")
Back to Journals » International Medical Case Reports Journal » Volume 17
Intramuscular Hemangioma of the Triceps Brachii Muscle: A Case Report
Received 24 September 2023
Accepted for publication 30 December 2023
Published 17 January 2024 Volume 2024:17 Pages 31—34
DOI https://doi.org/10.2147/IMCRJ.S441846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Cailiang Gao,1 Hu Wang,2 Huiting Liu1
1Department of Nuclear Medicine, Three Gorges Hospital, Chongqing University, Chongqing, People’s Republic of China; 2Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, USA
Correspondence: Huiting Liu, Department of Nuclear Medicine, Three Gorges Hospital, Chongqing University, No. 165, Xincheng Road, Wanzhou, Chongqing, 404000, People’s Republic of China, Email [email protected] Hu Wang, Department of neurology, Johns Hopkins University School of Medicine, Baltimore, MD, USA, Email [email protected]
Introduction: Intramuscular hemangioma (IMH) is a rare type of benign tumor that represents less than 1% of all hemangiomas. Chronic pain and a palpable mass are the most common symptoms. Due to the atypical clinical characteristics of the disease, accurate diagnosis is difficult. Misdiagnosis of IMH as malignancy can occur due to similarities in imaging features between IMH and malignancy. To diagnose IMH accurately, multiple imaging modalities, including X-ray, MRI, CT, and 18F-FDG PET/CT, can be used. However, the final diagnosis of IMH is confirmed through histopathological examination.
Case: This case reports a 16-year-old girl diagnosed with IMH in the triceps brachii muscle. Seek medical attention due to pain and discomfort in the left shoulder. Initial imaging with contrast-enhanced MRI and CT suggested synovial sarcomata. The moderate uptake of FDG on positron emission tomography/computed tomography (PET/CT) also raised suspicions of malignancy. The pathological findings revealed an intramuscular hemangioma with thrombosis and thrombus organization.
Conclusion: The accurate diagnosis of IMH can be challenging due to the absence of distinct clinical symptoms and imaging findings. When evaluating periarticular intramuscular lesions, IMH should be considered if the MRI shows mixed signals with heterogeneous enhancement. Despite the moderate uptake of FDG seen in some IMH cases, it should not automatically rule out the possibility of IMH. Hence, a combination of imaging modalities and histopathological examination is crucial in ensuring a correct diagnosis of IMH.
Keywords: intramuscular hemangioma, fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography, magnetic resonance imaging
Introduction
Intramuscular Hemangioma (IMH), which is a rare benign vascular tumor that often occurs in skeletal muscle.1–3 IMH is often mistaken for a malignant tumor due to the lack of clinical symptoms and specific imaging findings.4,5 It often presents as a vascular malformation and occurs in the skeletal muscles of the extremities or trunk.6 The accurate diagnosis is mainly based on postoperative pathological examination or biopsy.7 The case being reported is of an IMH in the triceps brachii muscle that was misdiagnosed preoperatively as a malignant tumor by different imaging examinations.
Clinical Presentation
The case is about a 16-year-old girl with a one-year history of a left shoulder mass with intermittent mild pain (Figure 1), the pain can be tolerated. There was no other discomfort or abnormality in the remaining whole body. The laboratory examination were negative. X-ray, CT, and MRI examinations have shown a mass within the triceps brachii muscle. X-ray displays a high-density shadow with blurred margins (Figure 1b). MRI shows a 56-mm soft tissue mass with mixed-intensity abnormal signal on T1 (Figure 1c) and T2-weighted images (Figure 1d), a predominantly iso-hypointensive signal mixed with high signal on DWI (Figure 1e), and a hyperintense, well-defined enhancing mass on contrast-enhanced coronal MRI (Figure 1f). CT shows a lobulated mixed-density mass with ill-defined margins (Figure 1g) in the triceps muscle with significant inhomogeneous enhancement (Figure 1h). Based on these findings, synovial sarcoma was considered as a potential diagnosis.
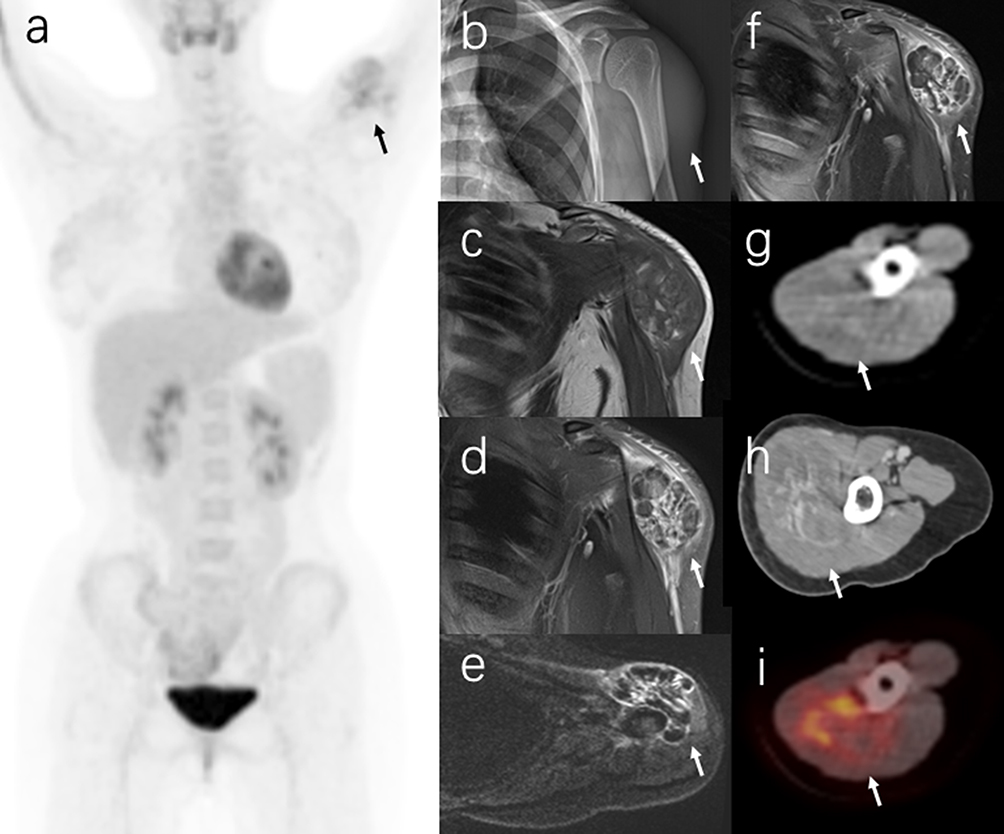 |
Figure 1 The figure shows the PET/CT images of a patient with IMH in the triceps brachii muscle. The maximum intensity projection (MIP) images show a solitary lesion of abnormal 18F-FDG activity in the left shoulder (a, black arrow). The X-ray examination reveals a dense shadow in the left shoulder with blurred margins (b, arrow). On MRI, the mass has mixed intensity abnormal signals on T1-weighted images (c, arrow) and T2-weighted images (d, arrow). The diffusion-weighted imaging (DWI) shows a mainly iso-hypointensive signal mixed with grid-like high signal (e, arrow). The contrast-enhanced coronal MRI displays a hyperintense, well-defined enhancing mass (f, arrow). CT scans show a lobulated mixed-density mass in the triceps muscle with ill-defined margins (g, arrow) and marked inhomogeneous enhancement (h, arrow). The axial fusion PET/CT (i, arrow) shows a 56mmx45mm mass in the triceps brachii muscle with a SUVmax of 5.2. |
The MIP image shows an 18F-FDG uptake in the left shoulder that is consistent with an abnormality (Figure 1a). Further analysis using axial fusion PET/CT (Figure 1i) confirms the presence of a 56 mm × 45 mm mass in the triceps brachii muscle with a maximum SUV of 5.2, indicating focal malignancy without metastasis. This information can aid in the differential diagnosis between benign and malignant conditions and provide information for systemic assessment.
The patient was transferred to a superior hospital for surgical treatment because the mass on the left shoulder was considered malignant on imaging. After surgery, pathology revealed the mass was an intramuscular hemangioma with thrombosis and thrombus formation. Immunohistochemistry was positive for CD34, ERG, Vim, SMA markers and negative for CK. Upon the successful excision, the girl’s symptoms and signs resolved completely.
Discussion
Intramural hemangioma (IMH) is a rare, benign tumor of the skeletal muscles, accounting for less than 1% of all hemangiomas.3,8,9 Its uncommon incidence, location, and lack of symptoms make diagnosis difficult.5 The preferred treatment for IMH is surgical resection, but complete excision can be challenging due to the local invasiveness of the lesion to surrounding tissues.10,11 MRI is the preferred method for diagnosing IMH, as it can clearly show the extent of the lesion and its proximity to surrounding tissues and can also reveal the intratumoral components.12 On MRI, IMH typically shows moderate or high-intensity signal in T1-weighted images, sometimes accompanied by heterogeneously intense signal in T2-weighted images.13,14 In the present case, the lesion showed mixed intensity abnormal signals on T1-weighted and T2-weighted images and was misdiagnosed as synovial sarcoma due to its location near the shoulder joint and mixed signal and heterogeneous enhancement on MRI.
The case reported in the previous statement shows that elevated 18F-FDG avidity (SUVmax 5.2) was observed in the lesion, which is inconsistent with previous reports that found low FDG uptake (SUVs ranged from 0.73 to 1.67) by musculoskeletal hemangiomas.15–17 This unexpected finding led to the initial misdiagnosis of the lesion as a malignant tumor. However, postoperative pathology confirmed the presence of intramuscular hemangioma with thrombosis and thrombus tissue, leading to speculation that the elevated FDG uptake might be related to the thrombus formation in the lesion. There is emerging evidence that suggests a connection between inflammation and thrombosis,18 with metabolically active inflammatory cells exhibiting high 18F-FDG uptake. Although few reports have described the application of 18F-FDG PET/CT in musculoskeletal hemangiomas, there appears to be no PET/CT reports specifically for intramuscular hemangioma, more data is needed to verify these findings.
Conclusion
This report suggested that MRI and 18F-FDG PET/CT may have limitations in identifying intramuscular hemangiomas (IMH) and some malignancies. It is important to consider IMH when periarticular intramuscular lesions show mixed signals and heterogeneous enhancement on MRI. IMH needs to be differentiated from synovial sarcoma and should not be excluded when there is elevated FDG avidity.
Abbreviations
IMH, Intramuscular hemangioma; CT, Computed tomography; MRI, Magnetic resonance imaging; 18F-FDG, fluorine-18-fluorodeoxyglucose; PET/CT, Positron emission tomography/computed tomography; DWI, Diffusion-weighted imaging; MIP, Minimum intensity projection; SUV, Standardized Uptake Value.
Standard of Reporting
CARE guidelines were followed for this study.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Chongqing University Three Gorges Hospital, China. Written informed consent has been obtained from the parental to have case details and images published.
Consent for Publication
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Acknowledgments
We would like to thank Editage (www.editage.co.kr) for English language editing.
Funding
This study did not receive any funding.
Disclosure
The authors declare no conflict of interest, financial or otherwise.
References
1. Li Y, Chou K, Xiong J, et al. Easily misdiagnosed intramuscular hemangioma: a case report. J Int Med Res. 2020;48(12):300060520966897. doi:10.1177/0300060520966897
2. Sayad Z, Dani B, Benazzou S, et al. An unusual location of a cavernous hemangioma: a case report. Pan Afr Med J. 2021;39:29. doi:10.11604/pamj.2021.39.29.28492
3. Garefis K, Nikolaidis V, Kipriotou A, et al. A rare clinical report of intramuscular hemangioma of the middle scalene muscle. Ear Nose Throat J. 2023;102(6):359–361. doi:10.1177/01455613211003834
4. Lescura CM, de Andrade BAB, Bezerra KT, et al. Oral intramuscular hemangioma: report of three cases. J Cutan Pathol. 2019;46(8):603–608. doi:10.1111/cup.13482
5. Rajeev A, Desai KM, Angadi PV, Kale AD. Intramuscular Hemangioma of the Masseter. Arch Iran Med. 2020;23(2):144–145.
6. Park JW, Kim CH, Moon CW. Intramuscular hemangioma in buccal cheek: a case report. J Korean Assoc Oral Maxillofac Surg. 2017;43(4):262–266. doi:10.5125/jkaoms.2017.43.4.262
7. Wild AT, Raab P, Krauspe R. Hemangioma of skeletal muscle. Arch Orthop Trauma Surg. 2000;120(3–4):139–143. doi:10.1007/PL00013761
8. Alami B, Lamrani Y, Addou O, et al. Presumptive intramuscular hemangioma of the masseter muscle. Am J Case Rep. 2015;16:16–19. doi:10.12659/AJCR.890776
9. Parajuli R, Thapa S, Maharjan S. Intramuscular hemangioma of thyrohyoid muscle. Case Rep Otolaryngol. 2016;2016:7158691. doi:10.1155/2016/7158691
10. Lu H, Chen Q, Yang H, et al. Aggressive intramuscular hemangiomas in the upper extremity: a case report. Medicine. 2017;96(3):e5939.
11. Verna C, Min KW. Intramuscular hemangioma: a benign tumor masquerading as malignant soft tissue tumor. Report of two cases. J Okla State Med Assoc. 1999;92(1):21–23.
12. Tang L, Yang B, Yin B, et al. Diagnosis and surgery for intramuscular hemangioma of skeletal muscle. Zhongguo Gu Shang. 2014;27(12):1033–1035.
13. Córdoba-Fernandez A, Lobo-Martín A, Escudero-Severín C, et al. Giant plantar epidermoid cyst with invasion of the interosseous muscles. J Am Podiatr Med Assoc. 2017;107(4):329–332. doi:10.7547/16-054
14. Lee HS, Hong YC, Jung KJ, et al. A huge plantar intramuscular hemangioma in the plantar area treated surgically: a case report and literature review. Int J Environ Res Public Health. 2021;18(17):9088. doi:10.3390/ijerph18179088
15. Hatayama K, Watanabe H, Ahmed AR, et al. Evaluation of hemangioma by positron emission tomography: role in a multimodality approach. J Comput Assist Tomogr. 2003;27(1):70–77. doi:10.1097/00004728-200301000-00013
16. Watanabe H, Inoue T, Shinozaki T, et al. PET imaging of musculoskeletal tumours with fluorine-18 alpha-methyltyrosine: comparison with fluorine-18 fluorodeoxyglucose PET. Eur J Nucl Med. 2000;27(10):1509–1517. doi:10.1007/s002590000344
17. Suzuki H, Watanabe H, Shinozaki T, et al. Positron emission tomography imaging of musculoskeletal tumors in the shoulder girdle. J Shoulder Elbow Surg. 2004;13(6):635–647. doi:10.1016/j.jse.2004.03.015
18. Kapoor S, Opneja A, Nayak L. The role of neutrophils in thrombosis. Thromb Res. 2018;170:87–96. doi:10.1016/j.thromres.2018.08.005
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.