semahegn A, Torpey K, Manu A, et al. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
55. Yoo SH, Kim GG, Kim SR, et al. Predictors of long-term medication adherence in stroke survivors: a multicentre, prospective, longitudinal study. J Clin Nurs. 2023;32(1–2):58–70. doi:10.1111/jocn.16472
56. Budiman T, Snodgrass K, Komatsu CA. Evaluation of pharmacist medication education and post-discharge follow-up in reducing readmissions in patients with ST-Segment Elevation Myocardial Infarction (STEMI). Ann Pharmacother. 2016;50(2):118–124. doi:10.1177/1060028015620425
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.