")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 15
Innovative Techniques in Video-Assisted Thoracoscopic Surgery: Lu’s Approach
Authors Wang B, Wang J, Sun T, Ding Y, Li S, Lu H
Received 15 November 2023
Accepted for publication 12 January 2024
Published 2 February 2024 Volume 2024:15 Pages 9—17
DOI https://doi.org/10.2147/LCTT.S446418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sai-Hong Ignatius Ou
Supplementary video of “Video-Assisted Thoracoscopic Surgery” [446418].
Views: 120
Baofeng Wang,1,2,* Jiang Wang,2,* Tongyu Sun,2 Yilin Ding,2 Shasha Li,3 Hengxiao Lu2
1School of Clinical Medicine, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 2Department of Thoracic Surgery, Weifang People’s Hospital, Weifang, Shandong, People’s Republic of China; 3Clinic, Weifang People’s Hospital, Weifang, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hengxiao Lu, Department of Thoracic Surgery, Weifang People’s Hospital, Weifang, Shandong, People’s Republic of China, Email [email protected]
Purpose: Lu’s approach for video-assisted thoracoscopic surgery (LVATS), which derives from Uniportal Video-Assisted Thoracoscopic Surgery(UVATS), is a novel surgical approach for VATS and carries out micro-innovation for lung cancer resection. The objective of this study is to elucidate the safety, feasibility, and efficacy of this novel surgical approach.
Patients and Methods: The clinical data of patients with non-small cell lung cancer (NSCLC) who underwent a curative thoracoscopic lobectomy between Mar. 2021 and Mar. 2022, were retrospectively collected and analyzed. Patients were divided into the LVATS group and the UVATS group. Propensity score matching (PSM) was used to reduce selection bias and create two comparable groups. Perioperative variables were compared, and a p-value < 0.05 was deemed statistically significant.
Results: A total of 182 patients were identified, among whom 86 patients underwent LVATS and 96 UVATS. Propensity matching produced 62 pairs in this retrospective study. There were no deaths during perioperative period. Patients in the LVATS group experienced a shorter operation time (88 (75, 106) VS 122 (97, 144) min, P < 0.001), less intraoperative blood loss (20 (20, 30) VS 25 (20, 50) mL, P = 0.021), shorten incision length (2.50 (2.50, 2.50) VS 3.00 (3.00, 3.50) cm, P < 0.001), and more drainage volume (460 (310, 660) VS 345 (225, 600) mL, P = 0.041) than patients in the UVATS group. There was not significant difference in the lymph node stations dissected (5 (4, 5) VS 5 (4, 5), P = 0.436), drainage duration (3 (3, 4) VS 3 (3, 4) days, P =0.743), length of postoperative hospital stay (4 (4, 5) VS 4 (4, 6) days, P = 0.608), VAS on the POD1 (4 (4, 4) VS 4 (4, 4), P=0.058) and POD3 (3 (3, 4) VS 4 (3, 4), P=0.219), and incidence of postoperative complications (P=0.521) between the two groups.
Conclusion: Lu’s approach for video-assisted thoracoscopic lobectomy is safe and feasible, potentially reducing surgery time, incision length, and intraoperative blood loss.
Keywords: non-small cell lung cancer, uniportal video-assisted thoracoscopic surgery, Lu’s approach for VATS, lobectomy
Introduction
Lung cancer is the leading cause of cancer-related mortality worldwide. Non-small cell lung cancer (NSCLC) is the most common type, accounting for approximately 85% of all lung cancer patients.1 It is broadly categorized into two types: small cell lung cancer and non-small cell lung cancer (NSCLC).2,3 Several risk factors have been identified for NSCLC, such as history of smoking, asbestos exposure, exposure to metal and mineral dust, and air pollution.4 Surgical resection remains the primary mode of treatment for early-stage NSCLC and is an essential component of multimodality therapy for even more advanced disease with curative intent.5
In 2011, Gonzalez-Rivas reported the first case of UVATS lobectomy.6 Subsequent research has shown UVATS to be preferable to multi-portal VATS,7,8 offering benefits like less blood loss and quicker postoperative recovery.9,10 However, UVATS faces scrutiny over technical challenges, particularly the limited space from a single-port entry that can affect instrument handling, leading to issues with bleeding control, suturing, and clear visualization.11,12 These limitations can extend the learning period and increase the complexity of the procedure.13,14 Therefore, building upon uniport thoracoscopy, we introduce the LVATS approach as a potential refinement.
This study aims to delineate the LVATS technique and evaluate its safety, feasibility, and efficacy for early NSCLC treatment.
Materials and Methods
Study Design
The study was approved by the institutional review board and the ethics committee of Weifang People’s Hospital. The medical records of 182 patients who underwent thoracoscopic lobectomy in the Thoracic Surgery Department of Weifang People’s Hospital from March 2021 to March 2022 were retrospectively collected and analyzed. Patients were assigned to the LVATS group (n=86) and the UVATS group (n=96), based on whether the Lu’s approach are applied during the operation. Preoperative examination including electrocardiography, pulmonary function test, chest computed tomography scan, bronchoscope and brain magnetic resonance imaging. All procedures were performed by a single thoracic surgical team, which consistently adhered to established clinical protocols, care practices, and postoperative rehabilitation strategies. And they were performed by the same lead surgeon who has completed his UVATS learning curve and is proficient in UVATS.
Inclusion and Exclusion Criteria
Inclusion Criteria
- NSCLC patients with primary and single lung lesions.
- with no previous thoracic interventions or surgery on the affected side.
- clinical staging of T1–T3 and N0–N2, and no distant metastases.
- patients with an American Society of Anesthesiologists (ASA) score of I–II.
Exclusion Criteria
- sub-pulmonary lobectomy and preoperative neoadjuvant therapy.
- cT3 tumors invading to the chest wall, diaphragm, or pericardium.
- had a history of malignancies other than NSCLC.
- patients with history of chest surgery.
Clinical Features and Outcomes
Clinical features including age, sex, smoking history, hypertension, diabetes, tumor location and diameter, tumor stage, histology, operation duration, estimated volume of blood loss, lymph node stations dissected, total drainage volume, drainage duration, postoperative hospital stay, VAS on the POD1 and POD3, and postoperative complications were recorded. The operation duration is the primary perioperative outcomes, and the others are secondary.
Surgical Procedure
Anesthesia and Analgesia
All patients received a general anesthesia and were provided with patient-controlled analgesia postoperatively. After intravenous induction, each patient was intubated with a double-lumen endotracheal tube to accomplish single-lung ventilation. Patients’ vital signs were followed during the operation. All patients were extubated at the end of surgery and transferred to the ward.
Position
The patient was kept in a folding knife gesture in the lateral decubitus position. Intraoperatively, the surgeon and the camera holder stood on the abdominal side of the patient, the assistant stood on the back side of the patient in the LVATS group (Figures 1A and 1B).
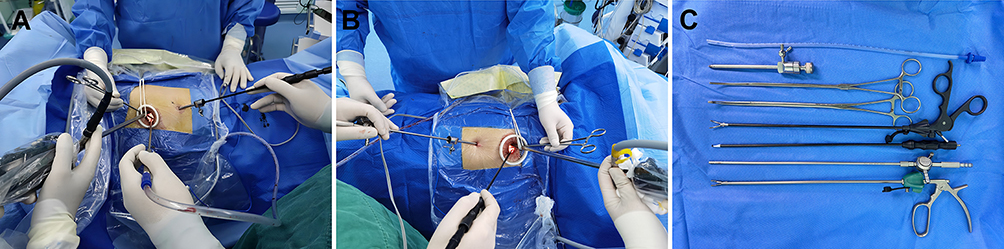 |
Figure 1 Surgical layout for the implementation of LVATS. (A) Configuration for left lung surgery. (B) Arrangement for right lung surgery, with appropriate modifications for operative access based on the surgeon’s preference. (C) Essential instruments used in LVATS. |
Surgical Approach
In LVATS lobectomy, a 2.0 to 3.0-cm utility incision was made at the fourth intercostal space along the anterior axillary line for any lobe resection. A soft plastic wound protector was applied to the incision without rib-spreading. The 10-mm 30° thoracoscope was introduced in the superior side of the incision during the operation. Different from UVATS, a 5mm incision was made at the seventh intercostal space along the midaxillary line and a 5mm trocar was placed in this incision to establish a channel (Figure 1A and B), through which any instrument with a diameter less than 5mm, such as energy instrument, aspirator, separation forceps and vascular clamp (Figure 1C), could be introduced to the surgical field.
The lead surgeon introduces instruments into the surgical field through the utility incision and a 5mm port, effectively resolving the issue of coaxial manipulation of instruments, thereby enabling the surgeon’s hands to operate within a larger range without being hindered. The accompanying figures demonstrate the directions and angles of entry into the surgical field for the fissure suturing (Figure 2A), the bronchus circling and transection (Figures 2B and C), arterial circling and transection (Figures 2D and E), venous circling and transection (Figures 2F and G), and resection of lymph nodes (Figures 2H and I).
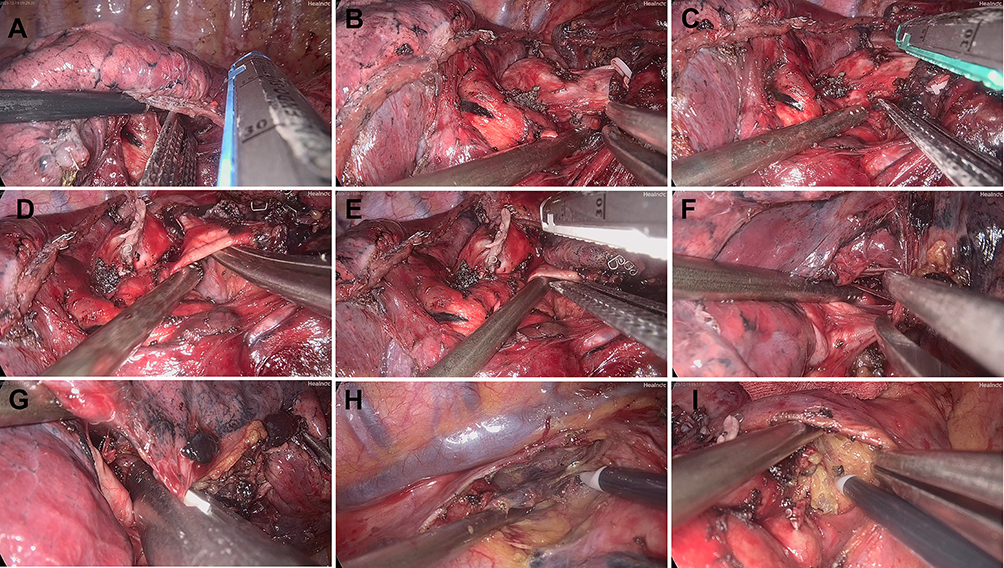 |
Figure 2 Appropriate instruments inserted through a 5mm incision enhance surgical exposure, enable efficient tissue mobilization, and allow for the precise deployment of a surgical stapler. (A) Transecting the oblique fissure. (B) Circling the bronchus of the right upper lobe. (C) Transecting the bronchus of the right upper lobe. (D) Circling the arterial branch of the right upper lobe. (E) Transecting the arterial branch of the right upper lobe. (F) Circling the vein of the right upper lobe. (G) Transecting the vein of the right upper lobe. (H) Lymphadenectomy of the 2nd and 4th nodal stations. (I) Lymphadenectomy of the 7th nodal station. |
The final steps of the procedure included irrigation of the thoracic cavity with normal saline to assess for hemostasis. Ventilation was transitioned from single lung to double lung to evaluate the re-expansion of the lung lobes and to check for any air leaks. A 16 Fr chest tube was placed through the 5mm port to facilitate low-position thoracic drainage (Figures 3A and B). The chest tube would be considered for removal if there was no evidence of air leakage, and the postoperative drainage volume was consistently less than 200 mL per day.
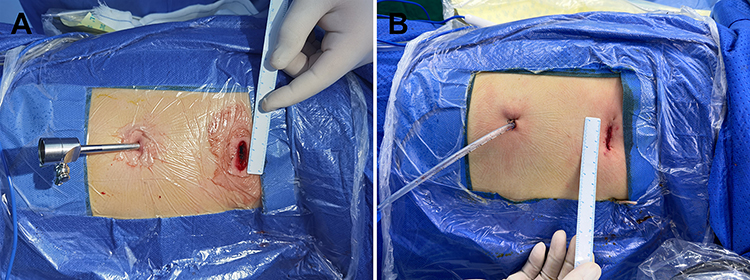 |
Figure 3 Location and details of the incisions. (A) A 2.5 cm utility incision was made in the 4th intercostal space, and a 5 mm trocar was placed in the 7th intercostal space. (B) A 16 Fr drainage tube was inserted into the 7th intercostal space. |
In UVATS lobectomy, a 3.0 to 4.0 cm incision was made at the fourth intercostal space along the anterior axillary line for upper lobe resection and the fifth intercostal space for middle and inferior lobe resection. In most cases, the thoracoscope is placed on the posterior side of the incision and the other working instruments are placed on the anterior side of the incision. The lead surgeon typically employs a suction device to maintain a clear view of the operative field and uses energy devices to mobilize tissue. The surgical procedure encompasses several key steps: Hilar exposure (Figure 4A), which is crucial for gaining access to the targeted area. Dissection of lymph nodes that may restrict subsequent surgical maneuvers (Figures 4B and C). Mobilization of the artery (Figure 4D), vein (Figure 4E), and bronchus (Figure 4F) to enable safe and precise resection. The UVATS surgical procedure is thoroughly documented in an extensive body of literature.15,16
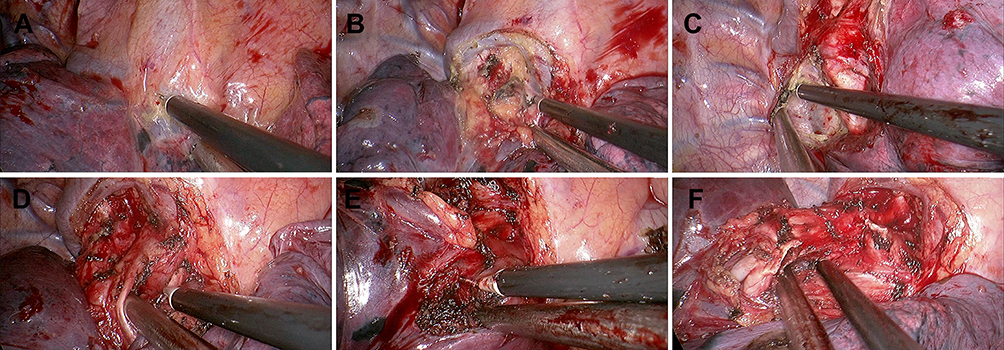 |
Figure 4 Coaxial manipulation of instruments during UVATS. (A) Dissection at the pulmonary hilum for clear access. (B) Lymphadenectomy of the 10th nodal station. (C) Lymphadenectomy of the 7th nodal station. (D) Mobilization of the right upper lobe’s arterial branch to secure vascular control. (E) Mobilization of the right upper lobe bronchus for bronchial management. (F) Mobilization of the right upper lobe vein for venous control. |
Statistical Analysis
Statistical analyses in this study were conducted using R software, version 4.2.1. To achieve equitable comparisons, propensity score matching was employed. The matching was achieved on a one-to-one ratio using the nearest neighbor technique, informed by a propensity score model derived from logistic regression, incorporating age, gender, tumor location, tumor diameter, COPD status, smoking history, and the presence of hypertension or diabetes.
Continuous variables were described using median values and interquartile ranges. Between-group comparisons for these variables were conducted using the Wilcoxon rank-sum test. For categorical variables, analysis was performed using either the Chi-square test or Fisher’s exact test, depending on the expected frequency of observations. A predefined significance level of 0.05 was used to determine statistical significance.
Results
Patient characteristics and PSM
A total of 182 patients were identified and divided into the two groups: the LVATS (n=86) and the UVATS (n=96). 62 LVATS lobectomies and 62 UVATS lobectomies were matched after the propensity scored analysis in this retrospective study. The clinical features of the study cohort before and after matching are listed in Table 1. There was no major difference between the two groups in the demographic information: age (P=0.828), gender (P=0.718), smoking history (P>0.999), hypertension (P=0.326), diabetes (P=0.769), COPD (P>0.999), tumor location (P=0.994), tumor diameter (P=0.251).
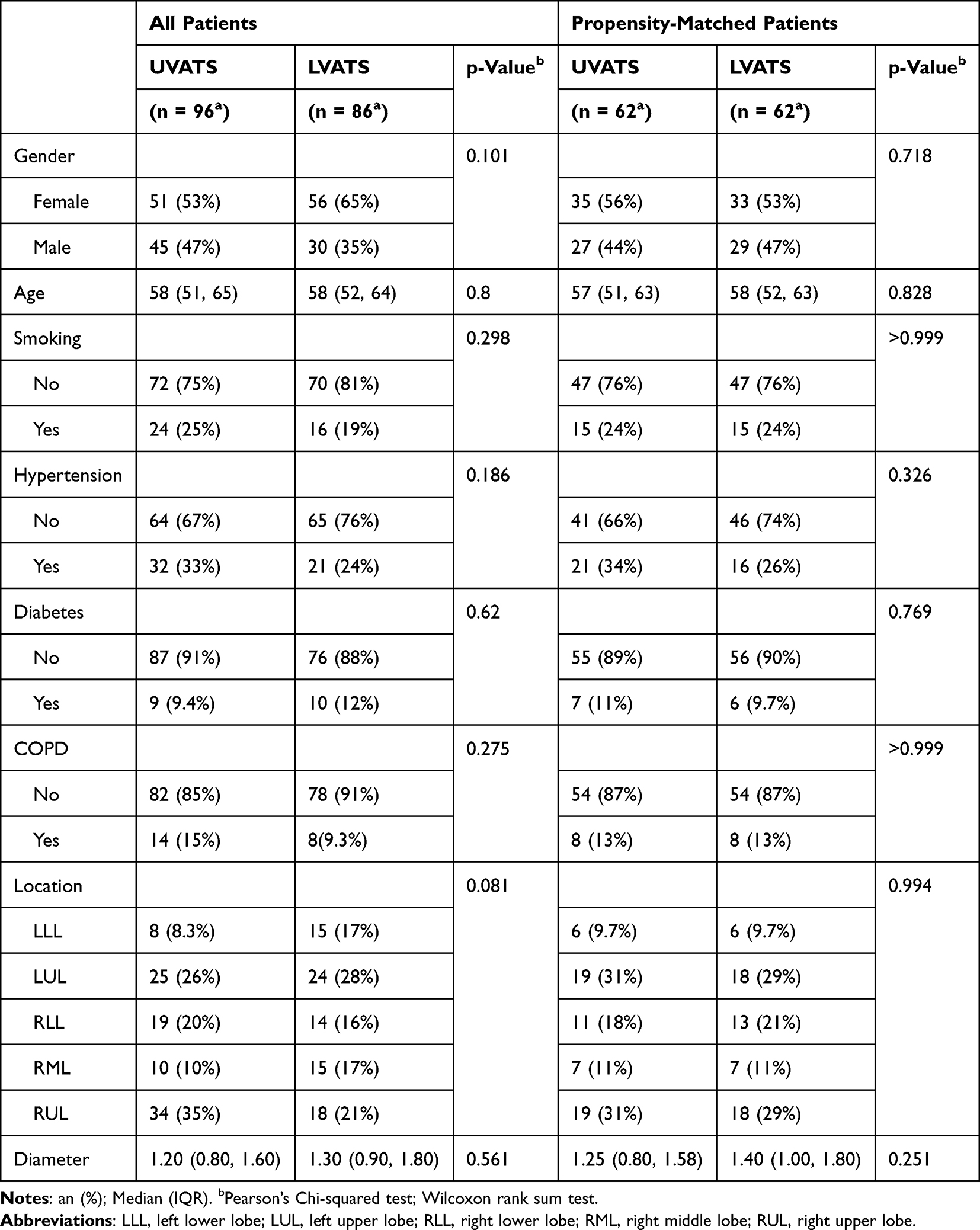 |
Table 1 Clinical Features Before and After Propensity-Matched |
Perioperative outcomes
The primary clinical result is the operation duration. The operation duration in LVATS was shorter than in UVATS (88 (75, 106) VS 122 (97, 144) min, P <0.001). The volume of estimated blood loss in LVATS was less than in UVATS (20 (20, 30) VS 25 (20, 50) mL, P = 0.021). The LVATS had shorten incision length (2.50 (2.50, 2.50) VS 3.00 (3.00, 3.50) cm, P <0.001) than UVATS. Patients in LVATS group had more drainage volume (460 (310, 660) VS 345 (225, 600) mL, P = 0.041) than in UVATS group. While the lymph node stations dissected (5 (4, 5) VS 5 (4, 5), P = 0.436), and drainage duration (3 (3, 4) VS 3 (3, 4), P =0.743) days, length of postoperative hospital stay (4 (4, 5) VS 4 (4, 6), P = 0.608) days, VAS on the POD1 (4 (4, 4) VS 4 (4, 4), P=0.058) and POD3 (3 (3, 4) VS 4 (3, 4), P=0.219) were similar between the two groups. And the postoperative complications between two groups were similar (P=0.521). The clinical results are recorded in Table 2.
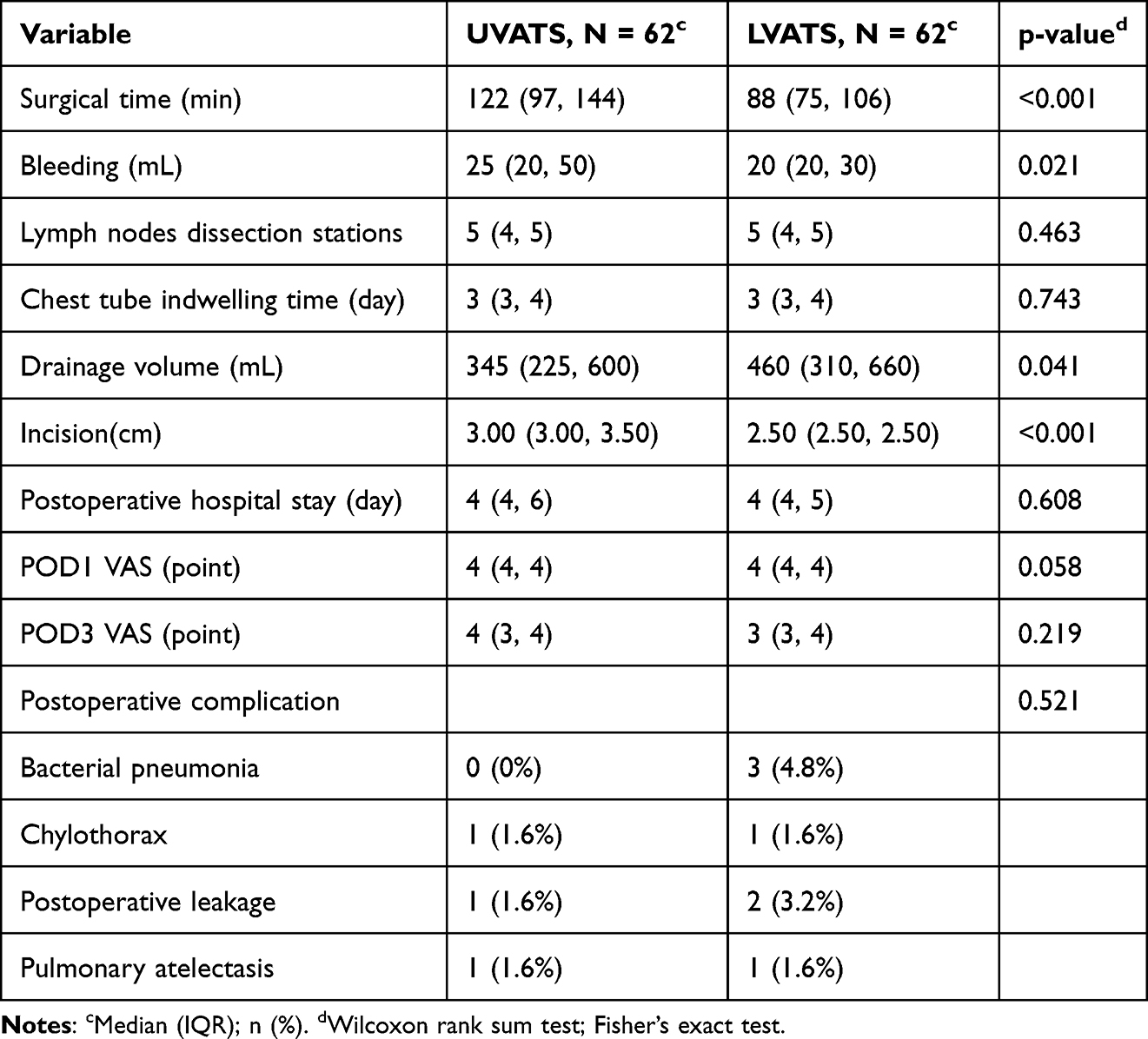 |
Table 2 Comparison on Perioperative Outcomes |
Morbidity and mortality
No mortality was recorded in either group. Complications in the LVATS group included three cases of bacterial pneumonia and one case of chylothorax, two cases of postoperative leakage, two cases of pulmonary atelectasis. Complications in the UVATS group included one case of chylothorax, one case of postoperative leakage and one case of pulmonary atelectasis. All patients were discharged following the confirmation of lung re-expansion by c hest CT. The average postoperative length of stay in hospital was 5.38±3.06 days in LVATS and 5.66±4.95 days (P = 0.608) in UVATS. Readmission to the intensive care unit was not recorded in this cohort.
Discussion
The refinement of the UVATS in our study involved the introduction of an additional 5mm port. This modification was aimed at exposure, and mobilization, as well as enhancing the application of surgical staplers and sutures. To the best of our knowledge, this is the first study to report on the utility of this modified approach for lung resection procedures. The preoperative characteristics between the two patient cohorts were similar, affirming the robustness of the comparison enabled by propensity score matching.
The perioperative outcomes favored the LVATS approach. Notably, operation duration was significantly shorter for LVATS, with a median time of 88 minutes versus 122 minutes for UVATS, which is a substantial reduction. This improvement is predominantly due to the effective management of the coaxial manipulation of instruments, which is a common issue in UVATS.17,18 As a result, LVATS facilitates a broader range of motion for the surgeon, thereby promoting enhanced maneuverability and efficiency during the operation. The LVATS ‘s efficiency in reducing operative time may lead to increased surgical throughput, allowing for a greater number of procedures within the same scheduling window, while concurrently decreasing the patients’ exposure to anesthesia and operative stress. This reduction in operative time is also expected to contribute to enhanced postoperative recovery outcomes.
Additionally, the adoption of a 5mm port in LVATS could potentially decrease the instrument count within the utility incision. Ordinarily, a LVATS utility incision is designed to house merely three instruments, compared to four instruments required by UVATS.19,20 This modification has also been associated with a shorter incision length in LVATS compared to UVATS. Moreover, the use of a shorter incision paired with a 16Fr drainage tube may aid in reducing postoperative pain, as indicated by the postoperative day 1 (POD1) Visual Analog Scale (VAS) scores, which show a trend towards improvement, though not statistically significant (p=0.058).
Interestingly, the group undergoing LVATS exhibited a greater volume of postoperative drainage despite the advantages of shorter operation times and shorter utility incision. This outcome was particularly notable given that the LVATS drainage tube was positioned at the seventh intercostal space, which is traditionally thought to enhance drainage efficiency compared to the placement at the fourth intercostal space. The positioning of the drainage tube is widely recognized to affect the volume of drainage, with lower placements typically facilitating better drainage.21,22 Nevertheless, the number and location of surgical incisions could also significantly impact drainage, suggesting a multifaceted set of factors influencing postoperative drainage outcomes.
The comparative analysis of postoperative complications between UVATS and LVATS demonstrated no statistically significant differences, with a p-value of 0.521. This suggests a comparable level of safety between the two surgical techniques. However, it is noteworthy that bacterial pneumonia was not observed in the UVATS cohort, whereas the LVATS group experienced a 4.8% incidence rate, representing three individual cases. While the difference did not reach statistical significance, it highlights a potential area for further scrutiny. Given the small scale of the study, these findings could be attributed to random variation. However, they may also suggest underlying procedural factors that could influence postoperative infection rates.
Limitations of this study include its retrospective nature and the inherent selection bias, despite the use of propensity score matching. Moreover, the findings may not be generalizable given the modest cohort size, single-center setting and the specific surgical expertise involved. Future multicenter, randomized controlled trials are needed to validate these results and potentially guide surgical practice towards the broader adoption of LVATS. Importantly, longitudinal multi-center studies would evaluate not only perioperative outcomes but also tumor recurrence and long-term survival.
Conclusion
In summary, Lu’s approach for video-assisted thoracoscopic surgery (LVATS) lobectomy is a safe, feasible, and effective procedure for treating patients with early NSCLC (Supplementary video). This technique has the potential to reduce operation duration, incision length and intraoperative blood loss and achieve better drainage of postoperative pleural effusion, which can ultimately benefit both patients and medical professionals.
Abbreviation
NSCLC, non-small cell lung cancer; POD, postoperative day; LVATS, Lu’s approach for video-assisted thoracoscopic surgery; UVATS, video-assisted thoracoscopic surgery; VAS, Visual Analogue Scale.
Ethics Statement
This study was approved by the Ethics Committee of Weifang People’s Hospital and performed with the Declaration of Helsinki (as revised in 2013). All patients or families provided the written informed consents.
Acknowledgments
Baofeng Wang and Jiang Wang share the first authorship for this study. The authors would like to express their gratitude to all those who helped during the writing of this manuscript and their efforts in the management of this patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Weifang Municipal Health and Health Committee Fund, with the project number WFWSJK-2023-321.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Jr M, Yang P, Sd C, et al. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–594. doi:10.4065/83.5.584
2. Cm R, Brambilla E, Faivre-Finn C, et al. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3. doi:10.1038/s41572-020-00235-0
3. Chen L, Fan Y, Lu H. Pulmonary Epithelial-Myoepithelial Carcinoma. J Oncol. 2022;2022:4559550. doi:10.1155/2022/4559550
4. Metzenmacher M, Griesinger F, Hd H, et al. Prognostic factors in nonsmall cell lung cancer: insights from the German CRISP registry. Eur Respir J. 2023;61(2):2201336. doi:10.1183/13993003.01336-2022
5. Al-Shahrabani F. Surgical strategies in the therapy of non-small cell lung cancer. World J Clin Oncol. 2014;5(4):595–603. doi:10.5306/wjco.v5.i4.595
6. Gonzalez D, Paradela M, Garcia J, et al. Single-port video-assisted thoracoscopic lobectomy. Interact Cardiovasc Thorac Surg. 2011;12(3):514–515. doi:10.1510/icvts.2010.256222.
7. Dimitrios Magouliotis M, Spiliopoulos FK, Athanassiadi K, Athanassiadi K. Uniportal versus multiportal video-assisted thoracoscopic lobectomy for lung cancer: an updated meta-analysis. Lung. 2021;199(1):43–53. doi:10.1007/s00408-020-00411-9
8. De M, Mp F, Spiliopoulos K, Athanassiadi K. Uniportal versus multiportal video-assisted thoracoscopic lobectomy for lung cancer: an updated meta-analysis published correction appears in lung. Lung. 2021;199(2):235. doi:10.1007/s00408-020-00411-9
9. Yang X, Li M, Yang X, et al. Uniport versus multiport video-assisted thoracoscopic surgery in the perioperative treatment of patients with T1-3N0M0 non-small cell lung cancer: a systematic review and meta-analysis. J Thorac Dis. 2018;10(4):2186–2195. doi:10.21037/jtd.2018.03.74
10. Yue H, Fan K, Zhang Z, et al. Clinical analysis of video-assisted thoracoscopic surgery for resection of solitary pulmonary nodules and influencing factors in the diagnosis of benign and malignant nodules. Evid Based Complement Alternat Med. 2021;2021:1490709. doi:10.1155/2021/1490709
11. Sihoe Alan DL. Reasons not to perform uniportal VATS lobectomy. J Thoracic Dis. 2016;8(Suppl 3):S333–43. doi:10.3978/j.issn.2072-1439.2016.02.41
12. Sano Y, Okazaki M, Shigematsu H, et al. Quality of life after partial lung resection with uniportal versus 3-port video-assisted thoracoscopic surgery: a prospective randomized controlled study.. Surg Today. 2021;51(11):1755–1763. doi:10.1007/s00595-021-02294-6.
13. Ojanguren A, Gonzalez M. What is the optimal way to succeed in uniportal VATS? J Thorac Dis. 2020;12(6):3018–3021. doi:10.21037/jtd.2020.03.38
14. Wang L. The feasibility and advantage of uniportal video-assisted thoracoscopic surgery (VATS) in pulmonary lobectomy. BMC Cancer. 2017;175:25. doi:10.1186/s12885-017-3069-z
15. Parade la de la morena M, De La Torre Bravos M, Fernandez PR, et al. Standardized surgical technique for uniportal video-assisted thoracoscopic lobectomy. Eur J Cardiothorac Surg. 2020;58(Supplement_1):i23–i33. doi:10.1093/ejcts/ezaa110.
16. Wang W, Rao S, Ma M, et al. The concept of broad exposure facilitates uniportal video-assisted thoracoscopic mediastinal lymph nodes dissection. J Cardio Thoracic Sur. 2021; 161: doi:10.1186/s13019-021-01519-6
17. González-Rivas D, Sihoe ADL. Important technical details during uniportal video-assisted thoracoscopic major resections. Thorac Surg Clin. 2017;27(4):357–372. doi:10.1016/j.thorsurg.2017.06.004
18. Li S, Wu J, Wan Z, et al. The learning curve for uniportal video-assisted thoracoscopic anatomical segmentectomy. J Surg Oncol. 2021;124(3):441–452. doi:10.1002/jso.26517
19. Han D, Cao Y, Wu H, et al. Uniportal video-assisted thoracic surgery for the treatment of lung cancer: a consensus report from Chinese Society for Thoracic and Cardiovascular Surgery (CSTCVS) and Chinese Association of Thoracic Surgeons (CATS). Transl Lung Cancer Res. 2020;9(4):971–987. doi:10.21037/tlcr-20-576.
20. Forster C, Gonzalez M. Uniportal video-assisted thoracic surgery segmentectomy: a promising new development for thoracic surgery. Transl Lung Cancer Res. 2023;12(6):1152–1155. doi:10.21037/tlcr-23-197.
21. Fu Y, Wang X, Xu H, et al. A novel drainage strategy using chest tube plus pleural catheter in uniportal upper lobectomy: a randomized controlled trial. Thoracic Cancer. 2022;14(4):399–406.
22. Abdelraouf A, Elkhayat H, Osman M, Elminshawy A. Do we need a small catheter drainage with chest tube after uniportal video-assisted thoracoscopic surgery for better drainage? CurrThoracic Sur. 2022;7(1):7. doi:10.26663/cts.2022.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.