")
Back to Journals » Open Access Surgery » Volume 16
Impact of War and COVID-19 on Major Surgery in a Tertiary Hospital in Tigray, Ethiopia: An Interrupted Time-Series Study
Authors Gebresilassie KB, Tequare MH , Gebremedhin MB, Tesfamariam WB , Tekle TH, Gebremedhin TT, Berhie KA , Berhe H, Abraha HE
Received 21 March 2023
Accepted for publication 31 May 2023
Published 14 June 2023 Volume 2023:16 Pages 49—54
DOI https://doi.org/10.2147/OAS.S411401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Kibrom Berhanu Gebresilassie, Mengistu Hagazi Tequare, Micheal Berhe Gebremedhin, Wegen Beyene Tesfamariam, Tesfay Hailu Tekle, Teame Tekleab Gebremedhin, Kidanemariam Alem Berhie, Hailemariam Berhe, Hiluf Ebuy Abraha
Mekelle University, College of Health Sciences, Mekelle, Ethiopia
Correspondence: Wegen Beyene Tesfamariam, Department of Medical Biochemistry & Molecular Biology, School of Medicine, College of Health Sciences, Mekelle University, P.o.box 1871, Mekelle, Ethiopia, Fax +251 0 344416681, Email [email protected]
Objective: To determine the effect of armed conflict and COVID-19 pandemic on the level and trend of surgical volume at Ayder Comprehensive Specialized Hospital, Tigray, Northern Ethiopia.
Methods: All major surgeries carried out over four consecutive years were included and subjected to an interrupted time-series analysis called segmented regression analysis to examine the effect of war and COVID-19 on level of and trend changes in major surgeries. The outcome was measured and estimated that there was a significant change in the number of major surgeries as a result of the conflict and COVID-19 pandemic compared to the baseline status.
Results: We analyzed 29,877 major surgeries conducted during the study period. The results indicate that, before the beginning of the intervention period, on average 632 surgeries per month were performed [632.1 (95% CI: 575.8, 688.41)]. Right after COVID-19, however, this number dropped by 359 patients per month [− 359.3 (95% CI: − 486.4, − 232.2)]. During the war period, the number of surgeries decreased by 232 patients per month [− 232.7 (95% CI: − 408.5, − 56.9)].
Conclusion: This study revealed that both COVID-19 and the war in Tigray have significantly reduced the number of major surgeries that could have been carried out in their absence at a large tertiary hospital in Northern Ethiopia.
Keywords: surgery, trend, armed conflict, COVID-19, Tigray, war
Introduction
War has devastating effects for the communities that experience it, and these consequences can last even after the conflict has ended. The impact is deep and far-reaching, extending beyond the battlefield, country borders and period of active warfare. In addition to claiming many lives, conflict has the ability to shatter political, economic and social institutions and adversely affect a nation’s opportunities for sustainable development.1,2
During an armed conflict a collapsing healthcare system results in massive human and financial costs both during and after the conflict. Higher mortality among patients with chronic diseases, permanent disabilities for people with traumatic injuries, higher rates of maternal and infant mortality, and psychological trauma are some of the consequences of war on the health system. It is therefore expected that countries that have meet their national goals on health policy find that their healthcare system is in ruins after experiencing armed conflict.2,3
Though Tigray was one of the regions which had a relatively good healthcare system in Ethiopia, more than 80% of the health facilities were destroyed after the devastating war erupted on November 4, 2020.4 Among the 40 hospitals that were providing healthcare services, 21 are now non-functional, 12 are partially functional, although with severe limitations, and the status of the remaining 7 is unknown as they are under the control of the invading forces. Similarly, of the 228 health centers in the region, only 40 (17.5%) are functional, while the remaining 188 are either completely non-functional, partially non-functional or their status is unknown.5
Curfews and the national state of emergency due to the COVID-19 pandemic affected the pattern of healthcare services, including surgical procedures.6 As a result, the number of surgeries performed at hospitals has declined.6–8 In addition to the global burden that COVID-19 imposed on the health system, the fully-fledged war in Tigray, Northern Ethiopia may also have caused the health system of the region to decline. Therefore, this study presents the impact of the war and COVID-19 on the level of and trends in major surgeries performed in Ayder Comprehensive Specialized Hospital.
Methods
Study Area and Period
This study was conducted at Ayder Comprehensive Specialized Hospital, a tertiary hospital in Tigray, Northern Ethiopia. The hospital serves Tigray and some parts of neighboring Afar and Amhara regional states. The study was conducted from July 2017 to June 2021 (from July 2017 to February 2020 and March 2020 to June 2021, as pre-intervention and post-intervention periods, respectively.
Study Design
An interrupted time series design was used.
Population
The study population included all patients who had major surgery between July 2017 and June 2021.
Interventions
In this study we have two unintended interventions: the COVID-19 restrictions and war. In the time sequences, COVID-19 pandemic-related actions were the first intervention deployed by the government after the first COVID-19 case in Ethiopia was reported, in March 2020. Following the case confirmation, Tigray regional government declared a state of emergency on 26 March 2020, imposing travel restrictions and other restrictive measures which could limit the movement of people seeking to visit hospitals. In the analysis, the start of the first intervention, COVID-19 and its restrictions, was therefore considered to be from April 2020. The second intervention was the war in Tigray, which flared up eight months after the country confirmed its first COVID-19 case, in November 2020.
Data Collection and Source
The data was retrieved retrospectively from the hospital’s health management and information system (HMIS), which was collected on a monthly basis for the purpose of health data generation.
Sensitivity Analysis
Following the start of the war, all COVID-19 related restrictions were abandoned by default. In this scenario, sensitivity analysis was performed considering that COVID-19 and its restrictions had no effect on surgery during the war period. Therefore, we expect exactly the same finding from the first analysis, except for β4 (level change due to war) and trend change after war, β5.
Data Requirements and Measurements
For an interrupted time-series study to be robust, different papers may mention different criteria regarding the number of data points. Some researchers recommend that one should have at least 12 data points before and 12 data points after the intervention, with at least 100 observations in each data point.4 Others advise that as few as 3 data points pre- and post-intervention are required.9 Some even say there are no fixed criteria as to the number of data points.10 In our case, data were organized on a monthly basis with 48 sequential measures; 33 of the data points were baseline observations, when neither of the two natural courses of the interventions (war and COVID-19 pandemic) occur, and,15 of the data points were after the interventions took place.
Outcome Measures
Our outcome is count data: number of patients undergoing major surgery in the service areas. The outcomes, measured in level and trend changes, estimate whether there was a significant change in the number of surgeries performed as a result of the armed conflict and COVID-19 pandemic compared to their baseline pre-pandemic and pre-war status.
Operational Definition
Major surgery: surgeries that require general or regional anesthesia, involve opening great body cavities, have risk of severe hemorrhage, put the patient’s life at risk and need postoperative care, and require special anatomical knowledge, manipulative skills, and specific equipment.
Surgical volume: number of major surgical procedures performed during the study period.
Ethical Considerations
This study complies with the Declaration of Helsinki. It was registered at of the Mekelle University College of Health Sciences Institutional Review Board (MU-IRB 1964/2022) and the ethics committee has waived the need for informed consent from patients in retrospective research. Moreover, consent was obtained from the hospital’s HMIS officer and data of patients was collected anonymously and kept strictly confidential throughout the study.
Results
Descriptions of COVID-19 and War
During the study period, 29,877 patients who attended the operation room for surgery were included in the analyses. The mean number of patient visits for the baseline was 692 per month. After the COVID-19 pandemic and its containment measures, this figure dropped by 33.1%. The added effect of war resulted in an even greater percentage decline, at 31.1% (Table 1).
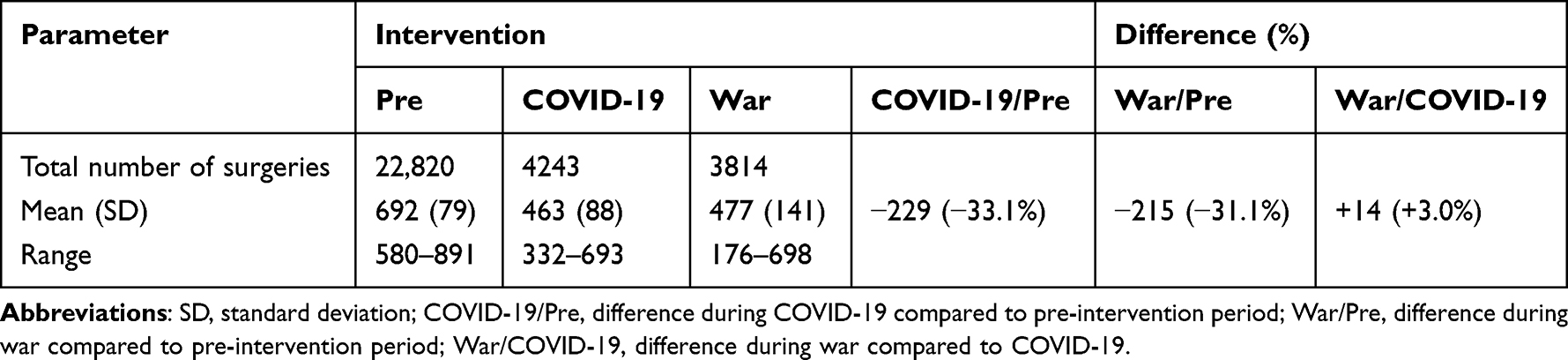 |
Table 1 Descriptive Statistics Related to Surgeries Performed Pre and During Intervention,Ayder Comprehensive Specialized Hospital, Tigray, Ethiopia, 2017–2021 (N=29, 877) |
The Effects of COVID-19 and War
The results indicated that before the beginning of the observation period, on average, there were 632 surgeries per month [632.1 (95% CI: 575.8, 688.41)], with a monthly increasing baseline trend [3.7 (95% CI: 692, 6.73)]. Right after COVID-19 and its restrictions, the number dropped by 359 patients per month [−359.3 (95% CI: −486.4, −232.2)]. The level of surgeries also decreased by 232 patients per month [−232.7 (95% CI: −408.5, −56.9)] during the war period (Table 2 and Figure 1).
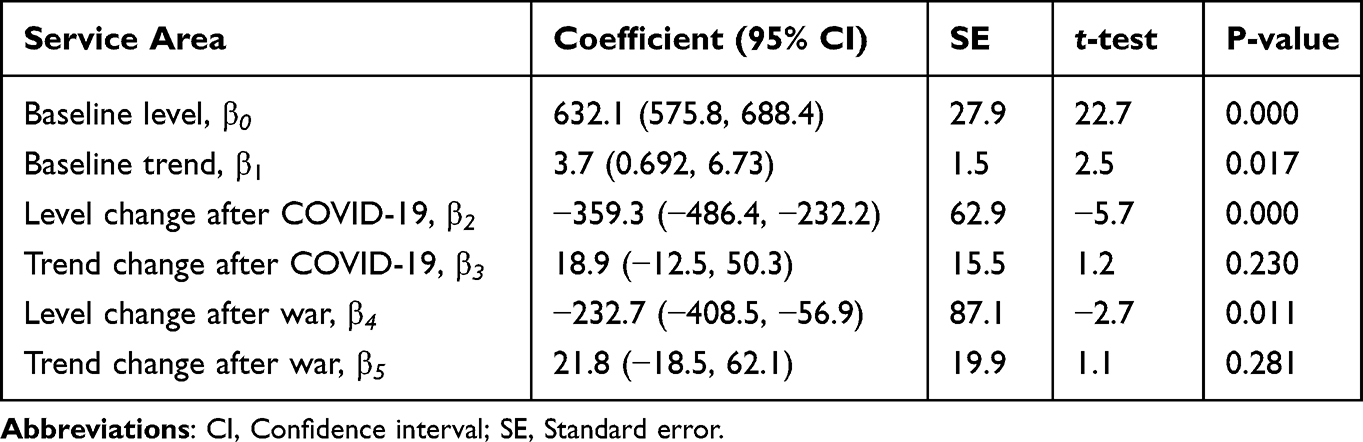 |
Table 2 Segmented Regression Analysis Models Predicting Levels of and Trends in Surgical Volume, Ayder Comprehensive Specialized Hospital, Tigray, Ethiopia, 2017–2021 (N=29, 877) |
 |
Figure 1 Level and trend of surgical volume in Ayder Comprehensive Specialized Hospital, Tigray, Ethiopia, 2017–2021 (N=29, 877). |
Sensitivity Analysis Findings
Surgical volume is not affected by COVID-19 alone; its containment measures, including travel restrictions and lockdowns, also had effects. We executed the analysis taking into consideration that COVID-19 restrictions were abandoned after the start of the war. The war caused a substantial drop in surgeries performed compared to the first analysis, where the impact of COVID-19 was presumed to continue in the same way even after the war broke out. Accordingly, after the war, the number of surgeries dropped by 460 patients per month (Supplementary Table 1).
Discussion
This interrupted time-series study was intended to evaluate whether the impact of COVID-19 and war had an effect on surgical service utilization of a tertiary care hospital in Tigray. It found that both COVID-19, with its imposed restrictions, and war led to an enormous reduction in surgical volume at Ayder Comprehensive Specialized Hospital, one of the top tertiary hospitals in Ethiopia.
This study revealed that there was a significant change in the mean number of major surgeries performed during the COVID-19 and war period as compared to the number of surgeries before the incidence of COVID-19 and war in Tigray. COVID-19 has reduced the mean number of surgeries performed by 33.1%. Similarly, the ongoing war in Tigray has also affected themajor surgeries which could be conducted in this tertiary care hospital, by 31.1%. This finding complies with studies from around the world (both developed and developing nations) revealing that COVID-19 has significantly affected health service utilization.11–14 Similarly, other international reports agreed with our finding that travel restrictions, lockdowns, and quarantine measures to prevent COVID-19 infection had significantly reduced surgical volume.4,5
In our case, the large reduction in patient visits caused by COVID-19 might have been exacerbated by the government’s minimal efforts to increase this community’s awareness of preventive measures.13
Compared to the baseline levels of and trends in surgical volume, the number of patients dramatically decreased by 359 per month, making this finding in line with a systematic review conducted on the effects of COVID-19.11
This study established that health service utilization, which was severely hit by COVID-19 and its restrictions, was further affected by the war in Tigray. Both the first and second sensitivity analyses uncovered that, following the armed conflict in Northern Ethiopia, access to major surgical services had significantly diminished by 233 patients, similar to studies conducted in Syria.15,16 This could be because people who live in a war zone face significant challenges in accessing healthcare services due to shortages of transport and medical services.17,18 In addition, lack of access to healthcare services could be the main reason for the decline in the number of surgeries performed and general medical services received, as the fully-fledged war in Tigray not only interrupted the referral service but also intentionally targeted health facilities and health professionals. Those who managed to arrive at the tertiary hospital were unable to cover their service costs as there was no access to banks and the community-based health insurance was not functioning at all since the war broke out.12,19
Limitation
It is not an easy task to uncover the entire impact of the war on Ayder hospital services. Doing so requires meticulous investigation while controlling for other important variables which might have positive or negative impacts.
Conclusion
This study disclosed that both the COVID-19 pandemic and the devastating war in Tigray had negative effects on health service utilization. They have caused an enormous reduction in the surgical services which can be provided at the tertiary care hospital. The war, in addition to the pandemic, further affected the provision of major surgeries at a tertiary hospital in Tigray as compared to those conducted during the same period in another tertiary hospital, in Addis Ababa, Ethiopia.20 COVID-19 has left an assignment for both local and international policy makers, health facilities and other stakeholder to stay tuned to and prepared to combat any pandemic which could arise at any time before it causes significant damage to the health system. Moreover, we recommend that the international community ensures that international humanitarian laws are respected and human rights (such as access to health services) are protected even during war times. We still want to call on the international community to immediately respond to the catastrophic damage to the health system in Tigray and provide lifesaving medical supplies to the needy people of Tigray, who are still under siege.21 Therefore, we recommend that governmental and nongovernmental organizations who are engaged in the health care delivery system must use innovative systems to overcome any other pandemic- or war-related problems.
Data Sharing Statement
The dataset used and/or analysed during the current study is available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funding for this work.
Disclosure
The authors declare that they have no competing interests.
References
1. Akseer N, Wright J, Tasic H, et al. Women, children and adolescents in conflict countries: an assessment of inequalities in intervention coverage and survival. BMJ Global Health. 2020;5:e002214. doi:10.1136/bmjgh-2019-002214
2. Sabes-Figuera R, McCrone P, Bogic M, et al. Long-term impact of war on healthcare costs: an eight-country study. PLoS One. 2012;7(1):e29603. doi:10.1371/journal.pone.0029603
3. Siem FF. Leaving them behind: healthcare services in situations of armed conflict. Tidsskr nor Laegeforen. 2017;137(17). Norwegian. PMID: 28925215. doi:10.4045/tidsskr.17.0524
4. Anonymous, Module 5, time series analysis. Pharmacoepidemiology: Behavioral and Cultural Themes. Newcastle: Center for Clinical Epidemiology and Biostatistics Australia; 2001.
5. Gesesew H, Berhane K, Siraj ES, et al. The impact of war on the health system of the Tigray region in Ethiopia: an assessment. BMJ Global Health. 2021;6:e007328. doi:10.1136/bmjgh-2021-007328
6. Mattingly AS, Rose L, Eddington HS, et al. Trends in US surgical procedures and health care system response to policies curtailing elective surgical operations during the COVID-19 pandemic. JAMA Netw Open. 2021;4(12):e2138038. doi:10.1001/jamanetworkopen.2021.38038
7. Centers for Medicare & Medicaid Services (CMS). Adult elective surgery & procedures recommendation: limit all non-essential planned surgeries and procedures, including dental, until further notice. Available from: https://www.cms.gov/newsroom/press-releases/cms-releases-recommendations-adult-elective-surgeries-non-essential-medical-surgical-and-dental.
8. Sevalie S, Youkee D, van Duinen AJ, et al. The impact of the COVID-19 pandemic on hospital utilisation in Sierra Leone. BMJ Global Health. 2021;6:e005988. doi:10.1136/bmjgh-2021-005988
9. The Cochrane effective practice and organisation of care group (EPOC). Available from: http://www.epoc.cochrane.org/Files/Website/Reviewer%20Resources/inttime.pdf.
10. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–355. PMID: 27283160; PMCID: PMC5407170. doi:10.1093/ije/dyw098
11. Moynihan R, Sanders S, Michaleff ZA, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. 2021;11:e045343. doi:10.1136/bmjopen-2020-045343
12. MSF. People left with few healthcare options as facilities were looted and destroyed in Tigray. Available from: https://msf-sa-press.prezly.com/tigray-ethiopia-msf-teams-report-that-70-of-106-health-facilities-they-visited-were-looted-30--damaged--just-13--percent-functioning-normally.
13. Scaramuzza A, Tagliaferri F, Bonetti L, et al. Changing admission patterns in paediatric emergency departments during the COVID-19 pandemic. Arch Dis Child. 2020;105:2–6. doi:10.1136/archdischild-2020-319397
14. Kalanj K, Marshall R, Karol K, Tiljak MK, Orešković S. The Impact of COVID-19 on hospital admissions in Croatia. Front Public Health. 2021;9(2020):1–11. doi:10.3389/fpubh.2021.720948
15. Ekzayez A, Alhaj Ahmad Y, Alhaleb H, et al. The impact of armed conflict on utilisation of health services in north-west Syria: an observational study. Confl Health. 2021;15:91. doi:10.1186/s13031-021-00429-7
16. Spiegel PB, Checchi F, Colombo S, Paik E. Health-care needs of people affected by conflict: future trends and changing frameworks. Lancet. 2010;375:341–345. doi:10.1016/S0140-6736(09)61873-0
17. REACH. Analysis of humanitarian trends in Luhansk and Donetsk Oblasts; 2018. Available from:https://reliefweb.int/sites/reliefweb.int/files/resources/reach_ukr_report_trend_analysis_june_2018.pdf.
18. Toni Joe Lebbos and Denizhan Duran. Health sector in Yemen – policy note; 2021.
19. Clarfield AM, Gill G, Leuner CJ, Moses AE, Paltiel O. An appeal to world leaders: health care for Ethiopians. Lancet. 2022;6736(22):6736. doi:10.1016/S0140-6736(22)00054-X
20. Ademe Y, Genetu A, Laeke T, et al. Impact of COVID-19 on surgical volume: single-center experience from Addis Ababa, Ethiopia. Ethiop J Health Sci. 2022;32(1):37. doi:10.4314/ejhs.v32i1.5
21. Aljazeera News. Blockade creates ‘hell’ in Ethiopia’s Tigray. Available from: https://www.aljazeera.com/news/2022/1/12/blockade-creates-hell-in-ethiopias-tigray-who.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.