")
Back to Journals » Open Access Surgery » Volume 16
Ileoileal Knotting as a Rare Cause of Acute Small Bowel Obstruction: Report of a Case with Review of Literature
Authors Mesfin T , Degefa A, Hassen IK , Gomora D, Sultan H, Seyoum K , Ibrahim E, Geta G , Ejigu N, Abebe SD, Tilahun T, Zenbaba D, Sahiledengle B , Desta F , Wakoya GK , Mohamoud SA, Tsegaye M
Received 24 August 2023
Accepted for publication 6 October 2023
Published 16 October 2023 Volume 2023:16 Pages 69—75
DOI https://doi.org/10.2147/OAS.S433281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Supplementary video of "Ileo-ileal knotting" [ID 433281].
Views: 402
Telila Mesfin,1 Abdella Degefa,2 Ibsa Kedir Hassen,1 Degefa Gomora,3 Hamza Sultan,2 Kenbon Seyoum,3 Elias Ibrahim,2 Girma Geta,3 Neway Ejigu,3 Sisay Dadi Abebe,4 Teketel Tilahun,5 Demisu Zenbaba,6 Biniyam Sahiledengle,6 Fikreab Desta,6 Getu Kusa Wakoya,1 Saddam Abdirahman Mohamoud,7 Mesfin Tsegaye1
1Department of Medicine, Madda Walabu University Goba General Hospital, Goba, Oromia, Ethiopia; 2Department of Surgery, Madda Walabu University Goba General Hospital, Goba, Oromia, Ethiopia; 3Department of Midwifery, Madda Walabu University Goba General Hospital, Goba, Oromia, Ethiopia; 4Department of Internal Medicine, Madda Walabu University Goba General Hospital, Goba, Oromia, Ethiopia; 5Department of Public Health, Menelik II Comprehensive Specialized Hospital, Finfinnee, Oromia, Ethiopia; 6Department of Public Health, Madda Walabu University Goba General Hospital, Goba, Oromia, Ethiopia; 7Department of Anesthesiology, Kalkaal Specialized Hospital 4J, Yakshid, Mogadishu, Somalia
Correspondence: Telila Mesfin, Department of Medicine, Madda Walabu University Goba General Hospital, P O Box 76, Goba, Oromia, Ethiopia, Tel +251931504321, Email [email protected]
Background: Small bowel obstruction is an acute surgical disease necessitating urgent diagnosis and intervention. Ileoileal knotting is a rare condition that can result in acute bowel obstruction and gangrene whereas ileosigmoid knotting is a relatively common surgical condition. There are few published studies so far on ileoileal knotting. Due to the scarcity of ileoileal knotting cases that have been published, the exact causes are not well known. We presenta rare case of small bowel obstruction which was managed successfully and had an uneventful postoperative period.
Case: A 45-year-old farmer from the rural kebele of Goba district of Bale Zone visited our institution with a complaint of sudden, colicky pain of 6 hours duration. On presentation, the pain was localized to the periumbilical area and then involved the whole abdomen. Associated with this, he had vomiting of ingested matter of three episodes. Objectively, he was in severe pain and tachycardic. On abdominal examination, there was direct and rebound tenderness over the periumbilical region. Abdominopelvic ultrasound revealed long segment ileoileal intussusception with adjacent mesenteric significant edema and proximal small bowel loop dilatation which was later found to be ileoileal knotting intraoperatively. The patient was put on intravenous fluid and antibiotics with a diagnosis of acute abdomen secondary to ileoileal knotting at the surgical emergency department. Exploratory laparotomy plus resection plus end to side ileotransverse anastomosis was done after written informed consent was received.
Conclusion: Ileoileal knotting is a rare condition that can result in acute bowel obstruction and gangrene. The diagnosis is usually made intraoperatively even though proper history, laboratory tests, and imaging are quite helpful. Clinicians should have a high index of suspicion of bowel knotting in patients with an acute abdomen and take early interventions to reduce the risk of gangrene.
Keywords: ileoileal knotting, bowel obstruction, gangrene, laparotomy, resection
Introduction
Small intestinal obstruction is one of the most prevalent acute surgical conditions requiring immediate diagnosis and care.1 It is a surgical emergency that causes 15% of all emergency department visits for acute abdominal discomfort.2 The most frequent causes of bowel obstruction are adhesions, neoplasms, and herniation, which account for 60%, 20%, and 10%, respectively.3 The intertwining of intestinal loops to form a knot is an uncommon cause of bowel obstruction. From all intestinal knots, ileoileal knotting is the rarest, with only a few cases reported in the literature.4 Intestinal knot development was first documented by Riverius in the 16th century and Rokitansky in 1836.1 Only a few instances of ileoileal knotting in children have been reported worldwide, and it mostly affects adults. Given the scarcity of ileoileal knotting cases that have been recorded, the specific causes are not fully known.5 We describe a rare case of small intestine obstruction that was effectively treated and had a smooth recovery.
Case Presentation
A 45-year-old male patient visited our facility with a complaint of abdominal pain of 6 hours duration. The pain was sudden, colicky, and maximal at the onset. Initially, it was localized to the periumbilical area and latter involved the whole abdomen. In addition to this, he had three episodes of vomiting of ingested matter. Otherwise, he had no failure to pass faeces and flatus. Similarly, he had no history of previous abdominal surgery, loss of consciousness, or trauma to his abdomen. He had no fever, chills, or rigors. He is an Oromo farmer from the rural area of the Goba district of Bale Zone. He cultivates mostly cereals and uses them as a staple diet.
Objectively, he was acutely sick looking. His vital signs were blood pressure 110/65 mmHg, pulse rate of 126 beats per minute, respiratory rate of 24 breaths per minute, temperature 36.7°C, and peripheral oxygen saturation 96% with intranasal oxygen. On head, ear, eye, nose, and throat examination, the conjunctiva was pink and the sclera was non-icteric. The pertinent positive finding was on abdominal examination. There was direct and rebound tenderness over the periumbilical region. There was formed stool on digital rectal examination. However, there were no signs of fluid collection, mass, or organomegaly.
He was investigated with laboratory tests and imaging. Likewise, complete blood count revealed white blood cell 12,000, hemoglobin 13 gm/dL, platelet 170,000, and neutrophil 84%. His blood group and Rh was A+. Chemistry tests were all in the normal range. Abdominopelvic ultrasound showed long segment ileoileal intussusception with adjacent mesenteric significant edema and proximal small bowel loop dilatation. The patient was put on intravenous fluid and antibiotics with a tentative diagnosis of acute abdomen secondary to ileoileal intussusception at the surgical emergency outpatient department.
After providing written informed consent the patient was taken to the operating room. Exploratory laparotomy was done through a vertical midline incision (see Supplementary Video). Intraoperative findings were hemorrhagic fluid all over the general peritoneum and gangrenous ileoileal knotting (Figure 1) involving the distal ileum, leaving only about 4 cm of terminal ileum from the ileocecal valve (Figure 2). Accordingly, hemorrhagic fluid was sucked out and the gangrenous segments were resected. Around 260 cm of small bowel was left behind the resection (Figure 3). End-to-side ileotransverse anastomosis was done (Figure 4). The mesentery was elongated and its defect was closed and the abdominal cavity was lavaged thoroughly with warm saline. The abdomen was closed layer by layer. Eventually, the patient was transferred to the surgical ward with stable vital signs.
 |
Figure 1 Gangrenous ileo-ileal knotting. |
 |
Figure 2 Tight ileal knots. |
 |
Figure 3 Gangrenous resected segment of the ileum. |
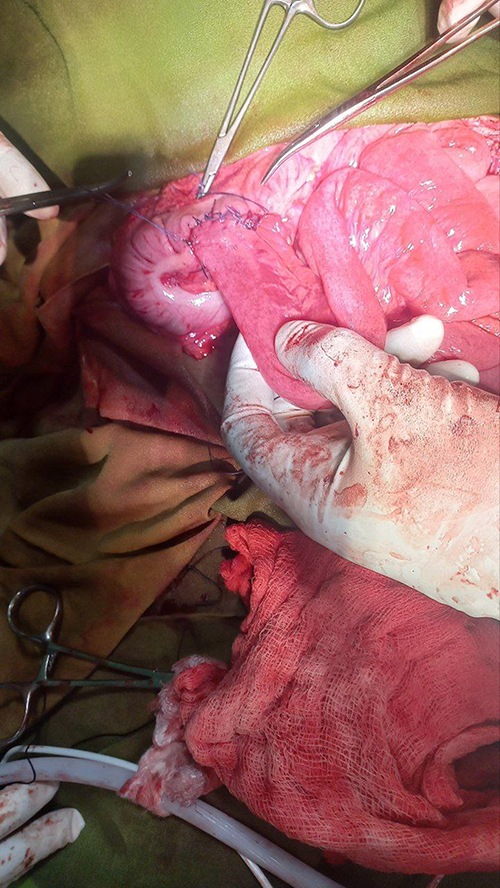 |
Figure 4 End to side ileotransverse anastomosis. |
He was put on maintenance fluid, analgesics, and intravenous antibiotics, ceftriaxone 1 gm intravenous twice per day, metronidazole 500 mg intravenous three times per day, Tramadol 50 mg intravenous three times per day, and diclofenac 75 mg intramuscular twice per day. The postoperative period was smooth and he was discharged after 5 days with an appointment after 2 weeks.
Discussion
Small bowel obstruction (SBO) is the most common surgical condition affecting the small intestine.6 It is a frequent emergency surgical condition. Small bowel volvulus and abdominal wall hernia are the two most typical causes of SBO in underdeveloped nations, including Ethiopia.7,8 The list also includes intussusceptions, adhesions, neoplastic diseases, and ileosigmoid knotting.9 Ileoileal knotting is a relatively rare condition that can result in acute intestinal obstruction and bowel gangrene.4 The ileoileal, ileosigmoid, cecosigmoid, and a loop formed between the colon and the appendix or Meckel’s diverticulum are among the various knotting kinds that were documented.10 Ileosigmoid knotting is the most prevalent type of intestinal knotting.11 Only a few occurrences of ileoileal knotting have ever been documented globally, according to the indexed literature.12 According to Beg,4 who conducted an extensive literature search from 1971 to 2019, there have been only 14 cases of ileoileal knots. Ileoileal knotting is a kind of closed-loop obstruction in which the ileum is divided into two parts, one of which is static and the other of which is coiled around it. Once a knot forms, it starts a vicious cycle of intestinal blockage, which is followed by persistent peristalsis and vascular compromise, all of which result in gangrene.1,13–15 Only a few occurrences of ileoileal knotting have been documented globally, and, to our knowledge, very few cases have been documented in Ethiopia.9,10,16 Unfortunately, we have never come across such cases so far at our institution and hence it is a good input for surgical societies.
The precise cause of ileoileal knotting is not well understood because there have only been a relatively small number of cases recorded. The proposed mechanisms leading to ileoileal knots are pregnancy, because it causes the displacement of bowel loops, loaded bowel with longer mesentery, abrupt or vigorous peristalsis, single bulky meal as during fasting, and intussusception associated with sudden strong peristalsis.4 Our case is from rural areas where high fiber cereals are cultivated and used as staple diet. This could probably be the cause for his condition.
It is quite challenging to diagnose intestinal knotting before surgery.16 Based on clinical history, such as the passing of “redcurrant jelly” stools, examination of the abdomen (looking for any lumps), and results from CT scan and ultrasonography, coexisting pathology, such as intussusception may be detected.17 It is always identified during surgery. An acute abdomen with abrupt onset abdominal distension is the typical presentation. The signs of intestinal obstruction can be seen on a plain abdominal x-ray taken when the patient is standing upright. If necessary, a CT scan of the pelvis and abdomen might be performed. The ability to detect any concomitant pathology is another benefit of CT scan.18 According to a recent case report from Ethiopia, when ileoileal knotting and intestinal obstruction are left undetected or the diagnosis is delayed due to a low index of suspicion, the morbidity and death rates are very severe. As a result of the clogged segment’s blood supply being cut off, gangrene and widespread peritonitis develop. Delayed diagnosis will result in higher morbidity and mortality rates.16 Literature indicated up to 9.5% mortality, and 34.9% of patients experienced complications when they were first seen.19 It was also reported that approximately 50% of the study participants visited health facilities 24 hours after being ill.19 In our case, abdominopelvic ultrasound was done and reported long segment ileoileal intussusception with adjacent mesenteric significant edema and proximal small bowel loop dilatation which was later found to be ileoileal knotting intraoperatively. Even though the patient arrived early and the investigation was hurried, intraoperatively the knotted bowel was not viable.
In contrast to the majority of SBO, ileoileal knotting lacks specific or recognizable signs and symptoms, with the exception of a rapid deterioration of the patient’s state. Similar to ileosigmoid knotting, discomfort is always the primary complaint. The patient is awakened from sleep by the sudden onset, which most frequently happens in the early morning hours. Vomiting frequently happens when the pain first appears. Ileoileal knotting differs from sigmoid volvulus, which is characterized by substantial distention, in that the patient does not typically complain of distention. Typically, the patient is in shock when they check into the hospital and has pale, dry skin. The majority of the time, gangrene and widespread peritonitis are noticed. The presence of a serious abdominal tragedy is typically very obvious.14,20,21 The literature reports gangrene rates of 78–80% with a substantial risk of morbidity and mortality.4,20 However, in certain cases, the knot might just be made up of one loose knot, in which case the bowel would still function normally and the knot could be readily undone.22 Similarly, our case presented with sudden onset of abdominal pain and vomiting of ingested matter. Likewise, there was no abdominal distension and he was not in shock on presentation.
Management should start with aggressive intravenous fluid resuscitation, nasogastric tube placement, and broad-spectrum intravenous antibiotics.9 Early intervention with an emergency laparotomy through a midline incision is required due to the seriousness of the effects of gangrene and peritonitis linked to knotting.23,24 Regarding the treatment of ileoileal knotting, various suggestions exist. Some advice is to release the knot first to assess how much of the small bowel can still be saved in order to prevent unnecessary bowel resection. Others, however, argue that the knot should not be untwisted to avoid contaminating the surgical site and allowing necrotic material to enter the bloodstream.24 However, since recurrence is uncommon, it’s usually advised to just untwist the knot on its own if the bowel is still alive and strangulation has not yet taken place.15 Following surgery, the patient should be checked for symptoms of anastomotic leak, anemia, and hydration status. Follow-up should check for symptoms of short bowel syndrome depending on how much of the small bowel is still present. Diet modification needs to be the first thing you do in this situation.10 Our patient was put on intravenous crystalloid antibiotics, and a nasogastric tube was inserted before exploratory laparotomy was done. Unfortunately, the bowel knots were not viable intraoperatively. Subsequently, the gangrenous segments of ileoileal knotting were resected and end-to-side ileotransverse anastomosis was done. The patient was okay after surgery and the postoperative period was uneventful.
Conclusion
Ileoileal knotting is by far the rarest surgical condition causing small bowel obstruction. The accurate diagnosis is usually made intraoperatively through exploratory laparotomy though proper patient history, laboratory tests, and imaging help a lot. Clinicians should be suspicious of intestinal knotting in patients with acute abdomen and intervene early to limit the risk of gangrene.
Data Sharing Statement
Data on the case clinical information, informed consent form, images and videos are available for review from the corresponding author upon reasonable request.
Ethical Approval
No ethical approval is required for this case report.
Consent
Written informed consent was taken from the patient for publication of his condition, accompanying video and images.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Prabhakar Krishna D, A Kishore, N Prasad, et al. Rare case of acute strangulated intestinal obstruction-ileo-ileal knotting. Int J Surg. 2019;3:24–25.
2. Jackson P, Raiji MT. Evaluation and management of intestinal obstruction. Am Fam Physician. 2011;83(2):159–165.
3. Cappell MS, Batke M. Mechanical obstruction of the small bowel and colon. Med Clin North Am. 2008;92(3):575–597. doi:10.1016/j.mcna.2008.01.003
4. Beg M, Bains L, Lal P, et al. Small bowel knots. Ann R Coll Surg Engl. 2020;102(8):571–576. doi:10.1308/rcsann.2020.0122
5. Knfe G, Tesfaye N, Tulicha T, et al. Ileoileal knotting as a rare cause of acute abdomen in adolescents: case report. Int J Surg Case Rep. 2023;105:107931. doi:10.1016/j.ijscr.2023.107931
6. Stewart B, Khanduri P, McCord C, et al. Global disease burden of conditions requiring emergency surgery. J Br Surg. 2014;101(1):e9–e22. doi:10.1002/bjs.9329
7. Tsegaye S, Osman M, Bekele A. Surgically treated acute abdomen at Gondar University Hospital Ethiopia. East Cent Afr J Surg. 2007;12(1):53–57.
8. Tegegne A. Small intestinal volvulus in adults of Gonder Region, northwestern Ethiopia. Ethiop Med J. 1992;30(2):111–117.
9. Mohammed M, Wondimu B, Abera E. A rare case report of viable ileo-ileal knotting of acute abdomen in adults. Int J Surg Case Rep. 2023;106:108285. doi:10.1016/j.ijscr.2023.108285
10. Abebe E, Asmare B, Addise A, Ileo-ileal knotting as an uncommon cause of acute intestinal obstruction. J Surg Case Rep. 2015;2015(8):rjv102. doi:10.1093/jscr/rjv102
11. Raveenthiran V. The ileosigmoid knot: new observations and changing trends. Dis Colon Rectum. 2001;44(8):1196–1200. doi:10.1007/BF02234644
12. Alver O, Ören D, Tireli M, et al. Ileosigmoid knotting in Turkey: review of 68 cases. Dis Colon Rectum. 1993;36(12):1139–1147. doi:10.1007/BF02052263
13. Shepherd J. Ninety-two cases of ileosigmoid knotting in Uganda. J Br Surg. 1967;54(6):561–566. doi:10.1002/bjs.1800540615
14. Cowley D, Iweze F, Spencer J. Knotting of the Small Intestine. SAGE Publications; 1971.
15. Kumar SS, Grace RD, Lavanya A. A rare cause of intestinal obstruction: ileo-ileal knotting. IOSR J Dent Med Sci. 2015;14:23–24.
16. Mohammed Y, Tesfaye K. Ileoileal knotting: a rare cause of intestinal obstruction: a case report. J Med Case Rep. 2021;15(1):1–3. doi:10.1186/s13256-021-02910-6
17. Cope Z. The Early Diagnosis of the Acute Abdomen. USA: Oxford University Press; 2006.
18. Kim YH, Blake MA, Harisinghani MG, et al. Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics. 2006;26(3):733–744. doi:10.1148/rg.263055100
19. Yilma Y. Management outcome of small intestinal obstruction in Mizan Aman General Hospital Ethiopia. J Clin Exp Pathol. 2018;8(6):359.
20. Pendse A, Prajapat G, Sharma A, et al. Ileo-ileal knotting causing intestinal obstruction. Indian J Pediatr. 1988;55(4):639–640. doi:10.1007/BF02868453
21. Dunkerley G. Intestinal obstruction due to knotting of two loops of small intestine. J Br Surg. 1953;41(165):66–70. doi:10.1002/bjs.18004116517
22. Uday S, Venkata PKC, Bhargav P, et al. Ileo-ileal knot causing small bowel gangrene: an unusual presentation. Int j Case Rep Imag. 2012;3(5):28–30. doi:10.5348/ijcri-2012-05-121-CR-6
23. Andromanakos N, Filippou D, Pinis S, et al. An unusual synchronous ileosigmoid and ileoileal knotting: a case report. J Med Case Rep. 2014;8(1):1–4. doi:10.1186/1752-1947-8-200
24. Kanamori K, Koyanagi K, Hara H, et al. Small bowel obstruction caused by a true ileo-ileal knot: a rare case successfully treated by prior ligation of mesenteric vessels. Surg Case Rep. 2021;7(1):1–6. doi:10.1186/s40792-021-01276-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.