")
Back to Journals » Vascular Health and Risk Management » Volume 18
How Much Debulking with Atherectomy is Enough When Treating Infrainguinal Arterial Interventions? The Balance Between Residual Stenosis and Adventitial Injury
Authors Shammas NW
Received 13 December 2021
Accepted for publication 26 March 2022
Published 5 April 2022 Volume 2022:18 Pages 211—218
DOI https://doi.org/10.2147/VHRM.S353775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mirna N Chahine
Nicolas W Shammas
The Midwest Cardiovascular Research Foundation, Davenport, IA, USA
Correspondence: Nicolas W Shammas, Research Director, Midwest Cardiovascular Research Foundation, 630 E 4th Street, Suite A, Davenport, IA, 52801, USA, Email [email protected]
Abstract: Atherectomy is an effective vessel prepping device but not all atherectomy devices are equal. The depth of vessel injury and residual narrowing vary considerably among atherectomy devices with significant implications on outcome. Precision imaging is critical to optimize outcome using atherectomy as a vessel prepping technique. Prospective trials need to test the hypothesis that precision imaging has a significant impact on how operators approach the treatment of infrainguinal arterial disease.
Keywords: atherectomy, aggressive debulking, vessel prepping, dissections, residual narrowing, complications, adventitial injury
Introduction
There is considerable debate about the optimal strategy in treating infrainguinal arterial disease. Drug coated balloons (DCB) and stents (bare metal (BMS) or drug-eluting stents (DES)) continue to be an important treatment of infrainguinal arterial disease supported by guidelines and driven by superior long-term patency and reduced target lesion revascularization (TLR) when compared to angioplasty.1 However, stents have their own limitations including stent fracture, restenosis and thrombosis. Also stents may become a problem for future surgical options if placed in non-stent zones such as the common femoral artery or popliteal artery. The combination of a vessel prepping device to minimize stenting in addition to DCB is thought to be a preferred alternative strategy to stenting in the infrainguinal arteries while maintaining an excellent long-term outcome. Multiple observational and small randomized trials2–4 support this alternative strategy to primary stenting but large multicenter randomized trials comparing it with stenting are lacking.
The use of paclitaxel-eluting technologies, however, dropped significantly after a recent warning from the Food and Drug Administration suggesting an increase in mortality with these devices.5 Although some recently published studies do not support the notion of mortality increase with paclitaxel,6,7 the utilization of these devices remains low particularly DCB and mostly in office-based settings. The lack of reimbursement for DCB and their overall cost also contributed to the reduction in DCB use.
Vessel prepping alone particularly in the femoropopliteal area, has not been shown to reduce TLR or improve patency when compared to PTA and bailout stenting.8,9 However acute procedural success yielding low residual narrowing and less bailout stenting is markedly improved with vessel prepping supported by several small randomized studies and observational registries.4,8–10 Angiography has been the cornerstone of decision-making for procedural steps and evaluating atherectomy results. Angiography, however, has serious limitations in detecting dissections, evaluating residual narrowing, defining plaque morphology and assessing vessel size. Recent data on precision imaging use, particularly with intravascular ultrasound (IVUS), suggested better outcomes in treating infrainguinal arterial disease.11,12 The use of IVUS may be a key procedural step to optimize outcomes of vessel prepping by defining more accurately plaque morphology and therefore the choice of the appropriate debulking device; define the presence of dissections and those that would need repair; accurately size the vessel which is critical in the choice of an appropriate DCB balloon diameter to gain maximum luminal area and achieving optimal drug transfer into the vessel wall; and finally to assess the residual narrowing following treatment. The long-term outcomes of debulking may have been compromised by the use of suboptimal angiographic imaging and therefore it is important that we reexamine this concept of debulking in light of precision imaging. Below, I will be discussing recent data that illustrate the importance of this dynamic interaction between precision imaging and vessel prepping.
Vessel Prepping with Debulking
We define vessel prepping as a plaque modification step using a device or a technique prior to final definitive treatment that allows maximal gain in minimal luminal area (MLA) with the least disruption to the deeper layers of the vessel wall. In the setting of applying drug-elution technologies, vessel prepping may also increase the likelihood of drug delivery into the vessel wall13 and therefore improve long-term outcomes. By reducing vessel disruption such as deeper or flow-limiting dissections, bailout stenting is reduced. Another, often not discussed concept, is the avoidance of deeper dissections with vessel prepping that is a high predictor for restenosis and loss of patency.14 Therefore, vessel prepping is not only about reducing metal burden and leaving the least behind, but also about choosing the appropriate device that would avoid deep adventitial injury to the vessel wall, only possible with precision imaging guidance such as IVUS or optical coherence tomography (OCT).15 Avoiding deep injury may be a critical step to reduce restenosis even without the use of drug-elution technology. The random “carpet bombing” debulking approach to a vessel wall guided by suboptimal imaging such as angiography needs to be challenged and replaced by “strategic bombing” guided by precision imaging. The latter strategy aims at preserving the adventitia, reducing plaque burden, improving final minimal luminal area, reducing flow-limiting flaps and therefore bailout stenting, and providing accurate vessel sizing.
There are several vessel prepping devices that exist on the market today (Table 1). These can be classified into the following plaque modifying techniques: a. Debulking devices which involve plaque excision whether with cutting, lasing or sanding; b. Plaque remodeling devices that induce changes within the plaque itself making it more likely to respond to treatment without the consequences of flow-limiting dissections. An example of this would be the shockwave balloon; c. Plaque scoring or focal force devices such as the longitudinal microincision catheter FLEX VP (VentureMed), cutting balloon (Boston Scientific), the Serranator balloon, Ultrascore focal force balloon (Bard), or the Angiosculpt balloon (Phillips). Another approach to plaque modification is the Chocolate balloon (Medtronic) encapsulated in a nitinol cage with the purpose of preventing dog-boning of the edges of the balloon, limiting dissections to small areas (“pillows”), and providing gaps (“grooves”) that limit the spread of dissections.
 |
Table 1 Vessel Prepping Mechanisms and Devices |
These technologies lead to different degrees of residual narrowing and dissections (superficial to deep) which are also mitigated by the use of drug-eluting technology (DCB or DES) and/or vessel repair (stenting or endovascular Tack); all create a wide variety of scenarios worth exploring. I will be focusing on the outcome of certain debulking devices in light of what we know about their vessel prepping characteristics defined by precision imaging.
There are differences among these devices and their abilities to remove plaque and how they interact with the deeper layers of the vessel. In order to capture this impact, the iDissection classification was created in 2018.16 Using IVUS, the depth (intima (A), media (B) and adventitia (C)) and extent of dissection (< 180 degrees (1) versus ≥180 degrees (2)) can be captured and accurately classified. Although the length of dissection is not included, this can be determined by using an automated pullback of the IVUS catheter. A total of 6 grades of dissections can now be described based on IVUS: A1, A2, B1, B2, C1, C2. OCT is also another precision imaging modality that can be utilized to characterize dissections but its main limitation is the penetration depth limited to approximately 1–3 mm and therefore it is not well suited for larger vessels. In addition, OCT is only available in limited laboratory and with a small number of operators familiar with image interpretation. Finally, OCT does not have the ChromaFlo available on some IVUS catheters (Phillips Volcano) and therefore may be limited in characterizing dissection extent.
There are several atherectomy devices approved in the United States. They can be classified into: a. Directional (Hawk (Medtronic) and Pantheris (Avinger)), b. Rotational (Rotablator (Boston Scientific), Jetstream (Boston Scientific), Phoenix (Phillips) and Rotarex (Bard)), c. Laser (Excimer 308 nm (Phillips), Auryon 355 nm (Angiodynamics), d. Orbital (Orbital Atherectomy (CSI)). There are large differences between the atherectomy devices in terms of their debulking extent and the occurrence of deeper dissections. Higher residual narrowing and deeper dissections are thought to correlate with reduced patency and higher TLR when adjunctive PTA is used. An aggressive debulking approach can be defined as the reduction in plaque severity by ≥50% or a residual narrowing to less than 50% with atherectomy alone, whereas a soft debulking approach is the reduction of lesion severity by 30–40% or a residual narrowing in the 50–60% range. Accomplishing an aggressive or softer debulking approach is device, operator and vessel size dependent. In the femoropopliteal arteries (vessel diameter 5 to 6 mm), the Jetstream and the Hawk devices can be aggressive debulking devices17,18 while the Auryon laser and orbital atherectomy are generally softer debulking devices.19,20
Adventitial Tears and Residual Narrowing
Atherectomy devices can now be classified using the iDissection classification into four categories based on their interaction with the deeper layer of the vessel wall and residual narrowing.
Low Residual Narrowing with High Rate of Deep Dissections (Figure 1)
An aggressive debulking strategy with the Hawk device or the Jetstream (blade up mode), could lead to a residual narrowing of <50% but at the expense of high rate of media/adventitial tears. The iDissection atherectomy study has shown that the Jetstream device results in 4 to 6 times more dissections on IVUS than seen on an angiogram. Of these dissections, 13% and 30.8% were ≥180° in circumference post atherectomy and adjunctive balloon angioplasty, respectively. Also, 39.1% and 33.3% involved the media and/or adventitia as seen on IVUS post atherectomy and adjunctive balloon angioplasty, respectively.21 Tarricone et al14 have also shown that adventitial injury was identified in 53% of 116 consecutive patients treated with directional atherectomy with an overall 1-year incidence of restenosis of 57%. 97% of patients with adventitial injury had restenosis versus 11% with no injury.
 |
Figure 1 Intravascular ultrasound imaging showing low residual narrowing with deep dissections (yellow arrow). |
The JET registry17 using PTA as an adjunctive treatment after Jetstream atherectomy has shown a TLR rate of 18.3% at 1 year. No drug-coated balloon was used in this study. Restenosis rate was 22.8%. In the JET SCE22 that included a more complex subset of patients, TLR rate was 32% at 1 year with the non DCB arm. In DEFINITIVE LE, mean lesion length was short at 7.4 cm. Restenosis was 22% with directional atherectomy. Finally, in the Hawk versus PTA randomized trial, there was no statistical difference in TLR (16.7% vs 11.1%) or TVR (21.4% vs 11.1%) between the PTA and atherectomy groups, respectively.8 We conclude that with adjunctive PTA, Jetstream atherectomy or SilverHawk atherectomy has a higher rate of adventitial tears and despite aggressive plaque excision, they carry no long-term advantage over PTA alone. On the other hand, combining these devices with drug-coated balloons seem to mitigate the negative impact of deeper dissections on outcome. The JET RANGER4 study, recently presented 1-year data, showed excellent angiographic results with no bailout stenting and with no TLR at 1 year in 31 patients that received Jetstream atherectomy with the In.PACT balloon or the RANGER balloon. The DCB arm alone, had also a low TLR rate at 6% but at the expense of 50% stenting rate in a complex set of lesions including long lesions, total occlusions or moderate to severe calcium. Similarly, in the JET SCE study,22 TLR rate at 1 year was ~5% in the Jetstream + DCB arm. Finally, in Definitive AR,2 technical success was high with the combination therapy of SilverHawk + DCB when compared to DCB alone and with a positive, non-significant trend, toward better patency at 1 year in long and calcified disease. These data indicate that DCB does mitigate some of the negative impact of deeper dissections whether it is post atherectomy or PTA but at a higher stent rate in the PTA arm.23
High Residual Narrowing with High Rate of Deep Dissections (Figure 2)
This is typically a situation seen with PTA where no debulking is performed and a high plaque burden continues to be seen post intervention. PTA also leads to deep dissections particularly in calcified disease, total occlusions and long lesions. To my knowledge, current data on atherectomy devices that fall into this category are not available.
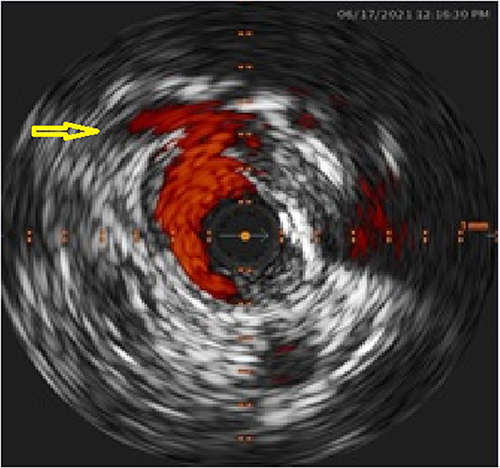 |
Figure 2 Intravascular ultrasound imaging showing high residual narrowing with deep dissections (yellow arrow). |
High Residual Narrowing with Low Rate of Deep Dissections (Figure 3)
This is likely to be a characteristic of the Auryon laser and orbital atherectomy. In 29 patients evaluated prospectively with IVUS and treated with the Auryon laser, there were 9 new dissections post laser (1 adventitial; 3≥180°) and 21 new dissections post laser and PTA (3 adventitial; 1≥180°).24 In the EX-PAD-03 study the average reduction in lesion severity was 33% irrespective of the degree of calcium severity. In the TRUTH study, residual narrowing after OA was 62.9% from a baseline of 84.4% (a delta of 21.9%) with no flow-limiting dissections (D to F) occurring angiographically. In the iDissection below the knee study, there were 7 angiographic dissections after PTA (6 C, 1 D), 1 dissection after OA (1 B), and 2 dissections after OA+PTA (1 A, 1 B; p=0.028 vs post PTA). By IVUS only 3 dissections out of 12 after OA were adventitial.
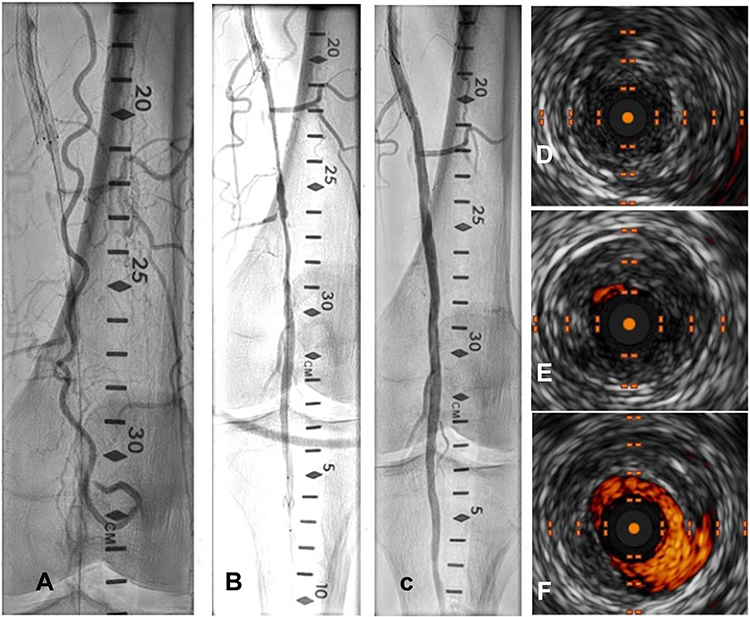 |
Figure 3 Angiographic (A–C) and Intravascular Ultrasound (D–F) showing baseline (A and D), post Auryon laser (B and E) and post final balloon angioplasty (C and F) findings. A high residual narrowing post laser was noted but with excellent angiographic results post final treatment (C) and with no deep dissections on ultrasound (F). |
The compliance trial has shown a marked reduction in bailout stenting with the OA arm versus PTA. Freedom from TLR was significantly reduced at 6 months in the OA arm but was similar at 1 year (81.2% vs 78.3% at 12 months, excluding adjunctive stenting (P>0.99)). In the calcium 360, vessel compliance improves with OA and PTA vs PTA alone with a trend toward lower bailout stenting and TLR at 1 year (statistically not significant). In the EX-PAD-03, the Auryon laser had a TLR rate of 3.3% at 6 months.25 Also at 6 months no TLR was seen in the Auryon SCE study.26 PTA with no DCB as an adjunctive treatment was used in 40% of patients in the EX-PAD-03 and this did not alter the outcome of low TLR rate indicating that preserving the adventitia is likely a more important variable than residual narrowing on the short term. The long-term impact, however, is unclear. One-year data with the Auryon laser is not available at this time and awaiting the results of the Pathfinder registry and the 1-year outcome of the Auryon SCE.
Low Residual Narrowing with Low Rate of Deep Dissections (Figure 4)
This is mostly seen with the Pantheris device or possibly the Auryon laser 2.35 with off centering. Using OCT and directional atherectomy, the Pantheris device is capable of cutting plaque while avoiding the adventitia. In the VISION trial,15 198 lesions were treated with the Pantheris catheter. Mean diameter stenosis was reduced from 78.7% at baseline to 30.3% after Pantheris alone (p<0.001) and to 22.4% after Pantheris ± adjunctive therapy (p<0.001). Histological analysis of atherectomy specimens confirmed <1% adventitia. TLR rate at 6 months was 6.4% despite 52.5% of lesions were treated with the Pantheris alone, 42.4% were treated with Pantheris + PTA, and 5.1% with Pantheris with adjunctive stenting. The VISION trial is of particular importance because it shows how by preserving the adventitia and reduce plaque burden, the overall outcome appears excellent even with no drug-elution applied.
 |
Figure 4 Intravascular ultrasound showing baseline (A), post laser (B) and post angioplasty (C) of a totally occluded superficial femoral artery. Low residual (<50%) and no dissections seen post Auryon laser. |
Dissection Repair
Dissection repair has been performed with stenting or recently with the use of the Tack Endovascular system (Phillips). Vessel prepping reduces the dissected segments that will need repair and therefore the ratio of the stented to treated segment is reduced, leaving the least behind. Although we believe that dissection repair needs to be performed for flow-limiting dissections (D and higher), this concept has been recently challenged with the TOBA series of studies where the Tack Endovascular system was used to repair a good percentage of minor dissections (A and B) with good long-term outcomes with and without DCB.27–29 Should we therefore be repairing all dissections? No randomized trials have tested repair of minor angiographic dissections versus conservative treatment on the overall outcome. Also IVUS has added a new dimension to the question of dissection repair as dissections identified on IVUS are several times more than we have seen on an angiogram. What dissections on IVUS need therefore to be repaired? The Tack Endovascular system leaves the least behind and so repair of minor angiographic dissections with and without the use of DCB continues to fulfill this strategy with good long-term outcome. When IVUS is used in our lab to repair dissections, we rely on 2 main parameters: the extent of the flap seen (over 180 degrees) and if the dissection has reached the adventitia. Adventitial dissections are typically repaired if only PTA is used as an adjunctive treatment. If DCB is used, we believe the need to repair these deeper, non-flow limiting dissections may not provide an additional advantage because DCB can mitigate many of the negative consequences of these dissections. Therefore, in an office-based lab where DCB use is very low, a low threshold for dissection repair becomes important. Also the choice of a device with the least damage to the adventitia becomes critical to reduce restenosis and TLR.
Conclusion
Vessel prepping is important for the acute procedural results and reducing the need for stenting. Also drug transfer into the vessel wall seems to improve with vessel prepping. Atherectomy is an effective vessel prepping device but not all atherectomy devices are equal. Precision imaging has revealed how various atherectomy devices affect the vessel wall and the extent of residual narrowing, two important variables in predicting long-term outcomes. Prospective trials, precision imaging based, need to test these hypotheses which will have a significant impact on how operators approach the treatment of infrainguinal arterial disease.
Disclosure
Dr Shammas receives educational and Research grants from Bard/BD, Angiodynamics, Boston Scientific, VentureMed Group, and Phillips. He is on the speaker Bureau of Janssen, Boehringer Ingelheim, Merck, Amgen, and Kiniksa.
References
1. Klein AJ, Jaff MR, Gray BH, et al. SCAI appropriate use criteria for peripheral arterial interventions: an update. Catheter Cardiovasc Interv. 2017;90(4):E90–E110. doi:10.1002/ccd.27141
2. Zeller T, Langhoff R, Rocha-Singh KJ, et al.; DEFINITIVE AR Investigators. Directional Atherectomy Followed by a Paclitaxel-Coated Balloon to Inhibit Restenosis and Maintain Vessel Patency: twelve-Month Results of the DEFINITIVE AR Study. Circ Cardiovasc Interv. 2017;10(9):e004848. doi:10.1161/CIRCINTERVENTIONS.116.004848.
3. Cioppa A, Stabile E, Popusoi G, et al. Combined treatment of heavy calcified femoro-popliteal lesions using directional atherectomy and a paclitaxel coated balloon: one-year single centre clinical results. Cardiovasc Revasc Med. 2012;13(4):219–223.
4. Shammas NW, Purushottam B, Shammas WJ, et al. TCT-17 Jetstream Atherectomy Followed by Paclitaxel-Coated Balloons Versus Balloon Angioplasty Followed by Paclitaxel-Coated Balloons: twelve-Month Results of the Prospective Randomized JET-RANGER Study. J Am Coll Cardiol. 2021;78(19_Supplement_S):B8.
5. Katsanos K, Spiliopoulos S, Kitrou P, et al. Risk of Death Following Application of Paclitaxel‐Coated Balloons and Stents in the Femoropopliteal Artery of the Leg: a Systematic Review and Meta‐Analysis of Randomized Controlled Trials. J Am Heart Assoc. 2018;7(24):e011245.
6. Schneider PA, Varcoe RL, Secemsky E, Schermerhorn M, Holden A. Update on paclitaxel for femoral-popliteal occlusive disease in the 15 months following a summary level meta-analysis demonstrated increased risk of late mortality and dose response to paclitaxel. J Vasc Surg. 2021;73(1):311–322.
7. Schneider PA, Brodmann M, Mauri L, et al. Paclitaxel exposure: long-term safety and effectiveness of a drug-coated balloon for claudication in pooled randomized trials. Catheter Cardiovasc Interv. 2020;96(5):1087–1099.
8. Shammas NW, Coiner D, Shammas GA, et al. Percutaneous lower-extremity arterial interventions with primary balloon angioplasty versus Silverhawk atherectomy and adjunctive balloon angioplasty: randomized trial. J Vasc Interv Radiol. 2011;22(9):1223–1228.
9. Wu Z, Huang Q, Pu H, et al. Atherectomy Combined with Balloon Angioplasty versus Balloon Angioplasty Alone for de Novo Femoropopliteal Arterial Diseases: a Systematic Review and Meta-analysis of Randomised Controlled Trials. Eur J Vasc Endovasc Surg. 2021;62(1):65–73. doi:10.1016/j.ejvs.2021.02.012
10. Dattilo R, Himmelstein SI, Cuff RF. The COMPLIANCE 360 Trial: a randomized, prospective, multicenter, pilot study comparing acute and long-term results of orbital atherectomy to balloon angioplasty for calcified femoropopliteal disease. J Invasive Cardiol. 2014;26(8):355–360.
11. Iida O, Takahara M, Soga Y, et al. Efficacy of intravascular ultrasound in femoropopliteal stenting for peripheral artery disease with TASC II class A to C lesions. J Endovasc Ther. 2014;21(4):485–492. doi:10.1583/14-4721R.1
12. Sheikh AB, Anantha-Narayanan M, Smolderen KG, et al. Utility of Intravascular Ultrasound in Peripheral Vascular Interventions: systematic Review and Meta-Analysis. Vasc Endovascular Surg. 2020;54(5):413–422. doi:10.1177/1538574420920998
13. Tzafriri AR, Garcia-Polite F, Zani B, et al. Calcified plaque modification alters local drug delivery in the treatment of peripheral atherosclerosis. J Control Release. 2017;264:203–210.
14. Tarricone A, Ali Z, Rajamanickam A, et al. Histopathological Evidence of Adventitial or Medial Injury Is a Strong Predictor of Restenosis During Directional Atherectomy for Peripheral Artery Disease. J Endovasc Ther. 2015;22(5):712–715. doi:10.1177/1526602815597683
15. Schwindt AG, Bennett JG, Crowder WH, et al. Lower Extremity Revascularization Using Optical Coherence Tomography-Guided Directional Atherectomy: final Results of the EValuatIon of the PantheriS OptIcal COherence Tomography ImagiNg Atherectomy System for Use in the Peripheral Vasculature (VISION) Study. J Endovasc Ther. 2017;24(3):355–366.
16. Shammas NW, Torey JT, Shammas WJ. Dissections in Peripheral Vascular Interventions: a Proposed Classification Using Intravascular Ultrasound. J Invasive Cardiol. 2018;30(4):145–146.
17. Gray W, Garcia LA, Amin A, Shammas NW; JET Registry Investigators. Jetstream Atherectomy System treatment of femoropopliteal arteries: results of the post-market JET Registry. Cardiovasc Revasc Med. 2018;19(5Pt A):506–511. doi:10.1016/j.carrev.2017.12.015.
18. McKinsey JF, Zeller T, Rocha-Singh KJ, et al.; DEFINITIVE LE Investigators. Lower extremity revascularization using directional atherectomy: 12-month prospective results of the DEFINITIVE LE study. JACC Cardiovasc Interv. 2014;7(8):923–933. doi:10.1016/j.jcin.2014.05.006.
19. Babaev A, Zavlunova S, Attubato MJ, et al. Orbital Atherectomy Plaque Modification Assessment of the Femoropopliteal Artery Via Intravascular Ultrasound (TRUTH Study). Vasc Endovascular Surg. 2015;49(7):188–194.
20. Shammas NW, Chandra P, Brodmann M, et al.; EX-PAD-03 Investigators. Acute and 30-Day Safety and Effectiveness Evaluation of Eximo Medical’s B-Laser™, a Novel Atherectomy Device, in Subjects Affected With Infrainguinal Peripheral Arterial Disease: results of the EX-PAD-03 Trial. Cardiovasc Revasc Med. 2020; 21(1):86–92. doi:10.1016/j.carrev.2018.11.022
21. Shammas NW, Torey JT, Shammas WJ, et al. Intravascular Ultrasound Assessment and Correlation With Angiographic Findings Demonstrating Femoropopliteal Arterial Dissections Post Atherectomy: results From the iDissection Study. J Invasive Cardiol. 2018;30(7):240–244.
22. Shammas NW, Shammas GA, Jones-Miller S, et al. Long-term outcomes with Jetstream atherectomy with or without drug-coated balloons in treating femoropopliteal arteries: a single center experience (JET-SCE). Cardiovasc Revasc Med. 2018;19(7Pt A):771–777. doi:10.1016/j.carrev.2018.02.003
23. Tepe G, Zeller T, Schnorr B, et al. High-grade, non-flow-limiting dissections do not negatively impact long-term outcome after paclitaxel-coated balloon angioplasty: an additional analysis from the THUNDER study. J Endovasc Ther. 2013;20(6):792–800.
24. Shammas NW, Torey JT, Shammas WJ, et al. Intravascular Ultrasound Assessment and Correlation With Angiographic Findings of Arterial Dissections Following Auryon Laser Atherectomy and Adjunctive Balloon Angioplasty: results of the iDissection Auryon Laser Study. J Endovasc Ther. 2021;1:15266028211028200. doi:10.1177/15266028211028200
25. Rundback J, Chandra P, Brodmann M, et al. Novel laser-based catheter for peripheral atherectomy: 6-month results from the Eximo Medical B-Laser IDE study. Catheter Cardiovasc Interv. 2019;94(7):1010–1017.
26. Shammas NW, Shammas GA, Halupnik G. Auryon™ Laser in Peripheral Arterial Interventions: a Single Center Experience (Auryon-SCE). J Inv Cardiol. 2022;1:456.
27. Gray WA, Cardenas JA, Brodmann M, et al. Treating Post-Angioplasty Dissection in the Femoropopliteal Arteries Using the Tack Endovascular System: 12-Month Results From the TOBA II Study. JACC Cardiovasc Interv. 2019;12(23):2375–2384.
28. Brodmann M, Wissgott C, Brechtel K, et al.; TOBA III Investigators. Optimized drug-coated balloon angioplasty of the superficial femoral and proximal popliteal arteries using the Tack Endovascular System: TOBA III 12-month results. J Vasc Surg. 2020; 72(5):1636–1647.e1. doi:10.1016/j.jvs.2020.01.078
29. Geraghty PJ, Adams G, Schmidt A; TOBA II BTK Investigators. Six-month pivotal results of tack optimized balloon angioplasty using the Tack Endovascular System in below-the-knee arteries. J Vasc Surg. 2021;73(3):918–929.e5. doi:10.1016/j.jvs.2020.08.135
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.