")
Back to Journals » Clinical Optometry » Volume 14
Knowledge, Attitudes, and Perceptions Towards Hand Hygiene of Optometry Students Pre- and Peri-COVID-19 at a Tertiary Institution in Johannesburg, South Africa
Authors Richter SM , Barnard TG
Received 1 July 2022
Accepted for publication 13 September 2022
Published 27 October 2022 Volume 2022:14 Pages 195—205
DOI https://doi.org/10.2147/OPTO.S379659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Susarah Maria Richter,1 Tobias George Barnard2
1Department of Optometry, University of Johannesburg, Johannesburg, South Africa; 2Water and Health Research Centre, University of Johannesburg, Johannesburg, South Africa
Correspondence: Susarah Maria Richter, Department of Optometry, University of Johannesburg, P.O. Box 17077, Doornfontein, Johannesburg, 2028, South Africa, Tel +27 011 559 6716, Fax +27 011 559 6654, Email [email protected]
Purpose: Limited research has been completed relating to the knowledge, attitudes and practices (KAP) towards hand hygiene in optometry. The necessity of identifying possible gaps in the cycle of the optometric examination that may have an impact on standard hygiene practices is essential, especially seen in the context of the COVID-19 pandemic. The purpose of the study was to determine if optometry students’ KAP towards hand hygiene changed pre- and peri-COVID-19 to minimize the risk of possible infection it may have for their patients, family, and themselves.
Patients and Methods: A cross-sectional purposeful sample study was completed among optometry students at a training institution in Johannesburg, South Africa, pre- (2019) and peri-COVID-19 (2022). The WHO hand hygiene knowledge and perception questionnaires for health care workers were adapted and used in the current study. Statistical analyses were performed to test for significant changes between the two groups.
Results: There was a significant change (p < 0.01) in the use of alcohol-based hand rub (ABHR) in 2022 (87.2%) compared to 2019 (46.5%), although only 41% of students peri-COVID-19 (2022), were aware that a minimum of 20 seconds is required to effectively clean hands. Students, both pre-COVID-19 (63.8%) and peri-COVID-19 (81.8%) perceived performing a hand hygiene regime during an optometric examination to be problematic. A significant peri-COVID-19 (2022) change in perception (p < 0.01) regarding the importance of completing required hand hygiene practices in front of a patient during examination was seen.
Conclusion: The COVID-19 pandemic provided a unique opportunity to research a possible change in KAP towards hand hygiene practices in optometry students that have not been investigated before. Students were more aware of the impact of hand hygiene practices and the perception thereof, especially by patients and fellow students during the peri-COVID-19 (2022) period. An important finding was the difficulty that students experienced to perform a hand hygiene regime during an optometric examination.
Keywords: COVID-19, optometric examination, surface contamination, alcohol-based hand rub
Introduction
To study knowledge, attitude and practices are to determine how people “know about certain things, how they feel and also how they behave1”. It helps to study these aspects to use it when planning interventions and educational programmes.2 Research conducted in the fields of Optometry and Ophthalmology as it relates to hand hygiene practices is limited. When assessing knowledge, attitudes and practices (KAP) only, more information is available and these include that of contact lens use in South Africa;3 medical students using contact lenses;4 KAP of contact lens users towards contact lens wear in Ghana;5 KAP related to COVID-19 among patients presenting at eye care hospitals in South India;6 KAP regarding COVID-19 ocular manifestations in Saudi Arabia;7 KAP related to ocular prophylactic measures taken by medical students during COVID-19;8 KAP related to the assessment of childhood ocular disorders among primary health care workers (HCW’s) in Kenya9 and KAP related to hospital acquired infection (HAI) prevention in Northern Ethiopia.10
The KAP questionnaires used to collect data in these studies were self-developed questionnaires except for Kumar et al4 where an adapted version of the World Health Organization (WHO) knowledge questionnaire on hand hygiene for HCW’s11 was used. This questionnaire forms part of the WHO “My 5 Moments for Hand Hygiene” model often used to establish HH knowledge among HCW’s.12 No South African studies are available where KAP on hand hygiene practices have been studied in either Optometry or Ophthalmology, but recent research related to KAP among university nursing and optometry students was published in Oman13 where the WHO knowledge questionnaire on hand hygiene for healthcare workers11 was used. It is the first time that data can be compared in the same profession although not on the same continent and to the same extent. Hand hygiene is reported to be the most effective way to ensure adherence to health guidelines and to improve patient care.14 Compliance to hand hygiene (HH) standards in developed countries have been described to be as low as 40%.15 The average compliance reported with HH practices was approximately 40–60%16 among HCW’s in a tertiary hospital in the USA. Various predictors that may influence HH compliance have been published and include “being busy, forgetful and fear of having skin damage due to alcohol hand rub”, “having sore/dry hands” and the requirements to wear gloves during procedures,17 laziness and negligence,18 challenging placement of HH resources, excessive patient numbers, congestion of staff, the time it takes to complete the HH procedure19 and frequently entering and exiting the ward.16 There is often resistance to HH compliance, especially from medical students, and this may be related to “lack of knowledge, ignorance to the risks, misconceptions and poor hand hygiene compliance by role models20” and not enough attention given to educate medical students regarding HH practices and related aspects.21
When considering the impact gender has on HH, it was shown in Ethiopia that female students tended to have better adherence to HH protocols22 with similar results in hospital environments in Iran23 and Syria.24 Contrary to this, disinfectant use was higher among males (78.8%) than females (62%) in a study of HCW’s in a civil hospital in Pakistan.25 More concerning it was reported that the higher the level of study year,26 the less advanced the knowledge of HH appeared to be. Students appeared to be less knowledgeable about the practice of HH and how to apply it. It has been shown that the retention of HH and infection control knowledge are not being sustained through the years of study.26 Thus, if the requirements for HH and ICP’s are not repeated on a regular basis, retention of the information is reduced.
Literature highlights the necessity to study HH KAP in Optometry to identify possible gaps in the cycle of the optometric examination that may have an impact on standard hygiene practices, especially seen in the context of the COVID-19 pandemic. There may be an associated risk of COVID-19 transfer to surfaces and the eye, and knowledge and perceptions related to specific practices needed to be established. The purpose of the current study was to determine if optometry students’ KAP towards hand hygiene changed pre- and peri-COVID-19 to minimize the risk of possible infection for their patients, family, and themselves.
Materials and Methods
A cross-sectional purposeful sample study was completed in 2019 and 2022 among third- and fourth year students registered for the bachelor’s in optometry degree at a tertiary institution in Johannesburg, South Africa to determine their knowledge, attitudes, and perceptions towards hand hygiene. Ethical approval for the study was obtained from the Research Ethics Committee (REC-01-168-2018) of the Faculty of Health Sciences and approval from the University of Johannesburg as enrolled students and employed staff were involved in the study. Guidelines and principles as stipulated by the Declaration of Helsinki for research were followed.
The purpose of the study was explained to students, and they were informed that their participation was voluntary and withdrawal from the study could take place at any time. It was made clear that confidentiality and anonymity were guaranteed. Written consent was obtained from all students for participation in the study. It was also explained that if a student decided not to participate, it would not have an impact on the student’s academic nor practical performance. The students were then requested to complete the “Hand Hygiene Knowledge, Attitude and Perception Questionnaire for Health-Care Workers” that was adapted from the original “Hand Hygiene Knowledge Questionnaire for Health Care workers11” and the “Perception Survey for Health Care Workers27”. The adapted research questionnaire was successfully used in a previous study by Blundell (2018)28 in a pre- and post-intervention study.
The wording of subsections of question 20 of the original WHO questionnaire11 was slightly altered to better represent the optometric clinic environment (and allow for better understanding), however it still represented the same requirements for the HH method required. “Before palpation of the abdomen” was changed to “Before palpation of the eye”; “Before giving an injection” was changed to “Before inserting a contact lens” and “After making a patient’s bed” was changed to “After examining the patient”. All answers were coded, values were assigned, and answers could not be traced back to the individual students. Data was transferred to a Microsoft Excel (2010) spreadsheet and all statistical analyses were conducted in IBM SPSS Statistics 22. Standard descriptive statistical analyses were completed on all data sets, including nonparametric methods of analysis, cross tabulations, tests for significance and geometric means, standard deviations, medians, and percentages. In all calculations, p < 0.05 was considered as the level of significance.
Results
The research questionnaire was completed by 71 optometry students in 2019 (n = 75; 94.7% response rate) and 78 students in 2022 (n = 80; 97.5% response rate) in their third and fourth year of study. No significant difference was seen between the distribution in numbers between the two groups (p = 0.779) of 2019 and 2022. Table 1 refers to a summary of age and gender between the third and fourth year students of 2019 and 2022.
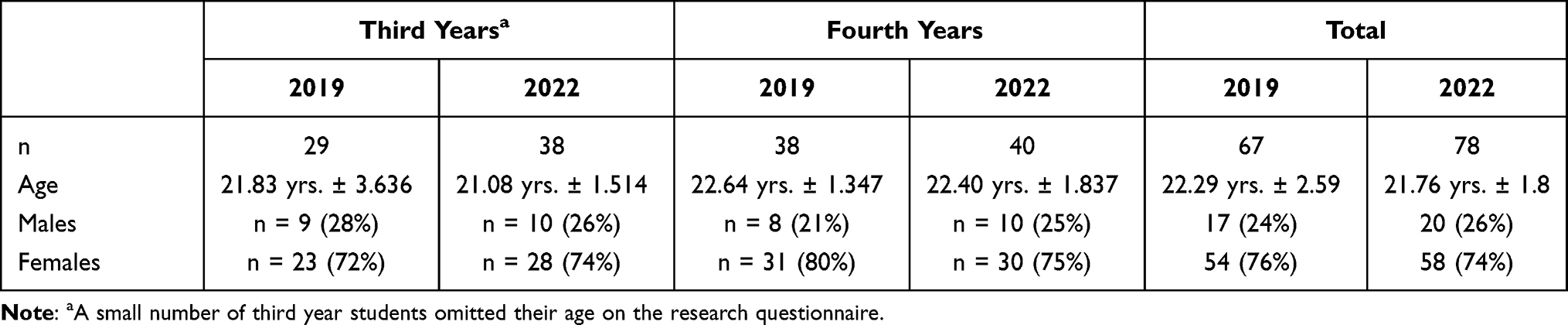 |
Table 1 Age and Gender of Third and Fourth Year Students in 2019 and 2022 |
The first question of the questionnaire required an answer from the participants relating to any training received in HH practices in the last three years and the second question was if the participant knew what the WHO “My 5 Moments for Hand Hygiene” (5MHH) referred to. Only 29.6% of students in 2019 indicated they received formal training in HH practices, which slightly improved to 34.6% in 2022. A decrease in the number of students being aware of the 5MHH was seen with the second question. Twenty-one percent of students in 2019 were aware of the 5MHH model, while only 11.5% indicated awareness of the model in 2022. There was no statistically significant difference present in the relationship between the answers provided (p = 0.172).
The mean knowledge percentage for the research questionnaire was calculated for 2019 and 2022. All answers to questions where a yes or no, true and false, or a specific answer to a question were required, were considered to calculate the mean knowledge percentage for each year. There were 27 answers to be considered. The mean HH knowledge score for the optometry students in 2019 was 50.98 ± 10.46% and in 2022, it was 50.65% ± 9.90%. Although no statistical difference was present between the knowledge score of the students in 2019 and 2022, there was less variation in the knowledge answers provided by the students in 2022 than in 2019.
The students’ routine use of an alcohol-based hand rub (ABHR) before seeing a patient was probed next. Figure 1 provides a graphic portrayal of the results obtained related to the routine use of ABHR between the years 2019 and 2022. The spread of answers between “yes” and “no” was fairly even in 2019, where slightly more students (53.5%) indicated that they did not make use of an ABHR for HH. This was an area of concern in 2019 as it was expected that students would clean their hands before commencing the consultation with a patient.
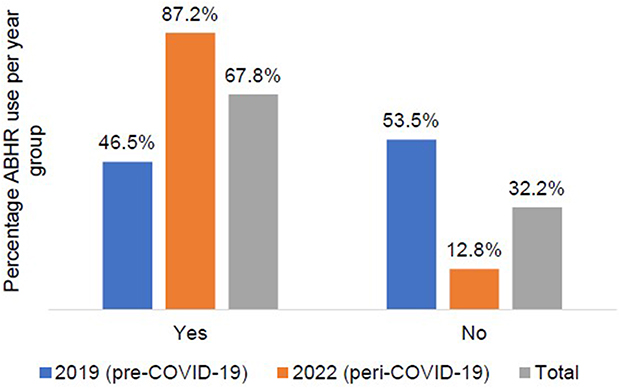 |
Figure 1 Students’ responses pre-COVID-19 (2019) and peri-COVID-19 (2022) to the routine use of alcohol-based hand rub (ABHR). |
There was a significant change in the routine use of ABHR in 2022 (p < 0.01). The majority of students (87.2%) indicated the routine use of an ABHR peri-COVID-19 (Figure 1). When the groups were probed regarding the minimum time required for an ABHR to have an effect to remove microbes from the hands, the following was obtained. Forty-four percent of students in 2019 indicated that 20 seconds is required for an ABHR to clean hands and slightly less students (41%) in 2022 indicated the same. It is interesting to note that although there was a significant increase in the use of ABHR among the students in 2022 (87.2% vs 46.5%), only 41% of the students knew the minimum required time of 20 seconds. There was also a significant difference in the association between the knowledge answers of the two groups if hand rubbing was more effective against germs than hand washing. According to the suggested answers by the WHO,29 this is a “true” statement29 and it is also suggested that hands should only be washed if it is visibly dirty.12 Significantly less students in 2022 believed that it was a true statement (44.6% vs 23.9%).
When identifying the source of germs responsible of HCAI’s, the correct knowledge option indicated by the WHO29 is that germs are “already present on or within the patient”. Only 28.1% of the group in 2019 was correct and it reduced noticeably to 16.7% in 2022. Surface contamination plays an important role in cross-contamination, especially in a clinical environment. Public awareness campaigns were introduced during the COVID-19 pandemic educating the general public on the dangers of transmission of the virus and the importance of washing hands, wearing a mask, and cleaning surfaces. Evidence is available to indicate that surface contamination is also contributing to the spread of disease but would theoretically be reduced if proper hand hygiene and mask wearing were performed. Slightly more than half of the group in 2019 (53.5%) provided the correct answer to the question which possible infections can be transferred from patients to the HCW’s if “glove use and hand hygiene practices were not in place”. Options were listed as “herpes simplex virus infection, MRSA colonization or infection, respiratory syncytial virus, and hepatitis B virus or all of the above” in the question. In 2022 (peri-COVID-19), only 50% indicated the correct answer and an increase in the choice “MRSA colonization or infection” was seen.
The perception questions related to HH were interspersed between the knowledge questions in an attempt to keep the students engaged throughout the completion of the questionnaire. Students felt strongly that HCAI’s have an impact on the patient’s clinical outcome. In 2019 (pre-COVID-19), the total perception was 82.9% and in 2022 (peri-COVID-19) it was 82.9% as well, although the perception in 2022 shifted from a “high” impact to a “very high” impact. The majority of students in 2019 (95.8%) indicated that HH had a “high” or “very high” effectiveness in the prevention of HCAI’s. Similarly in 2022, 97.5% of students report that HH may be effective in the prevention of HCAI’s. The next question in the perception questionnaire surveyed the students’ perception related to the importance that the institution may attach to HH practices and patient safety measures. In 2019, only 19.7% indicated a “high priority” perception and 16.9% a “very high priority” perception. In 2022, the perception of the students increased to 42.3% (“high”) and 42.3% (“very high”) respectively (Figure 2). A significant difference in the perception of students between 2019 and 2022 related to the importance of HH practices and patient safety at the institution (p < 0.01) were seen.
 |
Figure 2 Summary of student perceptions related to the importance of hand hygiene practices and patient safety at the institution, comparing pre-COVID-19 (2019) and peri-COVID-19 (2022). |
The ensuing questions probed the perception of the students related to the fact that they, themselves, performed HH. The first question related to the importance the student attached to the belief of fellow students/colleagues that proper HH practices were being performed by the individual. The response was formulated in a Likert-scale changing from 1 = no importance to 5 = very high importance. A notable shift was seen towards the higher end of the scale peri-COVID-19 (2022) in comparison with pre-COVID-19 (2019). In 2019, only 52.9% perceived that their fellow students and/or colleagues would find it noteworthy to see that HH was performed. In 2022, this perception shifted to 79.2% (Figure 3). A statistically significant difference was found in the change of perception of the students between 2019 and 2022 (p = 0.001).
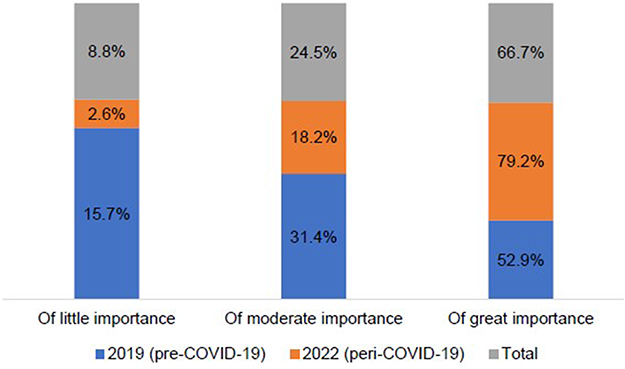 |
Figure 3 Students’ perception of the value that is being attached to fellow students (colleagues) watching hand hygiene practices being performed, comparing pre-COVID-19 (2019) and peri-COVID-19 (2022). |
The perception of the students related to the importance patients may attach to HH being performed were probed next also using the Likert-scale as with the previous question. In 2022, 79.2% of the group indicated that the patient would attach great importance to the fact that HH practices were being performed while they were present and in 2019, this was only 40.8% (Figure 4). The reason for this perception is not apparent as students were not required to provide any motivation, but the constant reminder of hand sanitization and surface cleaning in general due to COVID-19 (2020–2022) may have had an impact on the perception of general HH practices in the current group of students (2022). A statistically significant difference in the perception of students was seen (p < 0.01).
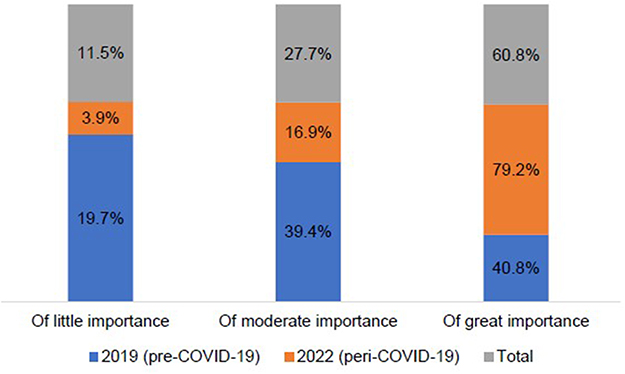 |
Figure 4 The perception of students related to the importance that patients may attach to watching hand hygiene practices being performed, comparing pre-COVID-19 (2019) and peri-COVID-19 (2022). |
The remaining question related to perception of HH practices was that the students should rate their perception of the effort that goes into performing HH when they have to care for their patients. The answers were in a Likert-scale format from 1 = no effort to 5 = big effort. A statistically significant difference (p = 0.035) was found between the perception of students in terms of the effort related to performing HH when examining patients pre-COVID-19 (2019) and peri-COVID-19 (2022) (Figure 5).
 |
Figure 5 The students’ perception related to the effort they have to put in by performing hand hygiene practices while examining patients, comparing pre-COVID-19 (2019) and peri-COVID-19 (2022). |
It is concerning to note that there was a significant increase in the perception of students in 2022 (81.8%) that it took effort to perform a hand hygiene regime while examining their patients. The majority of students during pre-COVID-19 (2019; 63.4%) indicated the same and a statistical difference was found in the perception of students related to this.
Discussion
Knowledge, attitudes, and practices (KAP) of hand hygiene in Optometry, using the WHO questionnaires11,27 have not been studied specifically. Two studies could be identified where KAP of HH in particular were investigated among optometry students. The research was completed where nursing and optometry students in their final year of study at a university in Oman participated.13 The other study where optometry students participated was when knowledge and attitude towards infection control was studied at a college in India.30
The response rate obtained in the current study (94.7% and 97.5%) compares favourably with a study on HH practices of medical students in the Netherlands31 where a response rate of 97% was achieved and a 98% response rate at the University of the Free State, South Africa32 where HH practices among medical students were also studied. When the KAP questionnaire was distributed among optometry students in Oman,13 a response rate of 98.57% was achieved.
In the current study, the gender breakdown in the study was 76% female and 24% male students in 2019, and 74% female and 26% male students in 2022. This correlates with the data reported on the perception of optometry students upon graduating in South Africa33 consisting of 72.7% female and 27.3% male students. When evaluating the introduction of experiential learning in the training of undergraduate optometry students at the University of the Free State, South Africa, 70.59% of the sample was female and 29.41% was male students.34 Only 29.6% of the students in 2019 specified that they received formal training in HH practices in the past three years of their study, which improved slightly to 34.6% in 2022. This is concerning as optometry students get acquainted with the concepts of hygiene and clinical practice in their first academic year of study and although students in 2019 were not affected by the COVID-19 pandemic and increased hand hygiene awareness, the students in 2022 was exposed to this and should have reported accordingly.
Nair et al35 reported that 79% of the medical and nursing students at a tertiary care centre in India, indicated that they received formal training in hand washing. When knowledge of HCW’s related to HH was reported at a teaching hospital in Ghana, 77.3% of participants indicated they received formal training.36 Setati (2019)37 showed that 57.1% of the respondents taking part in a KAP study related to HH in Limpopo, South Africa received training in hand washing and 60.4% indicated that the training was part of the undergraduate programme at their respective training institutions. Ugwu et al38 found that 53.2% of the healthcare workers at a university teaching hospital in Nigeria did not receive any training related to HH in the past three years. The results obtained in the current study are significantly lower than any of the reported research and will be communicated to the programme coordinator of the optometry course. The reason for the low percentages reported by the students has to be investigated (29.6% for 2019 and 34.9% for 2022). It may mean that there is no follow through in later academic years of study on HH training and it should be emphasized during each year. A possible solution might be to visually prompt students about HH practices and the specific procedure by placing posters in all examination rooms.
Likewise, only 21.1% (2019) and 11.5% (2022) of students in the current study reported that they were cognizant of what the 5MHH model was. This is concerning as HH practices form part of the introduction to basic clinical protocol, and the supposition was that students should at least be aware of the process or know the basics of when to wash/clean their hands and the minimum time required. The 5MHH model includes the following HH actions: a) before touching a patient, b) before an aseptic/clean procedure c) after a body fluid risk d) after touching a patient and e) after touching patient surroundings.39 It is concerning to see an actual decline in reporting of what the 5MHH model is in 2022. Literature explains that the 5MHH model may not be transferrable and not accommodative of all patients’ needs in different clinical environments.40 This may also be interpreted that the 5MHH model may not be applicable in its current format in all clinical environments. It has been reported that microbials present on the patient may already have been transferred in the waiting area and/or screening area before the patient even entered the examination area.40 It may even happen that certain “moments” are completely ignored or seen as “not that important” by the HCW. The apparent “lack of knowledge” relating to the 5MHH model can conceivably be explained as not being specific and directly applicable to an optometric clinical environment and that the students may not have paid much attention to it. The observation model developed in this study41 can possibly be used (with further adaptations) to explain the 5MHH model to incoming first year students in such a way to understand how to apply HH practices as required in an optometric environment.
A steep increase though, was seen between 2019 (57.7%) and 2022 (73.1%) in the incorrect option of “the clinic/hospital environment (surfaces)” in the current study as a possible cause of HCAI’s. Another study in Sudan42 noted that 54.2% of nurses and doctors also indicated that HCAI’s may be due to microbes present on environmental surfaces. Similar results were obtained from chiropractic students where 54.4% indicated that it may be the hospital (clinic) environment (surface) contributing to HCAI’s.28 No explanation can be provided for the significant change in 2022 towards surfaces being the cause of HCAI’s. The substantial increase in this opinion can possibly be interpreted in the background of the continued emphasis that the SARS-CoV-2/COVID-19 virus can stay alive on certain surfaces43 over a period of time, and it was reported that it was stable enough to be detected for up to 72 hours on steel and plastic.44 It is however an area of concern as students should understand how the transfer of micro-organisms occur and should be aware of patient-clinician transfer.
In the current study, 63.5% (2019) and 63.9% (2022) of the students indicated that it is true that hand rubbing would be more rapid in cleaning hands than hand washing. A similar finding (66.3%) was reported among nurses in Saudi Arabia45 while an observational study of HH practices in Senegal46 noted that hand rubbing occurred 80.3% of the time when HH actions were directly observed, although HH actions according to the 5MHH model occurred only 36.1% of the time. It is surprising however to see that there was not an increase in the knowledge related to hand rubbing with ABHR, as one would assume that the requirement of hand sanitization with the COVID-19 pandemic would possibly have influenced the opinion of the 2022 group. A recent review appeared47 discussing the fact that although hand rubbing with ABHR has been the standard in almost all healthcare settings, the influence of the application time, hand size, the volume of ABHR used and the friction to the hand have been insufficiently studied. The conclusion was that the afore mentioned factors should be considered in further HH research, but that it was insufficient to influence the WHO recommendations for ABHR.39
Thirty-one percent of HCW’s at the teaching hospital South Africa37 indicated that ABHR should be used for at least 20 seconds, while it was reported that only 8.7% of HCW’s in Ghana36 indicated the correct minimum time of 20 seconds for an ABHR to destroy most microbes on the hands. The current study reported slightly higher knowledge of the minimum time for ABHR to have an effect (44.3% in 2019 and 41% in 2022). It is still concerning seen in the light that students received training before commencing with examining patients in the clinic and proper HH practices is one of the basic requirements. It would seem that there is a probable gap between what is being provided as theoretical content and what students internalise and express as personal practice and/or experience.
There also appears to be a potential gap between knowledge related to the use of ABHR and the perception if HH practices are effective against preventing HCAI’s. Pre-COVID-19 (2019), 95.8% of students and peri-COVID-19 (2022), 97.5% of students indicated that they perceived HH to be either highly or very highly effective against preventing HCAI’s. This, however, is in contrast with their knowledge that a minimum of 20 seconds is required to remove most microbes from the hand. The perception related to HCAI’s reported in the current study compares favourably with that reported for HCW’s in Saudi-Arabia (2021)48 where 95.4% perceived HH to be effective against HCAI’s. Following on from the discussion of how long to use an ABHR and also if hand rubbing or hand washing would be the correct HH practice, the response to the question of if the individual used ABHR regularly is appropriate. In the current study only 46.5% of the students in 2019 (pre-COVID-19) provided a positive response. The response increased significantly to 87.2% in 2022 (peri-COVID-19) (Figure 1). It was a positive change seen in the setting of the COVID-19 pandemic, but in contrast with some of the previous responses of this group such as the minimum time required for ABHR to rid the hand of microbes or that 81.8% of the 2022 group (Figure 5) indicated that HH actions associated with patient care are a great effort to them. When considering the answer, one could include various variables such as the availability of hand sanitizer or ABHR, the ease of cleaning hands while busy examining a patient, the location of the sanitizer/hand rub/washing basin or the environment where the student has to examine the patient (the researcher's opinion). Examining a patient in a clinic environment opposed to an outreach clinic where the student has to make use of basic equipment and a non-technology friendly environment, may prove to be challenging to perform HH properly. The observation thus of the HH practices is crucial to see how the students’ perception of effort correlated with their actual practice of HH in the clinical environment.
It has been shown that the retention of HH and infection control knowledge are not being sustained through years of study. Thus, if the requirements for HH and infection control are not repeated on a regular basis, retention of the information is reduced. The suggestion is that HH modules should be included in each year of study during the course of a medical student’s learning programme.20 The current study found a mean HH knowledge score of 50.98% in 2019 and 50.65% in 2022. This would classify as moderate HH knowledge, which when compared with other research studies are fairly similar. Hand hygiene knowledge during COVID-19 in Saudi-Arabia48 was reported as moderate at 57.8%, and moderate among under-graduate students in India at 69.1%.49 One would have expected that HH knowledge should have been higher for the 2022 group due to their exposure in the COVID-19 pandemic, but it was not the case.
Conclusion
The KAP of optometry students towards hand hygiene have not been studied and by using the combined adapted research questionnaire, it provided new information related to KAP of HH pre-COVID-19 and peri-COVID-19 among optometry students. Some interesting results were obtained, including that of the definite change in perception towards HH practices and the impact on patients in the peri-COVID-19 group, despite them finding HH practices an effort when examining patients. Hand hygiene was one of the important aspects emphasized in the prevention of the spread of the COVID-19 pandemic at departmental, institutional, and national level since 2020. Many other reasons may have had an influence on the change in perception of the students related to the importance of HH at the institution, but the only significant difference during this time period was the COVID-19 pandemic. No changes were made to the curriculum, although students were receiving online lectures during the period April 2020 until November 2021. It is important to monitor if the significant change in perception and use of ABHR’s plateau or if it decreases again as students become accustomed or desensitized to the “new normal” of required HH practices and wearing a facial mask when working with patients in the clinic.
Abbreviations
5MHH, “My 5 Moments for Hand Hygiene” model; ABHR, Alcohol-based hand rub; HCAI’s, Healthcare-associated infections; HCW’s, Healthcare workers; HH, Hand hygiene; ICP’s Infection control protocols; KAP, Knowledge, attitudes, and perceptions; WHO, World Health Organization.
Data Sharing Statement
Data supporting the results are available from both authors and can be obtained via email. Data and results presented in the publication were collected as part of doctoral studies in Optometry.
Ethical Approval and Informed Consent
Ethical approval for the study was obtained from the Research Ethics Committee (REC-01-168-2018) of the Faculty of Health Sciences and from the University of Johannesburg as enrolled students and employed staff were involved in the study. Signed informed consent was obtained from all students before the research study commenced. Guidelines and principles as stipulated by the Declaration of Helsinki regarding research were followed.
Funding
No financial support was received for the completion of this part of the research study.
Disclosure
The authors report no conflicts of interest or financial interest in this work. Data and results obtained from the study form part of DPhil (Optometry) studies.
References
1. Kaliyaperumal K. Guideline for Conducting a Knowledge, Attitude and Practice (KAP) Study. AECS Illumination; 2004. Available from: http://v2020eresource.org/content/files/guideline_kap_Jan_mar04.pdf.
2. Bonilla-Escobar FJ, Ocampo-Dominguez HH. Red eye: next steps for conducting research in knowledge, attitude and practice in ophthalmology. Int J Med Students. 2012;1(1):24–27. doi:10.5195/ijms.2013.21
3. Khoza N, Moodley T, Sokhulu S, et al. Knowledge, attitude, and practices of contact lens use in a South African adolescent population. Afr Health Sci. 2020;20(2):768–774. doi:10.4314/ahs.v20i2.29
4. Kumar TV, Ranjee PH, Farokh SE. Knowledge, attitude and practice of medical students using contact lenses. Indian J Clin Exp Ophthalmol. 2017;3(3):333–336.
5. Ocansey S, Ogbomo G, Abu EK, Morny EKA, Adjei-Boye O. Profile, knowledge, and attitude of contact lens users regarding contact lens wear in Ghana. Contact Lens Ant Eye. 2019;42:170–177. doi:10.1016/j.clae.2018.10.012
6. Christy JS, Kaur K, Gurnani B, et al. Knowledge, attitude, and practise toward COVID-19 among patients presenting to five tertiary hospitals in South India – a multicentre questionnaire-based survey. Indian J Ophthalmol. 2020;68:2385–2390. doi:10.4103/ijo.IJO_2522_20
7. Alsaedi MG, AlQahtani BS, Zahrani AK, Alshareef SE, Alzubaidy KA. Assessment of knowledge, attitude and practice regarding COVID-19 ocular manifestations in the western region of Saudi Arabia. Open Ophthalmol J. 2021;15:25–33. doi:10.2174/1874364102115010025
8. Varsha V, Ramachandra S. Awareness and knowledge of ocular prophylactic measures and hand hygiene among medical students in the wake of the pandemic-COVID-19. Trop J Ophthalmol Otolaryngol. 2020;5(6):138–143. doi:10.17511/jooo.2020i06.04
9. Mbogo SO, Kahaki K, Njambi L. Knowledge, attitude, and practice in assessment of childhood ocular disorders among primary health workers in Garissa district, Kenya. J Ophthalmol East Cent S Afr. 2016;20(1):12–20.
10. Gezie H, Leta E, Admasu F, Gedamu S, Abebe D, Debrnesh G. Health care workers knowledge, attitude and practice towards hospital acquired infection prevention at Dessie referral hospital, Northeast Ethiopia. Clin J Nurs Care and Prac. 2019;3:059–063. doi:10.29328/journal.cjncp.1001019
11. World Health Organisation. Hand hygiene knowledge questionnaire for health care workers; 2009. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control/hand-hygiene/monitoring-tools.
12. World Health Organisation. Hand hygiene technical reference manual. Geneve, Switzerland: Patient Safety. A World Alliance for Safer Patient Care; 2009. Available from: https://cdn.who.int/media/docs/default-source/integrated-health-services-(ihs)/hand-hygiene/monitoring/9789241598606_eng.pdf?sfvrsn=f0870e7e_11.
13. Ayyappan JP, Varghese V, Mohammed Ismail G. Assessment of knowledge, practices, and attitude of hand hygiene among university nursing and optometry undergraduate students in their final year of training. Malas J Pub Health Med. 2021;21(2):226–233. doi:10.37268/mjphm/vol.21/no.2/art.956
14. Vikke HS, Vittinghus S, Giebner M, et al. Compliance with hand hygiene in emergency medical services: an international observational study. Emerg Med J. 2019;36(3):171–175. PMID: 30692145; PMCID: PMC6580871. doi:10.1136/emermed-2018-207872
15. Ateiyero Y, Dyson J, Graham M. Barriers to hand hygiene practices among health care workers in sub-Saharan African countries: a narrative review. Am J Infect Control. 2018;47:565–573. doi:10.1016/j.ajic.2018.09.014
16. Woodard JA, Leekha S, Jackson SS, Thom KA. Beyond entry and exit: hand hygiene at the bedside. Am J Infect Control. 2019;47:487–491. doi:10.1016/j.ajic.2018.10.026
17. Foote A, El-Masri M. Self-perceived hand hygiene practices among undergraduate nursing students. J of Res Nurs. 2016;21(1):8–19. doi:10.1177/1744987115606959
18. Muiru HW. Knowledge, attitude, and barriers to hands hygiene practice: a study of Kampala International University undergraduate medical students. Int J Community Med Public Health. 2018;5(9):3782–3787. doi:10.18203/2394-6040.ijcmph20183564
19. Kumar R, Gupta PK, Sharma P, et al. Hand hygiene, attitude and barriers among health care workers at a tertiary care teaching hospital, Uttarakhand. Int J Health Sci Res. 2017;7(9):159–165.
20. Kaur R, Razee H, Seale H. Setting the right foundations: improving the approach used to teach concepts of hand hygiene to medical students. J Hosp Infect. 2017;95:355–358. doi:10.1016/j.jhin.2017.01.006
21. Modi OD, Kumar O, Solanki R, Modi J, Chandramani S, Gill N. Hand hygiene practices among Indian medical undergraduates: a questionnaire-based survey. Cureus. 2017;9(7):e1463. doi:10.7759/cureus.1463
22. Engda T. The contribution of medical educational system of the college of medicine, and health sciences of the university of Gondar in Ethiopia on the knowledge, attitudes, and practices of graduate students of Health Sciences in relation to the prevention and control of nosocomial infections during the academic year of 2018. BMC Med Educ. 2020;20:378. doi:10.1186/s12909-020-02271-6
23. Nematian SSS, Palenik CJ, Mirmasoudi SK, Hatam N, Askarian M. Comparing knowledge and self-reported hand hygiene practices with direct observation among Iranian hospital nurses. Am J Infect Control. 2017;45:e65–e67. doi:10.1016/j.ajic.2017.03.007
24. Othman M, Jonker C. Hand hygiene among hospital staff: a survey of knowledge, attitude and practice in a general hospital in Syria. Indones J Nurs. 2018;21(3):139–149. doi:10.7454/jki.v21i3.513
25. Ahmed J, Malik F, Memon ZA, et al. Compliance and knowledge of healthcare workers regarding hand hygiene and use of disinfectants: a study based in Karachi. Cureus. 2020;12(2):e7036. PMID: 32211269; PMCID: PMC7082788. doi:10.7759/cureus.7036
26. Bin-Humran M, Alahmary K. Assessment of knowledge, attitude and practice of hand hygiene among medical and health profession students at King Saud bin Abdulaziz University for Health Sciences in Saudi Arabia. Saudi Crit Care J. 2018;2:66–72. doi:10.4103/sccj.sccj_6_19
27. World Health Organisation. Perception Survey for health-care workers; 2009. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control/hand-hygiene/monitoring-tools.
28. Blundell S. The impact of hand hygiene intervention on the bacterial populations on chiropractors hands. A dissertation as partial fulfilment for the Masters of Technology degree in Chiropractic, University of Johannesburg; 2018. Available from: https://ujcontent.uj.ac.za/vital/access/manager?Index?site_name=Research%20Output.
29. World Health Organisation. Data summary report framework; 2009. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control/hand-hygiene/monitoring-tools.
30. Kumar G, Sah NK, Boora N. Assessment of knowledge and attitude of infection control among paramedical students. Int J Res and Rev. 2021;8(6):340–346. doi:10.52403/IJRR.20210643
31. Erasmus V, Otto S, De Roos E, et al. Assessment of correlates of hand hygiene compliance among final year medical students: a cross-sectional study in the Netherlands. BMJ Open. 2020;10(2):e029484. PMID: 32054622; PMCID: PMC7045092. doi:10.1136/bmjopen-2019-029484
32. Bouwer M, Labuschagne S, Spamer S, Vermaak C. Knowledge of final-year medical students at the university of the free state of hand hygiene as a basic infection control measure. S Afr Fam Prac. 2018;60(3):74–78. doi:10.1080/20786190.2017.1396789
33. Oduntan A, Louw A, Moodley V, Richter M, von Poser P. Perceptions, expectations, apprehensions and realities of graduating South African optometry students (PEAR study, 2006). Afr Vis Eye Health. 2007;66(3):94–108. doi:10.4102/aveh.v66i3.241
34. Kempen E. Experiential learning in the expanded scope of the undergraduate optometry programme at the University of the Free State. Thesis submitted in fulfilment of the requirements for the degree Philosophiae Doctor in Health Professions Education (PhD HPE) in the Division Health Sciences Education Faculty of Health Sciences at the University of The Free State; 2020. Available from: https://scholar.ufs.ac.za/handle/11660/11496/.
35. Nair SS, Hanumantappa R, Hiremath SG, Siraj MA, Ragunath P. Knowledge, attitude, and practice of hand hygiene among medical and nursing students at a tertiary care centre in Raichur, India. ISRN Prev Med. 2014;4. doi:10.1144/2014/608927
36. Amissah I, Salia S, Craymah JP. A study to assess hand hygiene knowledge and practices among health care workers in a teaching hospital in Ghana. Int J Sci Res. 2013;ISSN:2319.
37. Setati ME. Hand hygiene knowledge, attitude, and practices among health care workers of Pietersburg tertiary hospital, Polokwane, Limpopo Province. Mini dissertation submitted in partial fulfilment of the requirements for the degree of Master of Medicine in Public Health Medicine in the Faculty of Health Sciences, (School of Medicine) at the University of Limpopo; 2019. Available from: http://ulspace.ul.ac.za/handle/10386/2982.
38. Ugwu MC, Muoka O, Okezie UM, et al. Perceptions, attitude and knowledge of five moments of hand hygiene practices among healthcare workers in Awka Anambra Nigeria. J Infect Dis Diagn. 2019;4:126.
39. World Health Organisation. WHO guidelines on hand hygiene in health care. first global patient safety challenge clean care is safer care. Geneve, Switzerland; 2009. Available from: https://www.who.int/publications/i/item/9789241597906.
40. Gould D, Purssell E, Jeanes A, et al. The problem with ‘my five moments for hand hygiene. BMJ Qual Saf. 2022;31:322–326. doi:10.1136/bmjqs-2020-011911
41. Richter SM, Barnard TG. Adaptation of the WHO hand hygiene observation form for application in optometry training facilities. Clin Optom. 2021;13:227–234. doi:10.2147/OPTO.S304315
42. Yousif MA, Tancred T, Abuzaid M. A survey of knowledge, attitudes and practices regarding hand hygiene among doctors and nurses in Ribat University Hospital. Int J Med Rev Case Rep. 2020;4(2):1. doi:10.5455/IJMRCR.hand-hygiene-doctors-nurses
43. Turakhia S, Saoji Y, Goyal A, et al. COVID-19 guidelines for optometry and optical services post-lockdown. Indian J Ophthalmol. 2020;68(8):1533–1539. PMID: 32709769; PMCID: PMC7640844. doi:10.4103/ijo.IJO_1827_20
44. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564–1567. PMID: 32182409; PMCID: PMC7121658. doi:10.1056/NEJMc2004973.
45. Al-Mohaithef M, Chandramohan S, Hazazi A, Elsayed EAS. Knowledge and Perceptions on hand hygiene among nurses in the Asir region, Kingdom of Saudi Arabia. Saudi J Health Sci. 2020;9:30–38. doi:10.4103/sjhs.sjhs_58_19
46. Niang BA, Chraiti MN, Nejad SB, et al. P126: direct observation survey of practice of alcohol-based handrubbing in Fann Teaching Hospital, Dakar, Senegal. Antimicrob Resist Infect Control. 2013;2(Suppl 1):P126. doi:10.1186/2047-2994-2-S1-P126
47. Price L, Gozdzielewska L, Alejandre JC, et al. Systematic review on factors influencing the effectiveness of alcohol-based hand rubbing in healthcare. Antimicrob Resist Infect Control. 2022;11:16. doi:10.1186/s13756-021-01049-9
48. Abalkhail A, Mahmud I, Alhumaydhi FA, et al. Hand hygiene knowledge and perception among the healthcare workers during the COVID-19 Pandemic in Qassim, Saudi Arabia: a Cross-Sectional Survey. Healthcare. 2021;9(12):1627. doi:10.3390/healthcare9121627
49. Thakker VS, Jadhav PR. Knowledge of hand hygiene in undergraduate medical, dental, and nursing students: a cross-sectional survey. J Fam Med Prim Care. 2015;4(4):582–586. PMID: 26985420; PMCID: PMC4776613. doi:10.4103/2249-4863.174298.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.