")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
HIV in Three Groups of Young People from Medellín: General Population, Organizations for People with Socioeconomic Vulnerability, and Men Who Have Sex with Other Men
Authors Cardona-Arias JA , Narváez Moreno NN, Higuita-Gutiérrez LF
Received 5 August 2023
Accepted for publication 29 September 2023
Published 1 November 2023 Volume 2023:15 Pages 641—648
DOI https://doi.org/10.2147/HIV.S434036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Jaiberth Antonio Cardona-Arias,1 Nicole Nahomy Narváez Moreno,1 Luis Felipe Higuita-Gutiérrez1,2
1Escuela de Microbiología, Universidad de Antioquia, Medellín, Antioquia, Colombia; 2Facultad de Medicina, Universidad Cooperativa de Colombia, Medellín, Antioquia, Colombia
Correspondence: Luis Felipe Higuita-Gutiérrez, Email [email protected]
Introduction: In Colombia, there are no studies that analyze the effect of socioeconomic vulnerability and belonging to the group of men who have sex with other men (MSM) on the prevalence of HIV in young people.
Objective: To compare the prevalence of HIV in three groups of young people from Medellín-Colombia: general population, socioeconomic vulnerability and MSM.
Methods: This cross-sectional analytical study included 2449 young people from the general population, 1736 from institutions that serve young people in situations of socioeconomic vulnerability, and 2269 MSM. The prevalence of infection in each group was determined, statistical differences were identified using Pearson’s Chi-square and Trend’s Chi-square, and crude and adjusted odds ratios were estimated using logistic regression with 95% confidence intervals. Analyses were performed in SPSS 29.0.
Results: HIV prevalence was 0.8% in the general population group, 1.3% in young people with socioeconomic vulnerability, and 5.6% in MSM. The groups with the highest HIV were as follows: (i) in MSM it was 4.1 compared to the general population, (ii) between 25– 28 years of age it was 2.9 times compared to those under 20 years, (iii) in men it was 10 times that registered in women, (iv) in young people with primary, secondary, technical and university studies it was 7.1; 6.7; 11.0 and 14.5 times that found in those who did not register studies, (v) in affiliates of the subsidized health regime it was 2.2 times and in those without affiliation 2.4 times compared to the infection in affiliates of the contributory health regime.
Conclusion: HIV prevalence was high, and explained by socioeconomic vulnerability, having sex between men, gender, age, education, and health affiliation, demonstrating the intersectionality of determinants of the health system, socioeconomic status, and determinants individuals in the occurrence of HIV in young people in Medellín.
Keywords: HIV, youth, determinants of health, health system, socioeconomic status, men who have sex with men
Introduction
The National Administrative Department of Statistics (DANE in Spanish) from Colombia defines youth as people aged 14–28 years. At this stage, the subjects are in the process of consolidating their intellectual, physical, moral, economic, social, and cultural autonomy.1 Youth involves facing multiple challenges of the transition to adult life and facing the future, concerns for personal development, new problems of daily life, and search for opportunities in different areas.2
The health of young people is an issue of great importance and concern in all societies. Among the health challenges faced by this group, HIV represents a highly relevant problem because of its clinical-epidemiological impacts. HIV can develop as an asymptomatic infection or cause different clinical outcomes, AIDS, and even death when it is not treated. The prevalence during the period 2010–2019 increased by 21% in Latin America, and in recent years (2021) there has been a higher record of new infections in women between 20 and 24 years old and men between 25 and 29 years old.3,4
In Colombia, there are around 135,000 people living with HIV, 44% of whom are young (52,650,135 men and 6750 women).3 New cases have increased 15% with a rate of 33.3/100,000 inhabitants in 2019 and 39.2/100,000 in 2022, mainly in young people, which prevents the country from meeting the goals established by the World Health Organization (WHO) for 2030.5,6 Despite the fact that the Ministry of Health reports a high magnitude of the infection in young people, the epidemiological profile of HIV in this population is not described in detail. Additionally, the research available in Medellín-Colombia generally reports the prevalence of infection in different groups, but very few analyze the intersectionality of being young with other risk conditions such as socioeconomic vulnerability or belonging to key groups.7
Unlike the evidence available in Colombia, studies in other countries have shown the importance of investigating HIV in young MSM or those with socioeconomic vulnerability. A study in five cities in the United States in the period 1994–2011 reported that the prevalence increased in the group of young MSM aged between 23 and 29 years, it was stable in those aged between 18 and 22 years, and some cities such as Baltimore presented a greater increase in cases.8 In 211 young MSM from Indonesia, the prevalence was 30% (almost 100 times higher than the general population and 7 times higher than young MSM from Asia), the main risk factors were being between 20 and 24 years of age and preferring the receptive position during sexual intercourse.9 In China, the change in epidemiological patterns has been reported once the active search for cases in this group has been emphasized, demonstrating that young MSM are highly vulnerable to infection, and they become a new critical point for transmission.10 In young MSM from Kenya, a prevalence of 8.3% was reported; 34% did not use a condom, 21% received money, and 41% consumed alcohol in their last sexual relationship; the main risk factors were studying in private institutions, last sexual partner older than 25 years, meeting the last sexual partner online, and a positive result for Neisseria gonorrhea.11 Other studies with MSM document their sexual risks, and it has been estimated that in some countries, more than 90% of young MSM with HIV became infected through sexual contact, ruling out the importance of other routes of transmission in this group.12 Additionally, several authors have shown the importance of HIV coinfections with Treponema pallidum, HBV, HCV and other STIs, in terms of clinical severity, progression of the clinical states of these STIs, among other epidemiological outcomes.13–16
In Medellín, according to data from the Epidemiological Surveillance System (SIVIGILA) in 2019, 1812 new cases of HIV were registered, 1556 were men, and close to half occurred in the population aged 20–29.17 Some studies in this city have identified factors associated with HIV, such as limited ability to make decisions, limited access to education, family and social problems that are aggravated by unemployment and significant economic difficulties, but without delving into issues specific to the young population.18,19
The objective of this research was to compare the prevalence of HIV and its associated factors (characteristics that have the potential to increase or decrease the frequency of a health outcome, that is, identify subgroups with a greater occurrence of the infection) in three groups of young people from Medellín-Colombia: general population, socioeconomically vulnerable, and MSM. The importance of this study is to generate updated and accurate information on the prevalence of HIV in young people in Medellín, and to identify group-specific risk factors with their intersectionality to propose strategies for prevention, early detection, and adequate care that respond to specific needs.
Methods
Type of Study and Population
A cross-sectional analytical study was carried out with 5771 young people aged between 15–28 years screened for HIV in a health service provider institution (HSIP) in Medellín and grouped into three populations: 2449 young people from the general population that the HSIP captures mainly in educational institutions and companies (does not include individuals who identified themselves as MSM), 1736 from institutions that serve young people in situations of socioeconomic vulnerability (the census of these institutions was obtained from the Medellín Youth Secretariat and the HSIP went to promote screening) and 2269 MSM (the HSIP captures them through contacts with leaders of key groups in the city and in workshops on HIV and other sexually transmitted infections in educational institutions and companies). Because this study analyzed the entire population screened by HSIP, no sample size or sampling calculation was made.
Eligibility Criteria
Young people between the ages of 15 and 28 who voluntarily agreed to screen for HIV in the HSIP during the years 2019–2022 were included (during the confinement by COVID-19 between March 20 and November 30, 2020, no had records) and residents of Medellín for at least the year prior to screening. Young people with HIV diagnosis prior to 2019 were excluded; those who demanded some type of remuneration for participating in the screening program and those who decided to withdraw their assent or informed consent in the pre-test counseling. The physician who performed the pre-test counseling evaluated that the subjects had the physical and mental capacities to full understand the procedures of this research.
Data Collection and Bias Control
The HSIP has an extramural work team in charge of making induced demand for screening for HIV and other infections. For young people, HIV screening is promoted through educational workshops on sexual rights, the main STIs in this group, HIV risk factors, the importance of timely detection, pre- and post-test counseling, the care route for positive cases, and processes that apply the HSIP to guarantee the confidentiality of the information. Those who agree to do the screening fill out the assent or informed consent, attend the pre-test counseling, answer a short survey, take the sample for the screening, and attend the delivery of the result in which a post-test counseling is done and in positive cases the care route was activated. The information of each young person is kept in the records of the HSIP.
HSIP used SD BIOLINE HIV1-/2, a rapid qualitative test that detects IgG, IgM and IgA antibodies against specific recombinant HIV-1 antigens, including HIV-2 subtypes O and gp36, in serum, plasma or whole blood. To confirm the diagnosis, HSIP used Alere Determine TM, an immunochromatography test that qualitatively detects p24 antigen and HIV 1–2 antibodies in a single combo. Subjects who obtained positive results in both tests were considered positive. Both tests have a sensitivity and specificity of 99%.
For this research, the data from the secondary source was taken and information biases were controlled through a double, blind, and independent extraction of the HSIP records by two researchers who designed a database in SPSS. Prior to data analysis, the agreement of the extracted data was confirmed by calculating the kappa coefficient for the study variables.
Analysis of Information
The description of the independent variables was carried out with frequencies, and these variables were compared between the three study groups with Pearson’s Chi-square tests for the nominal variables (sex, marital status and health affiliation regime), Chi-square of Trend for the ordinal variables (age group, educational level) and Kruskal Wallis H for age. The assumption of normality was evaluated using Kolmogorov–Smirnov with Lilliefors correction.
The prevalence of infection was determined with its 95% confidence interval for each group. HIV prevalence was compared between the study groups and with the independent variables, using odds ratios with their 95% confidence intervals, taking the group with the lowest prevalence as the reference group. To rule out confusion problems, multivariate adjustment was performed using logistic regression, and the goodness of fit was determined using the Wald and Hosmer-Lemeshow statistic. To explore the interaction between the independent variables and HIV prevalence, a multivariate logistic regression model was performed using the following formula:

Analyses were performed in SPSS 29.0, with p values <0.05 as significant.
Ethical Aspects
The guidelines of the Declaration of Helsinki and Resolution 8430 of the Colombian Ministry of Health of 1993, which classifies this research as a study without risk, were followed. The HSIP completes the informed assent for young people between the ages of 15–17 and the informed consent for those over 17 years of age, which includes the following data: objective of the screening, risks and benefits of the procedure, route of healthcare, voluntary participation and the authorization of the use of the information for investigative purposes.
In cases where possible, parental consent was obtained (In the majority of the group with socioeconomic vulnerability and some MSM, it was not possible to obtain it). However, according to sentence C-246/17 and T-675-17 about the Self-determination of minors; the Constitutional Court of the Republic of Colombia in 2017 determined that parental consent is not necessary in these cases given that the age of 14 has been established that minors may have the maturity to begin to assume obligations and responsibilities in society, such as marriage (and to consent to sexual relations), and the right to privacy in the family environment; as long as they meet certain conditions such as the evaluation of their evolutionary capacities, and the full understanding of the procedures or situations they face.
The HSIP undertakes to anonymize the files delivered to the researchers. The HSIP endorsed the performance of this study according to act 20,230,220–1 of the ethical scientific committee.
Results
In the study population, 60% were men, 87% were single, 48% completed basic education, and 73% were in the contributory regime; all these variables presented statistical differences between the three study groups (Table 1).
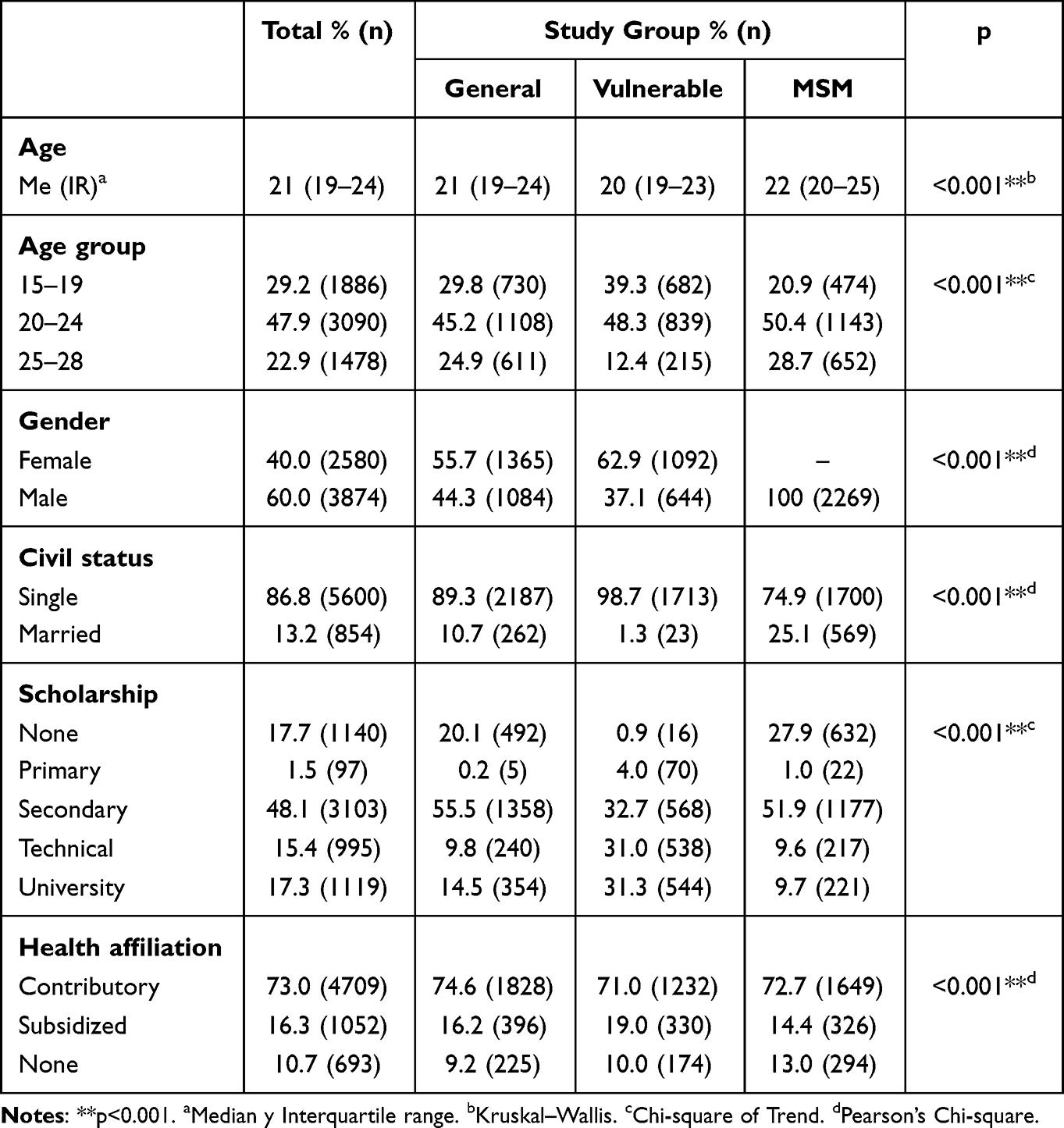 |
Table 1 General Description of the Sociodemographic Characteristics in the Study Population and Specific Characteristics in Each Group Analyzed |
HIV prevalence was 2.6% (n = 168, 95% CI 2.2–3.0). HIV prevalence did not present statistical differences with marital status, with 2.7% (n = 153) in singles and 1.8% (n = 15) among those married (Chi-square p = 0.095).
The prevalence of HIV presented statistically significant differences according to the study group, age group, sex, schooling and health affiliation regime; all these variables had a statistical association independent of the others according to the multivariate adjustment; the subgroups with the highest odds of infection were the following: (i) in MSM it was 4.1 times compared to that registered in young people from the general population, (ii) in young people between the ages of 25–28 it was 2.9 times in comparison with those under 20 years of age, (iii) in men it was 10 times that registered in women, (iv) in young people with primary, secondary, technical and university studies it was 7.1; 6.7; 11.0 and 14.5 times that found in those who did not register studies, (v) in affiliates of the subsidized regime it was 2.2 times and in those without affiliation 2.4 times compared to the infection in affiliates of the regime contributory (Table 2).
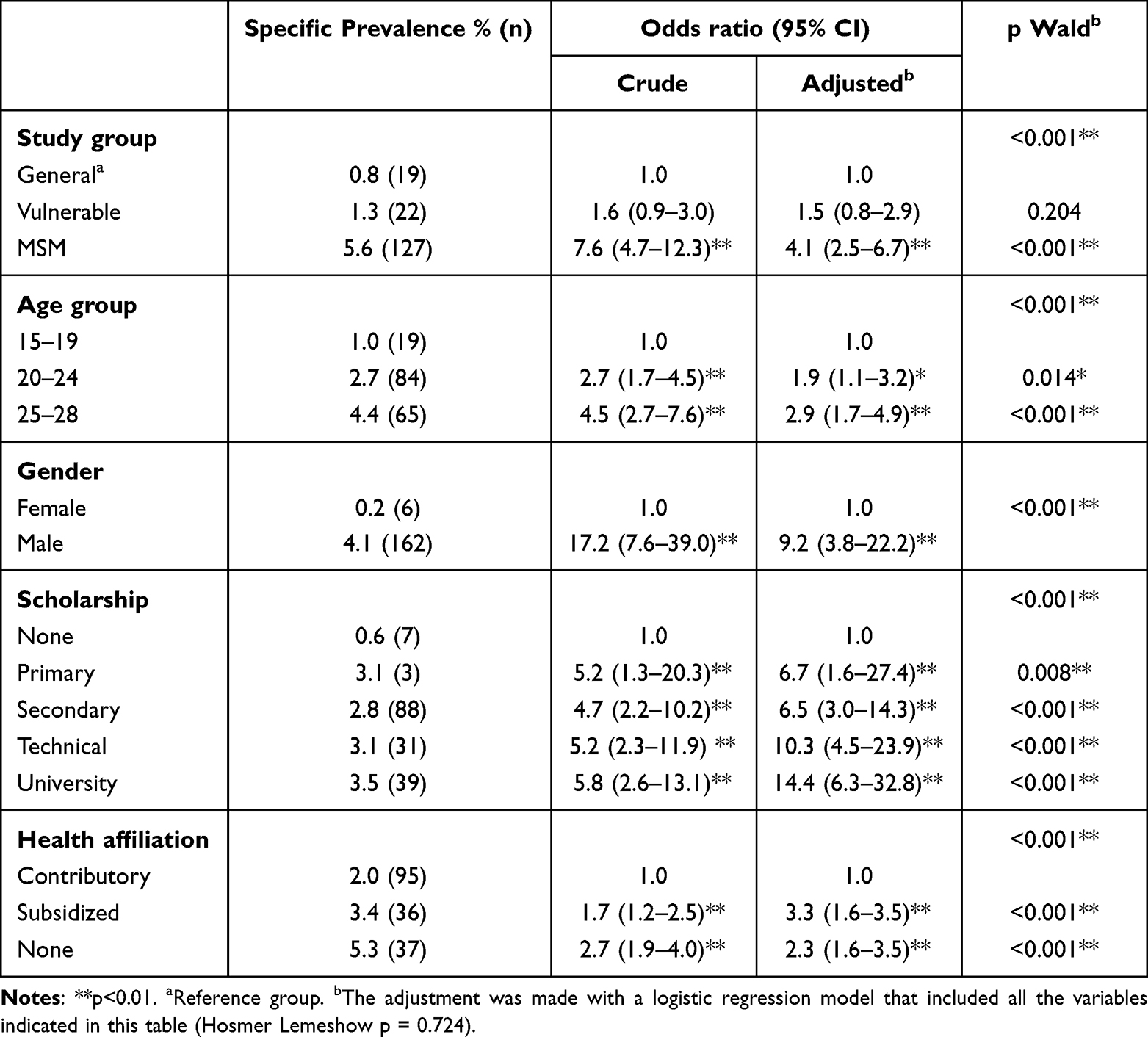 |
Table 2 HIV Prevalence in Each Study Group and Specific Prevalence According to the Sociodemographic Characteristics of the Study Population |
When evaluating the interaction of the independent variables of the study, only the following were found: having an education as a health technician without affiliation in health, the OR increases to 38 (95% CI 3–200), being a university student without health affiliation increases to 20 (95% CI 2–250), and being a man with socioeconomic vulnerability at 4.3 (95% CI 2.5–7.3).
Young people with HIV presented the following characteristics: (i) no coinfection with HCV or HBV was found, (ii) only the MSM group presented coinfection with Treponema pallidum with 7.1% (9/127), (iii) in the registry of opportunistic infections, only two patients in the MSM group presented tuberculosis, (iv) in the positives of the three groups the viral load was less than 40,000 copies/mL, and (v) the CD4+/CD8+ lymphocyte count was 617/mm3 in the general population group, 676/mm3 in the group with socioeconomic vulnerability and 624/mm3 in MSM.
Discussion
This study found an overall youth HIV prevalence of 2.6%. This frequency is higher than that reported by UNAIDS in 2021, which found a global prevalence of HIV in young people of 0.3%.20 It is also higher than the prevalence of HIV in the general population of Colombia, which is estimated at 0.7%.21 The differences between these calculations can be attributed to methodological factors in the representativeness of the samples, the age group considered young, and social, cultural, health system, and infection prevention factors specific to each country. However, UNAIDS acknowledges that progress in reducing infection among young people is uneven between and within countries, with strong reductions in new infections among young people in some African countries, but limited progress in other countries.20 These results allow us to affirm that Medellín is necessary to implement interventions that have demonstrated their excellent impact in other countries, especially considering the growing problem associated with sexual tourism in the city.22–24
The prevalence of HIV in young MSM was 4.1 times higher than that in general group. MSM refers to sexual behavior, regardless of sexual orientation.25 Calculations with data from 62 countries have shown that in the young population, the prevalence of infection in MSM is 6%, while in young people in the general population it is 0.3%, even the figures in MSM are higher than in other key groups such as young people who injecting drugs (5%), young sex workers (4%) and young prisoners (1%).20 MSM may be at increased risk of contracting HIV and other STIs due to their sexual network, biological or behavioral factors including number of sexual partners, sex without a condom, anal sex with its biological risks, and use of drug psychoactive that reduce the perception of risk.25 In this sense, a study with MSM in Medellín revealed that their average age of initiation of sexual relations was 16 years, half of the participants reported having at least 58 different sexual partners in their lives, an average of 14 sexual relations without protection in the last three months, and 65.2% admitted that they have used drugs at some point in their lives.26 This finding adds to the evidence indicating that MSM are a key group for HIV infection control because they are at a higher risk of contracting the virus.
The prevalence of HIV in men was 10 times that in women. This finding contrasts with the UNAIDS report that found that the prevalence in young women was 0.4%, while in young men it was 0.2%,20 but coincides with the figures for the general population in Colombia in 2020 with 81.7% of cases in men.27 In this sense, it is important to remember that HIV is a concentrated epidemic in Colombia because the prevalence is greater than 5% in some subpopulations (particularly men), and less than 1% in the general population.28 This disparity could be explained by the very origin of the epidemic, the inclusion of MSM in this subgroup, greater perception of care, adherence to health programs, and earlier seeking health services in women.29
The prevalence of HIV in young people with primary, secondary, technical, and university studies was 7.1; 6.7; 11.0 and 14.5 times that found in those who did not register studies. This finding is contrary to theories that suggest that health and education are inextricably linked and to empirical data that show the effect of education in reducing infant mortality, vaccination, and increasing life expectancy.30 A possible explanation for this finding is that education by itself may not be sufficient to prevent HIV infection, but depends on the quality of the education received, the specific inclusion of sexual and reproductive health issues, and the type of educator. On this last point, it has been described that peer education, that is, those that occur between people from the same population group, is more effective because peers can more easily influence the behavior of group members, having a higher level of trust that allows for more open discussions on sensitive topics. In addition, peers have better access to hidden populations that may have limited interaction with traditional health programs and have also been described as more cost-effective compared with those delivered by traditional health care providers.31,32 A recent meta-analysis found that peer education promotes HIV testing, condom use and reduces unprotected sex with long-term impact on behavior change among high-risk groups worldwide.33 In this sense, the implementation of educational interventions carried out by peers in the youth of the Medellín’s city is suggested.
The prevalence of HIV in affiliates of the subsidized regime was 2.2 times and in those without affiliation 2.4 times compared with the infection in affiliates of the contributory regime. According to a report from the Colombian National Health Institute, of the total reported HIV cases in 2020, 11.2% correspond to people without affiliation to the health system.27 To understand this finding, it is important to clarify that, in Colombia, a health system has been adopted that can be divided into three large groups: the special regime, the contributory regime, and the subsidized regime. In the special regime, state workers such as teachers or employees of the military are affiliated, in the contributory regime, workers in general and their family nucleus are affiliated, and in the subsidized regime, people without employment or with informal employment are affiliated. It is estimated that the insurance coverage of the health system in the country is 99.1%.34,35 Being affiliated with the health system enables the right to receive health promotion, disease prevention and health recovery actions, from basic care to highly complex treatments.34 The fact that the infection is circulating with high frequencies in groups without affiliation to the health system is worrying because it is precisely these groups that are not reached by health promotion and disease prevention actions, and present barriers to access antiretroviral treatment and greater difficulties for them to adhere to it. Taken together, these situations make it difficult to interrupt the transmission cycle in this population and constitute the nucleus on which all efforts must be focused to meet the global goal for the year 2025, which requires that 95% of all people living with HIV know their serostatus, 95% of all people with diagnosed infection receive continuous antiretroviral therapy, and 95% of all people receiving antiretroviral therapy achieve viral suppression.36
When assessing the interaction among the study’s independent variables, an intersectionality emerges, highlighting various factors that elevate the risk of infection. These factors include the connection between gender and socioeconomic vulnerability and the relationship between education and health affiliation. In this context, several academics advocate a more comprehensive understanding of HIV risks through a socioecological determinants model. This model encompasses structural elements, such as the functioning of the healthcare system, community-related aspects, including social networks, and individual factors, such as psychoactive substance use, poverty, sexual and gender minority status.37 Consequently, it becomes imperative for health authorities to understand the convergence of these factors when formulating intervention strategies. This study has the following limitations: (i) the sample is not representative of all young people in the city of Medellín; however, it includes a sample of 6454 young people, which constitutes one of the largest studies carried out in the country, (ii) the classification of young people differs from that established by UNAIDS. For UNAIDS, to be young is to be between 15 and 24 years, while for DANE, youth includes from 14 to 28 years. This difference can make international comparisons difficult, but it is useful for planning local actions, and (iii) as it is a cross-sectional study, the associations do not imply causal attributions.
Conclusion
A high prevalence of HIV was found, explained by socioeconomic vulnerability, having sex between men, gender, age, schooling, and health affiliation, while the interaction between these factors was evidenced, demonstrating the intersectionality of determinants of the health system, socioeconomic status, and individual determinants in the occurrence of HIV in young people.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Departamento Administrativo Nacional de Estadística [Sociodemographic Overview of Youth in Colombia]; 2020. Available from: https://onx.la/0ac37.
2. UNICEF. ¿Quiénes son los jóvenes de hoy? Una generación sin límites [Who are the youth of today? Generation unlimited]; 2020. Available from: https://onx.la/2381d.
3. Fondo Colombiano de Enfermedades de Alto Costo, Cuenta de Alto Costo (CAC). Situación del VIH y sida en Colombia 2021 [HIV and AIDS Situation in Colombia 2021]; Bogotá DC; 2021. Available from: https://onx.la/3129.
4. ONUSIDA. Estrategia mundial contra el sida (2021–2026). Acabar con las desigualdades [End inequalities. End AIDS]5. [Behavior of HIV/AIDS Reporting, Epidemiological Period XI]. Acabar con el sida; 2021. Available from: https://www.unaids.org/sites/default/files/media_asset/global-AIDS-strategy-2021-2026_es.pdf.
5. Instituto Nacional de Salud. Comportamiento de la notificación de VIH/sida, período epidemiológico XI; 2022. Available from: https://www.ins.gov.co/buscador-eventos/_layouts/15/DocIdRedir.aspx?ID=AVMXRNAJRR5T-1354320881-939.
6. World Health Organization. The Global Fund. State of inequality HIV, tuberculosis and malaria; 2023. Available from: https://www.who.int/publications/i/item/9789240039445.
7. Cardona-Arias JA, Cataño Correa JC, Higuita-Gutiérrez LF. HIV prevalence and associated factors in key groups and general population treated at a health care institution in Colombia in 2019: a cross-sectional study. HIV AIDS. 2020;12:381–391. doi:10.2147/HIV.S259792
8. Oster AM, Johnson CH, Le BC, et al. Trends in HIV prevalence and HIV testing among young MSM: five United States cities, 1994–2011. AIDS Behav. 2014;18(Suppl 3):S237–47. doi:10.1007/s10461-013-0566-1
9. Johnston LG, Soe P, Widihastuti AS, et al. Alarmingly High HIV prevalence among adolescent and young men who have sex with men (MSM) in Urban Indonesia. AIDS Behav. 2021;25(11):3687–3694. doi:10.1007/s10461-021-03347-0
10. Li QH, Wang JY, Liu SY, et al. Young MSM changed temporal HIV-1 epidemic pattern in Heilongjiang Province, China. Front Microbiol. 2022;13:1028383. doi:10.3389/fmicb.2022.1028383
11. Mwaniki SW, Kaberia PM, Mugo PM, Palanee-Phillips T. HIV prevalence and associated risk factors among young tertiary student men who have sex with men (MSM) in Nairobi, Kenya: a respondent-driven sampling survey. AIDS Res Ther. 2023;20(1):7. doi:10.1186/s12981-023-00502-6
12. Kusnan A, Alifariki O, Asriati BIMC, et al. Risk factors for HIV incidence in MSM (male sex man) communities in province of southeast Sulawesi. Enferm Clin. 2020;30(Suppl 2):80–83. doi:10.1016/j.enfcli.2019.07.037
13. Nieuwenburg SA, Sprenger RJ, Schim van der Loeff MF, de Vries HJC. Clinical outcomes of syphilis in HIV-negative and HIV-positive MSM: occurrence of repeat syphilis episodes and non-treponemal serology responses. Sex Transm Infect. 2022;98(2):95–100. doi:10.1136/sextrans-2020-054887
14. Soares CC, Georg I, Lampe E, et al. HIV-1, HBV, HCV, HTLV, HPV-16/18, and Treponema pallidum infections in a sample of Brazilian men who have sex with men. PLoS One. 2014;9(8):e102676. doi:10.1371/journal.pone.0102676
15. Taouqi M, Veyri M, Brégigeon S, et al. Enquête sur la pratique du dépistage du VIH, VHB et VHC en cancérologie, France [Survey on HIV, HBV and HCV screening practices in cancerology, France]. Bull Cancer. 2021;108(4):369–376. French. doi:10.1016/j.bulcan.2020.11.019
16. Al-Mughales JA. Co-infection assessment in HBV, HCV, and HIV patients in Western Saudi Arabia. J Med Virol. 2016;88(9):1545–1551. doi:10.1002/jmv.24503
17. Alcaldía de Medellín. En Medellín se sigue trabajando en prevenir la expansión del VIH Sida [In Medellín, efforts continue to prevent the spread of HIV/AIDS]; 2020. Available from: https://acortar.link/si6AAh.
18. Instituto Nacional de Salud. Vigilancia [Epidemiological surveillance]. SIVIGILA; 2023. Available from: https://www.ins.gov.co/Direcciones/Vigilancia/Paginas/SIVIGILA.aspx.
19. Berbesí D, Segura-Cardona A, Caicedo B, Cardona-Arango D. Prevalencia y factores asociados al VIH en habitante de calle de la ciudad de Medellín, Colombia [Prevalence and Factors Associated with HIV among the Street Dwellers of Medellin, Colombia]. Rev Fac Nac Salud Pública. 2015;33(2):200–205. doi:10.17533/udea.rfnsp.v33n2a07
20. UNAIDS. Young people and HIV; 2021. Available from https://www.unaids.org/sites/default/files/media_asset/young-people-and-hiv_en.pdf.
21. Montana JF, Ferreira GR, Cunha CLF, et al. The HIV epidemic in Colombia: spatial and temporal trends analysis. BMC Public Health. 2021;21(1):178. doi:10.1186/s12889-021-10196-y
22. El colombiano. Extranjeros ofrecen en Medellín ‘paquetes turísticos’ con un ‘harén’ .[Foreigners Offer 'Tourism Packages' with a 'Harem' in Medellín]; 2023. Available from: https://www.elcolombiano.com/antioquia/extranjeros-ofrecen-en-medellin-paquetes-turistcos-con-un-haren-KD20323485.
23. Semana. Las ‘gringo parties’: estas son las extravagancias del turismo sexual en Medellín . ['Gringo Parties': These Are the Extravagances of Sexual Tourism in Medellín]; 2023. Available from: https://www.semana.com/nacion/medellin/articulo/las-gringo-parties-estas-son-las-extravagancias-del-turismo-sexual-en-medellin/202339/.
24. Caracol radio. Una noche en las entrañas de las redes de explotación de niñas en Medellín [One Night in the Depths of Child Exploitation Networks in Medellín]; 2022. Available from https://caracol.com.co/emisora/2022/07/27/medellin/1658947827_026880.html.
25. Centers for disease control and prevention. Men Who Have Sex with Men (MSM); 2021. Available from: https://www.cdc.gov/std/treatment-guidelines/msm.htm.
26. Ossa-Giraldo AC, Correa JS, Moreno CL, et al. Sexual behaviors and factors associated with condomless sexual practice in Colombian men who have sex with men at high risk of HIV transmission. Arch Sex Behav. 2021;50(7):3175–3190. doi:10.1007/s10508-020-01856-y
27. Instituto Nacional de Salud. Informe del evento. VIH, SIDA y muerte por SIDA Colombia [Report on the Event: HIV, AIDS, and AIDS-Related Deaths in Colombia] 2020; Available from: https://www.ins.gov.co/buscador-eventos/Informesdeevento/VIH-SIDA_2020.pdf.
28. Día mundial del VIH y SIDA. Cuenta de Alto costo, Fondo Colombiano de Enfermedades de Alto Costo [High-Cost Account, Colombian High-Cost Disease Fund]; 2021. Available from: https://cuentadealtocosto.org/wp-content/uploads/2021/11/infografia_dia-mundial-del-sida.pdf.
29. Carriquiry G, Fink V, Koethe JR, et al. Mortality and loss to follow-up among HIV-infected persons on long-term antiretroviral therapy in Latin America and the Caribbean. J Int AIDS Soc. 2015;18(1):20016. doi:10.7448/IAS.18.1.20016
30. Raghupathi V, Raghupathi W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Health. 2020;78:20. doi:10.1186/s13690-020-00402-5
31. Bagnall AM, South J, Hulme C, et al. A systematic review of the effectiveness and cost-effectiveness of peer education and peer support in prisons. BMC Public Health. 2015;15:290. doi:10.1186/s12889-015-1584-x
32. Chola L, Fadnes LT, Engebretsen IM, et al. Cost-effectiveness of peer Counselling for the promotion of exclusive breastfeeding in Uganda. PLoS One. 2015;10(11):e142718. doi:10.1371/journal.pone.0142718
33. He J, Wang Y, Du Z, Liao J, He N, Hao Y. Peer education for HIV prevention among high-risk groups: a systematic review and meta-analysis. BMC Infect Dis. 2020;20(1):338. doi:10.1186/s12879-020-05003-9
34. Ministerio de salud y protección social. Aseguramiento al sistema general de salud [Health Insurance in the General Health System]; 2023. Available from: https://acortar.link/ACHrbw.
35. Ministerio de salud y protección social. Comportamiento del aseguramiento [Behavior of Health Insurance]; 2023. Available from: https://acortar.link/tvdhtp.
36. Frescura L, Godfrey-Faussett P, Feizzadeh AA, El-Sadr W, Syarif O, Ghys PD, on and behalf of the 2025 testing treatment target Working Group. Achieving the 95 95 95 targets for all: a pathway to ending AIDS. PLoS One. 2022;17(8):e0272405. doi:10.1371/journal.pone.0272405
37. Beyrer C, Adimora AA, Hodder SL, et al. Call to action: how can the US Ending the HIV Epidemic initiative succeed? Lancet. 2021;397(10279):1151–1156. doi:10.1016/S0140-6736(21)00390-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.