")
Back to Journals » International Journal of Women's Health » Volume 16
Infertile Jordanian Women’s Self-Perception About Societal Violence: An Interpretative Phenomenological Study
Authors Bawadi H, Al-Hamdan ZM , Clark CJ, Hall-Clifford R, Hamadneh JM, Al-Sharu EE
Received 27 November 2023
Accepted for publication 2 April 2024
Published 13 April 2024 Volume 2024:16 Pages 593—603
DOI https://doi.org/10.2147/IJWH.S451950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Hala Bawadi,1 Zaid M Al-Hamdan,2 Cari Jo Clark,3 Rachel Hall-Clifford,4 Jehan Mahmoud Hamadneh,5 Emad Elddeen Al-Sharu6
1Maternal and Child Health Nursing Department, the University of Jordan, Amman, Jordan; 2Faculty of Nursing, Jordan University of Science and Technology, Irbid, Jordan; 3Rollins School of Public Health, Emory University, Atlanta, GA, USA; 4Center for the Study of Human Health and Department of Sociology, Emory University, Atlanta, GA, USA; 5IVF Center/ King Abdullah University Hospital, Jordan University of Science and Technology, Ar-Ramtha, Jordan; 6OB-GYN Senior Specialist Reproductive Medicine(IVF), Royal Medical Services, Amman, Jordan
Correspondence: Zaid M Al-Hamdan, Email [email protected]; [email protected]
Background: Infertility affects one in six couples globally and is compounded by stigma and violence, particularly for women, in Jordan’s culture. While existing research has illuminated societal pressures faced by infertile women, there is, yet no comprehensive understanding of the violence they encounter in their daily lives.
Objective: This Interpretative Phenomenological study seeks to unravel the experiences of infertile women regarding societal violence in Jordan. By focusing on different types of community violence - physical, psychological, and emotional - The study aims to provide nuanced insights into the challenges these women confront. It also endeavors to identify contributing factors, including societal attitudes, cultural beliefs, and individual encounters, while informing policy and practice to mitigate this issue.
Methods: Employing a qualitative approach, this study conducted semi-structured interviews with purposively sampled infertile women. Thematic analysis was utilized to uncover recurring patterns and themes, facilitating a comprehensive exploration of their experiences.
Results: Five main themes were identified: How the surrounding people view me as an infertile woman; I am suffocated by their questions; they interfere in the smallest details; I got burned and turned to ashes, and I have no right to complain; The problem of childbearing and the treatment plan is a matter for me and my husband only; and who supports me and what do I want from those around me?
Implications: This study’s implications are significant for policy and practice. By foregrounding the prevalent violence faced by infertile women, it underscores the urgency of interventions. Raising awareness, providing education, and extending support can counteract societal stigma and violence. Creating a more compassionate societal fabric can ensure a safer, more inclusive environment for these women.
Keywords: infertile women, community violence, societal stigma, qualitative study, Jordan, cultural norms, psychological abuse, physical violence, emotional trauma
Background
Couples are deemed to have fertility problems only after they have spent a full year trying to conceive by having intercourse on a regular basis without any form of birth control. The World Health Organization estimates that out of every six couples, one will have problems getting pregnant.1 The Jordanian Demographic and Health Survey of 2019 reported that, among married reproductive-age individuals, 16% of females and 9% of males said that they were encountering fertility problems.2 In Arab society, forming a family is the major reason for getting married and is of the utmost importance. The pressure to conceive and produce children is high, and infertility can be seen as a significant obstacle to achieving family goals.3 Relationships suffer when one or both parties within the couple are diagnosed as being infertile, and the initial crisis is often compounded by the reactions of those around them. It is common for women to bear children within the first year of marriage to prove their fertility and actual or suspected infertility is highly stigmatizing.4
Infertility-related stigma and violence against infertile women in Jordan have been widely documented.5–7 Infertile women are often blamed for their inability to conceive and are considered a burden to their husbands and their families. In some cases, infertile women have been subjected to physical and emotional abuse by their in-laws or their own families, who see them as a source of shame and disappointment.8 The abuse encountered ranges from verbal abuse to physical violence. Many women live in fear of their husbands leaving them or marrying a second wife, all of which can bring about psychological trauma and be detrimental to their health.6,7
Infertile women in all parts of the world suffer mental anguish due to their inability to have a child. This can be exacerbated by community violence directed against them by family members and other people around them. Although infertility can indeed be caused by problems with the husband, women usually receive the blame for this “malfunction”. They are often subjected to discrimination and carry an insupportable stigma, whether the “fault” is with them or not. In some cases, infertile women can find themselves socially isolated and excluded from certain community events and activities, such as parties arranged for children in the extended family.9 Infertility can also significantly impact infertile women who may feel misunderstood or judged by their peers, family members, and society at large, leading to social withdrawal and a sense of alienation.10 Family members and others may pressure an infertile woman to undergo fertility treatments that are not only costly, but also potentially dangerous to the woman’s health.
In addition to the distress inherent to the situation, infertility in Arab societies can be seen as shameful. While men can deny that they have a fertility problem, women are often left to bear the stigma alone. Marital conflict and divorce are associated with infertility and could be a formerly unrecognized risk factor for domestic violence.11 In Jordan, pressure and discrimination from society can induce feelings of isolation and poor self-esteem in women who are having difficulty conceiving.12 While infertile men in Arab societies surely experience feelings of shame and disappointment at not being able to father a child, the stigma they face is markedly less than that endured by women.12 One study pointed out that infertility in men is kept private, and they are not pressured by their community to repeatedly talk about the details of their problem, as is often the case with women.13 While views of infertility in the Arab world may differ immensely, the general belief is that failure to procreate is down to the woman being unable to perform her natural function in life. Thus, such a woman can be become a target of stigma and a source of shame to her family.
This qualitative study seeks to examine and understand the lived experiences of women living with infertility in Jordan and the violence they sometimes face from their surrounding community, which can encompass physical, psychological, and emotional violence. Furthermore, we look at the societal attitudes and cultural beliefs surrounding infertility in Jordan with the aim of highlighting the challenges that face infertile women and how the resulting violence impacts their lives. Through the results, we seek to guide policy and practice so as to reduce, and possibly eliminate, violence against infertile Jordanian women.
Methodology and Methods
Study Design
This study adopted an interpretative phenomenological (IP) approach as it allows the researcher to ask in-depth questions and the participants to express their individual viewpoints and the meanings they attribute to their experiences.14
Setting and Participants
The study was conducted in Jordan, where participants were recruited from the Infertility and IVF unit at the King Al Hussein Medical Center, Royal Medical Service (RMS) in Amman, and the IVF Center at the King Abdullah University Hospital (KAUH) within the Jordan University of Science and Technology in Irbid. Over 20,000 patients utilize these sites annually for fertility services (Sharu, 2020). Women who have been married at least 2 years, seeking services for infertility treatment at study clinics and who reside in Jordan are eligible to participate. A purposive sampling technique with a maximum variation strategy15 was used including age, level of education, and type and duration of infertility. Initial participants were identified through the database of two IVF centers. Thirty women met the eligibility criteria and were contacted by phone. 17 women agreed to participate in the study. The sample size was determined by theme saturation.16 In this study, we interviewed 13 women until no new data emerged.
Data Collection
The researchers opted to collect data for this study using individual, in-depth semi-structured interviews as it is the most effective method for uncovering participants’ understanding of a complex experience.17 The interview method permits women to talk freely about their experiences, as well as giving the researcher ample opportunity to ask in-depth questions to collect additional information.18 The research team put together an interview guide, shown in detail in Table 1, to ensure that no important issues related to the topic were omitted. The interviews, all conducted in private, lasted between 50 to 70 minutes, and were conducted by the lead author, a native of Jordan and professional scholar.
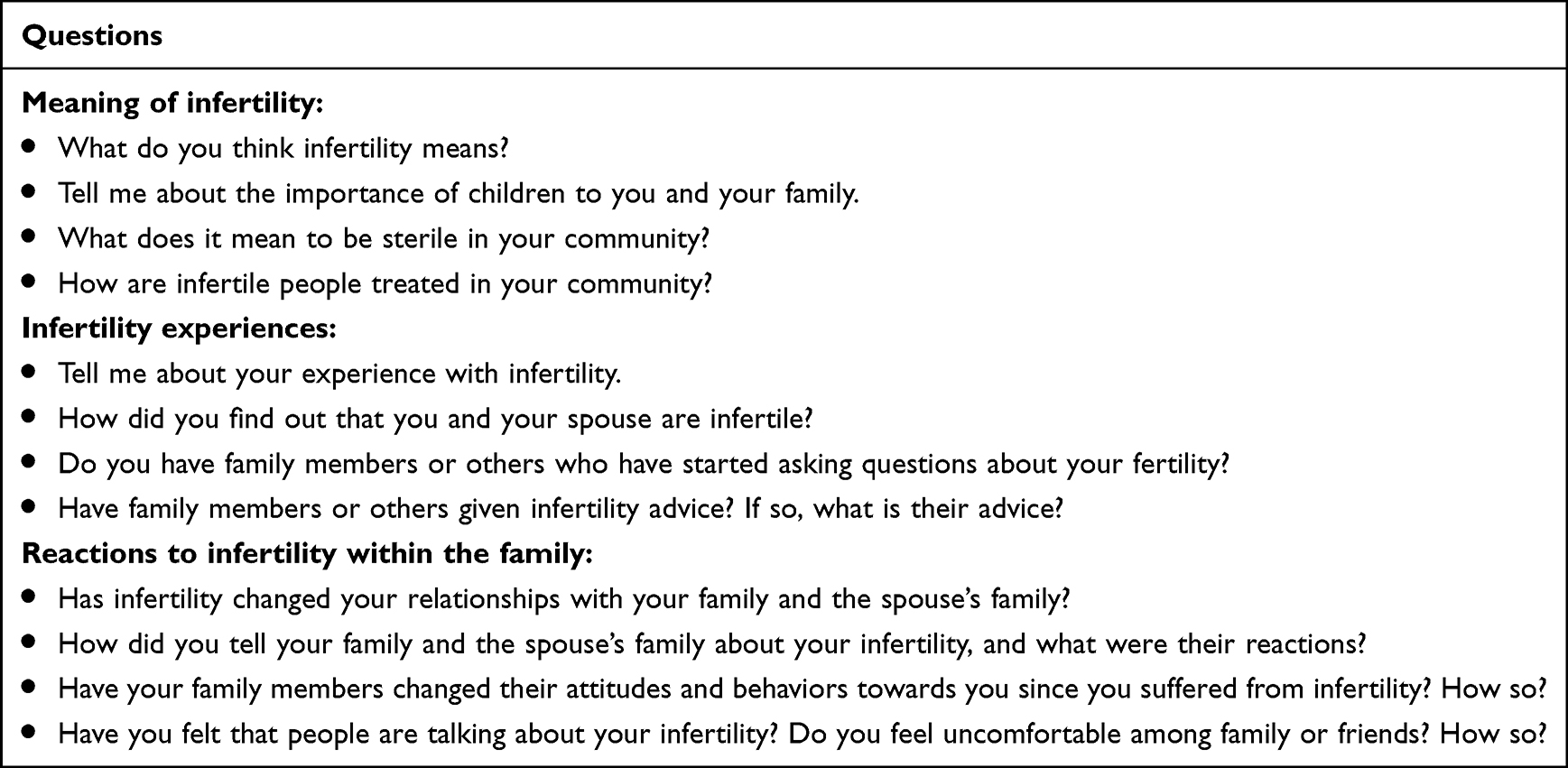 |
Table 1 Interview Guide |
Data Analysis
Upon completion of each interview, the audiotaped dialogue was transcribed verbatim in the Arabic language as soon as possible before being translated into English. The English text was imported into the NVivo 9 program (QSR International Pty Ltd, Doncaster, Victoria, Australia), which assists in organizing and categorizing data by labeling each paragraph with phrases that convey a specific standpoint, perspective, or concept. The first author conducted an analysis of the data using the interpretative phenomenological analysis (IPA) framework, as outlined by Smith et al. Utilizing the categorized data generated by the NVivo program, the analysis continued with the IPA principles being applied by hand. Single phrases were assigned to a group of sub-phrases that encompassed strongly linked ideas. Each phrase and its sub-phrase were linked to a fundamental idea that explained its meaning. The research team then arrived at a consensus to identify the themes from each idea through detailed discussions. Quotes extracted from the interviews were collated into a resulting list of themes.
Ethical Consideration
Ethical approval was sought through the Jordan University of Science and Technology (JUST) Institutional Review Board, along with review boards at Emory University and the RMS site. The researchers took care to assure the women that they were free to decline to participate and were under no obligation to do so. Informed consent was obtained from all participants prior to starting the interviews and the participants informed consent included publication of anonymized responses. All data were anonymized at the time of entry. The researchers opted to conduct the interviews at IVF clinics to ensure their own safety and that of the respondents. To ensure that the participants were treated with sensitivity, and with the aim of reducing their distress, the data collector underwent training in how to interact with them appropriately. The conduct of survey adhered to the principles of the Declaration of Helsinki.
Trustworthiness of the Study
The dependability, credibility, confirmability, and transferability criteria were followed to ensure the rigor of this investigation.19 A discussion was held between the first author and the research team about the emerging themes and their interpretations, and their remarks were taken into consideration. Some of the participants requested the opportunity to review the final list of themes to ensure that the analysis gave a true reflection of their expressed opinions, experiences, and needs. The authors naturally complied with their request.
Results
Thirteen women were interviewed individually. It should be noted that the experiences of women with infertility vary, as they take different cycles and lead to different consequences depending on the circumstances in which they occur. It should be understood that the experiences reported by women in this study are not intended to be representative of all infertile Jordanian women, whose experiences may differ from those presented here. In this study, there were women who described their mental health as fair, while others described it as poor. Furthermore, the etiology of infertility varied among participants, with seven attributing it solely to themselves, three to their spouses, and another three women the cause of infertility was shared by the husband and wife. It should therefore be born in mind that this analysis has emerged from the experiences of the particular group of women under study. The women share the following characteristics. The demographic data for the participants are listed in Table 2.
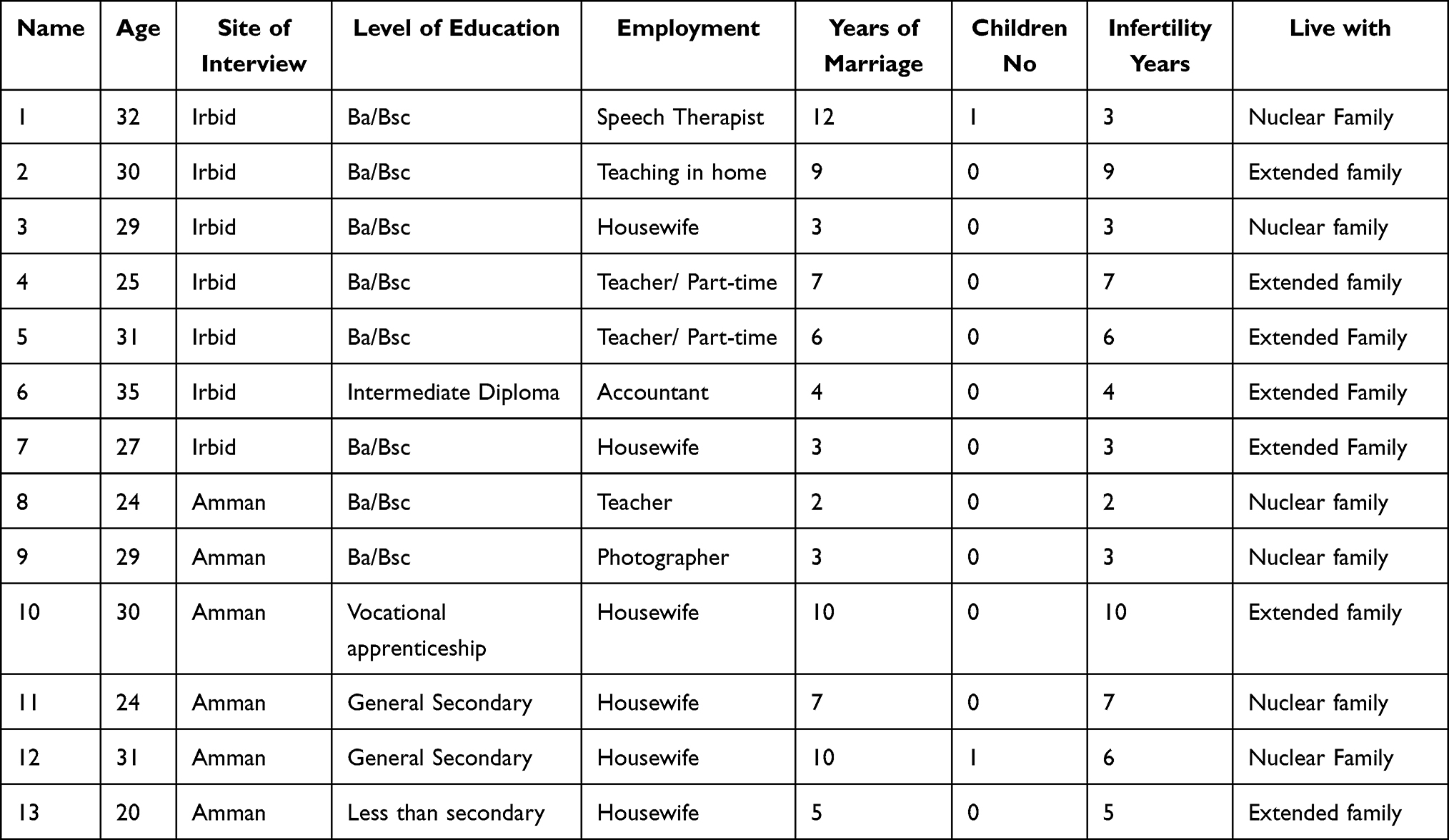 |
Table 2 Participants’ Demographic Data |
This paper is a part of series of publications about the violence against infertile women. This paper describes one part of the violence that infertile women are exposed to in Jordan, which is societal violence. Five main themes emerged from the analysis:
How the Surrounding People View Me as an Infertile Woman
A woman’s social status often depends on her reproductive achievement and her biological capacity for fertility and childbearing. The inability of the woman to carry out her traditional functions in pregnancy and childbearing constitutes an important driver in the unjust view of society and can become the sources of tension and conflict within the family. The existence of real suffering is borne by females due to the phenomenon of infertility and the attendant unjust societal repercussions in dealing with an infertile woman.
You feel that they look at you with a look of pity. They say things like ‘May God help you’ or ‘May God give you [a child]’. I feel that I am less than them. (P 10)
The thing that most breaks you is a look of pity, the view that this person is missing something. (Crying)… Relatives tell you that God will compensate you. I mean, this is a sweet thing to say, but it hurts. (Participant cries) (P 13)
Crying was the common factor in all interviews with the participants. The poor psychological health was a common trait among them, even those who have adapted to the issue of infertility and are now seeking treatment. They were narrating their stories with many tears, recounting how they have become very sensitive to the issue, even misinterpreting comments from others. The pressure and interference they experienced clearly negatively affected their self- confidence and felt themselves to be less than other women:
One day, I got into a taxi with another woman, and she asked me about the duration of the marriage, so I answered her for two years, and her reaction was that she was very sad and said, ‘Poor thing, may God give you [a child].’ I start crying in the taxi because of the tone of her voice. (P 8)
Although the problem of delayed childbearing, or what has been termed as “infertility”, affects both males and females equally, most of its psychological, health, and social consequences usually fall on the shoulders of females - especially in Middle Eastern societies, which are distinguished by the peculiarity of their social and cultural structures - and the one-sided attitudes and practices that it includes for women, surrounding them with their traditional roles “as a wife, mother, housewife, and conduit for having children”.
Society does not blame the man, but always puts the blame on the wife, because they see that the man is normal. There is nothing wrong with him, and the symptoms always come from the wife. She is the reason, including infertility. (P 6)
I Am Suffocated by Their Questions; They Interfere in the Smallest Details
Some participants reported that the question about pregnancy from the people surrounding the spouses starts from the first period of marriage, that is, during the first 3 months because the goal of marriage from the perspective of Jordanian society is to procreate.
My father-in-law wants to ask about the delay in childbearing. He asks my husband in private and not in front of me. My family and my female co-workers who teach with me are repeatedly asking about the reason for the delay, out of curiosity. (P 9)
Questions from family about pregnancy were many and urgent. Interference from the husband’s family from the beginning of the marriage was strong and it was common for the women to be advised to go to the doctor and reveal the reason for the delay in pregnancy. This caused a lot of stress and discomfort for some women.
I went to the doctor, of course, because of the pressure from my mother-in-law. She keeps telling me to go to the doctor, even though I have only been married for 4 months. (P 3)
Most of the participants stated that the people’s questions surrounding them caused them a lot of tension and harassment, but the level of social pressure varied according to the age of the woman, the length of her marriage, and which spouse was sterile. However, one of the participants, who had been married for 2 years, stated that she has not been subjected to psychological pressure because of the questions because she has a lot of time:
I am fortunate because I am not being pressured by those around me. (P 8)
Other participants, who had suffered from infertility for long periods, found that, with the passage of time, they got used to the questioning because they had no other option:
In the beginning, their questions affected me a lot, but now, after 10 years, I am used to these questions, and I accept it. (P 10)
Women whose husbands were the source of infertility mentioned that they are no longer being bothered by questions because the problem of infertility is from the man and not from them, so the feeling is different because she is not accused of negligence:
Yes, there are frequent questions, but I do not feel disturbed. Everyone knows that my husband suffers from a problem (zero sperm), which is the reason for the delay in childbearing. (P 11)
Some mothers-in-law did not accept that the cause of infertility came from the man and denied it. For them it was emasculating to their sons. To hide the fact that their son has a problem with childbearing, they demanded that their son marry again and did not hesitate to insult the wife:
My husband went and told his mother … that the doctor said that my wife did not have a problem and that he had problems that delayed childbearing. She said this is not true and that her son does not suffer from any problem and that she is sure that the problem lies with his wife and asked him to marry another. As for my sisters-in-law. (P 13)
The most disturbing cause for women is the interference of those surrounding them in their personal lives and their details. Everyone wants to know the cause of the problem, and the nature of the problem. In addition, the husband’s mother sometimes interferes in the marital relationship and wants to follow the smallest details:
The wives of my brothers-in-law repeat their questions, and they want to know the details, and sometimes they deny what I say and confirm that there is a strong reason for my delay in having children. The neighbors always want to know what the doctor said. (P 7)
What bothers me the most is my mother-in-law’s repeated question about the date of my period and whether my period came this month, or not. (P 2)
I Got Burned and Turned to Ashes, and I Have No Right to Complain
Most of the time, the women felt that they were being given additional burdens by the family because they did not have children, so they had to help any family member without asking for their consent or whether they had the energy or time to help. The women described that this exploitation bothered them greatly, but that they could not object or refuse:
If guests are invited to lunch at my in-laws’ house, I must be present at their house in the morning to help with cooking food and other household chores, because I do not have children, so I must always be there to help. (P 2)
From the point of view of others, you do not have children. You do not have responsibilities. You should always be available for help regardless of your mental or physical condition. It is forbidden to complain that you are tired or busy. (P 11)
Some participants did not object to providing assistance to any family member who needed to do so. The ladies only asked that there be some sympathy for their situation and to take into account that their psychological situation is bad most of the time due to not having children, and how much they wish to have a child, so how can they provide assistance and share with another woman her joy because she gave birth and take care of her and not take into account her feelings:
Anyone who has a hospital appointment must accompany him. Any woman from the family who has given birth, go and help her in the first week of giving birth. No one cares that you are suffering because you do not have children. Complaining is forbidden and you do not have the right. (P 6)
The women had no solution but to remain patient, make supplication to God, and to cry. These are their only options to escape their ordeal and strengthen themselves to face society:
In the fifth year of infertility, my life became very difficult. When I hear about any woman getting pregnant, my soul feels destroyed, and I spend a whole day crying. It is difficult for me. (P 5)
Some of the women had a family that cared for their emotions and the people around them became aware of the difficulty of the situation for the spouses. So, they avoid mentioning the subject of children in front of them too much:
They do mention the issue of pregnancy, but it is very rare and not directly. (P 12)
Some women were less fortunate than others. The husband’s family put enormous psychological pressure on them, as one participant said:
My husband’s mother and his sisters didn’t say a kind word to me at all. My sisters-in-law keep saying that they are better than me because they can have children. (P 11)
Most of the participants reported that they are now living in social isolation and that they prefer this situation. Staying away from people is more comfortable for them. Women feel that people’s eyes are watching them from all sides, and they feel everyone whispering, so they decided to isolate themselves so that they do not hear people’s comments and constant hints. Their psyche cannot bear more, and society is cruel:
Now I avoid most of my work friends and neighbors. I don’t want to see anyone. (P 9)
I hate to go out of my house. (P 4)
Some women even cut ties with close friends. They want to take a break from everyone. This indicates the difficult psychological situation that the participants are living in and the entry of most of them into a state of frustration:
I stopped going to them at all. My friends contact me, but I am bored, and my psychological state is destroyed. (P 5)
The Problem of Childbearing and the Treatment Plan is a Matter for Me and My Husband Only
Most women told us that they do not prefer to disclose the cause of the infertility problem and to discuss it with relatives and friends. This is because people interpret things according to their whims and do not rely on any scientific basis. Therefore, some women in the study found that keeping the reality of their reproductive status between them protected them against being viewed differently by society, which will negatively affect the woman’s relationship with herself, her husband, and her society:
I do not like to go into details because if I told people that I have weak ovulation, this will stay stuck in their minds for life. They say she has a big problem, while with doctors, it may be a simple problem. When they ask me, I never give them details. I always say that I don’t have anything, nor does he have anything. (P 1)
Most of the participants preferred to hide the nature of infertility. Also, they were keeping the treatment plan a secret. The participants made it clear that they did not want to be subjected to more pressure from people and pursued by their questions about whether the treatment is successful or not, and people follow up on the details of the treatment plan:
For the first two years, I did not tell anyone I was being treated. Of course, the first time I had an egg planted, I did not tell anybody. My husband took care of me at home. (P 3)
Who Supports Me and What Do I Want from Those Around Me?
Most of the women explained that they were constantly receiving support from their parents. Often the wife’s family was the main source of support. As for the nature of the support, it was divided into moral support in encouraging women, raising their morale, and praying for them:
My Family Supports Me More, Especially My Sister… Saying, “God Willing, Things Will Be Resolved. (P 12)
Some women reported that the support was also financial. The parents donated the costs of the treatment, especially when making an IVF:
My mother and father are more affectionate with me. They often think about my condition, and my sister too. They told me, “Go and make an IVF baby and we will give you money. Don’t think about the costs. (P 1)
My mother-in-law provided financial and moral support, as she secured the money to try to make an IVF baby, and when this experiment failed, she said, “No problem and age is ahead of you. (P 7)
Most of the women praised the support given to them by the family. But because of the great psychological pressure they felt from others, including family members, they preferred to forgo the support to avoid hurtful questions and comments.
I want from them to leave me alone. Not interfere in my life. I am the type who does not interfere with anyone, so I do not want anyone to interfere with me. (P 6)
I don’t want support from them. I just want them to stop their questions and hints. (P 4)
Ultimately, the insecurity bothered the women a lot. They wanted a sense of stability, a feeling of security from their husbands and families-in-law, and were resigned to the fact that Allah had not given them children:
I wish I could feel safe.(crying).My life is unstable, and it is possible for my husband to leave me at any moment because of the pressure from people around him. (P 2)
The participants agreed that it was spiritual practices and pure worship of God that were rebuilding their fragile psyche. When they were communicating with God through their prayers, they felt calm and comfortable, and that God was with them and would choose what was best for them:
The thing that makes me feel most comfortable and hopeful is getting closer to God through prayer and supplication. After all the difficulties I have been through, people may give me some temporary relief, but God gives me the strength and patience to continue my life”. (P 5)
Discussion
This study supports the understanding that infertility negatively impacts the social and psychological experiences of women seeking infertility treatment in Jordan. The existing literature indicates that, throughout the Middle East, women who have fertility problems and the wives of men with fertility issues face high levels of depression and anxiety,3 reflected in this study where women discuss overwhelming despair and constant crying caused by the words of those around them. Conversations with the intended mothers suggest internalization of society’s blame placed upon them for infertility, where their perceived lower social status results in poor self-image and distress. However, with some interviewed women describing how those around them intentionally do not bring up their infertility to support them, this study suggests, to some extent, how the unspoken nature of infertility may also covertly reinforce stigma.
Substantially responsible for the emotional distress involved with infertility in the Middle East, the high prevalence of in-law violence discussed in this study largely explains the internal experiences of infertile wives in Jordan. It is well documented that women in the Middle East experience violence because of their condition, including psychological and emotional violence which are the most common forms inflicted by family members other than a woman’s spouse.20
As intended mothers continuously face social pressure for childbearing, women in this study further explain their internal reactions to the responses of those around them. Some express extreme offense to repeated questioning, while others resign to external curiosity due to an inability to stop the constant inquiries. Those who internalize the pressure may go out of their way to avoid questions by not attending social gatherings, while others give in to their in-laws’ demands to frequently visit the doctor in search of alternate explanations for their infertility. This aligns with existing studies that document similar responses and coping mechanisms in Jordan and other Middle Eastern countries.6,9 Some women in the study feel comforted through self-reasoning, searching for explanations that relieve themselves of personal responsibility for their conditions. Young, intended mothers express that questions about their infertility do not bother them due to their age, convinced that the condition will inevitably resolve itself, while others find relief by placing their trust in God’s will to deny them a child. As women self-reason to reduce stress, generally still the intended mothers incorporate others’ pity and prying into a degrading view of themselves that demands intentional action for them to personally resolve the infertility problem. Relieving infertile women from social pressure and repeated questioning requires a combination of education, advocacy, setting boundaries, and fostering a supportive environment. Empowering infertile women in Jordan and reintegrating them into society involves a holistic approach that addresses their physical, emotional, social, and economic needs. Infertile women should be encouraged to communicate openly with family, friends, and colleagues about their situation, setting clear boundaries regarding questions or comments about their fertility status. Assertive communication can help deter intrusive inquiries.
Women in Jordan experience a higher perceived need for parenthood than men.21 This is likely due to deeply rooted social expectations placed upon them for childbearing. Existing literature indicates that women in Arab societies disproportionately carry the emotional burden of infertility, even when it has been medically confirmed that the husband is the infertile partner.22 Intended mothers in this study, however, mention relief brought from the discovery that their husbands were the cause of the couples’ infertility, suggesting that women may release some, but not all, internal liability when faced with objective proof of their spouse’s responsibility for the circumstances. As women describe their in-laws’ denial of the husbands’ influence on the infertility, intended mothers continue to emotionally carry the external blame assigned to them regardless of their own abnegation of guilt. So in supporting the infertile women health care providers should include partners in counseling sessions or support groups to address the impact of infertility on relationships and promote open communication and mutual support between couples.
Previous studies largely discuss the differential experiences of social pressure and support for infertile women in Arab societies, with family members more often than non-kin relationships serving to encourage and support infertile couples.23 This study similarly recognizes the positive impact of a woman’s natal family but also brings up the possibility for couples to reject familial support in turn for comfort brought by social isolation. While some families have positive intentions with their support, interviewed women describe a desire to make treatment plans without external opinions; intended mothers increasingly seek health agency in a society where extended family traditionally involves itself in children’s life choices.23 This also indicates how women may unintentionally inflict greater distress on themselves when facing infertility by misinterpreting others’ support as invasive, leading to potentially harmful self-imposed isolation.
Limitations of the Study
Interpretive phenomenological studies typically involve small sample sizes. The methodology and the limited number of participants enable the researcher to explore the participants’ experiences in great depth. However, these factors make it more difficult to generalize the findings to a broader population. In this case, our objective was to understand the lived experiences of the participating infertile women, rather than obtaining generalizable results.
When conducting an interpretive phenomenological study, the researcher is inherently actively involved in the interpretation and analysis of the data. Consequently, he/she must acknowledge the importance of not allowing the results to be biased by personal values, opinions, and preconceptions. It is thus imperative that the research team engage in regular debate and collaborate closely in the process, ensuring that a full range of interpretations are taken into consideration, thus reaching a more comprehensive understanding of the data.
Conclusion
In conclusion, this study has yielded a valuable overview of the societal violence encountered by infertile women in Jordan. By making an in-depth examination of participants’ lived experiences, this research illuminates the various aspects of societal violence and how its presence impacts the lives of infertile women. The findings make it clear that greater efforts are needed to better comprehend the social and cultural factors that facilitate and condone this particular type of violence. There is evidently a need for a fundamental change in how society views and treats infertile women. Ultimately, the research findings indicate the necessity of a broader societal dialogue, greater awareness, and effective interventions to ameliorate the position of infertile women within their society. Armed with a better understanding of the challenges and needs of women who are unable to conceive, we are better positioned to prevent them from being stigmatized and excluded by society. Instead, we can work to ensure that they receive the appropriate support, and create a society that is more inclusive, embraces diversity, and promotes empathy, respect, and equality for all individuals, regardless of their reproductive status.
Future studies needed to include a greater number of Jordanian infertile women of varying socio-economic status and educational levels.
Implications for Nursing and Health Policy
This study makes a valuable contribution raising awareness of the problem of societal violence against infertile women. It is important because it actually gives voice to their experiences and sheds light on their struggles. The results gleaned from this study can be used to inform policymakers and healthcare professionals, and support organizations in the creation and development of appropriate practices that can aid women to face and overcome the societal violence they encounter as a consequence of their infertility.
Ethical Approval
Ethical approval was received by the Institutional Review Boards of Emory University (MOD002-STUDY00003211) and Jordan University of Science and Technology (Ref: 6/141/2021).
Funding
This research was supported by the Sexual Violence Research Initiative (SVRI), South Africa.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization. Infertility. World Health Organization; 2020.
2. Department of Statistics/Jordan I. Jordan Population and Family Health Survey 2017–18. Amman, Jordan, and Rockville, Maryland, USA: Department of Statistics/Jordan I; 2019.
3. Vioreanu A-M. The psychological impact of infertility. Directions for the development of interventions. Mental Health. 2021;4:1.
4. Mahadeen AI, Hamdan-Mansour AM, Habashneh SA, Dardas LA. Sexual satisfaction among infertile couples: demographics and psychosocial health factors. J Psychos Nurs Ment Health Serv. 2020;58(9):40–47. doi:10.3928/02793695-20200812-01
5. Alia M, Ayman M, Jehad AH, Samira AH, Aya BK. Psychosocial wellbeing of infertile couples in Jordan; 2018.
6. Daibes MA, Safadi RR, Athamneh T, Anees IF, Constantino RE. ‘Half a woman, half a man; that is how they make me feel’: a qualitative study of rural Jordanian women’s experience of infertility. Culture Health Sexuality. 2018;20(5):516–530. doi:10.1080/13691058.2017.1359672
7. Obeisat S, Gharaibeh MK, Oweis A, Gharaibeh H. Adversities of being infertile: the experience of Jordanian women. Fertil Sterility. 2012;98(2):444–449. doi:10.1016/j.fertnstert.2012.04.036
8. Öztürk R, Bloom TL, Li Y, Bullock LF. Stress, stigma, violence experiences and social support of US infertile women. J Reprod Inf Psychol. 2021;39(2):205–217. doi:10.1080/02646838.2020.1754373
9. Hasanpoor-Azghady SB, Simbar M, Vedadhir AA, Azin SA, Amiri-Farahani L. The social construction of infertility among Iranian infertile women: a qualitative study. J Reprod Inferti. 2019;20(3):178.
10. Rahebi SM, Rahnavardi M, Rezaie-Chamani S, Nazari M, Sabetghadam S. Relationship between domestic violence and infertility. East Mediterr Health J. 2019;25:8. doi:10.26719/emhj.19.001
11. Stellar C, Garcia-Moreno C, Temmerman M, van der Poel S. A systematic review and narrative report of the relationship between infertility, subfertility, and intimate partner violence. Int J Gynecol Obstet. 2016;133(1):3–8. doi:10.1016/j.ijgo.2015.08.012
12. S-u-N H, Zahra A, Parveen N, Iqbal N, Mumtaz S, Batool A. Quality of infertility care services and emotional health of South Asian women. Psychol Res Beh Manag. 2022;1131–1146. doi:10.2147/PRBM.S357301
13. Hanna E, Gough B. The social construction of male infertility: a qualitative questionnaire study of men with a male factor infertility diagnosis. Sociol Health Illness. 2020;42(3):465–480. doi:10.1111/1467-9566.13038
14. Malagon-Maldonado G. Qualitative research in health design. HERD Health Env Res Des J. 2014;7(4):120–134. doi:10.1177/193758671400700411
15. Van Manen M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Routledge; 2016.
16. Dworkin SL. Sample Size Policy for Qualitative Studies Using in-Depth Interviews. Springer; 2012:1319–1320.
17. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs—principles and practices. Health Serv Res. 2013;48(6pt2):2134–2156. doi:10.1111/1475-6773.12117
18. DiCicco‐Bloom B, Crabtree BF. The qualitative research interview. Medical Education. 2006;40(4):314–321. doi:10.1111/j.1365-2929.2006.02418.x
19. Lincoln YS, Guba EG. Naturalistic Inquiry. sage; 1985.
20. Sharu E. Research Paper on Infertility in Jordan. Amman: Jordan Higher Population Council; 2020.
21. Jaber DJ, Basheer HA, Albsoul-Younes AM, et al. Prevalence and predictive factors for infertility-related stress among infertile couples. Sau Med J. 2022;43(10):1149–1156. doi:10.15537/smj.2022.43.10.20220411
22. Turner KA, Rambhatla A, Schon S, et al. Male infertility is a women’s health issue—research and clinical evaluation of male infertility is needed. Cells. 2020;9(4):990. doi:10.3390/cells9040990
23. Kavas S, De Jong J. Exploring the mechanisms through which social ties affect fertility decisions in Turkey. J Marr Family. 2020;82(4):1250–1269. doi:10.1111/jomf.12668
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.