")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Knowledge, Attitudes, and Practices Among Middle-Aged and Elderly Population Towards Ultrasound Screening for Strokes
Authors Wang W, Peng Y, Tang K, Zheng Z, He L, Yang S
Received 9 October 2023
Accepted for publication 3 January 2024
Published 9 January 2024 Volume 2024:17 Pages 147—157
DOI https://doi.org/10.2147/JMDH.S443865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Wenwen Wang,1,* Yuanyuan Peng,2,* Keqiang Tang,3 Ziwei Zheng,1 Lan He,1 Shaoling Yang1
1Department of Ultrasound Medicine, Shanghai Eighth People’s Hospital, Shanghai, 200235, People’s Republic of China; 2Department of Imaging Medicine and Nuclear Medicine, Anhui University of Science and Technology, School of Medicine, Huainan, Anhui, 232001, People’s Republic of China; 3Department of Intensive Rehabilitation, Shanghai Yangzhi Rehabilitation Hospital, Shanghai, 201619, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaoling Yang, Department of Ultrasound Medicine, Shanghai Eighth People’s Hospital, Shanghai, 200235, People’s Republic of China, Tel +86-18930240812, Email [email protected]
Purpose: This study aimed to assess the knowledge, attitudes and practices (KAP) among middle-aged and elderly population towards ultrasound screening for strokes.
Patients and Methods: This web-based cross-sectional study was conducted between March, 2023, and May, 2023 at Shanghai Eighth People’s Hospital. A self-designed questionnaire was developed to collect demographic information of middle-aged and elderly population and assess their knowledge, attitudes and practices toward ultrasound screening for strokes.
Results: A total of 552 participants enrolled in this study, among them 151 (27.36%) aged above 60 years old, 306 (55.43%) resided in rural area, 239 (43.30%) possessed educational attainment at the level of junior college, college or above. The mean knowledge, attitudes and practice scores were 5.53 ± 2.56, 40.22 ± 5.60 and 38.30 ± 7.38, respectively. Pearson’s analysis was performed to assess the relationship between knowledge, attitudes, and practices. It was shown that knowledge and attitudes were positively correlated (r = 0.544, P < 0.001), and knowledge and practices were also positively correlated (r = 0.404, P < 0.001). Additionally, there was a positive correlation between attitude and practice scores (r = 0.566, P < 0.001).
Conclusion: The results of this study demonstrate that the middle-aged and elderly population exhibited insufficient knowledge, positive attitudes, and moderate practices towards ultrasound screening for strokes. There is a need to improve the understanding of stroke risk factors, symptoms, and emergency measures among this population.
Keywords: knowledge, attitudes, practice, stroke, ultrasound imaging, middle-aged, elderly
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Akollo has been published for this article.
Introduction
Stroke constitutes a cerebrovascular event characterized by the abrupt interruption of cerebral blood supply, culminating in neurological dysfunction.1,2 In China, stroke holds a significant position within the continuum of mortality and disability. According to findings derived from the Global Burden of Disease Study 2019, China witnessed 3.94 million incident cases of stroke, alongside 28.76 million cases that were prevalent. Moreover, the year 2019 recorded 2.19 million fatalities attributable to stroke in the nation. Noteworthy, strokes are frequently entwined with a spectrum of deleterious consequences encompassing enduring disability, cognitive impairment, and heightened susceptibility to subsequent cardiovascular events. These ramifications collectively impose a substantial encumbrance upon healthcare infrastructures, inducing pronounced financial ramifications stemming from medical expenditure and a decrement in workforce productivity.3,4
In congruence with the advancing demographic shift, the onus of stroke impact intensifies. Older adults substantiate a considerable segment of stroke victims, amplifying the urgency for effective preemptive strategies.4,5 Amid these countermeasures, ultrasound screening has surged to prominence attributed to its non-invasive, expeditious, and precision-laden diagnostic prowess.6,7 Timely detection affords opportune interventions that serve to alleviate the gravity of stroke sequelae and enhance patient prognoses.8
Nevertheless, notwithstanding the manifest merits of ultrasound screening, an appreciable cognition void persists among the middle-aged and elderly demographic pertaining to its pivotal role in stroke prevention.6,9 Constrained awareness coupled with incomplete discernment of ultrasound’s functional significance engenders suboptimal utility of this diagnostic modality. This informational dearth impedes proactive embracement of preemptive practices, thereby thwarting efficacious stroke risk abatement within this susceptible cohort.
The Knowledge, Attitudes, and Practices (KAP) paradigm furnishes a methodical apparatus to fathom the intricate interplay between knowledge assimilation, attitudes, and pragmatic behaviors.10,11 Within the medical milieu, KAP investigations elucidate determinants that sway health-related decision-making and conduct. By scrutinizing participants’ comprehension of ultrasound’s pivotal role in stroke preemption, their predispositions towards preventative protocols, and their tangible adherence to screening regimens, this framework yields insights into the obstacles and catalysts governing the incorporation of ultrasound screening within the middle-aged and elderly population.
The present investigation aspires to bridge this extant hiatus via a comprehensive exploration of KAP factors that bear upon the integration of ultrasound screening for stroke prevention amidst the middle-aged and elderly populace. Through the identification of misconceptions, hurdles, and potential incentivizing agents, this study endeavors to furnish discernment that informs precisely targeted pedagogic interventions, thereby fomenting cognizance and fostering the embrace of ultrasound screenings.
Materials and Methods
Study Design and Subjects
This cross-sectional study was conducted between March, 2023, and May, 2023 at Shanghai Eighth People’s Hospital. The study participants were middle-aged and elderly population. The study was approved by the Ethics Committee of Shanghai Eighth People’s Hospital (approval No. 2023–043-003), and all participants provided informed consent.
The inclusion criteria were as follows:1) age above 45years 2) fluent in Chinese 3) willing to provide informed consent to participate in the study.
The exclusion criteria were as follows: 1) diagnosed cognitive impairments (eg, dementia, severe memory deficits) that could affect their ability to respond accurately. 2) individuals with severe medical conditions that may hinder their ability to participate (eg, terminal illnesses, critical care).
Questionnaire
The questionnaire was developed with guidance from 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack12 and relevant literatures.9,13 The first draft was revised with input from senior experts in stroke prevention and treatment and then pilot tested on a small scale (n=53), resulting in a Cronbach’s alpha coefficient value of 0.902, indicating good internal consistency.
The final questionnaire was presented in Chinese and encompassed four dimensions: demographic details, knowledge, attitudes, and practices. The demographic section encompassed 13 items, while the knowledge, attitude, and practice segments comprised 10 items each. The knowledge items were scored 1 point for a correct answer and 0 points for incorrect answers, resulting in a possible score range of 0–10. The attitude items scored on a five-point Likert scale ranging from very positive (5 points) to very negative (1 point), with a possible score range of 10 to 50. The practice items also scored on a five-point Likert scale, ranging from always (5 points) to never (1 point), with a possible score range of 10 to 50.
Data collection was facilitated through an online questionnaire deployed on the Sojump platform (http://www.sojump.com). Dissemination of the online survey transpired through diverse social media conduits, comprising WeChat, online forums, and web links. In order to forestall redundancy, a mechanism employing IP restrictions was enacted, thereby warranting singular survey completion per unique IP address.
Statistical Analysis
STATA 17.0 (Stata Corporation, College Station, TX, USA) was used for statistical analysis. The continuous variables was expressed as mean±SD, and the categorical variables was expressed as n (%). The continuous variables conformed to a normal distribution were tested by the t-test or ANOVA. The structural equation model (SEM) of knowledge, attitudes and practices among middle-aged and elderly population towards ultrasound screening for strokes was constructed with AMOS 24.0 (IBM, NY, United States). The model fitting was evaluated with CMIN/DF (Chi-square fit statistics/degree of freedom), RMSEA (root mean square error of approximation), IFI (incremental fix index), TLI (Tucker-Lewis index) and CFI (comparative fix index). Two-sided p<0.05 were considered statistically significant.
Results
A total of 552 participants enrolled in this study, among them 151 (27.36%) aged above 60 years old, 306 (55.43%) resided in rural area, 239 (43.30%) possessed educational attainment at the level of junior college, college or above. The mean knowledge, attitudes and practice scores were 5.53 ± 2.56, 40.22 ± 5.60 and 38.30 ± 7.38, respectively (Table 1).
 |
Table 1 Sociodemographic Characteristics and KAP Scores |
The three knowledge items with the highest correctness rates were as follows: “The rehabilitation programs for stroke victims include training in limb function, language skills, cognitive functions, and psychological recovery”. (K6) with a correctness rate of 79.71%, “The optimal timing for administering thrombolysis after a stroke” (K5) with a correctness rate of 77.54%, “The ultrasound screening method uses echo reflection imaging of ultrasound in human tissues”. (K8) with a correctness rate of 74.28%. The three items with the lowest correctness rates were “The risk factors for stroke”. (K2) with a correctness rate of 5.98%, “The emergency measures in the event of a stroke”. (K3) with a correctness rate of 12.50%, “The symptoms of a stroke”. (K1) with a correctness rate of 30.62% (Table 2).
 |
Table 2 Knowledge |
Meanwhile, a significant majority of the participants (87.50%) strongly agreed/ agreed that they bear the responsibility of self-initiated stroke (A1). 84.96% of them strongly agreed/ agreed that disseminating information about stroke and ultrasound screening through public media and the community holds (A5). Moreover, 81.88% of them strongly agreed/ agreed that they have the willingness to acquire knowledge about stroke ultrasound screening through online resources (A2). However, in the previous study, still about a quarter of them (25.91%) mistakenly believe that ultrasound screening is harmful (A7) (Table 3).
 |
Table 3 Attitudes |
Furthermore, 65.95% of the participants reported that they are very likely/likely to take proactive steps to acquire knowledge towards stroke prevention and treatment from diverse sources (P1). 71.56% of them reported that they purposefully undertake stroke prevention measures, which encompass dietary control, regular exercise, and lifestyle enhancement (P4). 57.42% claimed that they consciously seek understanding of emerging ultrasound screening technologies for stroke, such as ultra-microvascular imaging (P9) (Table 4).
 |
Table 4 Practices |
Pearson’s analysis was performed to assess the relationship between knowledge, attitudes, and practices. It was shown that the knowledge and the attitudes were positively correlated (r = 0.544, P < 0.001), and knowledge and practices were also positively correlated (r = 0.404, P < 0.001). Additionally, there was a positive correlation between attitude and practice scores (r = 0.566, P < 0.001) (Table 5).
 |
Table 5 Pearson’s Analysis |
Based on the results of the Pearson’s analysis, the structural equation model was established to further investigate whether middle-aged and elderly population’s knowledge and attitude toward ultrasound screening for strokes affect their practice, whether attitude plays an intermediary role between knowledge and practice, and whether knowledge can directly affect their practice according to the KAP theory. It also investigated the effect of other factors including “marital status”, “physical exercise frequency”, and “monthly income per capita” on the three dimensions mentioned above (Figure 1).
Hypothesis 1: The path coefficient from knowledge to attitudes is 1.193 (P < 0.001), which indicates that middle-aged and elderly population’s knowledge level is positively and significantly associated with their attitudes. Hypothesis 2: The path coefficient from knowledge to practice is 0.410 (P < 0.001), which indicates that their knowledge level is positively and significantly associated with their practices. Hypothesis 3 The path coefficient from attitude to practice is 0.656 (P < 0.001), indicating that the middle-aged and elderly population’s attitude was positively associated with practices.
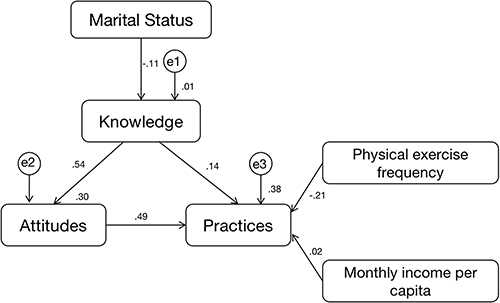 |
Figure 1 Structural equation modeling. |
The effect of other factors including “marital status”, “physical exercise frequency”, and “monthly income per capita” on the three dimensions mentioned above were also investigated (Table 6).
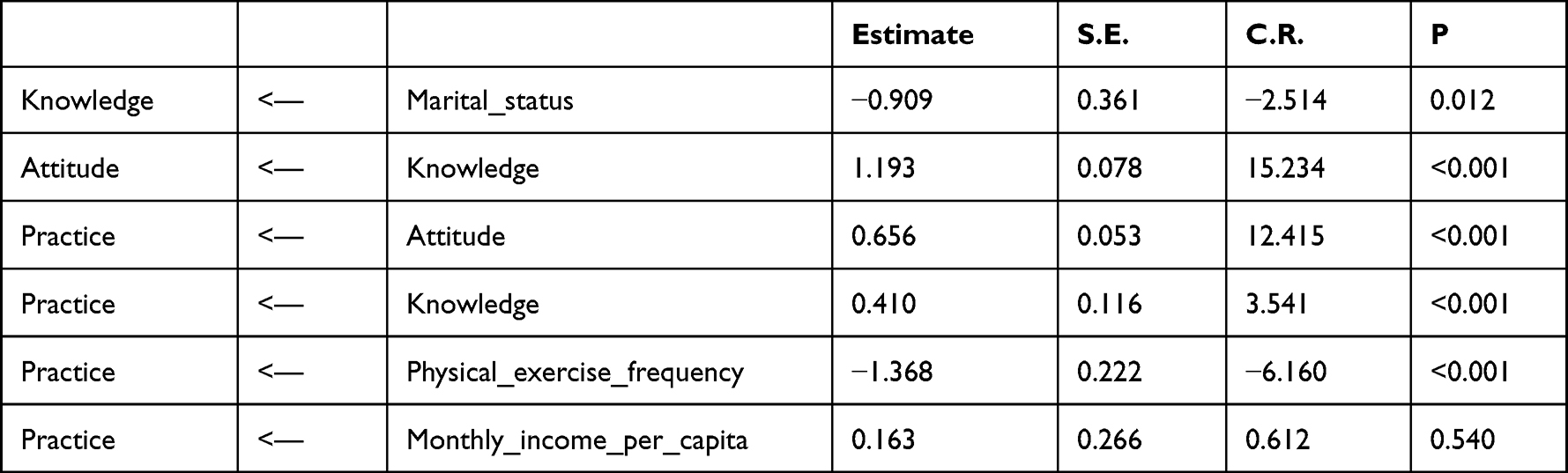 |
Table 6 Test Results of the Hypothesis |
The fitting index of the structural model (CMIN/DF = 0.949; RMSEA<0.001; IFI = 1.001; TLI = 1.002; CFI = 1.000) outperformed the respective threshold value, signifying that the data fit the structural model satisfactorily (Table 7).
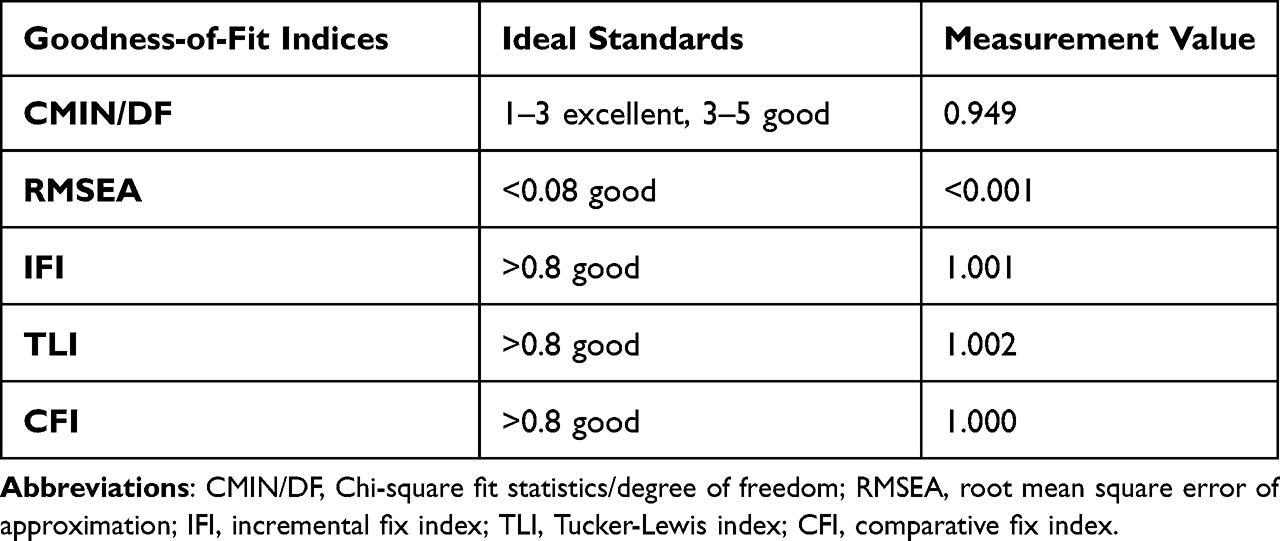 |
Table 7 Model Fitness Indices for the KAP Structural Equation Model |
Discussion
The findings of this study illustrate that the middle-aged and elderly population residing in Shanghai manifest insufficient knowledge, positive attitudes, and moderate practices towards ultrasound screening for strokes. There exists a requisite for enhancing comprehension pertaining to stroke risk factors, symptoms, and urgent interventions within this cohort.
The previous study revealed a spectrum of understanding across various domains encompassing stroke symptoms. The investigation unearthed areas of concern. Participants displayed comparatively diminished knowledge pertaining to stroke risk factors (K2) and techniques of ultrasound screening (K8), factors that may influence their grasp of stroke prevention and screening. Additionally, while a heightened awareness was observed concerning the optimal timing for post-stroke thrombolysis (K5) and the role of ultrasound screening (K9), instances of misconceptions or inadequate comprehension were still prevalent. The findings of the prior investigation are consistent with those of a cross-sectional study encompassing 228,240 adults who engaged in the 2017 Korean Community Health Survey.14 Within this study, there was a notable deficiency in the awareness of symptoms associated with stroke and heart attacks. In a parallel vein, an integrative assessment of published studies concerning stroke cognition and consciousness was undertaken by querying electronic bibliographic repositories utilizing specified keywords, spanning the temporal interval from 1966 to 2008. This review unveiled a paucity in the comprehension of stroke identification and prevention within the surveyed populace.15 Similarly, in a study assessing the understanding of stroke in Spain, it was noted that a cohort of adolescents exhibited limited knowledge regarding cerebrovascular diseases.16 Hence, there exists a clear imperative for enhanced educational initiatives and awareness campaigns aimed at augmenting public enlightenment in these areas. Additionally, a compelling rationale emerges for integrating this knowledge into the school curriculum.
In the previous study, the outcomes underscored that a majority of respondents harbored a sense of responsibility for self-initiated stroke prevention (A1), expressed a readiness to acquire knowledge about ultrasound screening through diverse channels (A2), displayed interest in participating in ultrasound education initiatives (A3), and articulated an intent to engage medical practitioners in discussions about ultrasound screening (A4). However, noteworthy concerns also emerged. Some respondents held a fallacious belief that ultrasound screening bears potential harm (A7), an aspect possibly stemming from misconceptions about ultrasound technology, signifying an exigent need for more precise information dissemination. Moreover, although a majority of participants evinced the aspiration to advocate for ultrasound screenings for stroke prevention (A9), the actual realization of this intent may encounter certain constraints. An investigation focusing on interventions addressing racial/ethnic disparities in stroke prevention and treatment has delved into an examination of the social determinants of health as well as the factors contributing to racial/ethnic disparities in healthcare. The study presents a concentrated synopsis of specific interventions designed to mitigate stroke risk factors, enhance recognition of stroke symptoms, and facilitate access to stroke care. These interventions are poised to effectively diminish discrepancies in stroke fatality rates among different racial and ethnic groups. Additionally, the study deliberates on areas of insufficient understanding and charts potential trajectories for future research.17 To more effectively expedite stroke prevention and control, sustained endeavors in public awareness and education are indispensable for instilling accurate attitudes and convictions.
As for the tangible practices associated with ultrasound screening for strokes, the study identified a spectrum of proactive behaviors exhibited by respondents. For instance, they evinced a willingness to glean knowledge from diverse sources (P1), conveyed an inclination to initiate communication with medical professionals to arrange appointments for ultrasound screening (P2), and displayed enthusiasm for participation in educational initiatives centered around ultrasound screening (P3). However, practical challenges also came to the fore. Despite intentions, certain respondents might encounter impediments in initiating discussions about ultrasound screening with medical practitioners or actively participating in the establishment of health records (P7, P10). Additionally, some respondents displayed a limited awareness of emerging ultrasound screening technologies (P9), underscoring the need for heightened public education. A study focusing on the prevention, management, and rehabilitation of stroke in low- and middle-income countries has recommended that individuals grappling with a persistent condition such as stroke might necessitate lifelong pharmaceutical intervention, the maintenance of a particular lifestyle, acquisition of self-management proficiencies, and robust caregiver and family backing. These measures are imperative for attaining optimal health outcomes. In this regard, rehabilitation serves to ameliorate the physical, speech, and cognitive faculties of stroke-afflicted individuals.18 Furthermore, an investigation into the efficacy of a self-management intervention for stroke risk among adults with prehypertension has demonstrated that the implementation of such an intervention is practicable and correlates with enhanced self-administration of stroke risk determinants. This positive association is especially notable in the context of primary stroke prevention within the prehypertensive populace.19
This study has several limitations. Primarily, the utilization of self-reported data introduces the potential for recall bias and subjectivity, thus exerting an influence on the veracity of responses. Additionally, the study’s cross-sectional design inherently precludes the establishment of causal relationships, consequently restricting the capacity to deduce causality links among knowledge, attitudes, practices, and demographic factors. Nevertheless, this study addresses a crucial gap, it not only evaluates middle-aged and elderly population’s level of knowledge but also provides an in-depth analysis of their attitudes and actual behaviors towards stroke preventive screening-areas that have been insufficiently explored in previous research.
Based on the findings of this study, there are potential avenues for future research. Primarily, future investigations may consider expanding the study’s participant demographic to encompass a broader age spectrum, specifically including the ultra-elderly population aged over 85 years. Given the notable differences in comorbidity profiles between this age group and others, it is conceivable that their KAP toward ultrasound screening for strokes may exhibit disparities. This subgroup may present unique challenges and opportunities that warrant further exploration. Secondly, it is worth contemplating the development of KAP-based intervention programs as an extension of the current research. By assessing KAP scores both before and after the implementation of these interventions, researchers can effectively gauge the efficacy of such programs in effecting behavioral and knowledge changes within the target population.
Conclusions
The comprehensive evaluation of knowledge, attitudes, and practices concerning ultrasound screening for strokes yields invaluable insights into the disposition of the middle-aged and elderly cohort towards embracing preventive protocols. This underscores the presence of a foundational platform that can facilitate the development of bespoke educational interventions targeted at addressing the specific knowledge lacunae pinpointed within this investigation.
Data Sharing Statement
All data generated or analysed during this study are included in this article.
Ethics Approval and Consent to Participate
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study participants were middle-aged and elderly population. The study was approved by the Ethics Committee of Shanghai Eighth People’s Hospital (approval No. 2023-043-003), and all participants provided written informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
Acknowledgment
The authors extend their gratitude to every participant involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shanghai Natural Science Foundation (No. 23ZR1447800); Molecular imaging diagnosis and treatment of vulnerable carotid plaques with dual-targeted functionalized ultrasound microbubbles and Shanghai Xuhui District’s Key Medical Disciplines, No. SHXHZDXK202319. The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Benesch C, Glance LG, Derdeyn CP, et al. Perioperative neurological evaluation and management to lower the risk of acute stroke in patients undergoing noncardiac, nonneurological surgery: a scientific statement from the American Heart Association/American Stroke Association. Circulation. 2021;143(19):e923–e946. doi:10.1161/CIR.0000000000000968
2. Owolabi MO, Thrift AG, Mahal A, et al. Primary stroke prevention worldwide: translating evidence into action. Lancet Public Health. 2022;7(1):e74–e85. doi:10.1016/S2468-2667(21)00230-9
3. Wang YJ, Li ZX, Gu HQ, et al. China stroke statistics: an update on the 2019 report from the national center for healthcare quality management in neurological diseases, China national clinical research center for neurological diseases, the Chinese Stroke Association, national center for chronic and non-communicable disease control and prevention, Chinese Center for disease control and prevention and institute for global neuroscience and stroke collaborations. Stroke Vasc Neurol. 2022;7(5):415–450. doi:10.1136/svn-2021-001374
4. Wu S, Wu B, Liu M, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019;18(4):394–405. doi:10.1016/S1474-4422(18)30500-3
5. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the global burden of disease study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
6. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: results from a Nationwide Population-Based survey of 480 687 adults. Circulation. 2017;135(8):759–771. doi:10.1161/CIRCULATIONAHA.116.025250
7. Gutierrez J, Turan TN, Hoh BL, Chimowitz MI. Intracranial atherosclerotic stenosis: risk factors, diagnosis, and treatment. Lancet Neurol. 2022;21(4):355–368. doi:10.1016/S1474-4422(21)00376-8
8. Chao BH, Yan F, Hua Y, et al. Stroke prevention and control system in China: CSPPC-stroke program. Int J Stroke. 2021;16(3):265–272. doi:10.1177/1747493020913557
9. Tu WJ, Hua Y, Yan F, et al. Prevalence of stroke in China, 2013–2019: a population-based study. Lancet Reg Health West Pac. 2022;28:100550. doi:10.1016/j.lanwpc.2022.100550
10. Aldhamy H, Maniatopoulos G, McCune VL, et al. Knowledge, attitude and practice of infection prevention and control precautions among laboratory staff: a mixed-methods systematic review. Antimicrob Resist Infect Control. 2023;12(1):57. doi:10.1186/s13756-023-01257-5
11. Wahlen R, Bize R, Wang J, Merglen A, Ambresin AE, Zweigenthal VEM. Medical students’ knowledge of and attitudes towards LGBT people and their health care needs: impact of a lecture on LGBT health. PLoS One. 2020;15(7):e0234743. doi:10.1371/journal.pone.0234743
12. Kleindorfer DO, Towfighi A, Chaturvedi S, et al. Correction to: 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e483–e484.
13. Duering M, Biessels GJ, Brodtmann A, et al. Neuroimaging standards for research into small vessel disease-advances since 2013. Lancet Neurol. 2023;22(7):602–618. doi:10.1016/S1474-4422(23)00131-X
14. Han CH, Kim H, Lee S, Chung JH. Knowledge and poor understanding factors of stroke and heart attack symptoms. Int J Environ Res Public Health. 2019;16(19):19. doi:10.3390/ijerph16193665
15. Jones SP, Jenkinson AJ, Leathley MJ, Watkins CL. Stroke knowledge and awareness: an integrative review of the evidence. Age Ageing. 2010;39(1):11–22. doi:10.1093/ageing/afp196
16. Arboix A, Arboix-Alio A, Hernandez-Arrieta M. [Scant knowledge about cerebrovascular disease in a sample of teenagers]. Rev Neurol. 2003;37(5):500. Spanish.
17. Levine DA, Duncan PW, Nguyen-Huynh MN, Ogedegbe OG. Interventions targeting racial/ethnic disparities in stroke prevention and treatment. Stroke. 2020;51(11):3425–3432. doi:10.1161/STROKEAHA.120.030427
18. Yan LL, Li C, Chen J, et al. Prevention, management, and rehabilitation of stroke in low- and middle-income countries. eNeurologicalSci. 2016;2:21–30. doi:10.1016/j.ensci.2016.02.011
19. Song HY, Nam KA. Effectiveness of a stroke risk self-management intervention for adults with prehypertension. Asian Nurs Res. 2015;9(4):328–335. doi:10.1016/j.anr.2015.10.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.