")
Back to Journals » Clinical Ophthalmology » Volume 16
IgG4-Related Dacryoadenitis in Egyptian Patients: A Retrospective Study
Authors Salama OH , Ibrahim ENA , Hussein MO, Alkady AMM , Abd El-Salam ME , Ghanem S
Received 18 June 2022
Accepted for publication 10 August 2022
Published 23 August 2022 Volume 2022:16 Pages 2765—2773
DOI https://doi.org/10.2147/OPTH.S378583
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Omar Hassan Salama,1 Ezzat Nabil Abbas Ibrahim,1 Mostafa Osman Hussein,1 Ahmed Mohammed Madinah Alkady,1 Mohammed Eid Abd El-Salam,1 Saad Ghanem2
1Ophthalmology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 2Rheumatology and Rehabilitation Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Correspondence: Omar Hassan Salama, Lecturer of Ophthalmology, Faculty of Medicine, Al Azhar University, El Hussain University Hospital, Gawhar Al Qaed Street, Al Darrasah, Cairo, 11561, Egypt, Tel +201146316323, Email [email protected]
Purpose: To report clinical, serological, and histopathological findings in Egyptian patients with dacryoadenitis associated with ImmunoglobulinG4-related disease (IgG4-RD).
Methods: We retrospectively revised medical records of patients presented to Al-Azhar University Hospitals with lacrimal gland (LG) swelling between June 2016 and February 2022. We included patients with definite IgG4-related disease (IgG4-RD) diagnosis and excluded those with possible, probable, or unlikely IgG4-RD based on The Japanese Ministry of Health, Labour, and Welfare’s 2011 guidelines.
Results: Sixteen cases were included in the study (Fourteen females and two males, mean age 39.2± 12.2 years); Seven cases met the criteria of Mikulicz disease, and nine cases met full clinical, serological, and histopathological criteria. Mean reported serum IgG was 1792.5 ± 313.7 (range 1063– 2134) mg/dl, mean serum IgG4 was 576.25± 215.3 (range 112– 841) mg/dl, and mean Serum IgG4/IgG ratio was 31.9 ± 12.4%. The mean number of IgG4+ plasma cells/HPF was 74 ± 21.2, and the mean IgG4+ plasma cell percentage was 55 ± 9.7%. Serum IgG4 level showed a positive correlation to tissue IgG4+plasma cell percentage, while serum IgG4/IgG ratio positively correlated to both percentage and number of IgG4+plasma cells. Steroids had a good initial response, but recurrences were common.
Conclusion: A considerable proportion of patients with lacrimal gland swelling fall within the range of IgG4-RD. Proper diagnosis requires clinical, serological, and histopathologic correlation. Patients require long follow-up periods.
Keywords: IgG4-RD, IgG4-ROD, IgG4-related dacryoadenitis, Mikulicz disease
Introduction
Over the past two decades, IgG4-related disease (IgG4-RD) represented a newly identified disorder with variable fibroinflammatory manifestations that may involve one or more organs. Characteristic histopathologic features include storiform fibrosis, abundant infiltration with IgG4 positive plasma cells and eosinophils, and obliterative phlebitis. Other features may include peripheral eosinophilia and elevated serum levels of IgG4.1
In 2001, the Japanese first described the disease in association with primary pancreatitis as “autoimmune pancreatitis (AIP)”, where patients had elevated serum IgG4 levels.2
Characteristic serologic and histopathologic features of IgG4-RD were then detected in various extra pancreatic sites. Many pathologic conditions previously considered separate and unrelated disorders are part of the IgG4-RD spectrum.3
The Japanese Ministry of Health, Labour, and Welfare’s 2011 set the guidelines for IgG4-RD definitions. Based on clinical, serological, and histopathological diagnosis is set to Definite, probable, possible, or unlikely IgG4-RD.4
Orbital involvement is a common entity in IgG4-RD (Known as IgG4-related ophthalmic disease [IgG4-ROD]) as an isolated condition or part of the systemic disease. The most frequently involved site was the lacrimal glands, which was also one of the earliest reported extra pancreatic manifestations of IgG4-RD. Other ocular involvement patterns included the trigeminal nerve, extraocular muscles (EOMs), and orbital mass lesions.5
Purpose
To report clinical, serological, and histopathological findings in Egyptian patients with dacryoadenitis associated with IgG4-RD.
Methods
A retrospective study of available electronic medical records of patients presented with LG swelling. Patients were selected from Oculoplastic outpatient clinics at Al-Azhar University Hospitals (Sayed Galal University Hospital and El Hussain University Hospital), Cairo, Egypt between June 2016, and February 2022.
Medical records were revised for personal, clinical, laboratory, and imaging data. Personal and clinical data included age, sex, systemic conditions, the onset of manifestations, and complete examination data, mainly visual acuity, proptosis, lid, conjunctiva, pupillary reactions, ocular motility, and fundus examination. Laboratory data included CBC, serum IgG, serum IgG4, Thyroid function tests (free T3, free T4, TSH, Antithyroglobulin antibodies, antithyroid peroxidase antibodies), Serum calcium, and Serum ACE assay (for Sarcoidosis). Patients with salivary gland swellings had Anti-SS-A/Anti-SS-B antibodies (for Sjogren’s Syndrome). All cases had Photographs, orbital imaging (Computed Tomography (CT) and/or Magnetic Resonance Imaging (MRI)), and some cases had also Hess screen. Medication regimens and follow-up results were also reported.
This study considered The Japanese Ministry of Health, Labour, and Welfare’s 2011 guidelines for defining definitive, possible, probable, or unlikely IgG4-RD.3
Inclusion Criteria
Egyptian patients presented with dacryoadenitis, serum IgG4 ≥135mg/dl, and definite IgG4-RD histopathologic features. Patients with organ‑specific criteria for Mikulicz disease (Symmetrical swelling of the lacrimal, parotid, or submandibular gland (SMG), involving at least two pairs of glands and persisting for >3 months) were also included.
Exclusion Criteria
Abnormal thyroid profile, positive Anti-SS-A/Anti-SS-B antibodies, patients with possible, probable, or unlikely IgG4-RD. Due to ethnic and racial differences, non-Egyptian patients were also excluded.
Results
Available medical records included 36 patients with LG swelling. Three non-Egyptian patients (two Ethiopian and one Malaysian) were excluded. Based on clinical, serological, and histological data, patients were classified into four categories:
Unlikely IgG4-RD
Ten cases presented LG swellings with normal serum IgG4 (<135 mg/dl) and no associated sialadenitis. Histopathologic examination revealed sarcoidosis (3 cases), reactive lymphoid hyperplasia (6 cases), and marginal zone lymphoma (1 case). None of the cases met the serological nor the histopathological criteria for IgG4-RD. Rheumatologists referred two cases with Sjogren’s syndrome diagnosis. Both presented with dacryoadenitis, sialadenitis, dry eye, and dry mouth. Laboratory profile showed high serum IgG, normal Serum IgG4, and positive Anti-SS-A/Anti-SS-B antibodies.
Possible IgG4-RD (Positive Serology with No/Negative Histopathology)
Three cases (two females and one male) met the criteria of possible IgG4-RD, they have insidious bilateral dacryoadenitis with increased serum IgG4 >135 mg/dl, but no biopsy was obtained. Cases had no history or signs of salivary glands swelling.
Probable IgG4-RD (Negative Serology with Positive Histopathology)
Two cases (2 females) met the criteria probable IgG4-RD; one case had left suspicious LG swelling, and the other had persistent bilateral dacryoadenitis. Serum IgG4 levels were <135 mg/dl. Histopathology revealed abundant infiltration with IgG4 positive plasma cells. Cases had no history or signs of salivary gland swelling.
Definite IgG4-RD
Seven cases (six females and one male) met the criteria of Mikulicz disease with swelling of both lacrimal and salivary glands either simultaneously or sequentially. Submandibular salivary glands were involved in 4 cases, while Parotid glands were involved in 5 cases (Table 1). Two cases presented initially with salivary gland swelling only and had SMG histopathology that was positive for IgG4-RD with characteristic fibrosis and abundant infiltration with IgG4 positive plasma cells, both cases developed dacryoadenitis several months later. Lid edema was observed in 3 cases.
 |
Table 1 Demographic, Clinical, Serological, and Histopathologic Findings |
Another nine cases (eight females and one male) met the clinical, serological, and histopathological criteria of IgG4-RD with no history or signs of salivary gland swelling (Table 1). Four cases had lid edema, conjunctival hyperemia, and chemosis. Two cases were associated with diffuse EOMs enlargement with diplopia and pain in ocular motility. Although both cases were euthyroid, one had thyroidectomy a few years ago, and the other presented with goiter at the time of presentation. One case had systemic hypertension with a history of cholecystectomy for calcular cholecystitis three years before presentation. Other systemic associations included a case of type II diabetes mellitus and a case of rheumatoid arthritis (Table 1). Histopathology showed that the number of IgG4+ plasma cells/HPF was 40–100 (mean 74±20.1) with an IgG4+/IgG+ cell ratio of 40–70% (mean 55±9.2) (Tables 1 and 2). Storiform fibrosis was evident in all specimens, with a diffuse distribution in 7 cases and focal distribution in 2 cases. None of the specimens showed phlebitis.
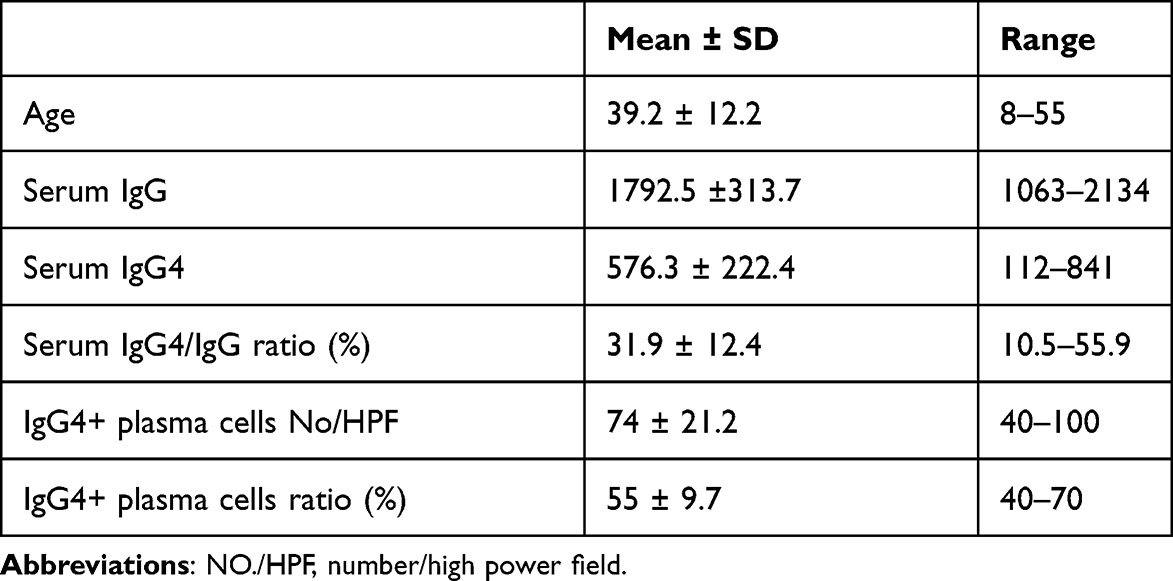 |
Table 2 Statistics of Numerical Data |
Patients with possible, probable, or unlikely IgG4-RD were excluded. A total of sixteen cases that met the criteria of definitive IgG4-RD were reported (Table 1), fourteen females and two males, mean age of 39.2±12.2 (range 8–55) years. Two cases presented with acute onset of manifestations, while fourteen cases presented with an insidious onset. Mean reported serum IgG was 1792.5 ± 313.7 (range 1063–2134) mg/dl, while mean serum IgG4 was 576.25±215.3 (range 112–841) mg/dl (Table 2).
Statistically, serological, and histopathologic findings showed no correlation to age (Table 3). Although the disease showed more predilection in females than in males (87.5% and 12.5%, respectively), both serum IgG4 and serum IgG4/IgG Ratio showed no gender differences (Table 4). On correlating serological and histopathological findings, Serum IgG4 level showed a positive correlation to tissue IgG4+plasma cell percentage and no correlation to the number of IgG4+plasma/HPF (Table 5). In contrast, the serum ratio showed a positive correlation to both percentage and number of IgG4+plasma cells (Table 6).
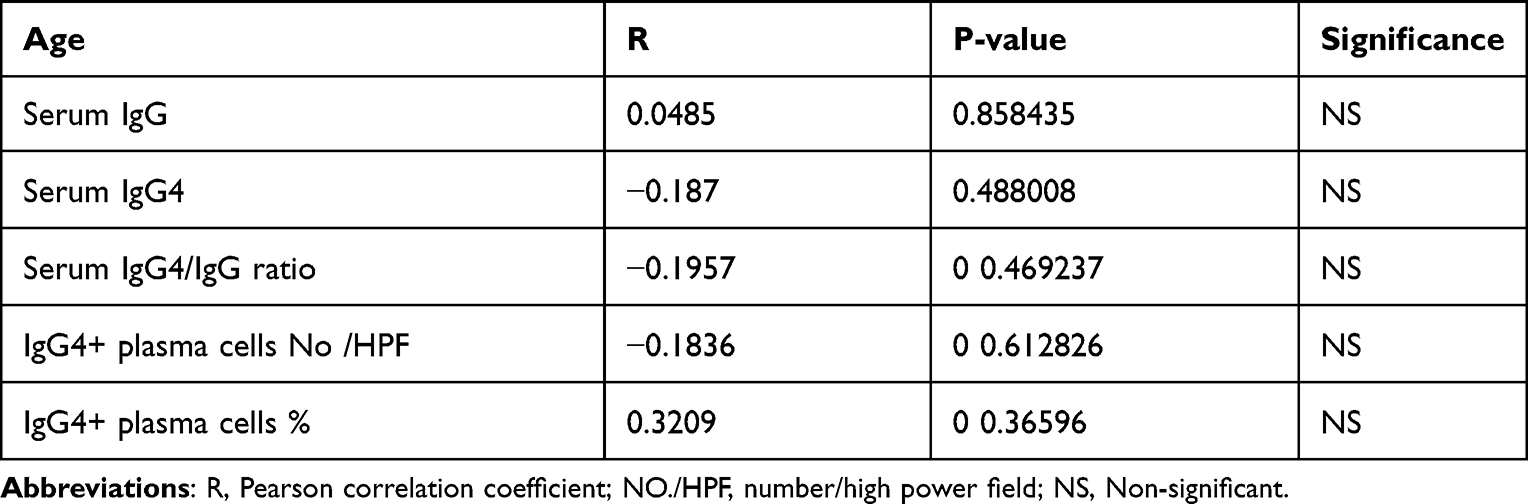 |
Table 3 Correlation Between Age and Serological and Histopathologic Findings |
 |
Table 4 Correlation Between Gender and Serological Findings |
 |
Table 5 Correlation Between Serum IgG4 and Histopathologic Features |
 |
Table 6 Correlation Between Serum IgG4/IgG Ratio and Histopathologic Features |
Orbital CT scans of studied cases showed diffuse enlargement involving the palpebral and orbital lobes with heterogeneous appearance and contrast enhancement. Inferomedial globe displacement and minimal globe indentation were detected in some cases, but bone erosions were not. MRI T1-weighted images showed slightly hyperintense signals to EOMs, and T2-weighted images showed variable signal intensity being isointense to slightly hyperintense signals to EOMs. Images showed well-defined, mostly heterogenous, enlarged glands with moderate enhancement.
Treatment
Eleven cases (68.75%) had a good initial response to oral steroids, starting with 1mg/kg/day, with a maximum dose of 60 mg/day, followed by gradual tapering, then a maintenance dose of 5mg/day for several weeks. Two cases with acute manifestations had pulse intravenous steroid therapy with methylprednisolone 500mg/day for five days, followed by an oral regimen. Three cases failed to respond to steroid treatment and were prescribed other immunosuppressive drugs, including azathioprine and methotrexate.
Follow-up period extended from 7 to 52 months (mean 34.31 ± 15.02 months). Nine cases (56.25%) developed recurrence within 4–23 months (mean 13.67±6.32 months) after cessation of treatment. Recurrent cases had the same regimen as primary cases but were assigned for more extended maintenance periods up to 1 year. Seven cases had oral steroids, while 2 cases had immunosuppressives as they were initially steroid-resistant. None of the recurrent cases required intravenous steroids. Recurrent cases were followed up for 2–44 months (mean 20.66 ± 13.1 months) with no further recurrences.
Discussion
The earliest reports of IgG4-RD disease came from east Asia;2,6 awareness of the disease has improved later with reports from other parts of the world. To our knowledge, only a few reports from the middle east/north Africa have documented systemic features of IgG4-RD,7–9 but no published reports have documented ophthalmic manifestations of IgG4-RD.
Since 2014, we have started investigating patients with orbital manifestations for serological, histopathological, and systemic features of IgG4-RD. In this report, we documented cases with dacryoadenitis that have proven to be part of IgG4-RD in Egyptian patients.
The Japanese study group, 2013 reported that there were no patients younger than 20 years in the IgG4-related orbital inflammation group.10 However, many authors have reported IgG4-ROD11–13 and IgG4-related dacryoadenitis14 in children. The patients’ ages in the study ranged from 8 to 55 years. The youngest in our study was a female child, eight years old, who presented with bilateral dacryoadenitis and increased serum IgG4; the patient had a history of persistent submandibular sialadenitis 15 months before ophthalmic manifestations where SMG biopsy was positive for definite IgG4-RD. Another case was 19 years old, whereas all other cases were older than 30 years (Table 1).
Gender distribution in this study was noticeable with a female to male ratio of 7:1. Zen and Nakanuma mentioned that the proportion of women was higher in patients with head and neck IgG4-RD.15 While, in their meta-analysis and in contrary to our findings, Andrew et al reported the female to male ratio in IgG4-ROD was almost equal, at 1:1.3.16 This discrepancy in gender distribution may be explained by the relatively small sample size in our study, ethnic differences, or because we considered only cases with dacryoadenitis rather than other manifestations of IgG4-ROD.
Dacryoadenitis was reported as the most common manifestation of IgG4-ROD.5,17–20 The cutoff diagnostic tissue criteria are controversial. Early reports considered the presence of 10 IgG4+ plasma cells/HPF was sufficient for diagnosis.21 While Deshpande et al stated that IgG4+ plasma cells should be >100/HPF for an LG specimen.22 The use of IgG4+/IgG+ plasma cell ratio rather than absolute IgG+ plasma cells/HPF was suggested by Cheuk et al.23 Andrew et al reported that the ratio of IgG4+/IgG+ plasma cells of >40% was standard for all cases with IgG4-ROD, while the absolute number of IgG4+ plasma cells/HPF was variable.24 But a ratio of >40% may also occur in rheumatoid arthritis and other rare conditions,1 so authors confirm the importance of correlating clinical, serological, and histopathologic data for proper diagnosis.4,5
In our study, the number of IgG4+ plasma cells ranged from 40 to >100/HPF, and the ratio of IgG4+/IgG+ plasma cells ranged from 40% to 70%. We also reported variable eosinophilic infiltration and excessive fibrosis with a storiform pattern in all specimens, but obliterative phlebitis was not detected. McNab and McKelvie reported IgG+ plasma cells >100/HPF in 93% of LG biopsies without obliterative phlebitis.1
Similarly, a serum IgG4 level of >135mg/dl is generally accepted as one of the three primary diagnostic criteria of IgG-RD. Other serological clues were also suggested for the diagnosis of IgG4-RD. The normal IgG4/IgG ratio is about 5–6%; an elevated IgG4/IgG ratio <8% may be considered in the diagnosis in some cases when the serum IgG4 concentration is less than the diagnostic level of 135 mg/dL, a common finding in patients with single-organ involvement.25,26
In our study, only one case had a serum IgG4 of 112 mg/dl, less than the serological diagnostic level, but diagnosis based on clinical criteria of Mikulicz disease. This case had serum IgG4/IgG ratio of 10.5%, and the overall serum IgG4/IgG ratio was 31.98 ± 11.96% (range 10.5–55.9%). Also, serum IgG4/IgG ratio showed a positive correlation to both percentage and number of IgG4+plasma cells (Table 6), while serum IgG4 level showed positive correlation only to tissue IgG4+plasma cell percentage but not to the number of IgG4+plasma/HPF (Table 5). The serum IgG4/IgG ratio may be of greater diagnostic value than the serum IgG4 level.
We reported 2 cases with associated diffuse myositis, diplopia, and disturbed ocular motility. Interestingly, one case had thyroidectomy a few years ago, where the gland was removed due to compression effects with no frank history of hyperthyroidism. The other case had goiter with normal thyroid function tests at time of presentation. Specific forms of Riedel and Hashimoto thyroiditis are on the spectrum of IgG4-RD. IgG4-related thyroiditis may be associated with massive thyroid enlargement due to diffuse lymphocytic infiltration; thyroidectomy may be indicated in these patients.27,28 Associated thyroid disorder in reported cases may be IgG4-related disorder as both cases were euthyroid and EOMs enlargement pattern was not typical for thyroid eye disease.
One of our cases had cholecystectomy due to calcular cholecystitis. She had normal liver functions and normal abdominal ultrasound with no history of jaundice. IgG4-related cholangitis was unlikely. Another case had rheumatoid arthritis; she had an IgG4+/IgG+ plasma cell ratio of 50% and fulfilled the clinical serological and histopathological features of IgG4-RD.
Lacrimal glands’ radiological findings in the cases of IgG4-related dacryoadenitis were indistinct from radiologic features of dacryoadenitis due to other causes such as an idiopathic orbital inflammatory disease. Orbital radiographs were valuable for detecting other IgG4-ROD features such as enlarged EOMs, enlarged orbital nerves, and orbital soft tissue masses. None of the reported cases had enlarged orbital nerves or orbital masses.
Corticosteroids have been the mainstay of treatment. Conventional oral steroid regimens and pulse steroid therapies were both used. The response is often excellent, but relapses are common.29,30 Immunosuppressant agents, including azathioprine, methotrexate, and mycophenolate, have been involved in managing IgG4-RD as steroid-sparing or in cases of relapses.5,31 Data has shown that Rituximab, an anti-CD20 monoclonal antibody, can be used successfully to treat IgG4-RD.32–34 Radiotherapy in low doses has been reported in the treatment of IgG4-ROD in a small number of cases.35
We got a 68.75% primary success rate with oral steroids, cases with a suboptimal response, and those with relapses had immunosuppressive drugs (azathioprine, methotrexate), with favorable results. Medications, doses, and duration of treatment were prescribed in collaboration with rheumatologists. We have used pulse steroid therapy in 2 cases with an acute presentation. None of our cases had received radiotherapy. The reported recurrence rate in our study was 56.25% within 4–23 months. Other recurrent cases may evolve on longer follow-up.
Conclusion
A significant proportion of cases with lacrimal gland swelling may be part of IgG4-RD. Laboratory work, histopathology, and systemic workup are essential for proper management. The disease had a higher predilection in females. The serum IgG4/IgG ratio may be of greater diagnostic value than the serum IgG4 level. Cases require long-term follow-up due to the high recurrence rate.
Ethical Considerations
The study adhered to Al-Azhar Medical Research Ethical Committee’s instructions and the Helsinki Declaration. Before starting the study, the study was discussed with patients (or their guardians), and written consent for study participation and data sharing was obtained from all patients (or their guardians).
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests concerning the work described.
References
1. McNab AA, McKelvie P. IgG4-related ophthalmic disease. Part I: background and pathology. Ophthalmic Plast Reconstr Surg. 2015;31(2):83–88. doi:10.1097/IOP.0000000000000363
2. Yamamoto M, Ohara M, Suzuki C, et al. Elevated IgG4 concentrations in serum of patients with Mikulicz’s disease. Scand J Rheumatol. 2004;33(6):432–433. doi:10.1080/03009740410006439
3. Mahajan V, Mattoo H, Deshpande V, Pillai S, Stone J. IgG4-related disease. Annu Rev Pathol Mech Dis. 2014;9:315–347. doi:10.1146/annurev-pathol-012513-104708
4. Umehara H, Okazaki K, Masaki Y, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Modern Rheumatol. 2012;22(1):21–30. doi:10.3109/s10165-011-0571-z
5. McNab AA, McKelvie P. IgG4-related ophthalmic disease. Part II: clinical aspects. Ophthal Plast Reconstr Surg. 2015;31(3):167–178. doi:10.1097/IOP.0000000000000364
6. Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732–738. doi:10.1056/NEJM200103083441005
7. Allen SG, Soliman AS, Toy K, et al. chronic mastitis in Egypt and Morocco: differentiating between idiopathic granulomatous Mastitis and IgG4-related disease. Breast J. 2016;22(5):501–509. doi:10.1111/tbj.12628
8. Regev K, Nussbaum T, Cagnano E, Giladi N, Karni A. Central nervous system manifestation of IgG4-related disease. JAMA Neurol. 2014;71(6):767–770. doi:10.1001/jamaneurol.2014.40
9. El Hadary HF, Dadour NM, Ahmed H, Mo’nes D. IgG4-related disease misdiagnosed as cholangiocarcinoma. On J Neur Br Disord. 2018;1(2). doi:10.32474/OJNBD.2018.01.000107
10. Japanese study group of IgG4-related ophthalmic disease. A prevalence study of IgG4-related ophthalmic disease in Japan. Jpn J Ophthalmol. 2013;57(6):573–579. doi:10.1007/s10384-013-0266-4
11. Griepentrog GJ, Vickers RW, Karesh JW, et al. A clinicopathological case study of two patients with pediatric orbital IgG4-related disease. Orbit. 2013;32:389–391. doi:10.3109/01676830.2013.822899
12. Kalapesi FB, Garrott HM, Moldovan C, et al. IgG4 orbital inflammation in a 5-year-old child presenting as an orbital mass. Orbit. 2013;32(2):137–140. doi:10.3109/01676830.2013.764449
13. Sane M, Chelnis J, Kozielski R, Fasiuddin A. Immunoglobulin G4- sclerosing disease with orbital involvement in a 12-year-old girl. J AAPOS. 2013;17:548–550. doi:10.1016/j.jaapos.2013.05.017
14. Notz G, Intili A, Bilyk JR. IgG4-related dacryoadenitis in a 13-year old girl. Ophthal Plast Reconstr Surg. 2014;30:e161–e163. doi:10.1097/IOP.0000000000000016
15. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010;34:1812–1819. doi:10.1097/PAS.0b013e3181f7266b
16. Andrew N, Kearney D, Selva D. IgG4-related orbital disease: a meta-analysis and review. Acta Ophthalmol. 2013;91(8):694–700. doi:10.1111/j.1755-3768.2012.02526.x
17. Takahira M, Ozawa Y, Kawano M, et al. Clinical aspects of IgG4-related orbital inflammation in a case series of ocular adnexal lymphoproliferative disorders. Int J Rheumatol. 2012;2012:635473. doi:10.1155/2012/635473
18. Kubota T, Moritani S. Orbital IgG4-related disease: clinical features and diagnosis. ISRN Rheumatol. 2012;2012:412896. doi:10.5402/2012/412896
19. Sogabe Y, Ohshima K, Azumi A, et al. Location and frequency of lesions in patients with IgG4-related ophthalmic diseases. Graefes Arch Clin Exp Ophthalmol. 2014;252:531–538. doi:10.1007/s00417-013-2548-4
20. Wallace ZS, Deshpande V, Stone JH. Ophthalmic manifestations of IgG4-related disease: single-center experience and literature review. Semin Arthritis Rheum. 2014;43:806–817. doi:10.1016/j.semarthrit.2013.11.008
21. Plaza JA, Garrity JA, Dogan A, et al. Orbital inflammation with IgG4-positive plasma cells: manifestation of IgG4 systemic disease. Arch Ophthalmol. 2011;129:421–428. doi:10.1001/archophthalmol.2011.16
22. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192. doi:10.1038/modpathol.2012.72
23. Cheuk W, Yuen HK, Chan JK. Chronic sclerosing dacryoadenitis: part of the spectrum of IgG4-related Sclerosing disease? Am J Surg Pathol. 2007;31:643–645. doi:10.1097/01.pas.0000213445.08902.11
24. Andrew N, Kearney D, Selva D. Applying the consensus statement on the pathology of IgG4-related disease to lacrimal gland lesions. Mod Pathol. 2013;26:1150–1151. doi:10.1038/modpathol.2013.46
25. Umehara H, Okazaki K, Masaki Y, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012;22:1–14. doi:10.3109/s10165-011-0508-6
26. Masaki Y, Kurose N, Yamamoto M, et al. Cutoff values of serum IgG4 and Histopathological IgG4+ plasma cells for diagnosis of patients with IgG4-related disease. Int J Rheumatol. 2012;2012:1–5. doi:10.1155/2012/580814
27. Dahlgren M, Khosroshahi A, Nielsen GP, Deshpande V, Stone JH. Riedel’s thyroiditis and multifocal fibrosclerosis are part of the IgG4 related systemic disease spectrum. Arthritis Care Res. 2010;62:1312–1318. doi:10.1002/acr.20215
28. Watanabe T, Maruyama M, Ito T, et al. Clinical features of a new disease concept, IgG4 related thyroiditis. Scand J Rheumatol. 2013;42:325–330. doi:10.3109/03009742.2012.761281
29. Ghazale A, Chari ST, Zhang L, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology. 2008;134:706–715. doi:10.1053/j.gastro.2007.12.009
30. Tomiyama T, Uchida K, Matsushita M, et al. Comparison of steroid pulse therapy and conventional oral steroid therapy as initial treatment for autoimmune pancreatitis. J Gastroenterol. 2011;46:696–704. doi:10.1007/s00535-010-0361-y
31. Matsushita M, Ikeura T, Fukui T, Uchida K, Okazaki K. Refractory autoimmune pancreatitis: azathioprine or steroid pulse therapy? Am J Gastroenterol. 2008;103:1834.
32. Khosroshahi A, Carruthers MN, Deshpande V, et al. Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medicine. 2012;91(1):57–66. doi:10.1097/MD.0b013e3182431ef6
33. Lindfield D. Rituximab in IgG4-related inflammatory disease of the orbit and ocular adnexae. Eye. 2012;26:1386. doi:10.1038/eye.2012.147
34. Carruthers MN, Topazian MD, Khosroshahi A, et al. Rituximab for IgG4-related disease: a prospective, open-label trial. Ann Rheum Dis. 2015;74(6):1171–1177. PMID: 25667206. doi:10.1136/annrheumdis-2014-206605
35. Lin YH, Yen SH, Tsai CC, Kao SC, Lee FL. Adjunctive orbital radiotherapy for ocular adnexal IgG4-related disease: preliminary experience in patients refractory or intolerant to corticosteroid therapy. Ocul Immunol Inflamm. 2014;10:1–6.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.